Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Embolia e Microembolia
VII° Corso Nazionale Congiunto Ultrasonologia Vascolare Diagnosi e Terapia Embolia e Microembolia Bertinoro 2009 ULTRASUONI E STENT ALFIO AMATO UO di Angiologia e Malattie della Coagulazione “Marino Golinelli” Dpt. Cardio Toraco Vascolare Policlinico Universitario S.Orsola-Malpighi, Bologna Direttore: Prof. G.Palareti

2
II° Corso Nazionale Congiunto Ultrasonologia Vascolare Diagnosi e Terapia
Bertinoro 2002 STENT ARTERIOSO DALLA TESTA AI PIEDI ALFIO AMATO

6
xxxxxxxxx

8
Real Time US Evaluation in PTA Stentings
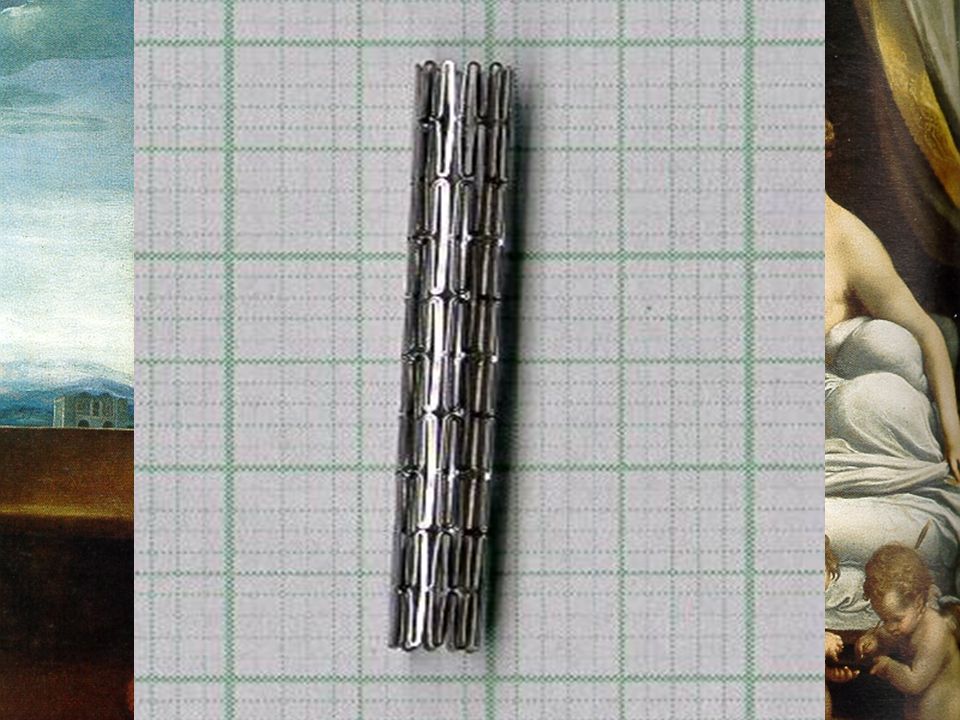
The concept of vascular stenting originated with Charles Dotter in 1969, but did not become part of clinical practice until the late 1980s.

10
Stent: controllo angiografico e con IVUS

12
Evaluation of Four-Year Coronary Artery Response After Sirolimus-Eluting Stent Implantation Using Serial Quantitative Intravascular Ultrasound and Computer-Assisted Grayscale Value Analysis for Plaque Composition in Event-Free Patients Jiro Aoki, Alexandre C. Abizaid et Al. J Am Coll Card, 2005.

13
STENT ARTERIOSI E ULTRASUONI
PTA: la prima metodica di controllo della angioplastica e’ stato l’EcoDoppler e successivamente l’EcoColorDoppler, PTA-STENTING, non si differenziano per quanto riguarda il tipo di diagnostica, ma nel riconoscere parete arteriosa e sistema impiantato.

14
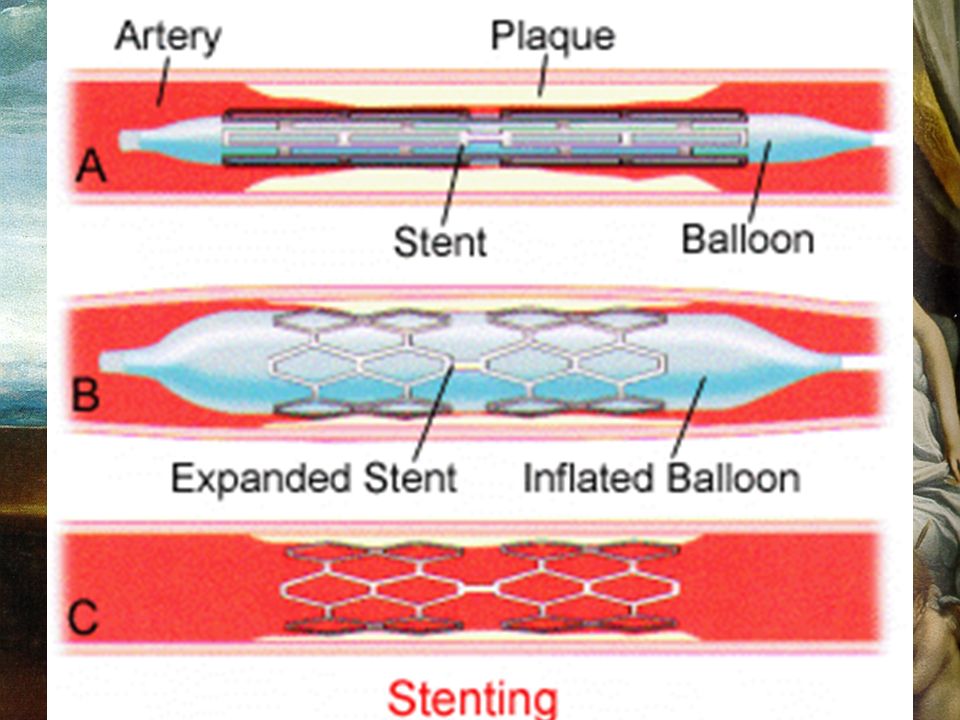
Perché gli stent si vedono?
Echogenic medical device such as a stent for insertion into a biological tissue or vessel comprising an elongate tube and having at least one lumen extending substantially along a longitudinal axis. The elongate tube comprises a material having an acoustic impedance different from the acoustic impedance of the biological tissue or vessel of a patient body such that ultrasonic imaging of the tube inside the patient’s body may be achieved. The elongate tube may comprise a plastic material such as polyethylene or any formable, pliable material. Perché gli stent si vedono?

16
STENT ARTERIOSI E ULTRASUONI
La richiesta di controllo ECD di PTA deve considerare 1-ESATTA SEDE DEL TRATTAMENTO 2-MATERIALE PARIETALE RESIDUO 3-STENOSI RESIDUA 4-STUDIO EMODINAMICO DOPPLER 5-DISSEZIONI SEGMENTARIE 6-FLAP INTIMALI O FRAMMENTI MOBILI

17
STENT ARTERIOSI E ULTRASUONI
Controllo PTA-STENTING -LETTURA DELLE MAGLIE -SEDE DI IMPIANTO PREVISTO -EVENTUALE MIGRAZIONE -DIMENSIONI: diametro, lunghezza. -STENT IMPRONTATO DALLA LESIONE

18
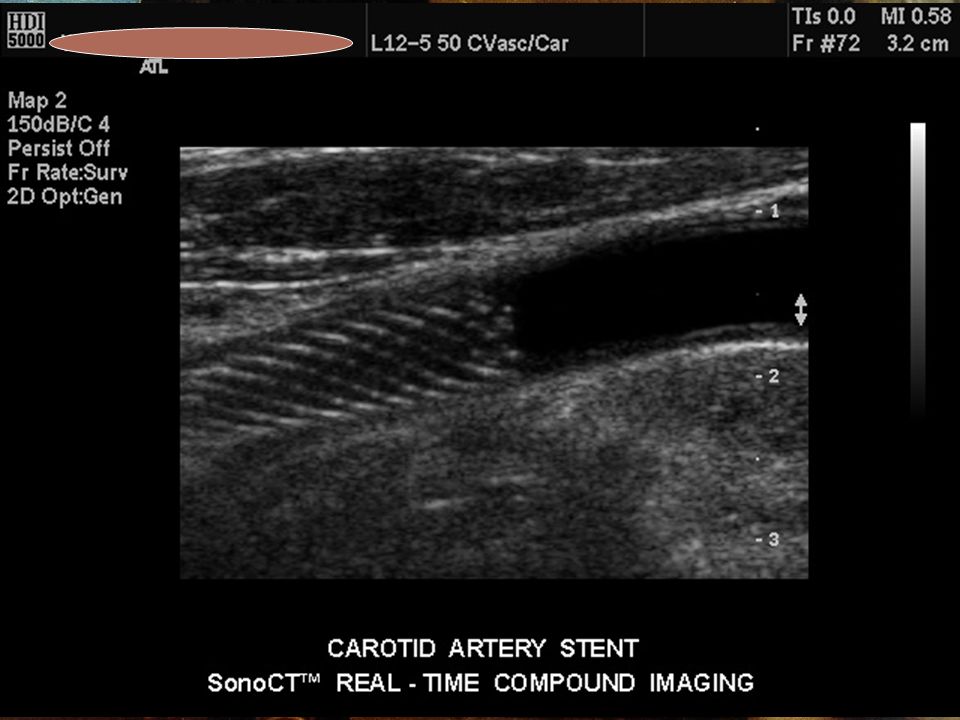
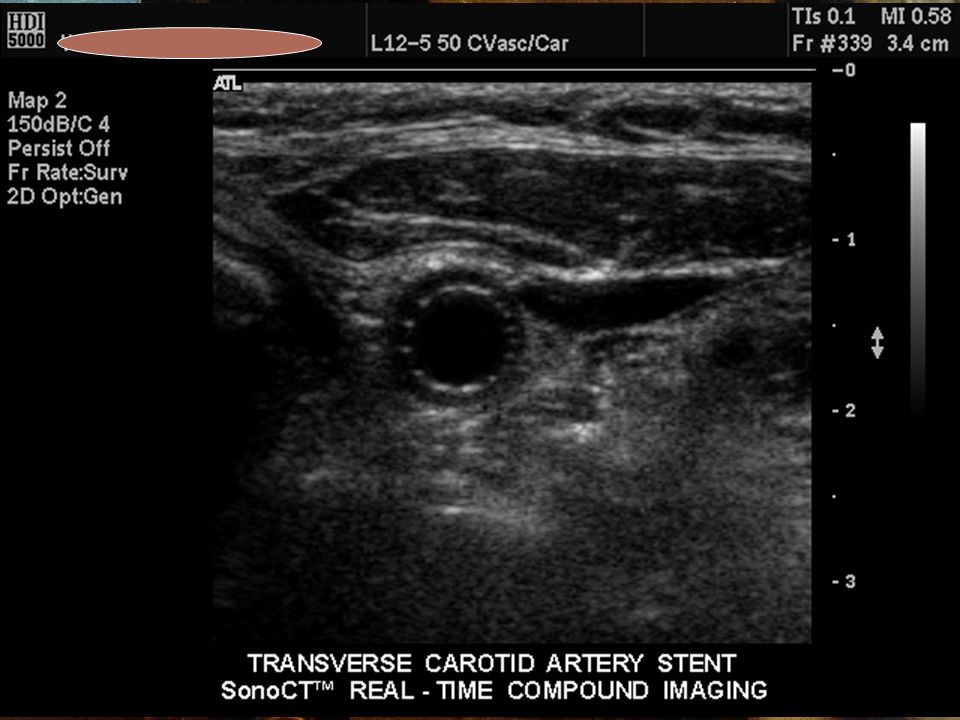
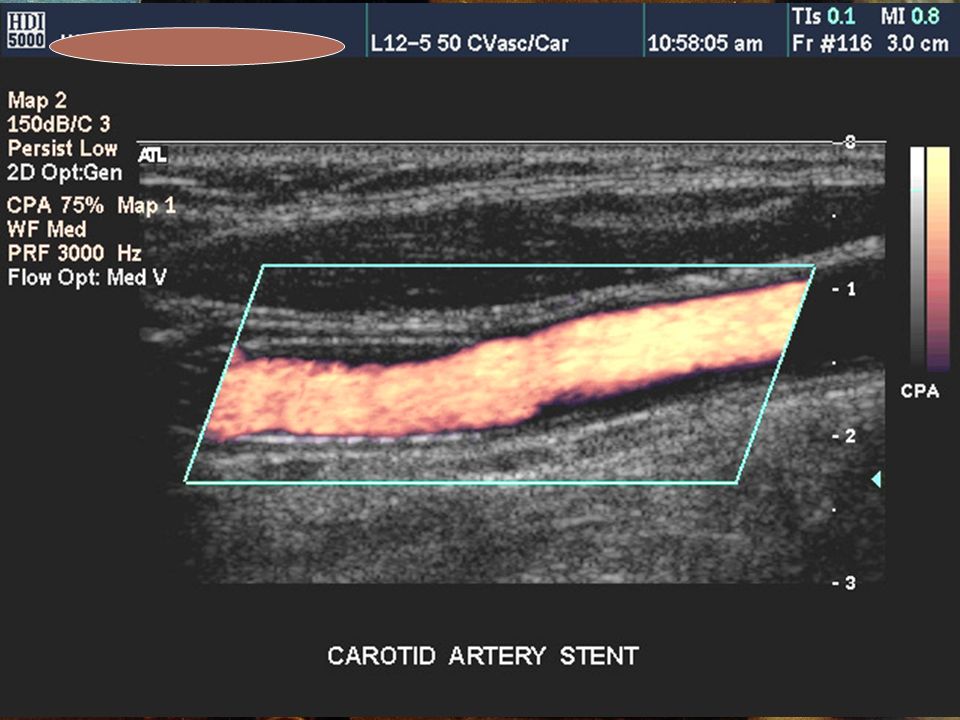
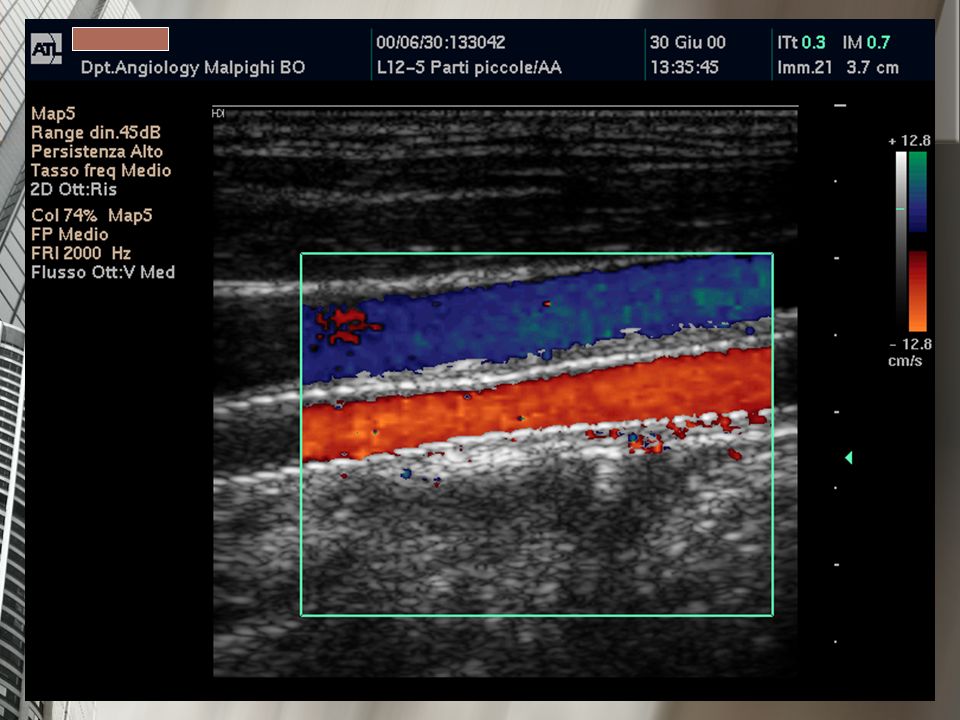
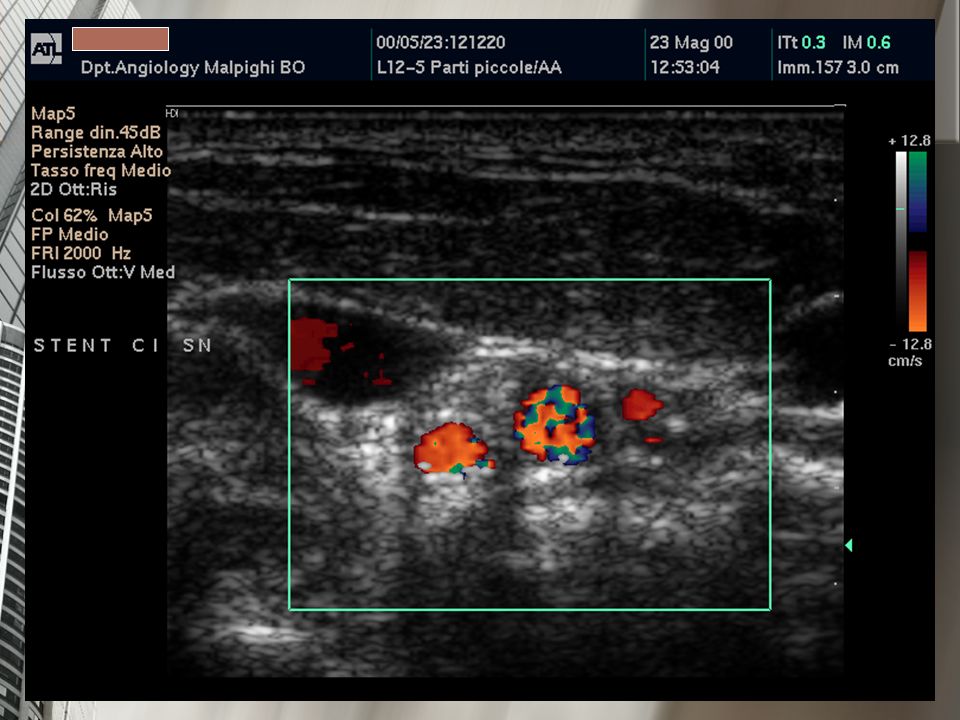
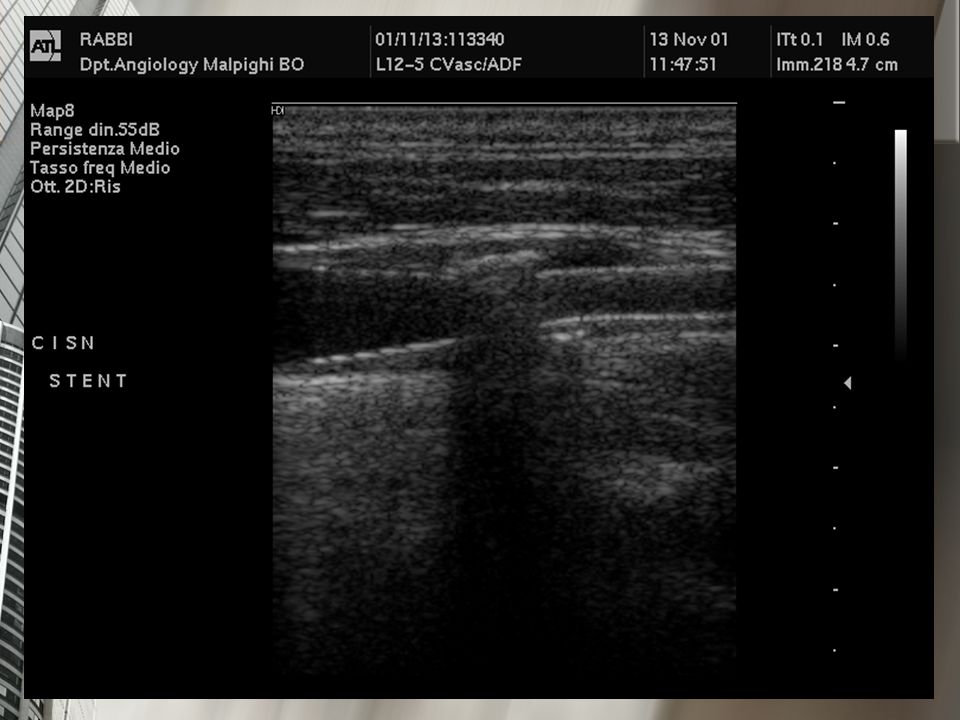
STENT CAROTIDEO

25
STENT POST RESTENOSI IN SEGUITO A TEA CAROTIDEA

26
STENTING CAROTIDEO E TEA Controllo Non Invasivo dei Trattamenti
CONTROLLI POST TEA Pervietà della CI e CE Grado di ristenosi: segmento trattato, tratto a monte e a valle -morfologia e velocità- Trombo parietale e sede Gradino della CC Lembi mobili Dissezioni parietali

28
xxxxxxxxx

29
xxxxxxxxx POST-TEA

31
xxxxxxxxx

33
xxxxxxxxx

37
STENT ARTERIA ILIACA

39
xxxxxxxxx

40
Occlusione di stent: dissezione sottointimale e stenosi compressiva

41
Le procedure endovascolari sempre piu’ diffuse richiedono abitualmente un importante utilizzo di xRay. Lo sviluppo attuale dei sistemi EchoColor e Power Doppler, basic or with armonics, and also the echo-enhancers bubbles, …dovrebbe indirizzare ad un maggior utilizzo nella PTA-stenting dei sistemi US.

43
STENT ARTERIA POPLITEA (?)
")
45
xxxxxxxxx

48
STENTING CAROTIDEO E TEA Controllo Non Invasivo dei Trattamenti
CONTROLLI POST TEA morfologia : ecogenicità della lesione superficie, estensione, diametro minimo velocità: criteri adeguati alla nuova condizione segmentaria

49
STENTING CAROTIDEO Eco Color Doppler
Adesione dello stent alla parete del vaso Presenza di angolazioni (kinking) della carotide interna alla fine dello stent prodotte dalla diversa compliance fra stent e carotide Migrazione dello stent Integrità o rotture dello stent Eventuali complicanze relative ad un precedente intervento di endoarterectomia (distacco di patch) Diametro – area residua lungo lo stent PSV – EDV
 della carotide interna alla fine dello stent prodotte dalla diversa compliance fra stent e carotide. Migrazione dello stent. Integrità o rotture dello stent. Eventuali complicanze relative ad un precedente intervento di endoarterectomia (distacco di patch) Diametro – area residua lungo lo stent. PSV – EDV.")
50
• Pervietà della carotide esterna
VALUTAZIONE ECD STENT I parametri da valutare sono diversi da quelli che si considerano dopo intervento chirurgico • Pervietà della carotide interna • Pervietà della carotide esterna • Presenza di stenosi nel segmento trattato • Presenza di stenosi (nuovo ateroma, iperplasia, trombo) all’interno dello stent (in-stent restenosis) • Presenza di stenosi a monte o a valle dello stent • Presenza di trombo parietale
 all’interno dello stent. (in-stent restenosis) • Presenza di stenosi a monte o a valle dello stent. • Presenza di trombo parietale.")
51
CONTROLLI ECO COLOR DOPPLER POST TEA
Color Doppler a mesi. poi a anni. Se la carotide controlaterale è stenotica eseguire i controlli secondo il follow-up per le stenosi note. ANALOGHI CONTROLLI POST STENT (?) E dopo molti anni (?)
 E dopo molti anni ( )")
52
ICAROS STUDY Imaging in Carotid Angioplasties and Risk Of Stroke
Registro internazionale multicentrico stenting carotideo Indentificazione pazienti ad alto e basso rischio di stroke ad 1 anno Biasi GM, Nicolaides AN et Al, J Endovasc Ther, 2001 Biasi GM, Diethrich EB, Nicolaides AN, Circulation, 2004

53
IVUS IN CAROTID STENTING
CONTROLLI SERIATI ENDOVASCOLARI POST PROCEDURA E DOPO 6 MESI Diametro minimo del lume Misurazione dell’area di impianto Area dello stent Area dell’iperplasia neointimale Clark DJ et Al, J Am Coll Cardiol, 2006

54
IVUS IN CAROTID STENTING
I “self-expanding stents” determinano una notevole iperplasia della neointima Processo bilanciato dal tardivo incremento del diametro dello stent Dimensioni ridotte dello stent subito dopo la procedura sono associate con alto rischio di “in-stent restenosis” Clark DJ et Al, J Am Coll Cardiol, 2006

55
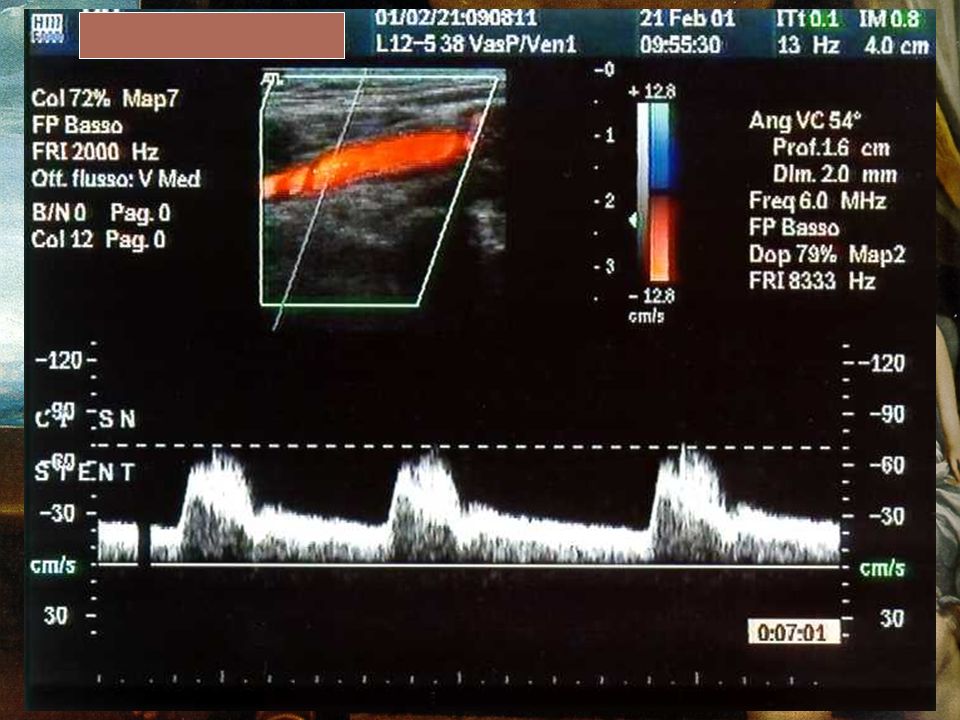
nuovi criteri velocimetrici
Lo stent riduce la compliance dell’arteria e pertanto i criteri velocimetrici normalmente utilizzati per la valutazione della stenosi possono non essere applicabili. Gli studi in Letteratura in proposito sono in incremento.

56
nuovi criteri velocimetrici
Lal BK et Al. propongono i seguenti valori per identificare una carotide normale dopo stenting (stenosi < 20%): • PSV < 150 cm/s, • ICA/CCA ratio < 2.16 J Vasc Surg Jan;39(1):58-66 Dovranno essere definiti nuovi criteri velocimetrici per le varie classi di stenosi
: • PSV < 150 cm/s, • ICA/CCA ratio < J Vasc Surg Jan;39(1): Dovranno essere definiti nuovi criteri velocimetrici per le varie classi di stenosi.")
57
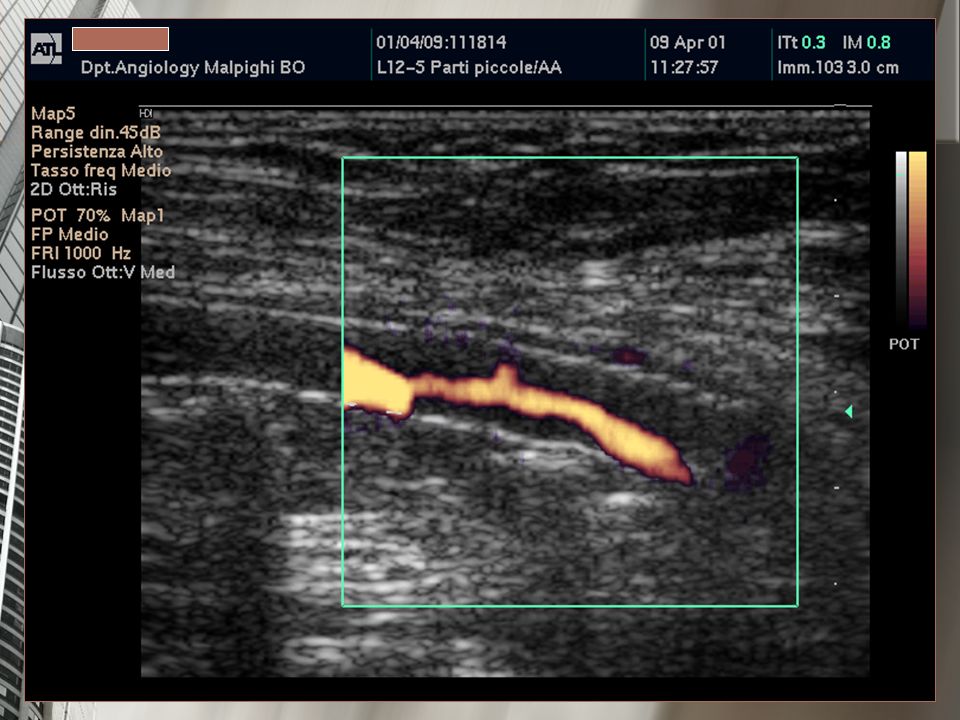
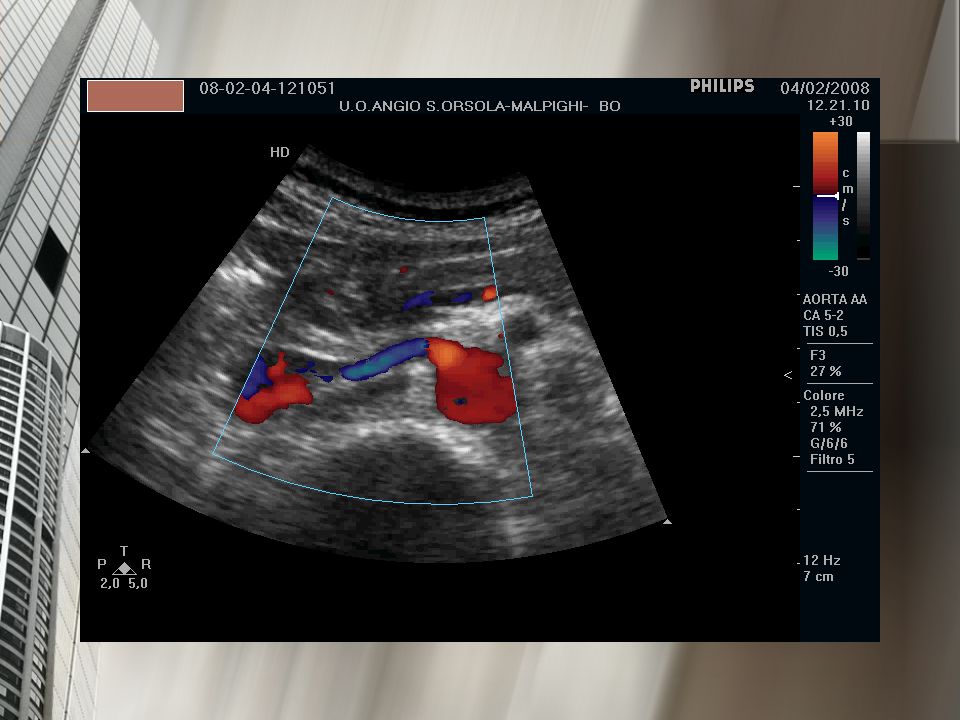
Real Time US Evaluation in PTA Stentings
In 1988 our group in Bologna, together with angioradiologists, performed an Echo Doppler PTA procedure of Common Iliac Artery stenosis. It was the first Echo-Duplex guided PTA treatment in Italy. We presented the procedure on video-tape during a session of the Italian Society of Vascular Pathology.

58
Real Time US Evaluation in PTA Stentings
A young male smoker (aged 42 years), with a segmentary atheromasic lesion of the common iliac artery discovered by Duplex Scanner evaluation for PAD symptoms,underwent a simple PTA of the vessel. Stents were not yet used in clinical practical.
, with a segmentary atheromasic lesion of the common iliac artery discovered by Duplex Scanner evaluation for PAD symptoms,underwent a simple PTA of the vessel. Stents were not yet used in clinical practical.")
59
PTA-STENTING Possibilità di effettuare la procedura con guida Eco Color Doppler (?) per: Valutare gli effetti sulla parete vasale Effettuare brevi campionamenti Doppler Ridurre la durata della manovra ??

60
Real Time US Evaluation in PTA Stentings
STENTS CANNOT PREVENT RESTENOSIS 1. Restenosis is believed to start the instant of balloon angioplasty –stent placement secondary to the vascular injury that occurs when a narrowed artery is forcibly expanded. 2. Trauma to the vessel in the form of shearing of the intima and fissuring on the wall of the vessel may induce excessive deposition of fibrin, platelets and leukocytes. Schatz, Circulation,1989; Palmaz, AJR, 1993; Serruys, Heparin pilot study, Circul.1996

61
TREATMENT OF CAROTID STENOSIS: CAROTID SURGERY OR STENT?
ROLE OF DUPLEX ULTRASOUND (US): Degree of stenosis Plaque morphology - soft vs hard -trhombotic or ulcerous formations • Detection of HITS by transcranial Doppler
: Degree of stenosis. Plaque morphology - soft vs hard. -trhombotic or ulcerous formations. • Detection of HITS by transcranial Doppler.")
62
CAROTID STENTS: Duplex US follow-up of arterial remodelling
Diameter increase (over 2 years) Neo-intimal thickness increase (up to 12 months) Flow-ratio increase (douring first year) Compliance reduction Intravascular us scanning of beta emitting ((55)Co) stents
 Neo-intimal thickness increase (up to 12 months) Flow-ratio increase (douring first year) Compliance reduction. Intravascular us scanning of beta emitting ((55)Co) stents.")
63
US Evaluation in PTA Stentings Factors not reducing restenosis
Type of metal Surface area of the stent Degree of hoop strength of the stent Heparin coating Long term Warfarin Anti-platelet therapy (?)
")
64
Plaques with: stenosis ≥90% low echogenicity
produced a higher number of embolic particles after ex vivo balloon angioplasty and stenting. Therefore these lesions may be less suitable for balloon angioplasty and stenting with currently used devices. Ex vivo human carotid artery bifurcation stenting: Correlation of lesion characteristics with embolic potential. Takao Ohki, Michael L. Marin, Ross T. Lyon, George L. Berdejo, Krish Soundararajan, Mika Ohki, Peter L. Faries, Reese A. Wain, Luis A. Sanchez, William D. Suggs, Frank J. Veith. J Vasc Surg 1998; 27:463-71

65
STENT MARKET ? 17% ANNUAL GROWTH FORECAST IN PERIPHERAL VASCULAR STENT MARKET MR-velocity mapping in vascular stents to assess peak systolic velocity. In vitro comparison of various stent designs made of Stainless Steel and Nitinol. Jacqueline van Holten, Patrik Kunz, Paul G. H. Mulder,Peter M.T. Pattynama, Hildo J. Lamb, Magnetic Resonance Materials in Physics, Biology and Medicine 15 (2002) 52-57
")
66
The missing stent Missed Double-J stent by ultrasonography.
G. Pandurangan, B.Bastani. Nephrol Dial Transplant (2000) 15: The Missing Stent - The Most Improbable Complication B. Schmidta, A. Gramseb, A. Heringb, U. Liebersa, S. Hörniga, M. Johna, C. Witta. Respiration 2005;72:304
 15: The Missing Stent - The Most Improbable Complication B. Schmidta, A. Gramseb, A. Heringb, U. Liebersa, S. Hörniga, M. Johna, C. Witta. Respiration 2005;72:304.")
67
Healing of Carotid Stents: A Prospective Duplex Ultrasound Study Andrea Willfort-Ehringer; Ramazanali Ahmadi; Michael E. Gschwandtner; Angelika Haumer; Gottfried Heinz; Wilfried Lang; Herbert Ehringer Journal of Endovascular Therapy: Vol. 10, No. 3, 2005 Day after the stent procedure and at 1, 3, 6, 12, and 24 months in follow-up: The maximal thickness and echogenicity of the layer between the stent and the perfused lumen (SPL) were evaluated. Echogenicity was classified as echogenic if the SPL layer was clearly detected in B mode and echolucent if the SPL layer was barely visible in B mode, its border defined by assistance of color-coded flow. 1) an early unstable period soon after stent placement with an echolucent (thrombotic) SPL layer, (2) a moderately unstable phase with ingrowing neointima (1–12 months), (3) a stable phase from the second year on. These data may indicate the need for different intensities of therapy and surveillance intervals.
 were evaluated. Echogenicity was classified as echogenic if the SPL layer was clearly detected in B mode and echolucent if the SPL layer was barely visible in B mode, its border defined by assistance of color-coded flow. 1) an early unstable period soon after stent placement with an echolucent (thrombotic) SPL layer, (2) a moderately unstable phase with ingrowing neointima (1–12 months), (3) a stable phase from the second year on. These data may indicate the need for different intensities of therapy and surveillance intervals.")
68
Risk of Stroke in Carotid Stenting (?)
Plaque Echolucency Is Not Associated With the Risk of Stroke in Carotid Stenting Markus Reiter; Robert A. Bucek; Isabella Effenberger; Johanna Boltuch; Wilfried Lang; Ramazanali Ahmadi; Erich Minar; Martin Schillinger. Stroke. 2006;37: ?

69
Survival Following Renal Artery Stent Revascularization.
Four-year Follow-up. Mayra Guerrero, Asmir Syed, Sandeep Khosla. J Invasive Cardiology, 2004 In our database, patients undergoing renal artery stent revascularization for suspected renovascular hypertension had an overall survival of 83% at 4 years post procedure. Patients with higher baseline serum creatinine, male gender, bilateral renal artery stenosis and systolic dysfunction, had statistically significant lower survival at 4 years.

70
The future It is hoped that the next generation of stents will combine the mechanical advantages of stents with pharmacologic advantages and coverings which will prove to have a substantial impact on the restenosis issue.

Presentazioni simili




























 devices receive FDA approval annually 3500 medium-risk (class II) products are approved for marketing.>")
