Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Dipartimento Cardiovascolare, Cà Foncello, Treviso
ANTIPIASTRINICI E ANTICOAGULANTI NEI PAZIENTI CON SCA Quando come e perché gli inibitori P2Y12 Zoran Olivari Dipartimento Cardiovascolare, Cà Foncello, Treviso Genova 15 novembre 2013,

2
Inibitori recettore piastrinico P2Y12
Clopidogrel Prasugrel Ticagrelor Cangrelor Dosaggio 60 mg/die (os) 10 mg /die (os) mg/die (os) EV Reversibilità NO SI’ Si’ Profarmaco SI’ (two steps) SI’ (one step) Tempo alla max. inibizione piastrinica 4-6 ore 2-4 ore 1-2 ore immediato Emivita 6 ore 7 ore 7-8,5 ore 3-5 minuti
 10 mg /die (os) mg/die (os) EV. Reversibilità. NO. SI’ Si’ Profarmaco. SI’ (two steps) SI’ (one step) Tempo alla max. inibizione piastrinica. 4-6 ore. 2-4 ore. 1-2 ore. immediato. Emivita. 6 ore. 7 ore. 7-8,5 ore. 3-5 minuti.")
3
Inibitori recettore piastrinico P2Y12
Clopidogrel Prasugrel Ticagrelor Cangrelor Studi a disposizione CURE (2001) TRITON TIMI 38 (2007) TRILOGY ACS (2012) ACCOAST (2013) PLATO (2009) CHAMPION (2013)
 TRITON TIMI 38 (2007) TRILOGY ACS (2012) ACCOAST (2013) PLATO (2009) CHAMPION (2013)")
4
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% The Lancet, 2013 Pretrattati con clopidogrel 11%

5
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% Morte, IMA, isch. driven revasc, trombosi stent 48 ore 30 gg The Lancet, 2013 Pretrattati con clopidogrel 11%

6
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% Morte, IMA, isch. driven revasc, trombosi stent 48 ore 30 gg The Lancet, 2013 Pretrattati con clopidogrel 11%

7
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% Trombosi stent 48 ore 30 gg The Lancet, 2013 Pretrattati con clopidogrel 11%

8
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% Trombosi stent 48 ore 30 gg The Lancet, 2013 Pretrattati con clopidogrel 11%

9
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% The Lancet, 2013 Pretrattati con clopidogrel 11%

10
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% 0,5% vs 0,7% NNT = 500 The Lancet, 2013 Pretrattati con clopidogrel 11%

11
Pretrattati con clopidogrel 11%
24910 pz STEMI 11,6% NSTEMI 57,4% Stable 31% TIMI non CABG bleeding 48 ore NNH = 1000 The Lancet, 2013 Pretrattati con clopidogrel 11%

12
24910 pz Conclusione personale Quesiti aperti
STEMI 11,6% NSTEMI 57,4% Stable 31% Conclusione personale Cangrelor è più efficace rispetto al clopidogrel nel ridurre gli eventi periprocedurali della PCI (fondamentalmente nelle prime 6 ore), senza incremento di complicanze emorragiche maggiori IN PAZIENTI NON PRETRATTATI CON LA DAPT Quesiti aperti 1) in pz pretrattati con clopidogrel ? 2) prasugrel/ticagrelor durante la procedura ?
, senza incremento di complicanze emorragiche maggiori. IN PAZIENTI NON PRETRATTATI CON LA DAPT. Quesiti aperti. 1) in pz pretrattati con clopidogrel 2) prasugrel/ticagrelor durante la procedura")
13
Quale farmaco a quale paziente?
STEMI vs NSTEMI Strategia conservativa in UA/NSTEMI Dopo PCI in pazienti a rischio aumentato: anziani, già TIA/stroke, diabetici, insufficienza renale

14
Quale farmaco a quale paziente?
STEMI vs NSTEMI Strategia conservativa in UA/NSTEMI Dopo PCI in pazienti a rischio aumentato: anziani, già TIA/stroke, diabetici, insufficienza renale

15
Primary Efficacy Endpoint
Primary Composite Endpoint Over Time in the STEMI Populations in PLATO and TRITON Trials PLATO TRITON N=7544 Primary Efficacy Endpoint 2 4 8 12 6 10 Clopidogrel Ticagrelor Cumulative incidence (%) Primary Efficacy Endpoint 15 10.8 N=3534 Cumulative incidence (%) 12.4 p=0.07 p=0.02 9.4 10.0 10 9.5 6.5 5 Clopidogrel Prasugrel HR=0.87 (0.75–1.01) HR=0.79 (0.65–0.97) 50 100 150 200 250 300 350 400 450 Time (Months) Time (Days) Steg PG, et al. Circulation 2010;122:2131 Montalescot G, et al. Lancet 2009;373:723
 Primary Efficacy Endpoint N=3534. Cumulative incidence (%) p=0.07. p= Clopidogrel. Prasugrel. HR=0.87 (0.75–1.01) HR=0.79 (0.65–0.97) Time (Months) Time (Days) Steg PG, et al. Circulation 2010;122:2131. Montalescot G, et al. Lancet 2009;373:723.")
16
Primary Efficacy Endpoint
Primary Composite Endpoint Over Time in the STEMI Populations in PLATO and TRITON Trials PLATO TRITON N=7544 Primary Efficacy Endpoint 2 4 8 12 6 10 Clopidogrel Ticagrelor Cumulative incidence (%) Primary Efficacy Endpoint 15 10.8 N=3534 Cumulative incidence (%) 12.4 p=0.07 p=0.02 9.4 10.0 10 9.5 6.5 Non beneficio se sottoposti alla PCI primaria 5 Clopidogrel Prasugrel HR=0.87 (0.75–1.01) HR=0.79 (0.65–0.97) 50 100 150 200 250 300 350 400 450 Time (Months) Time (Days) Steg PG, et al. Circulation 2010;122:2131 Montalescot G, et al. Lancet 2009;373:723
 Primary Efficacy Endpoint N=3534. Cumulative incidence (%) p=0.07. p= Non beneficio se sottoposti alla PCI primaria. 5. Clopidogrel. Prasugrel. HR=0.87 (0.75–1.01) HR=0.79 (0.65–0.97) Time (Months) Time (Days) Steg PG, et al. Circulation 2010;122:2131. Montalescot G, et al. Lancet 2009;373:723.")
17
Mortalità totale nello STEMI
PLATO (12 mesi) Triton TIMI 38 (15 mesi) HR = 0.82 ( ), p=0,05 HR = 0.76 ( ), p=0,11
 Triton TIMI 38 (15 mesi) HR = 0.82 ( ), p=0,05. HR = 0.76 ( ), p=0,11.")
18
Prasugrel > Clopidogrel Ticagrelor > Clopidogrel
…quindi nello STEMI Prasugrel > Clopidogrel Ticagrelor > Clopidogrel

19
STEMI: cosa dicono le Linee Guida
ESC 2012 pz sottoposti alla PCI classe livello ASA + ticagrelor oppure ASA + prasugrel (invece di ASA+ clopiodgrel) I A
 I. A.")
20
STEMI: cosa dicono le Linee Guida
ESC 2012 pz sottoposti alla PCI ACC/AHA 2013 pz sottoposti alla PCI classe livello ASA + ticagrelor oppure ASA + prasugrel (invece di ASA+ clopiodgrel) I A classe livello ASA + Clopidogrel I B ASA + Ticagrelor ASA + Prasugrel
 I. A. classe. livello. ASA + Clopidogrel. I. B. ASA + Ticagrelor. ASA + Prasugrel.")
21
End point primario nello UA/NSTEMI (morte CV+IMA+stroke)
TRITON TIMI PLATO (15 mesi) (12 mesi) RRR = 18% RRR = 17% HR = 0.83 CI HR = 0.82 CI
 (12 mesi) RRR = 18% RRR = 17% HR = CI HR = CI")
22
Sanguinamenti TIMI major (non CABG related)
TRITON TIMI PLATO (15 mesi) (12 mesi) p = 0, p = 0.03
 (12 mesi) p = 0,03 p =")
23
…quindi nell’ UA/NSTEMI + PCI
Prasugrel > Clopidogrel Ticagrelor > Clopidogrel

24
NSTEMI: cosa dicono le Linee Guida
ESC : 2011 classe livello Ticagrelor a tutti i pz con rischio almeno moderato (Tp+), inclusi anche coloro già in terapia con clopidogrel I B Prasugrel in pz non in terapia con inibitori P2Y12 (in particolare i diabetici), con anatomia coronarica nota e che fanno PCI, non ad alto rischio emorragico Clopidogrel in coloro che non possono ricevere né prasugrel né ticagrelor A
, inclusi anche coloro già in terapia con clopidogrel. I. B. Prasugrel in pz non in terapia con inibitori P2Y12 (in particolare i diabetici), con anatomia coronarica nota e che fanno PCI, non ad alto rischio emorragico. Clopidogrel in coloro che non possono ricevere né prasugrel né ticagrelor. A.")
25
NSTEMI: cosa dicono le Linee Guida
ESC : 2011 ACC/AHA : 2012 (strategia invasiva) classe livello Ticagrelor a tutti i pz con rischio almeno moderato (Tp+), inclusi anche coloro già in terapia con clopidogrel I B Prasugrel in pz non in terapia con inibitori P2Y12 (in particolare i diabetici), con anatomia coronarica nota e che fanno PCI, non ad alto rischio emorragico Clopidogrel in coloro che non possono ricevere né prasugrel né ticagrelor A classe livello PRE PCI Ticagrelor o clopidogrel I B DOPO PCI Clopidogrel se non iniziato prePCI A Ticagrelor o prasugrel
 classe. livello. Ticagrelor a tutti i pz con rischio almeno moderato (Tp+), inclusi anche coloro già in terapia con clopidogrel. I. B. Prasugrel in pz non in terapia con inibitori P2Y12 (in particolare i diabetici), con anatomia coronarica nota e che fanno PCI, non ad alto rischio emorragico. Clopidogrel in coloro che non possono ricevere né prasugrel né ticagrelor. A. classe. livello. PRE PCI. Ticagrelor o clopidogrel. I. B. DOPO PCI. Clopidogrel se non iniziato prePCI. A. Ticagrelor o prasugrel.")
26
Quale farmaco a quale paziente?
STEMI vs NSTEMI Strategia conservativa in UA/NSTEMI Dopo PCI in pazienti a rischio aumentato: anziani, già TIA/stroke, diabetici, insufficienza renale

27
Tasso pz NON rivascolarizzati UA/NSTEMI
RCT: prevista strategia invasiva RCT: nessuna specifica strategia prevista per protocollo UA/NSTEMI Studi osservazionali

28
CURE (CV death, MI,stroke)
")
29
CURE (CV death, MI,stroke)
")
30
CURE

31
Assenza di interazione tra i 2 periodi: 0-360 e 361-900
Obiettivo Primario di efficacia a 30 mesi Analisi principale Assenza di interazione tra i 2 periodi: e

32
Assenza di interazione tra i 2 periodi: 0-360 e 361-900
Obiettivo Primario di efficacia a 30 mesi Analisi principale Assenza di interazione tra i 2 periodi: e

33
HR 0,75 (0,61-0,93), p = 0,010 HR 0,85 (0,73-1,00), p = 0,045 non inv non inv
, p = 0,010 HR 0,85 (0,73-1,00), p = 0,045 non inv non inv")
34
HR 0,75 (0,61-0,93), p = 0,010 HR 0,85 (0,73-1,00), p = 0,045 non inv non inv
, p = 0,010 HR 0,85 (0,73-1,00), p = 0,045 non inv non inv")
35
HR 1,17 (0,98-1,39), p = 0,079
, p = 0,079")
36
Ticagrelor Clopidogrel HR 12.2% 15.2% 0,81 (0.68-0.97)
3948/7955 pz con NSTEMI (escluse UA e STEMI) non rivascolarizzati in H (a prescindere della strategia iniziale) Ticagrelor Clopidogrel HR 1-Y Primary end point (CV death, MI, stroke) 12.2% 15.2% 0,81 ( ) Major bleeding = ?
 non rivascolarizzati in H. (a prescindere della strategia iniziale) Ticagrelor. Clopidogrel. HR. 1-Y Primary end point. (CV death, MI, stroke) 12.2% 15.2% 0,81 ( ) Major bleeding =")
37
…quindi nell’ UA/NSTEMI e strategia conservativa
Ticagrelor > Clopidogrel Prasugrel = Clopidogrel

38
I A B Classe LOE Pz in terapia medica (no stent) ASA (per sempre)
Clopidogrel (75 mg) o Ticagrelor (90 mg x 2) per 12 mesi B
 o Ticagrelor (90 mg x 2) per 12 mesi. B.")
39
Quale farmaco a quale paziente?
STEMI vs NSTEMI Strategia conservativa in UA/NSTEMI Dopo PCI in pazienti a rischio aumentato: anziani, già TIA/stroke, diabetici, insufficienza renale

40
Pz con pregresso TIA / stroke

41
Am J Cardiol 2011;108:905–911 III = già TIA/stroke

42
Am J Cardiol 2011;108:905–911 III = già TIA/stroke

43
Controindicazione assoluta al prasugrel
Am J Cardiol 2011;108:905–911 III = già TIA/stroke Controindicazione assoluta al prasugrel

44
Circulation. 2012;125:

45
Are the data presented today reassuring enough to treat ACS patients with a history of stroke routinely with ticagrelor rather than with clopidogrel? The number of patients with previous stroke in the ACS trials mentioned is low (4%–6%), and the number of excess intracranial bleedings by novel dual antiplatelet therapy even lower (1%–2% of that subpopulation). Therefore, in the case of ticagrelor the test for interaction is not statistically significant, but given the insufficient data an interaction cannot be excluded either. Given the above, there is no safe ground to treat ACS patients with a previous stroke or TIA routinely with the novel platelet P receptor antagonists prasugrel or ticagrelor rather than with clopidogrel. Circulation. 2012;125:
, and the number of excess intracranial bleedings by novel dual antiplatelet therapy even lower (1%–2% of that subpopulation). Therefore, in the case of ticagrelor the test for interaction is not statistically significant, but given the insufficient data an interaction cannot be excluded either. Given the above, there is no safe ground to treat ACS patients with a previous stroke or TIA routinely with the novel platelet P receptor antagonists prasugrel or ticagrelor rather than with clopidogrel. Circulation. 2012;125:")
46
…quindi in pz con già TIA/stroke
Ticagrelor > o = Clopidogrel Prasugrel < Clopidogrel

47
Pz anziani (> 75 anni)
")
48
Am J Cardiol 2011;108:905–911 II = <60 kg o >75 anni

49
PLATO 2009

50
PLATO 2009

51
…quindi nel pz > 75 anni
Ticagrelor = ( o >) Clopidogrel Prasugrel = Clopidogrel
 Clopidogrel Prasugrel = Clopidogrel")
52
Diabete mellito

53
Primary efficacy end-point
I = no TIA/stroke + >60 kg + <75 anni II = <60 kg o >75 anni Am J Cardiol 2011;108:905–911

54
Il beneficio clinico risulta ancora più elevato nei pazienti diabetici.
Wiviott SD, N Engl J Med 2007;357(20):
:")
55
PLATO 2009

56
…quindi in pz diabetici
Ticagrelor > Clopidogrel Prasugrel >> Clopidogrel

57
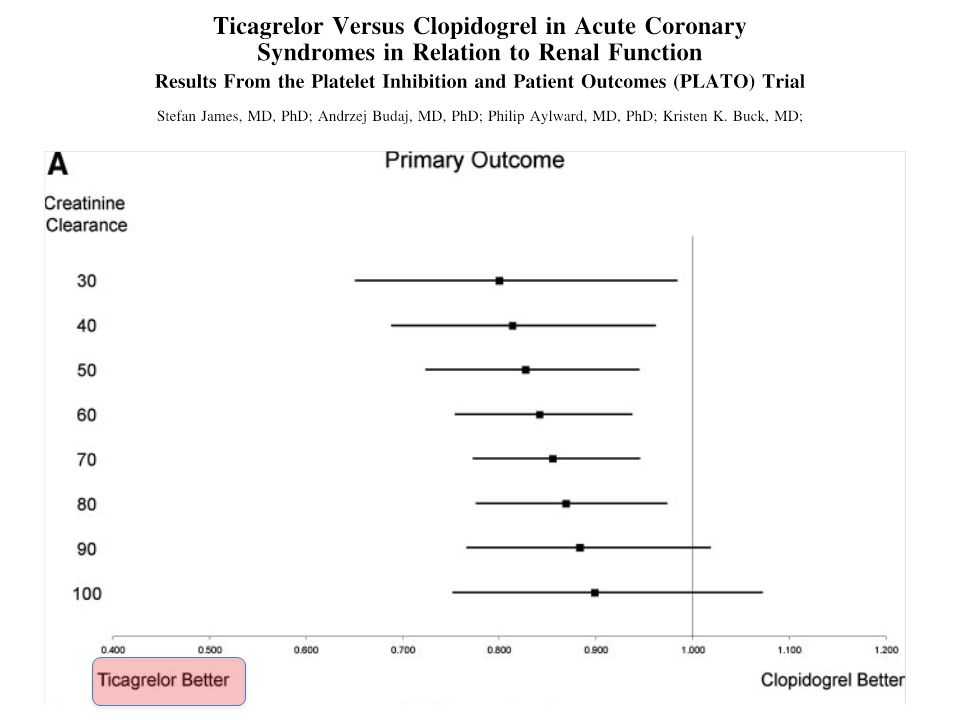
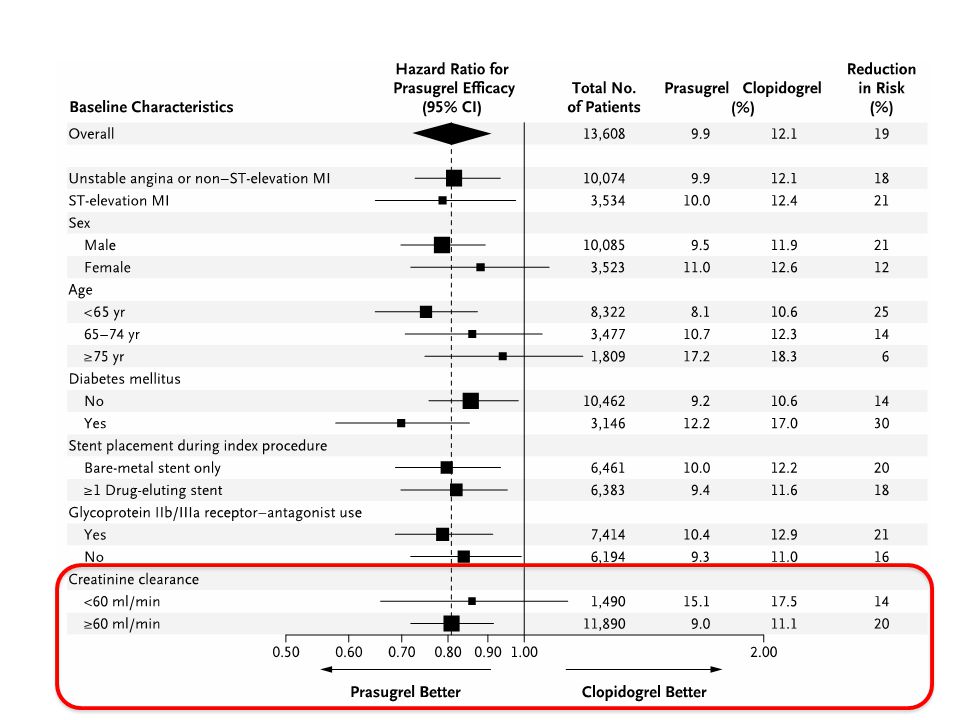
Insufficienza renale

59
HR = 0,72 (0,58-0,89) 14 % 10% Clopidogrel Ticagrelor
 14 % 10% Clopidogrel Ticagrelor")
60
HR = 1,28 (0,97-1,68) 8,5% 7,3% HR = 1,22 (0,98-1,51)
 8,5% 7,3% HR = 1,22 (0,98-1,51)")
62
…quindi in pz con insufficienza renale
Ticagrelor >> Clopidogrel Prasugrel > Clopidogrel

64
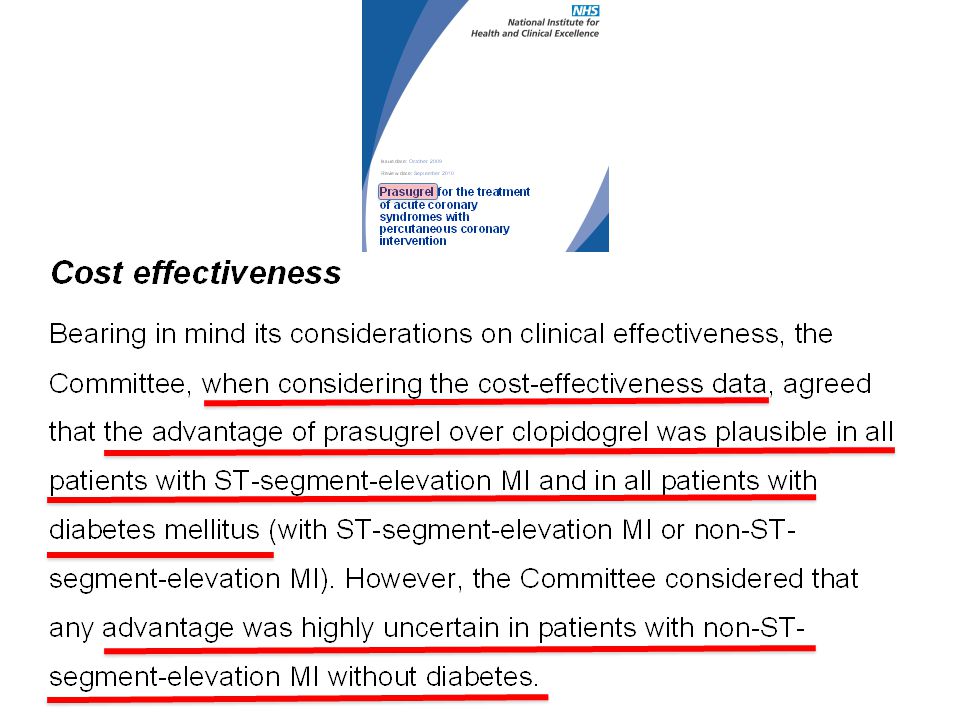
Most likely cost-effectiveness estimate (given as an ICER)
The Committee accepted the ERG's adjustments to the manufacturer's model and agreed that the central ICERs from the ERG's sensitivity analysis : £7897 per QALY gained for all ACS, £8872 per QALY gained for STEMI, £7215 per QALY gained for NSTEMI and £9131 per QALY gained for unstable angina represented the most plausible estimates for the cost effectiveness of ticagrelor compared with clopidogrel. Ticagrelor cost/effective in tutte le manifestazioni cliniche delle SCA

65
…. quello che non si dovrebbe fare, ma nella pratica clinica non si può fare a meno

66
14 RCT Prasu vs clopi SD (2) Tica vs clopi SD (1)
Clopi HD vs clopi SD (9) Prasu vs clopi HD (2) Thromb Haemost 2012; 108: 318–327
 Prasu vs clopi HD (2) Thromb Haemost 2012; 108: 318–327.")
67
14 RCT Prasu vs clopi SD (2) Tica vs clopi SD (1)
Clopi HD vs clopi SD (9) Prasu vs clopi HD (2) Thromb Haemost 2012; 108: 318–327
 Prasu vs clopi HD (2) Thromb Haemost 2012; 108: 318–327.")
68
14 RCT Prasu vs clopi SD (2) Tica vs clopi SD (1)
Clopi HD vs clopi SD (9) Prasu vs clopi HD (2) Thromb Haemost 2012; 108: 318–327
 Prasu vs clopi HD (2) Thromb Haemost 2012; 108: 318–327.")
69
Jukema JW, Current Medical Research & Opinion Vol. 28, No. 2, 2012, 203–211,

70
+ CONTROINDICAZIONI ALL’USO Clopidogrel Prasugrel Ticagrelor
Ipersensibilità + Sanguinamento in atto NOAC Pregresso TIA/stroke Pregressa emorragia intracranica Epatopatia severa

71
Come mi comporto nella mia pratica clinica
Clopidogrel Prasugrel Ticagrelor STEMI e PCI primaria + ++ UA/NSTEMI e PCI UA/NSTEMI e strategia conservativa - > 75 anni +(+) Diabetici Pz con TIA/stroke Pz ad aumentato rischio di SAT Insufficienza renale < 60 ml/min
 Diabetici. Pz con TIA/stroke. Pz ad aumentato rischio di SAT. Insufficienza renale < 60 ml/min.")
Presentazioni simili











>")







