Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Clinica Urologica ed Andrologica
SESSUALITA’ E STOMIA Dott. A. Zucchi Clinica Urologica ed Andrologica Università di Perugia

2
La sessualita’ nel paziente stomizzato
La qualita’ di vita nel pz sottoposto a confezionamento di una stomia intestinale si modifica sotto il profilo sociale e psicologico.Si assiste a un cambiamento del proprio ruolo nella famiglia,nelle relazioni con gli amici e non dal ultimo rilevanti sono solo alterazioni della sessualita’ .

3
La sessualita’ nel pz stomizzato
Problematiche sessuali nello stomizzato: Cause organiche Psicologiche Ormonali Coesistenza di tutte le problematiche

4
Vescica 16,000 (10%)
")
5
Pelvic surgery are among the most common causes of organic sexual dysfunction in men and women
Sexual dysfunction is highly prevalent even after multiple technical advances in the field of oncological surgeries in which prevalences varies from 8 to 82% Pathophisiology of sexual dysfunction after pelvic surgery is unique because it can be either vascular or neurogenic factors alone, or a combination of both Zippe C et al. Int J Impot Res 2006;18(1):1-18
:1-18.")
6
ANATOMIA PELVICA

7
CHIRURGIA DEMOLITIVA ADDOMINO PELVICA E DISFUNZIONE ERETTILE
LE ALTERAZIONI DELLA SESSUALITA’ CORRELATE AL DANNO NERVOSO PERIFERICO: ORTO E PARASIMPATICO

9
MECCANISMO DEL DANNO NEUROLOGICO
Insulto meccanico o termico delle strutture nervose, parziale o totale Neuroaprassia: lesione lieve (blocco di conduzione) senza degeneraz. Walleriana (durata: settimane) Assonotmesi: assone e mielina sono interrotti, ma le strutture circostanti (cellule di Schwann, perinervio ed epinervio) rimangono integre. La ricrescita assonale può procedere lungo il tubo endoneurale intatto (durata: mesi) Neurotmesi: completa distruzione del tronco nervoso: impossibilità di ricrescita
 senza degeneraz. Walleriana (durata: settimane) Assonotmesi: assone e mielina sono interrotti, ma le strutture circostanti (cellule di Schwann, perinervio ed epinervio) rimangono integre. La ricrescita assonale può procedere lungo il tubo endoneurale intatto (durata: mesi) Neurotmesi: completa distruzione del tronco nervoso: impossibilità di ricrescita.")
10
Autonomic Innervation to Corpora Cavernosa
Pudendal Nerve Dorsal nerve of penis (autonomic to corpora and sensory to skin). Pelvic Plexus Visceral Branches Bladder, seminal vesicles, prostate, urethra, corpora cavernosa. Muscular Branches Levator ani, coccygeus, striated sphincter.
. Pelvic Plexus. Visceral Branches. Bladder, seminal vesicles, prostate, urethra, corpora cavernosa. Muscular Branches. Levator ani, coccygeus, striated sphincter.")
11
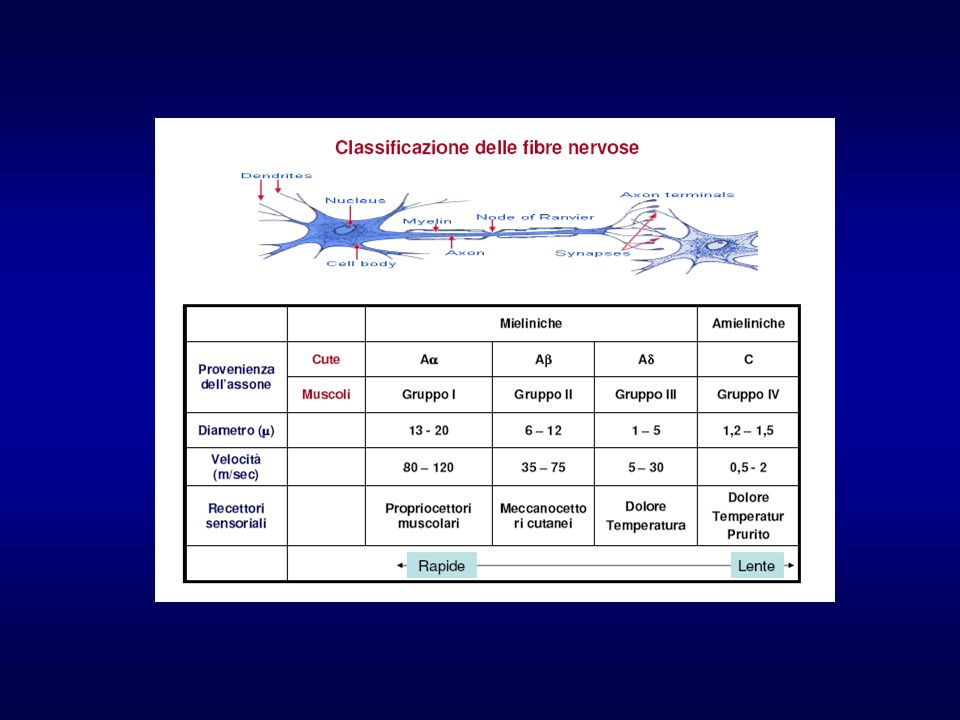
NERVI SOMATICI NERVI CAVERNOSI
Fibre di tipo o gruppo A, sono le tipiche fibre mieliniche dei nervi spinali (velocità di conduzione da 120 a circa 6 m/s, diametro da 20 a 1 µm); NERVI CAVERNOSI Fibre di tipo o gruppo C, fibre amieliniche di piccolo diametro e quindi a bassa velocità di conduzione, che costituiscono la totalità delle fibre postgangliari del sistema nervoso autonomo (velocità di conduzione da 2 a 0,5 m/s, diametro inferiore a 1,2 µm). La delicata struttura di queste fibre spiega: difficoltà di identificazione sensibilità all’insulto meccanico e termico perdita di funzione per periodo lungo
; NERVI CAVERNOSI. Fibre di tipo o gruppo C, fibre amieliniche di piccolo diametro e quindi a bassa velocità di conduzione, che costituiscono la totalità delle fibre postgangliari del sistema nervoso autonomo (velocità di conduzione da 2 a 0,5 m/s, diametro inferiore a 1,2 µm). La delicata struttura di queste fibre spiega: difficoltà di identificazione. sensibilità all’insulto meccanico e termico. perdita di funzione per periodo lungo.")
12
Quando e come si determina il danno neurogeno?
Lesione alta a livello del plesso ipogastrico superiore: PER LEGATURA DELLA ARTERIA MESENTERICA INFERIORE che vascolarizza la parte terminale dell’intestino crasso : ANEIACULAZIONE

13
Quando e come si determina il danno neurogeno?
Lesione del PLESSO PELVICO allorquando si isola il retto dalla parete laterale del piccolo bacino o si esegue la linfoadenectomia Lesione DEI NERVI CAVERNOSI quando si asporta la parte terminale del retto o lo sfintere anale DISFUNZIONE ERETTILE AR (anastomosi bassa) - APR (Miles)
 - APR (Miles)")
14
Alterazioni della sessualita’ nel sesso femminile
Nella donna colostomizzata o ileostomizzata il danno prevalente e’ : la compromissione del processo di lubrificazione Eccitazione ed orgasmo conservati Nelle pz irradiate dopo chirurgia possibile compromissione anche di questi aspetti della sessualita’

15
Exeresi colorettale nelle malattie neoplastiche
Il trattamento standard negli stadi A e B di Dukes (T1->T4, no MTS) è l’exeresi mesorettale totale (TME). Se la lesione è a meno di 3-5 cm dalla linea dentata -> Resezione addominoperineale (APR) o intervento di Miles Nella terapia del cancro del retto hanno un ruolo importante : RDT neo-adiuvante, RDT adiuvante, con effetto negativo sulla funzione sessuale
 è l’exeresi mesorettale totale (TME). Se la lesione è a meno di 3-5 cm dalla linea dentata -> Resezione addominoperineale (APR) o intervento di Miles. Nella terapia del cancro del retto hanno un ruolo importante : RDT neo-adiuvante, RDT adiuvante, con effetto negativo sulla funzione sessuale.")
16
Exeresi colorettale nelle malattie neoplastiche
DE di vario grado riportata nel 10 fino al 60% delle TME NS (risultati oggi migliori con VLS) DE fino al 92% nelle APR Potency rate correla con l’età ma non con lo stadio della malattia Keating JP ANZ J Surg 2004 Apr; 74(4): 189 Danzi M et al. Dis Colon Rectum Oct;26(10):
 DE fino al 92% nelle APR. Potency rate correla con l’età ma non con lo stadio della malattia. Keating JP ANZ J Surg 2004 Apr; 74(4): 189. Danzi M et al. Dis Colon Rectum Oct;26(10):")
17
La sessualita’ nel pz stomizzato

18
Impact of autonomic nerve preservation and lateral node dissection on male urogenital function after total mesorectal excision for lower rectal cancer. Kyo K, Sameshima S, Takahashi M, Furugori T, Sawada T. Department of Surgery, Colorectal Division, Gunma Prefectural Cancer Center, Takabayashi Nishimachi, Ota-shi, Gunma, , Japan. INTRODUCTION: Urogenital dysfunction is a well recognized complication of rectal cancer surgery. The aim of this study was to assess the impact of autonomic nerve preservation (ANP) and lateral node dissection (LND) on male urogenital function after total mesorectal excision for lower rectal cancer. METHODS: We studied, using a questionnaire, preoperative and current urogenital function in 47 male patients who underwent total mesorectal excision with the ANP technique for lower rectal cancer. Patients with and without LND were analyzed separately. RESULTS: A total of 37 patients (78.7%) (22 patients without LND, 15 with LND) returned the questionnaire. Among the 15 patients with LND, 2 underwent unilateral ANP. One patient without LND had urinary dysfunction preoperatively, and among the other 21 patients only 2 (9.5%) reported minor urinary complications postoperatively. After LND, 5 patients (33%) reported minor complications; there were no severe complications. Among patients who were sexually active prior to the operation, 90% and 70% of patients without LND and 50% and 10% of those with LND maintained sexual activity and ejaculation, respectively. However, 50% of patients who underwent low anterior resection or Hartmann resection without LND and all patients with abdominoperineal resection or LND reported reduced overall sexual satisfaction. CONCLUSIONS: The ANP technique offers the great advantage of maintaining urogenital function after rectal cancer surgery. After LND, although the ANP technique minimized urinary dysfunction, sexual function, particularly ejaculation, was often damaged. Careful follow-up is important even after ANP to improve postoperative sexual satisfaction.
 and lateral node dissection (LND) on male urogenital function after total mesorectal excision for lower rectal cancer. METHODS: We studied, using a questionnaire, preoperative and current urogenital function in 47 male patients who underwent total mesorectal excision with the ANP technique for lower rectal cancer. Patients with and without LND were analyzed separately. RESULTS: A total of 37 patients (78.7%) (22 patients without LND, 15 with LND) returned the questionnaire. Among the 15 patients with LND, 2 underwent unilateral ANP. One patient without LND had urinary dysfunction preoperatively, and among the other 21 patients only 2 (9.5%) reported minor urinary complications postoperatively. After LND, 5 patients (33%) reported minor complications; there were no severe complications. Among patients who were sexually active prior to the operation, 90% and 70% of patients without LND and 50% and 10% of those with LND maintained sexual activity and ejaculation, respectively. However, 50% of patients who underwent low anterior resection or Hartmann resection without LND and all patients with abdominoperineal resection or LND reported reduced overall sexual satisfaction. CONCLUSIONS: The ANP technique offers the great advantage of maintaining urogenital function after rectal cancer surgery. After LND, although the ANP technique minimized urinary dysfunction, sexual function, particularly ejaculation, was often damaged. Careful follow-up is important even after ANP to improve postoperative sexual satisfaction.")
19
Sexual function after rectal excision.
ANZ J Surg Apr;74(4):189. Sexual function after rectal excision. Keating JP. Departments of Surgery and Anaesthesia, Wellington School of Medicine and Health Sciences, Wellington, New Zealand. BACKGROUND: Rectal excision is associated with a risk of autonomic nerve damage and associated sexual dysfunction (SD). The evolution of our understanding of the anatomy and physiology of sexual function together with continual refinement of surgery for both benign and malignant disease has led to a decrease in the incidence of SD after rectal surgery. A knowledge of the degree of risk of postoperative SD is important both for the patient and as a benchmark for audit of individual colorectal practice. METHODS: The available literature on the anatomy, physiology and surgical aspects of this topic has been researched through the Medline database. The more recently available data are reviewed in the context of the historical evolution of surgery for benign and malignant rectal disease. RESULTS AND CONCLUSIONS: In the best hands, permanent impotence occurs in less than 2% of patients following restorative proctocolectomy and at a similarly low rate after proctocolectomy and ileostomy. Isolated ejaculatory dysfunction is also numerically a minor problem post operation for benign disease. Patient age is the most important predictor of SD after surgery for rectal cancer. The incidence of permanent impotence remains high (>40%) after abdomino-perineal excision of the rectum (APE) but the continued decline in the use of this operation in favour of low anterior resection (LAR), which carries about half the risk of impotence compared to sphincter ablating surgery, is likely to have resulted in a fall in the absolute number of patients rendered impotent as a result of rectal cancer surgery. Anatomical dissection of the pelvis with preservation of the named autonomic fibres results in a low and predictable rate of sexual morbidity. Surgeons could profitably spend more time with their patients discussing the possible effects of surgery on sexual function. Further research is required to determine the effects of adjuvant therapy for rectal cancer on sexual function.
:189. Sexual function after rectal excision. Keating JP. Departments of Surgery and Anaesthesia, Wellington School of Medicine and Health Sciences, Wellington, New Zealand. BACKGROUND: Rectal excision is associated with a risk of autonomic nerve damage and associated sexual dysfunction (SD). The evolution of our understanding of the anatomy and physiology of sexual function together with continual refinement of surgery for both benign and malignant disease has led to a decrease in the incidence of SD after rectal surgery. A knowledge of the degree of risk of postoperative SD is important both for the patient and as a benchmark for audit of individual colorectal practice. METHODS: The available literature on the anatomy, physiology and surgical aspects of this topic has been researched through the Medline database. The more recently available data are reviewed in the context of the historical evolution of surgery for benign and malignant rectal disease. RESULTS AND CONCLUSIONS: In the best hands, permanent impotence occurs in less than 2% of patients following restorative proctocolectomy and at a similarly low rate after proctocolectomy and ileostomy. Isolated ejaculatory dysfunction is also numerically a minor problem post operation for benign disease. Patient age is the most important predictor of SD after surgery for rectal cancer. The incidence of permanent impotence remains high (>40%) after abdomino-perineal excision of the rectum (APE) but the continued decline in the use of this operation in favour of low anterior resection (LAR), which carries about half the risk of impotence compared to sphincter ablating surgery, is likely to have resulted in a fall in the absolute number of patients rendered impotent as a result of rectal cancer surgery. Anatomical dissection of the pelvis with preservation of the named autonomic fibres results in a low and predictable rate of sexual morbidity. Surgeons could profitably spend more time with their patients discussing the possible effects of surgery on sexual function. Further research is required to determine the effects of adjuvant therapy for rectal cancer on sexual function.")
20
Proctocolectomia nelle malattie infiammatorie
Stahlgren e Ferguson riportano 25% di DE di vario grado nel 1959 Lindsay nel 2001 somministra IIEF in 156 pz con FU medio di 74 mesi: solo 6 (3,8%) con DE grave tutti > 50y 21 pz (13,5%) di DE lieve Nessun disturbo dell’eiaculazione Lindsay I et al. Dis. Clon Rectum Jun;44(6):831-35
 con DE grave tutti > 50y. 21 pz (13,5%) di DE lieve. Nessun disturbo dell’eiaculazione. Lindsay I et al. Dis. Clon Rectum Jun;44(6):")
21
Impotence after mesorectal and close rectal dissection for inflammatory bowel disease.
Lindsey I, George BD, Kettlewell MG, Mortensen NJ. Department of Colorectal Surgery, John Radcliffe Hospital, Oxford, United Kingdom. PURPOSE: Close rectal dissection is a surgical technique used by some surgeons in inflammatory bowel disease. It is performed within the mesorectum, close to the rectal muscle wall, with the aim of minimizing damage to the pelvic sexual nerves. Other surgeons dissect in the more anatomical mesorectal plane. Our aim was to determine whether close rectal dissection is more protective of the pelvic sexual nerves than mesorectal dissection. METHOD: Patients undergoing surgery for inflammatory bowel disease were entered prospectively into a database. Male patients were mailed a standardized, validated, urologic impotence questionnaire: the International Index of Erectile Function. RESULTS: There was an 81 percent response rate. Six of 156 assessable patients were totally impotent (3.8 percent). They were all in the 50-year-old to 70-year-old age group, with no impotence in patients younger than 50 years old. Twenty-one patients complained of minor diminution of erectile function (13.5 percent), where sexual activity was still possible. There was no statistical difference in the rate of complete (2.2 percent vs. 4.5 percent, P = 0.67) or partial (13.5 percent vs percent, P = 0.99) impotence between close rectal and mesorectal dissection (Fisher's exact test). There were no ejaculatory difficulties. The time elapsed since surgery ranged from 2.7 months to months, with a median of 74.5 months. CONCLUSION: Rectal excision for inflammatory bowel disease can be conducted with low rates of impotence. Minor degrees of erectile dysfunction may be more common than currently recognized. We could not demonstrate that close rectal dissection significantly protects the patient from impotence compared with operating in the anatomical mesorectal plane. Age appears to be the most important risk factor for postoperative impotence.
. They were all in the 50-year-old to 70-year-old age group, with no impotence in patients younger than 50 years old. Twenty-one patients complained of minor diminution of erectile function (13.5 percent), where sexual activity was still possible. There was no statistical difference in the rate of complete (2.2 percent vs. 4.5 percent, P = 0.67) or partial (13.5 percent vs percent, P = 0.99) impotence between close rectal and mesorectal dissection (Fisher s exact test). There were no ejaculatory difficulties. The time elapsed since surgery ranged from 2.7 months to months, with a median of 74.5 months. CONCLUSION: Rectal excision for inflammatory bowel disease can be conducted with low rates of impotence. Minor degrees of erectile dysfunction may be more common than currently recognized. We could not demonstrate that close rectal dissection significantly protects the patient from impotence compared with operating in the anatomical mesorectal plane. Age appears to be the most important risk factor for postoperative impotence.")
22
Chirurgia colorettale nelle malattie infiammatorie

23
Prevenzione della disfunzione erettile
PROBABILI “KEY FACTORS” 1 . Bilaterale Nerve Sparing Technique 2. Young patient age 3. Surgeon’s experience (Patient number vs 1001 – 3477) Kundu S.D. et al. J Urol.,172: ,2004
 Kundu S.D. et al. J Urol.,172: ,2004.")
24
Principi generali nella chirurgia “potency sparing”
Valutazione Potency pre-op (e post!): questionari? Età pz Rispetto della sicurezza oncologica Esperienza del chirurgo (eventuale) RDT terapia adiuvante (Riabilitazione post-op)
: questionari Età pz. Rispetto della sicurezza oncologica. Esperienza del chirurgo. (eventuale) RDT terapia adiuvante. (Riabilitazione post-op)")
25
Le soluzioni possibili !
Inibitori delle PDE5 Farmacoterapia intracavernosa MUSE Vacuum device CHIRURGIA PROTESICA

26
La sessualita’ dopo la stomia
Gli aspetti psicologici RUOLO DEL/LA PARTNER IL counselling psicosessuologico

27
Sessualita’ e stomia aspetti psicologici
Il confezionamento di una stomia: modifica la propria immagine corporea Riduce l’autostima e l’autonomia di alcune funzioni Altera le relazioni interpersonali: lavorative,amicizie,affetti Viene compromesso il delicato equilibrio della vita sessuale: Diminuiscono il numero dei rapporti Minore piacere Tendenza ad evitare il contatto fisico per atteggiamenti difensivi di assoluta chiusura,legati ad un’idea di disgusto correlato alla stomia

28
Sessualita’ e stomia aspetti psicologici
Il ruolo del couselling pre e post intervento CHIRURGO, ANDROLOGO PSICOSESSUOLOGO STOMATERAPISTA SVILUPPARE LA RESILIENZA Aiutare il pz ad aprirsi e manifestare i propri sentimenti, il bisogno di aiuto, rassicurazione,di vicinanza fisica, evitando pericolosi atteggiamenti isolamento autoprotettivo sentimentale e sociale.

Presentazioni simili













 abbiamo cominciato a lavorare utilizzando i maniera didattica tecnologie di tipo hardware.>")




>")
