Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Francesco Vittorio Costa Università degli Studi di Bologna
Il trattamento dell’Ipertensione nel paziente diabetico Francesco Vittorio Costa Università degli Studi di Bologna

2
Diabete e ipertensione
Diabete+ipertensione: dimensione del problema 2. La terapia antipertensiva produce vantaggi nei diabetici? 3. Quale la PA da raggiungere nei diabetici? 4. Quali antipertensivi utilizzare?

3
Prevalence of Hypertension in Type 2 Diabetes
Normoalbuminuria (n = 323) Microalbuminuria (n = 151) Macroalbuminuria (n = 75) Total (n = 549) 100 93 90 80 71 Prevalence of hypertension (%) 50 Slide 68. Prevalence of Hypertension in Type 2 Diabetes Hypertension is frequently found in patients with diabetes, with a prevalence approximately twice that of the nondiabetic population [Epstein et al, 1992]. The presence of hypertension further increases the already high risk of cardiovascular disease associated with type 2 diabetes [Epstein et al, 1992; The Hypertension in Diabetes Study Group, 1993b]. A study including a cohort of 549 patients with type 2 diabetes (mean age 60 years) demonstrated a high prevalence of hypertension (defined as an average BP 140/90 mm Hg during a 3-year follow-up period). Eighty percent of the patients were classified as hypertensive, ranging from 71% of patients with normal urinary albumin excretion (UAE 30 mg/24 h) to 93% in patients with macroalbuminuria (UAE 300 mg/24 h). Only 41% of the patients were receiving antihypertensive treatment. Two out of 3 untreated hypertensive patients had isolated systolic hypertension. Even in patients receiving antihypertensive therapy, 92% of those with normoalbuminuria, 92% of those with microalbuminuria, and 88% of those with macroalbuminuria remained hypertensive (BP 140/90 mm Hg), with an average BP of 163/90, 165/88, and 161/92 mm Hg in the 3 groups, respectively [Tarnow et al, 1994]. Hypertension defined as BP 140/90 mm Hg. Tarnow L et al. Diabetes Care 1994;17:
 Microalbuminuria (n = 151) Macroalbuminuria (n = 75) Total (n = 549) Prevalence of. hypertension. (%) 50. Slide 68. Prevalence of Hypertension in Type 2 Diabetes. Hypertension is frequently found in patients with diabetes, with a prevalence approximately twice that of the nondiabetic population [Epstein et al, 1992]. The presence of hypertension further increases the already high risk of cardiovascular disease associated with type 2 diabetes [Epstein et al, 1992; The Hypertension in Diabetes Study Group, 1993b]. A study including a cohort of 549 patients with type 2 diabetes (mean age 60 years) demonstrated a high prevalence of hypertension (defined as an average BP 140/90 mm Hg during a 3-year follow-up period). Eighty percent of the patients were classified as hypertensive, ranging from 71% of patients with normal urinary albumin excretion (UAE 30 mg/24 h) to 93% in patients with macroalbuminuria (UAE 300 mg/24 h). Only 41% of the patients were receiving antihypertensive treatment. Two out of 3 untreated hypertensive patients had isolated systolic hypertension. Even in patients receiving antihypertensive therapy, 92% of those with normoalbuminuria, 92% of those with microalbuminuria, and 88% of those with macroalbuminuria remained hypertensive (BP 140/90 mm Hg), with an average BP of 163/90, 165/88, and 161/92 mm Hg in the 3 groups, respectively [Tarnow et al, 1994]. Hypertension defined as BP 140/90 mm Hg. Tarnow L et al. Diabetes Care 1994;17:")
4
L’evidenza: DM + HT è pericolosa

5
Relative Risk of DM + HTN
Diabetes + HTN versus Diabetes • Neuropathy • Nephropathy • Retinopathy • Stroke • CHD . Mortality

6
CV Mortality Risk Doubles with Each 20/10 mm Hg BP Increment
8 7 6 5 4 3 2 1 115/75 135/85 155/95 175/105 SBP/DBP (mm Hg) Lewington S, et al. Lancet. 2002; 60: JNC VII. JAMA
 Lewington S, et al. Lancet. 2002; 60: JNC VII. JAMA")
7
Terapia dell’ipertensione e diabete
2- la terapia antiipertensiva produce vantaggi nei diabetici ? Confronto con placebo

8
* * * * * * * * * * * * Risk reduction in meta-analyses
of placebo RCTs. Diabetic hypertensives Stroke CHF CHD Death Diuretics * * dose * * * * dose * * * * b- * *p<0.05 * Psaty et al JAMA 1997;277:739 BPLT Lancet 2000;356:1955

9
La terapia antipertensiva produce vantaggi nei diabetici
La terapia antipertensiva produce vantaggi nei diabetici ? Confronto con placebo SI La terapia antipertensiva riduce gli eventi in maniera significativa nei pazienti diabetici

10
Risultati ottenuti nel controllo pressorio dei pazienti diabetici
Terapia dell’ipertensione e diabete Risultati ottenuti nel controllo pressorio dei pazienti diabetici

11
Awareness, treatment and control of hypertension according to diabetes status. aP<0.05 vs. nondiabetes mellitus (non- DM), BP<0.05 vs. known-DM. Diabetes Metab J 2014;38:51-57

12
Failure to Intensify Antihypertensive Treatment by Primary Care Providers: A Cohort Study in Adults with Diabetes Mellitus and Hypertension In this highly adherent cohort of adults with diabetes and hypertension, failure to intensify treatment for high blood pressure was a common problem: primary care providers intensified treatment at only 13% of visits where blood pressure was unequivocally elevated. J Gen Intern Med 2008, 23(5):543–50
:543–50.")
13
Terapia dell’ipertensione e diabete
1. Diabete+ipertensione: dangerous duo 2. La terapia antipertensiva produce vantaggi nei diabetici ? 3. Quale la PA da raggiungere nei diabetici? 4. Quali antipertensivi utilizzare?

14
Any diabetes-related endpoint Microvascular complications
UKPDS Event Rates for Select Endpoints With Tight vs Less Tight Blood Pressure Control P=0.005 Tight (n=758) mean achieved BP 144/82 mmHg Less tight (n=390) mean achieved BP 154/87 mmHg Events per 1000 patient yrs P=0.02 P=0.009 P=0.01 UKPDS Event Rates for Select Endpoints With Tight vs Less Tight Blood Pressure Control In the UK Prospective Diabetes Study (UKPDS), a total of 1,148 patients aged with newly diagnosed diabetes were randomized to a tight blood pressure control group [(n=758) goal of <150/85 mmHg] or a less tight control group [(n=390) goal of <180/105 mmHg]. The goal was to assess the impact of levels of blood pressure control on the primary outcomes of any diabetes-related endpoint (myocardial infarction, heart failure, angina, sudden death, stroke, amputation, retinal photocoagulation, renal failure, vitreous hemorrhage), death-related to diabetes, and death from all causes. Secondary analyses were conducted to assess the impact of the two treatment approaches on different types of vascular disease. These included myocardial infarction, stroke, amputation or death from peripheral vascular disease, and microvascular complications. Patients in the tight control group were treated with captopril or atenolol, while the less tight group avoided ACE inhibitors and beta-blockers (for a median follow-up of 8.4 years). Over nine years of follow-up, the mean blood pressure in patients under tight control was 144/82 mmHg and in the less tight group it was 154/87 mmHg (P<0.0001, for both compared to baseline values). Patients assigned to the tight control group had a 24% reduction in risk of developing any diabetes-related endpoint (P=0.005), a 32% reduction in risk of diabetes-related death (P=0.02), a 44% reduction in risk of fatal and non-fatal stroke (P=0.01), and a 37% reduction in risk of microvascular complications (P=0.009), all compared to the group with less tight control. Reference: Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317(7160): Any diabetes-related endpoint Diabetes- related death Stroke Microvascular complications UKPDS Group. BMJ. 1998;317:703–713.
 mean achieved BP 144/82 mmHg. Less tight (n=390) mean achieved BP 154/87 mmHg. Events per 1000 patient yrs. P=0.02. P= P=0.01. UKPDS Event Rates for Select Endpoints With Tight vs Less Tight Blood Pressure Control. In the UK Prospective Diabetes Study (UKPDS), a total of 1,148 patients aged with newly diagnosed diabetes were randomized to a tight blood pressure control group [(n=758) goal of <150/85 mmHg] or a less tight control group [(n=390) goal of <180/105 mmHg]. The goal was to assess the impact of levels of blood pressure control on the primary outcomes of any diabetes-related endpoint (myocardial infarction, heart failure, angina, sudden death, stroke, amputation, retinal photocoagulation, renal failure, vitreous hemorrhage), death-related to diabetes, and death from all causes. Secondary analyses were conducted to assess the impact of the two treatment approaches on different types of vascular disease. These included myocardial infarction, stroke, amputation or death from peripheral vascular disease, and microvascular complications. Patients in the tight control group were treated with captopril or atenolol, while the less tight group avoided ACE inhibitors and beta-blockers (for a median follow-up of 8.4 years). Over nine years of follow-up, the mean blood pressure in patients under tight control was 144/82 mmHg and in the less tight group it was 154/87 mmHg (P<0.0001, for both compared to baseline values). Patients assigned to the tight control group had a 24% reduction in risk of developing any diabetes-related endpoint (P=0.005), a 32% reduction in risk of diabetes-related death (P=0.02), a 44% reduction in risk of fatal and non-fatal stroke (P=0.01), and a 37% reduction in risk of microvascular complications (P=0.009), all compared to the group with less tight control. Reference: Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317(7160): Any diabetes-related endpoint. Diabetes- related death. Stroke. Microvascular complications. UKPDS Group. BMJ. 1998;317:703–713.")
15
HOT Diabetic Subgroup Reduction in Cardiovascular Events
Target diastolic BP (mmHg) Achieved† systolic BP diastolic # of patients with diabetes 90 143.7 85.2 501 85 141.4 83.2 80 139.7 81.1 499 †mean of all blood pressures for all study patients in BP subgroups from 6 months of follow-up to end of study Number of events* per 1000 patient-yrs HOT Diabetic Subgroup Reduction in Cardiovascular Events The Hypertension Optimal Treatment (HOT) Study enrolled 18,790 hypertensive patients at risk for cardiovascular complications to assess the optimal diastolic blood pressure for the prevention of cardiovascular outcomes. The target study diastolic blood pressures were 90 mmHg (n=6,264), 85 mmHg (n=6,264), and 80 mmHg (n=6,262). Felodipine 5 mg daily was given as baseline therapy, with the addition of other agents as needed according to a five-step regimen. In addition, 9,399 patients were assigned 75 mg/day acetylsalicylic acid and 9,391 patients were assigned placebo. In the subgroup of 1,501 patients with diabetes at baseline, tighter control of diastolic blood pressure resulted in fewer cardiovascular events. Among this group, the relative risk for major cardiovascular events was halved for the 80 mmHg group compared to the 90 mmHg group (P=0.005). Reference: Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S, Menard J, Rahn KH, Wedel H, Westerling S. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet. 1998;351(9118): *Includes all myocardial infarction, all strokes, and all other cardiovascular deaths Hansson L, et al. Lancet. 1998;351:1755–1762.
 Achieved† systolic. BP. diastolic. # of patients with diabetes. †mean of all blood pressures for all study patients in BP subgroups from 6 months of follow-up to end of study. Number of events* per 1000 patient-yrs. HOT Diabetic Subgroup Reduction in Cardiovascular Events. The Hypertension Optimal Treatment (HOT) Study enrolled 18,790 hypertensive patients at risk for cardiovascular complications to assess the optimal diastolic blood pressure for the prevention of cardiovascular outcomes. The target study diastolic blood pressures were 90 mmHg (n=6,264), 85 mmHg (n=6,264), and 80 mmHg (n=6,262). Felodipine 5 mg daily was given as baseline therapy, with the addition of other agents as needed according to a five-step regimen. In addition, 9,399 patients were assigned 75 mg/day acetylsalicylic acid and 9,391 patients were assigned placebo. In the subgroup of 1,501 patients with diabetes at baseline, tighter control of diastolic blood pressure resulted in fewer cardiovascular events. Among this group, the relative risk for major cardiovascular events was halved for the 80 mmHg group compared to the 90 mmHg group (P=0.005). Reference: Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S, Menard J, Rahn KH, Wedel H, Westerling S. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet. 1998;351(9118): *Includes all myocardial infarction, all strokes, and all other cardiovascular deaths. Hansson L, et al. Lancet. 1998;351:1755–1762.")
16
Change from baseline (mmHg)
UKPDS Effetto sugli eventi del controllo stretto vs. meno stretto di glicemia e di PA Change from baseline (mmHg) MICRO-HOPE Change in Systolic Blood Pressure A more significant change in blood pressure was noted in the ramipril group compared to the placebo group at 1 month, 2 years and the final visit. The changes in systolic blood pressure for the ramipril and placebo groups were –1.92 mmHg and 0.55 mmHg at the final visit, respectively (P<0.001). The changes in diastolic blood pressure for the ramipril and placebo groups were –3.3 mmHg and –2.3 mmHg at the final visit, respectively (P=0.008). Although the differences between the 2 groups in systolic and diastolic pressure were small, it is possible that some of the beneficial effect of ramipril on cardiovascular and renal event rates may have been due to blood pressure reduction rather than to a unique effect of ACE inhibition. Reference: Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet. 2000;355(9200): † UKPDS Group. BMJ. 1998;317:703–713.
 MICRO-HOPE Change in Systolic Blood Pressure. A more significant change in blood pressure was noted in the ramipril group compared to the placebo group at 1 month, 2 years and the final visit. The changes in systolic blood pressure for the ramipril and placebo groups were –1.92 mmHg and 0.55 mmHg at the final visit, respectively (P<0.001). The changes in diastolic blood pressure for the ramipril and placebo groups were –3.3 mmHg and –2.3 mmHg at the final visit, respectively (P=0.008). Although the differences between the 2 groups in systolic and diastolic pressure were small, it is possible that some of the beneficial effect of ramipril on cardiovascular and renal event rates may have been due to blood pressure reduction rather than to a unique effect of ACE inhibition. Reference: Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet. 2000;355(9200): † UKPDS Group. BMJ. 1998;317:703–713.")
17
UKPDS: NNT per i diversi end-point (controllo PA vs controllo glicemia)
Qualunque complicanza del diabete 9 31 Mortalità correlata al diabete 16 112 Mortalità totale 23 125 IMA 46 ICTUS 169 Complicanze microvascolari 17 42 NNT1 = “ tight blood pressure control” NNT2 = “tight glicemic control” (da Snow et Al, Ann Intern Med 2003)
")
18
The New England Journal of Medicine
Follow-up of Blood-Pressure Lowering and Glucose Control in Type 2 Diabetes (ADVANCE) Hazard Ratios for Events, According to Blood-Pressure–Lowering Study Group The New England Journal of Medicine September 24, 2014.
 Hazard Ratios for Events, According to Blood-Pressure–Lowering Study Group. The New England Journal of Medicine. September 24,")
19
Hazard Ratios for Events, According to Glucose-Control Study Group.
Follow-up of Blood-Pressure Lowering and Glucose Control in Type 2 Diabetes (ADVANCE) Hazard Ratios for Events, According to Glucose-Control Study Group. The New England Journal of Medicine September 24, 2014.
 Hazard Ratios for Events, According to Glucose-Control Study Group. The New England Journal of Medicine. September 24,")
20
Terapia dell’ipertensione e diabete FINO A CHE VALORI SCENDERE?
Ci sono vantaggi addizionali se il trattamento antiipertensivo è più aggressivo? SI A una maggior riduzione pressoria corrisponde una maggior riduzione degli eventi FINO A CHE VALORI SCENDERE?

21
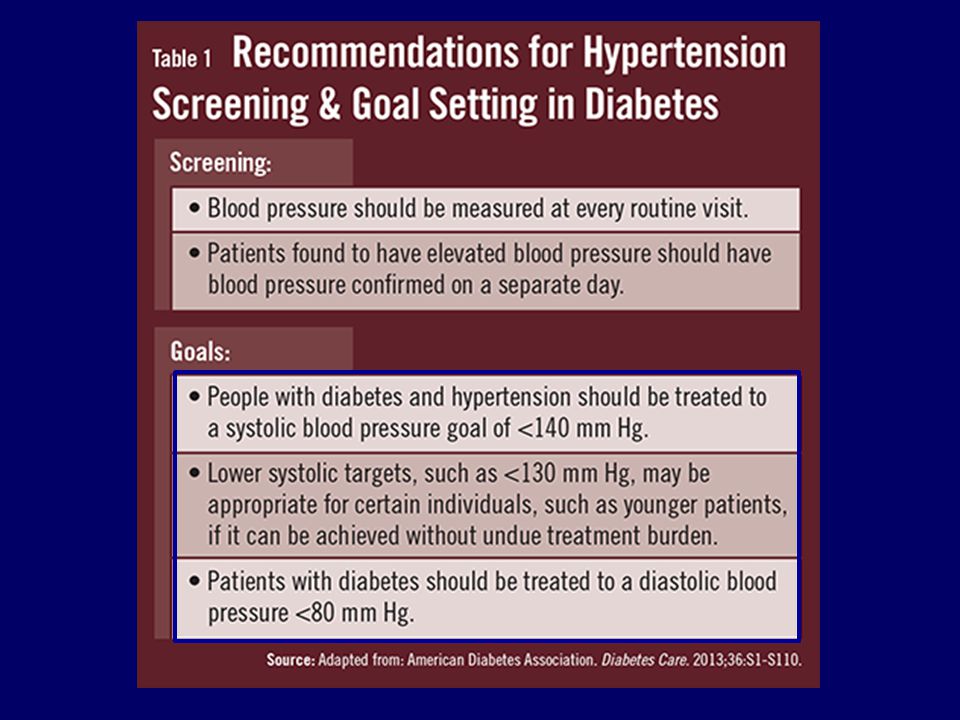
Cosa dicono le Linee guida?

23
Blood Pressure Targets in Subjects With Type 2 Diabetes
Mellitus/Impaired Fasting Glucose Observations From Traditional and Bayesian Random-Effects Meta-Analyses of Randomized Trials “In patients with type 2 diabetes mellitus/impaired fasting glucose/impaired glucose tolerance, a systolic BP treatment goal of 130 to 135 mm Hg is acceptable. However, with more aggressive goals (<130mm Hg), the risk of stroke continued to fall, but there was no benefit on the risk of other macrovascular or microvascular (cardiac, renal and retinal) events, and the risk of serious adverse events even increased. (Circulation. 2011;123: )
, the risk of stroke continued to fall, but there was no benefit on the risk of other macrovascular or microvascular (cardiac, renal and retinal) events, and the risk of serious adverse events even increased. (Circulation. 2011;123: )")
24
C’è un aumento di rischio per pressioni più basse?

25
Subgroup Analyses From the ONTARGET
Safety and Efficacy of Low Blood Pressures Among Patients With Diabetes Subgroup Analyses From the ONTARGET Proportion of Outcome Events by Achieved SBP, Divided Into Deciles JACC Vol. 59, No. 1, 2012

26
Terapia dell’ipertensione e diabete
Diabete+ipertensione: dangerous duo 2. La terapia antipertensiva produce vantaggi nei diabetici ? 3. Quale la PA da raggiungere nei diabetici? 4. Quali antipertensivi utilizzare?

27
Effetti degli antipertensivi sul metabolismo glucidico

28
Incident diabetes in clinical trials of antihypertensive drugs: a network meta-analysis
Lancet 2007; 369: 201–07 22 clinical trials, patients. Initial diuretic used as referent agent. Size of squares (representing the point estimate for each class of antihypertensive drugs) is proportional to number of patients who developed incident diabetes.
 is proportional to number of patients who developed incident diabetes.")
29
Tutti i sartani producono lo stesso effetto sul metabolismo glucidico?

30
Effects of Telmisartan & Losartan in Patients with metabolic syndrome
FPGlucose FPInsulin HOMA IR HbA1c -10 -20 -30 P<0.05 P<0.05 P<0.06 Change from baseline (%) Double-Blind Parallel Group Comparison of 3 Months Therapy with Telmisartan 80mg and Losartan 50mg Daytime ABPM Reductions Telmisartan 13.5 / 8.9 mmHg Losartan 10.0 / 5.6 mmHg Night-time ABPM Reductions Telmisartan 8.7 / 7.8 mmHg Losartan 7.8 / 4.7 mmHg Telmisartan (n=20) Losartan (n=20) P<0.05 Vitale et al. Cardiovasc Diabetol. 2005;15:6.
 Double-Blind Parallel Group Comparison of 3 Months Therapy with Telmisartan 80mg and Losartan 50mg. Daytime ABPM Reductions. Telmisartan 13.5 / 8.9 mmHg. Losartan 10.0 / 5.6 mmHg. Night-time ABPM Reductions. Telmisartan 8.7 / 7.8 mmHg. Losartan 7.8 / 4.7 mmHg. Telmisartan (n=20) Losartan (n=20) P<0.05. Vitale et al. Cardiovasc Diabetol. 2005;15:6.")
31
Effetti di Telmisartan e Eprosartan sui lipidi plasmatici
* * This study was a 1-year comparison of telmisartan 40 mg with eprosartan 600 mg or placebo in 119 patients with type 2 diabetes and mild hypertension.1 Telmisartan significantly reduced trough DBP, but not SBP, compared with eprosartan (p<0.05). Telmisartan also significantly improved cholesterol and lipid profile compared with eprosartan. Derosa G, et al. Effects of telmisartan compared with eprosartan on blood pressure control, glucose metabolism and lipid profile in hypertensive, type 2 diabetic patients: a randomized, double-blind, placebo-controlled 12-month study. Hypertens Res 2004;27:457–464. * * P<0.05 vs Eprosartan Study duration = 1 year Derosa et al. Hypertens Res 2004;27:457–464
. Telmisartan also significantly improved cholesterol and lipid profile compared with eprosartan. Derosa G, et al. Effects of telmisartan compared with eprosartan on blood pressure control, glucose metabolism and lipid profile in hypertensive, type 2 diabetic patients: a randomized, double-blind, placebo-controlled 12-month study. Hypertens Res 2004;27:457–464. * * P<0.05 vs Eprosartan Study duration = 1 year. Derosa et al. Hypertens Res 2004;27:457–464.")
32
Comparative Cardio-Metabolic Studies with Telmisartan
Trial Patients N Duration (weeks) Comparator Agent(s) BP differential Improved Insulin Sensitivity Improved Lipid Profile Anti-oxidant/ Inflammatory Action Derosa 2004a HT, T2DM 119 52 Eprosartan/Placebo No (P yes) No Yes - Derosa 2004b 116 Nifedipine GITS Vitale 2005 HT, MS 40 12 Losartan Yes? Miura 2005 18 Candesartan/Valsartan Koulouris 2005 NT, T2DM Ramipril Honjo 2005 38 Candesartan Benndorf 2006 HT 37 6 Nisoldipine No? Negro 2006a 16 Amlodipine Negro 2006b HT, obese,IR 46 26 Irbesaratn Bahadir 2007 HT, MS 42 10 Derosa 2007 188 Irbesartan Sharma 2007 HT, obese 840 Valsartan HCTZ
 Comparator. Agent(s) BP. differential. Improved. Insulin. Sensitivity. Improved Lipid Profile. Anti-oxidant/ Inflammatory Action. Derosa 2004a. HT, T2DM Eprosartan/Placebo. No (P yes) No. Yes. - Derosa 2004b Nifedipine GITS. Vitale HT, MS Losartan. Yes Miura Candesartan/Valsartan. Koulouris NT, T2DM. Ramipril. Honjo Candesartan. Benndorf HT Nisoldipine. No Negro 2006a. 16. Amlodipine. Negro 2006b. HT, obese,IR Irbesaratn. Bahadir HT, MS Derosa Irbesartan. Sharma HT, obese Valsartan HCTZ.")
33
Protezione dagli eventi
e dal danno d’organo

34
(modificato da Pahor et al. Diabetes Care 2000;23:888)
ACE- I vs altri Farmaci nei pazienti diabetici: effetti su tutti gli eventi cardiovascolari Study (95% CI) OR ABCD 0.57 CAPPP 0.55 0.50 FACET 0.88 STOP2 UKPDS 1.29 z=1.97 p=.05 0.83 (0.69,1.00) .1 .2 1 5 10 Het. p=.0073 (modificato da Pahor et al. Diabetes Care 2000;23:888)
 OR. ABCD CAPPP FACET STOP2. UKPDS z=1.97 p= (0.69,1.00) Het. p= (modificato da Pahor et al. Diabetes Care 2000;23:888)")
35
LIFE: Diabetes – Total Mortality
24 20 16 12 8 4 Atenolol Losartan Proportion of patients, % Adjusted Risk Reduction = 39%; p=0·002 Unadjusted Risk Reduction = 40%; p=0·001 6 12 18 24 30 36 42 48 54 60 66 Study Month LH Lindholm, et al Lancet 2002; 359:

36
Effetti sugli eventi CV maggiori, morti CV e Mortalità Totale in Trial che Confrontano Regimi Basati su Classi Differenti di Antipertensivi in Pazienti con Diabete tipo 2 Comparison Trial SBP/DBP diff. A vs B Major CV events RR (95% CI) CV death RR (95% CI) Total mortality RR (95% CI) N CA vs D/B INSIGHT / ( ) ( ) ( ) NORDIL / ( ) ( ) ( ) STOP / ( ) ( ) ( ) ACEI vs D/B UKPDS / ( ) ( ) ( ) CAPPP 572 0/ ( ) ( ) ( ) STOP / ( ) ( ) ( ) ACEI vs CA ABCD-NT 480 0/ ( ) ( ) ( ) ABCD-HT 470 0/ ( ) ( ) ( ) STOP / ( ) ( ) ( ) AIIA vs D/ LIFE / ( ) ( ) ( ) AIIA vs CA IDNT / ( ) ( ) ( ) 0.1 0.3 0.5 0.7 1.0 2.0 3.0 Favours drug class A Favours drug class B Major CV events CV death Total mortality Zanchetti A et al., J Hypertens 2002
 CV death RR (95% CI) Total mortality RR (95% CI) N. CA vs D/B. INSIGHT / ( ) 0.93 ( ) 0.75 ( ) NORDIL / ( ) 0.24 ( ) 1.15 ( ) STOP / ( ) 0.80 ( ) 0.82 ( ) ACEI vs D/B. UKPDS / ( ) 1.34 ( ) 1.14 ( ) CAPPP 572 0/ ( ) 0.51 ( ) 0.57 ( ) STOP / ( ) 0.93 ( ) 0.90 ( ) ACEI vs CA. ABCD-NT 480 0/ ( ) 1.66 ( ) 0.95 ( ) ABCD-HT 470 0/ ( ) 0.55 ( ) 0.78 ( ) STOP / ( ) 1.16 ( ) 1.10 ( ) AIIA vs D/ LIFE / ( ) 0.63 ( ) 0.61 ( ) AIIA vs CA. IDNT / ( ) 1.36 ( ) 1.05 ( ) Favours drug class A. Favours drug class B. Major CV events. CV death. Total mortality. Zanchetti A et al., J Hypertens")
37
Scegliere un sartano o un ACEI?

38
Confronto efficacia ACE-I vs. sartani

39
Sospensione del trattamento per reazioni avverse : ACEI vs Sartani

40
Corrao G et al J Hypertens. 2008;26(4):819-24.
Interruzioni del trattamento antipertensivo con monoterapia iniziale a 1 anno (Lombardia Data-base: n=445356) Diuretics Beta-blockers Alpha-blockers Calcium channel blockers ACE-inhibitors ARBs 1.83 ( ) 1.64 ( ) 1.23 ( ) 1.08 ( ) 0.92 ( ) 0.5 1.0 2.0 - + I sartani garantiscono i livelli migliori di persistenza Corrao G et al J Hypertens. 2008;26(4):
 Diuretics. Beta-blockers. Alpha-blockers. Calcium channel blockers. ACE-inhibitors. ARBs ( ) 1.64 ( ) 1.23 ( ) 1.08 ( ) 0.92 ( ) I sartani garantiscono i livelli migliori di persistenza. Corrao G et al J Hypertens. 2008;26(4):")
41
Rischio relativo di non-persistenza a seconda del farmaco prescritto inizialmente
+970% Cio’ corrisponde ad un incremento dei costi della terapia di circa il 20%. FV Costa et al, 2009 High Blood Press Cardiovasc Prev 2009; 16 (4): 1-10 NB: ogni 10 paz, che interrompono il sartano ce ne sono 21 che interrompono l’ACEI. Ogni 10 paz che interrompono Sartano+diur ce ne sono 24 che interrompono ACEI+diur
: NB: ogni 10 paz, che interrompono il sartano ce ne sono 21 che interrompono l’ACEI. Ogni 10 paz che interrompono Sartano+diur ce ne sono 24 che interrompono ACEI+diur.")
42
Confronto sartani Ca-antagonisti

43
J Clin Hypertens (Greenwich). 2014:1–8.
Calcium Channel Blocker Compared With Angiotensin Receptor Blocker for Patients With Hypertension: A Meta-Analysis of Randomized Controlled Trials Heart failure P<0.06 J Clin Hypertens (Greenwich). 2014:1–8.
. 2014:1–8.")
44
J Clin Hypertens (Greenwich). 2014:1–8.
Calcium Channel Blocker Compared With Angiotensin Receptor Blocker for Patients With Hypertension: A Meta-Analysis of Randomized Controlled Trials Stroke P<0.04 J Clin Hypertens (Greenwich). 2014:1–8.
. 2014:1–8.")
45
Number of Drugs Needed to Achieve a Goal BP Value in Pts with HBP and Diabetes
1 2 3 5 Drugs (Nr.) LIFE (<90mmHg) MDRD (<92mmHg) HOT (<80mmHg) UKPDS (<85mmHg) IDNT (<85mmHg) RENAAL (<90mmHg) ABCD (<75mmHg) 4 2.7 3.3 3.4 2.8 3.6
 LIFE (<90mmHg) MDRD (<92mmHg) HOT (<80mmHg) UKPDS (<85mmHg) IDNT (<85mmHg) RENAAL (<90mmHg) ABCD (<75mmHg)")
46
Valutare nel tempo l’efficacia della terapia

47
Diabetologia, DOI 10.1007/s00125-014-3330-9 July 2014
Mortality and morbidity in relation to changes in albuminuria, glucose status and systolic blood pressure: an analysisof the ONTARGET and TRANSCEND studies Adjusted HRs according to global effects of albuminuria, glycaemia and BP status. Diabetologia, DOI /s July 2014

48
Conclusions/interpretation
Mortality and morbidity in relation to changes in albuminuria, glucose status and systolic blood pressure: an analysisof the ONTARGET and TRANSCEND studies Conclusions/interpretation Patients who showed improvement to normoalbuminuria over 2 years were at lower risk of all-cause and cardiovascular mortality and of cardiovascular and renal events than those who deteriorated to microalbuminuria over time. Albuminuria over time was significantly better than glucose status and BP control in predicting mortality and both cardiovascular and renal outcomes in patients at a high cardiovascular risk.

49
Reno-protective effects of renin–angiotensin system blockade in type 2 diabetic patients:
Macroalbuminuria Microalbuminuria Diabetologia (2012) 55:566–578
 55:566–578.")
50
Metanalisi (25425 paz) degli effetti di telmisartan e altri farmaci su proteinuria o albuminuria
 degli effetti di telmisartan e altri farmaci su proteinuria o albuminuria")
51
Take home message 1 La associazione Diabete+ ipertensione è estremamente comune e particolarmente rischiosa Una riduzione pressoria + stretta riduce maggiormente il rischio CV e lo riduce maggiormente rispetto al controllo + stretto della glicemia Le percentuali di diabetici con PA ben controllata sono di gran lunga insufficienti e ciò dipende soprattutto da atteggiamenti terapeutici poco aggressivi L’ottenimento di un buon controllo pressorio richiede quasi sempre terapie di associazione

52
Take Home message 2 ACE-i e ancor più i sartani non producono effetti sfavorevoli sul metabolismo glucidico . Il Temisartan migliora alcuni parametri metabolici glucidici e lipidici ACE-i e sartani sono egualmente efficaci nel prevenire gli eventi ma i sartani garantiscono livelli più elevati di aderenza al trattamento L’indice migliore per valutare l’efficacia del trattamento in termini di prevenzione degli eventi, è l’andamento della albuminuria Telmisartan migliora l’albuminuria più degli altri sartani, più degli ACE-i e delle altre classi di farmaci

54
Journal of Hypertension 2013, 31:1281–1357

59
Cosa dicono le Linee Guida?

Presentazioni simili













 N. Pazienti in Dialisi (2002: 308.910)>")

e mostra un ritmo irregolare che varia continuamente nella forma. La frequenza ventricolare media.>")






