Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Scienze Umane 3 Roberto Iovine Direttore UOC medicina Riabilitativa
AUSL di Bologna Osp. San Giovanni in Persiceto

2
Scienze Umane 3: obiettivi
Lo spirito critico Quando una terapia è “efficace” La “compliance” La “disponibilità” Farsi le domande Il ruolo della probabilità Le banche dati per il medico Cenni di etica della ricerca

3
Programma Il medico è oggetto di propaganda La terapia “efficace”
La compliance: il rifiuto del medico Il consenso realmente informato Il PICO La logica Bayesiana Un trattamento di dimostrata efficacia… Esercitazione sul PICO Le banche dati e l’approccio EBM Il concetto di “evidenza” Note di etica della ricerca (Alltrials) Finale
 Finale.")
4
Le carote…

5
Il quesito La laser fa bene all’artrosi?

6
Il quesito Categorizziamo i 3 termini: 1. Artrosi 2. Laser 1 Paziente
3. Fa bene 1 Paziente 2 Intervento 3 Outcome

7
La domanda in 3 parti P (Paziente) I (Intervento) C (Comparazione)
O (Outcome)
")
8
Esercitazione I vostri PICO

9
Tesi Nella maggior parte dei casi, un trattamento
dimostrato efficace non cambia la prognosi della maggioranza della popolazione cui è prescritto

10
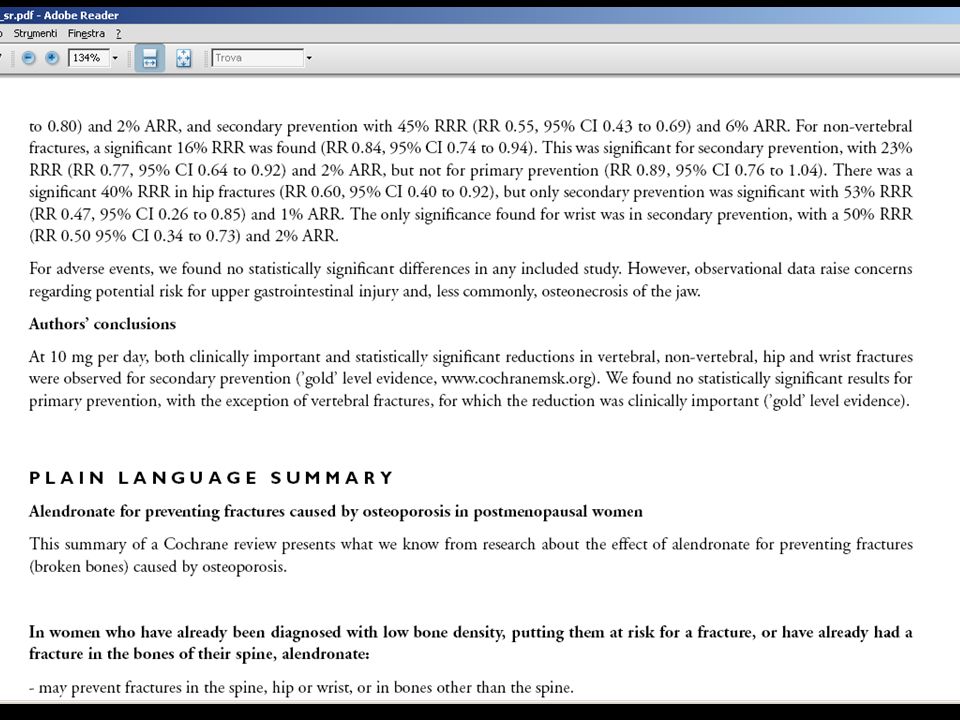
Scenario 1 La Sig.ra B. ha 65 anni , è in menopausa da 9; ha recentemente subito un crollo vertebrale di L3; sua madre non si era mai fratturata; è leggermente sovrappeso, non fuma ed ha fatto recentemente una MOC che ha mostrato un T = -1,5. Viene da voi per sapere se deve iniziare una terapia con alendronato, come hanno fatto alcune sue conoscenti.

11
Scenario 1 La Sig.ra B. ha 65 anni , è in menopausa da 9; ha recentemente subito un crollo vertebrale di L3; sua madre non si era mai fratturata; è leggermente sovrappeso, non fuma ed ha fatto recentemente una MOC che ha mostrato un T = -1,5. Viene da voi per sapere se deve iniziare una terapia con alendronato, come hanno fatto alcune sue conoscenti.

12
Il PICO P In donne in età post menopausale ad alto rischio,
I il trattamento con alendronato, C non trattamento con alendronato O riduce il rischio di rifrattura patologica?

13
La ricerca dell’informazione
Dove cercare l’informazione?

14
Classificazione del quesito
E’ una “domanda in 3 parti” Riguarda l’efficacia di un trattamento Scegliete di consultare per prima …

17
Quindi: Il farmaco è efficace nel ridurre l’incidenza della frattura del terzo prossimale del femore in una popolazione di donne in età menopausale a rischio elevato (già fratturate)
")
18
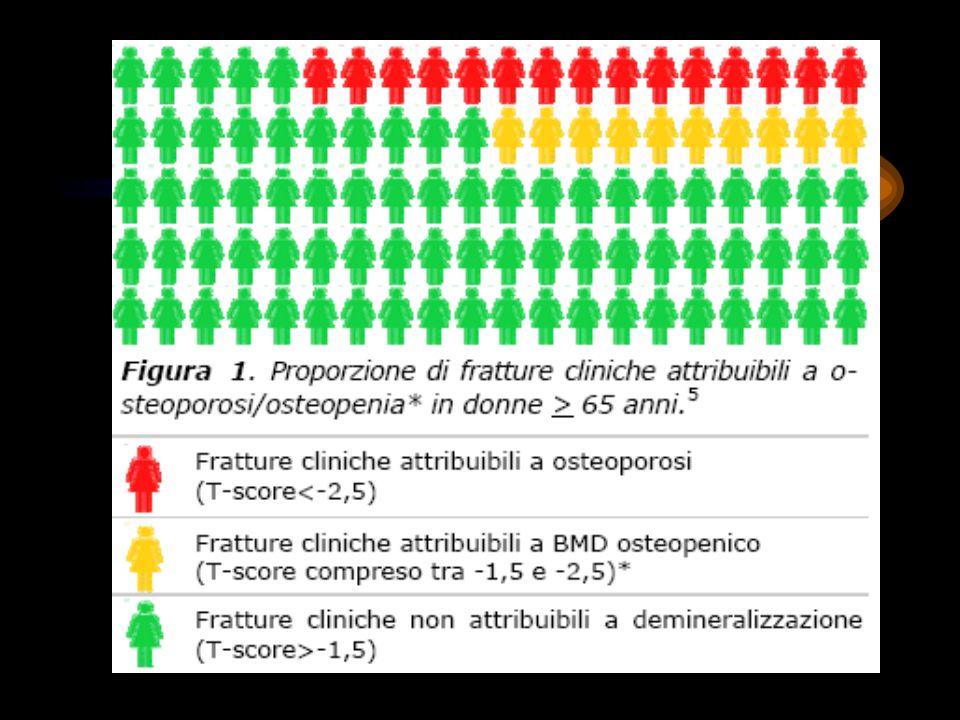
Individualizzazione del rischio
Passare dalla valutazione del rischio in una popolazione alla valutazione del rischio nel nostro singolo paziente. O quanto meno: valutare il rischio in una sottopopolazione più simile alla nostra paziente L’indice di Black (2001)
")
19
1 2 = 3

21
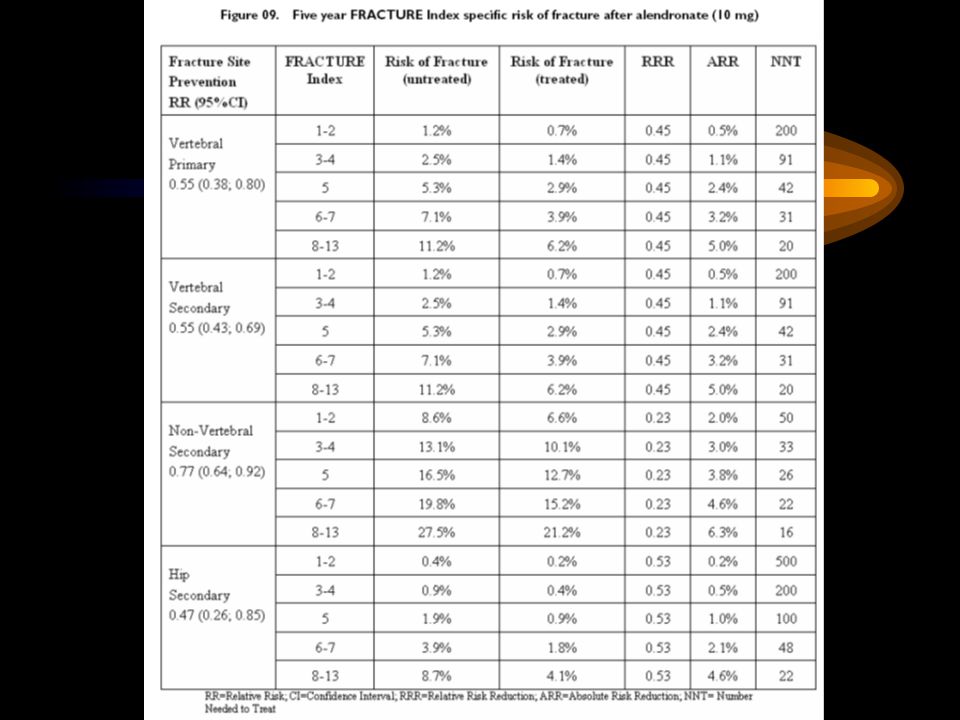
Rischio (non trattate) (trattate) RRR ARR NNT 0,4% 0,2% 0,53 500 0,9% 0,5% 200 1,9% 1,0% 100 3,9% 1,8% 2,1% 48 8,7% 4,1% 4,6% 22 1-2 3-4 5 6-7 8-13

22
Considerazioni Non trattate = 9 fratture su 1000 donne
991 non si fratturano anche se non trattate 4 si fratturano anche se trattate A 995 donne il trattamento non cambia destino 5 su 1000 ne hanno un vantaggio NNT =200

23
Rischio (non trattate) (trattate) RRR ARR NNT 1-2 3-4 5 6-7 8-13 0,4% 0,2% 0,53 500 0,9% 0,5% 200 1,9% 1,0% 100 3,9% 1,8% 2,1% 48 8,7% 4,1% 4,6% 22

24
Considerazioni 2 Non trattate = 8,7 fratture su 100 donne
91,3 non si fratturano anche se non trattate 4,1 si fratturano anche se trattate A 95,4 donne il trattamento non cambia destino 4,6 su 100 ne hanno un vantaggio NNT =22

25
QED Un trattamento dimostrato efficace non cambia la prognosi della
maggioranza della popolazione cui è prescritto

27
“Ma insomma, in definitiva, l’alendronato glielo devo prescrivere o no
Dipende…

28
Dipende…

29
Bilancio costo/beneficio

31
Ma allora… E’ interessante notare… che la EBM viene accusata di volere imbrigliare i medici in schemi di trattamento ferrei ed insindacabili, di avere cooperato alla produzione di linee guida che stringono i professionisti in comportamenti coatti come camicie di forza… da questo esempio scopriamo invece che l’adozione del paradigma ci pone molti più dubbi che certezze, ci obbliga ad usare il nostro giudizio clinico nell’applicare i risultati della ricerca, e ci ricorda che le abilità da coltivare sono anche le nostre capacità comunicative, empatiche, di conoscenza della psicologia dei nostri pazienti, che insomma ci obbliga a fare i medici.

32
Pausa?

33
Scenario 3 La vostra prima idea è di consigliare alla
paziente di provare, “…tanto che male le può fare?” ma temete di fare la figura di un medico superficiale. Prendete tempo anche perché vi ricordate di avere letto su Tempo Medico un articolo favorevole all’agopuntura. Telefonate ad un collega neurologo per avere conferma ma questi vi fa una tirata contro le medicine alternative e vi congeda seccato.

34
Esercitazione Scrivete la domanda secondo il PICO

35
Emicrania ed agopuntura: il quesito
P In pazienti con emicrania I la agopuntura, C verso la non agopuntura O riduce la frequenza e/o l’intensità degli attacchi?

36
Classificazione del quesito
E’ una “domanda in 3 parti” Riguarda l’efficacia di un trattamento Scegliete di consultare per prima …

37
Scenario 5 Vi telefona vostro zio settuagenario perché gli è stato proprio oggi diagnosticato un cancro della prostata. Vi legge il referto specialistico che riporta una diagnosi di “…carcinoma localizzato ben differenziato”. Lo zio nasconde la sua preoccupazione con qualche battuta di spirito ma voi percepite la sua ansia e, poiché sul momento non avete le idee chiare su questa patologia, gli dite che gli telefonerete stasera dopo il lavoro.

38
Classificazione del quesito
E’ una domanda PICO? NO E’ una domanda cui è possibile rispondere? SI Scegliete di consultare per prima … Trip eMedicine Up To Date Clinical Evidence

39
Quesiti Foreground (3-part question)
Background (Who, What, When, Where, Why, …) The five w’s of journalism
 The five w’s of journalism.")
40
PEDro The Physiotherapy Evidence Database
Le fonti Benvenuti nel sito GIMBEâ Realizzato per diffondere in Italia la Evidence-based Medicine Cochrane Library PEDro Riviste secondarie Bandolier TRIP DB di Linee Guida (NGC ecc.) … PEDro The Physiotherapy Evidence Database
 … PEDro The Physiotherapy Evidence Database.")
42
Pausa?

43
La valutazione critica
Quali criteri fanno di un articolo un “buon” articolo?

44
La valutazione critica
Bontà metodologica Rilevanza clinica

45
L’evoluzione dell’informazione in Scienza e Medicina (2) Numero di articoli presenti in Medline. Dal 2000 al 2003 inseriti 2 milioni di articoli

46
Cos’è essenziale? “Molto meno del 5% degli articoli che appaiono nelle attuali riviste di Medicina contiene un messaggio che sia al tempo stesso scientificamente valido e rilevante per i medici” Delamothe T, Smith R: Moving beyond journals: the future arrives with a crash. BMJ, 1999; 318:

47
Piramide della produzione della letteratura medica
Revisioni Sistematiche

48
Gerarchia EBM della consultazione della letteratura medica
Revisioni Sistematiche Cochrane Library DARE

49
Il ricercatore ha scelto il tipo di ‘esposizione’?
No Si Studio sperimentale Studio osservazionale Allocazione casuale ? Gruppo di confronto ? Si No Si No CT non rando-mizzato RCT Studio analitico Stud. descrittivo Direzione ? Esposizione ed esito contemporanei Esposizione ->esito Esito -> esposizione Studio cross-sezionale Studio di coorte Studio caso-controllo

50
Il ricercatore ha scelto il tipo di ‘esposizione’?
No Si Studio sperimentale Studio osservazionale Allocazione casuale ? Gruppo di confronto ? Si No Si No CT non rando-mizzato RCT Studio analitico Stud. descrittivo Direzione ? Esposizione ed esito contemporanei Esposizione ->esito Esito -> esposizione Studio cross-sezionale Studio di coorte Studio caso-controllo

51
The James Lind Library Il trattato sullo scorbuto
L’esperimento di James Lind

53
BACINO DI RECLUTAMENTO
RCT BACINO DI RECLUTAMENTO CAMPIONE RANDOMIZZAZIONE GRUPPO di TRATTAMENTO GRUPPO di CONTROLLO T 0 TEMPO MAX SOMIGLIANZA CONFRONTO ESITI T 1 N° ESITI N° ESITI

54
Randomized Controlled Studies
A randomized controlled study is one in which: There are two groups, one treatment group and one control group. The treatment group receives the treatment under investigation, and the control group receives either no treatment or some standard default treatment. Patients are randomly assigned to all groups. Assigning patients at random reduces the risk of bias and increases the probability that differences between the groups can be attributed to the treatment. Having a control group allows us to compare the treatment with alternative choices. For instance, the statement that a particular medication cures 40% of cases tells us very little unless we also know how many cases get better on their own! (Or with a different treatment). With certain research questions, randomized controlled studies cannot be done for ethical reasons. For instance, it would be unethical to attempt to measure the effect of smoking on health by asking one group to smoke two packs a day and another group to abstain, since the smoking group would be subject to unnecessary harm. Randomized controlled trials are the standard method of answering questions about the effectiveness of different therapies. If you have a therapy question, first look for a randomized controlled trial, and only go on to look for other types of studies if you don't find one.
. With certain research questions, randomized controlled studies cannot be done for ethical reasons. For instance, it would be unethical to attempt to measure the effect of smoking on health by asking one group to smoke two packs a day and another group to abstain, since the smoking group would be subject to unnecessary harm. Randomized controlled trials are the standard method of answering questions about the effectiveness of different therapies. If you have a therapy question, first look for a randomized controlled trial, and only go on to look for other types of studies if you don t find one.")
55
The Double Blind Method
A double blind study is one in which neither the patient nor the physician knows whether the patient is receiving the treatment of interest or the control treatment. For example, studies of treatments that consist essentially of taking pills are very easy to do double blind - the patient takes one of two pills of identical size, shape, and color, and neither the patient nor the physician needs to know which is which. A double blind study is the most rigorous clinical research design because, in addition to the randomization of subjects which reduces the risk of bias, it can eliminate the placebo effect which is a further challenge to the validity of a study. The placebo effect could be thought of in this way: Patients who believe they are receiving a new experimental treatment tend to be more optimistic about the outcome. This means that, when asked, they tend to minimize health problems and give more weight to positive effects. They also tend to take better care of themselves and comply better with the conditions of the experiment. There is also substantial evidence that, independent of all this, patients who have positive beliefs about their treatment do better than patients who do not. In many situations, the placebo effect is at least as strong as any objective effects of the treatment! Doctors who believe that a patient is receiving a new experimental treatment tend to be more optimistic about that patient's chances, evaluate their state of health more favorably, and communicate positive expectations to the patients, who in turn try to get better so as to prove their doctor right!

56
Cohort Studies A Cohort Study is a study in which patients who presently have a certain condition and/or receive a particular treatment are followed over time and compared with another group who are not affected by the condition under investigation. For instance, since a randomized controlled study to test the effect of smoking on health would be unethical, a reasonable alternative would be a study that identifies two groups, a group of people who smoke and a group of people who do not, and follows them forward through time to see what health problems they develop. Cohort studies are not as reliable as randomized controlled studies, since the two groups may differ in ways other than in the variable under study. For example, if the subjects who smoke tend to have less money than the non-smokers, and thus have less access to health care, that would exaggerate the difference between the two groups. The main problem with cohort studies, however, is that they can end up taking a very long time, since the researchers have to wait for the conditions of interest to develop. Physicians are, of course, anxious to have meaningful results as soon as possible, but another disadvantage with long studies is that things tend to change over the course of the study. People die, move away, or develop other conditions, new and promising treatments arise, and so on. Even so, cohort studies are generally preferred to case control studies, since they involve far fewer statistical problems and generally produce more reliable answers.

57
Case Control Studies Case control studies are studies in which patients who already have a certain condition are compared with people who do not. For example: a study on which lung cancer patients are asked how much they smoked in the past and the answers are compared with a sample of the general population would be a case control study. Case control studies are less reliable than either randomized controlled trials or cohort studies. Just because there is a statistical relationship between two conditions does not mean that one condition actually caused the other. For instance, lung cancer rates are higher for people without a college education (who tend to smoke more), but that does not mean that someone can reduce his or her cancer risk just by getting a college education. The main advantages of case control studies are: They can be done quickly. By asking patients about their past history, researchers can quickly discover effects that otherwise would take many years to show themselves. Researchers don't need special methods, control groups, etc. They just take the people who show up at their institution with a particular condition and ask them a few questions. The first study to suggest a new medical conclusion will often be a case control study, perhaps designed to check on a hypothesis suggested by a case series. If possible, researchers will generally try to confirm the results with a randomized controlled trial or a cohort study.
, but that does not mean that someone can reduce his or her cancer risk just by getting a college education. The main advantages of case control studies are: They can be done quickly. By asking patients about their past history, researchers can quickly discover effects that otherwise would take many years to show themselves. Researchers don t need special methods, control groups, etc. They just take the people who show up at their institution with a particular condition and ask them a few questions. The first study to suggest a new medical conclusion will often be a case control study, perhaps designed to check on a hypothesis suggested by a case series. If possible, researchers will generally try to confirm the results with a randomized controlled trial or a cohort study.")
58
Case Series and Case Reports
Case series and case reports consist either of collections of reports on the treatment of individual patients, or of reports on a single patient. For example: one of your patients has a condition that you have never seen or heard of before and you are uncertain what to do. A search for case series or case reports may reveal information that will assist in a diagnosis. However, for any reasonably well-known condition you should be able to get better evidence. Case series and case reports, since they use no control group with which to compare outcomes, have no statistical validity .

59
Systematic Reviews and Meta-Analyses
Important medical questions are typically studied more than once, often by different research teams in different locations. A systematic review is a comprehensive survey of a topic in which all of the primary studies of the highest level of evidence have been systematically identified, appraised and then summarized according to an explicit and reproducible methodology. A meta-analysis is a survey in which the results of all of the included studies are similar enough statistically that the results are combined and analyzed as if it was one study. In general a good systematic review or meta-analysis will be a better guide to practice than an individual article. Pitfalls specific to meta-analysis include: It's rare that the results of the different studies precisely agree, and often the number of patients in a single study is not large enough to come up with a decisive conclusion. If the authors are interested in supporting a particular conclusion, they can include studies that support that conclusion and omit studies that do not. Do the authors explain in their paper exactly on what basis they included studies , and do their reasons make sense? Studies that show some kind of positive effect tend to be published more often than those that do not. This means that if the authors include only published studies, several weak positive studies may seem to add up to a strong positive result. Do weak negative studies exist? This effect is known as Publication bias.

61
Pausa?

62
La Medicina Basata sulle Evidenze
La EBM consiste nel consapevole, esplicito e ragionevole uso delle migliori prove di efficacia esistenti nelle decisioni che riguardano la cura del singolo paziente La EBM consiste nell’integrare l’esperienza clinica con la migliore letteratura scientifica disponibile

63
An Intuitive Explanation of Bayesian Reasoning
La logica Bayesiana 1% of women at age forty who participate in routine screening have breast cancer. 80% of women with breast cancer will get positive mammographies. 9.6% of women without breast cancer will also get positive mammographies. A woman in this age group had a positive mammography in a routine screening. What is the probability that she actually has breast cancer? An Intuitive Explanation of Bayesian Reasoning

64
Lo screening 2 Quali sono sensibilità e specificità del test?
Potrebbe questo essere un buon test di screening della popolazione? (L’incidenza di cancro dell’ovaio è dello 0,04% in donne > 35 anni)
")
65
A proposito di test diagnostici

66
I mattoni della valutazione dell’eticità di uno studio clinico

67
Scaletta 1 – Etica e conoscenza 2 – Etica e metodologia
3 – Etica e trasparenza

68
85% research waste = over 85 bilion $ / year !!!

70
Pubblico o non pubblico? Dipende…
Uno studio pubblicato sul BMJ di ieri: su 585 trial clinici con almeno 500 pazienti arruolati, ben 171 di questi trial, per un totale di quasi pazienti, non risultano pubblicati dopo 60 mesi, e per 133 di essi non sono riportati i risultati neppure su clinicaltrial.gov BMJ 2013;347:f6104

71
Ben Goldacre

72
Svelare il conflitto di interesse: I trial di disseminazione
A seeding trial is marketing in the guise of science. The apparent purpose is to test a hypothesis. The true purpose is to get physicians in the habit of prescribing a new drug. Ann Intern Med. 2008;149(4):
:")
73
Ma gli articoli pubblicati fanno avanzare la Medicina?
Solo il 50% degli articoli genera almeno un citazione, l’altro 50% è totalmente ignorato dai ricercatori Meno del 20% degli articoli sono citati più di 10 volte European Molecular Biology Organization reports 2005; 5:

74
Fare le scale… …fa bene

75
Patient-oriented medicine
La EBM come strumento di una medicina orientata al paziente

76
Etimologia Dottore – s.m. [Dal Lat. Doctor –oris maestro, der. di
docere insegnare] 1. Propr. Chi ammaestra in una dottrina, chi esercita l’ufficio d’insegnare: Poscia ch’io ebbi il mio dottore udito (Dante)… La piccola Treccani, Dizionario enciclopedico, 1995
… La piccola Treccani, Dizionario enciclopedico,")
77
Dover essere sempre all’altezza della perfezione è una delle prime cause dell’infelicità umana.
Michele Serra (La Repubblica )
")
78
Grazie!

Presentazioni simili