Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
L’importanza della diagnostica molecolare nella
L’importanza della diagnostica molecolare nella immunoterapia allergene specifica Salvatore Tripodi UOC Pediatria & Servizio Allergologia Pediatrica Ospedale Sandro Pertini Roma

2
Produttore di allergene Fonte allergenica Molecola allergenica Der p 1 Ghiandole salivari e cutanee Fel d 1 Ghiandole salivari e cute Can f 1

3
Componenti Allergeniche specifiche e cross-reattive
specifici allergeni cross-reattivi Componenti Allergeniche specifiche e cross-reattive sensibilizzanti primari panallergeni

4
Una sola fonte, ma molte componenti
Allergene KD Der p 1 cysteine protease 25 Der p 2 14 Der p 3 trypsin 28/30 Der p 4 amylase 60 Der p 5 14 Der p 6 chymotrypsin 25 Der p 7 22/28 Der p 8 glutathione transferase Der p 9 collagenolytic serine pro. Dermatophagoides pteronyssinus European house dust mite Der p 1 antigen P1, cysteine protease 25 C 62, see list of isoallergens Der p 2 14 62A-C, see list of isoallergens Der p 3 trypsin 28/30 63 Der p 4 amylase 60 P 64 Der p 5 65 Der p 6 chymotrypsin 66 Der p 7 22/28 67 Der p 8 glutathione transferase 67A Der p 9 collagenolytic serine pro. 67B Der p 10 tropomyosin 36 Y14906 Der p 11 paramyosin 103 AY189697, 67C Der p 14 apolipophorin like prot. Epton p.c. Der p 20 arginine kinase 40* Thomas p.c. Der p 10 tropomyosin 36 Der p 11 paramyosin 103 Der p 14 apolipophorin like prot. Der p 20 arginine kinase 40*

5
Phl p 1 Phl p 2 Phl p 3 Phl p 4 Phl p 5 Phl p 6 Phl p 7 Phl p 11
mix Phleum pratense pollen grains pp Phl p 1 Phl p 1 Phl p 2 Phl p 3 Phl p 4 Phl p 5 Phl p 6 Phl p 7 Phl p 11 Phl p 12 Polcalcina Profilina

6
IgE-Ab at molecular level
Conventional Diagnosis based upon allergenic extracts anamnesis physical examination tentative diagnosis 1 2 conventional allergy test (SPT, IgE-Ab) IgE-Ab at molecular level 3 CRD = The third diagnostic step
 IgE-Ab at molecular level. 3. CRD = The third. diagnostic step.")
7
Schema delle molecole allergeniche primarie e cross-reattive
Bianchi A, et Al. RIAP 1/2011

8
FATTORI DA CONSIDERARE PER LA PRESCRIZIONE DELL’ITS
1. Meccanismo IgE accertato (skin test/RAST) 2. Chiara relazione causale tra esposizione all’allergene e sintomatologia 3. Esclusione di altri fattori scatenanti 4. Gravità dei sintomi (inclusi effetti su attività lavorativa o scolastica) 5. Risposta alla farmacoterapia 6. Disponibilità di estratto standardizzato di cui sia stata dimostrata efficacia. 7. Assenza di controindicazioni (trattamento con beta- bloccanti, malattie immunologiche sistemiche, asma grave, accertata mancanza di compliance) 8. Costi WHO, 1998, ARIA, 2008 © 2012 PROGETTO LIBRA • • 73
 2. Chiara relazione causale tra esposizione all’allergene. e sintomatologia. 3. Esclusione di altri fattori scatenanti. 4. Gravità dei sintomi (inclusi effetti su attività lavorativa. o scolastica) 5. Risposta alla farmacoterapia. 6. Disponibilità di estratto standardizzato di cui sia stata. dimostrata efficacia. 7. Assenza di controindicazioni (trattamento con beta- bloccanti, malattie immunologiche sistemiche, asma. grave, accertata mancanza di compliance) 8. Costi. WHO, 1998, ARIA, © 2012 PROGETTO LIBRA • • 73.")
9
ITS NEI POLISENSIBILI: il punto di vista americano
Allergen immunotherapy: A practice parameter second update Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. J Allergy Clin Immunol Sep;120(3 Suppl):S25-85. Once the relevant allergens for each patient are identified, it is necessary to prepare a mixture that contains each of these allergens. Standardized extracts should be used, when available, and can be mixed with nonstandardized extracts. da E.Ridolo, modificata
:S Once the relevant allergens for each patient are identified, it is necessary to prepare a mixture that contains each of these allergens. Standardized extracts should be used, when available, and can be mixed with nonstandardized extracts. da E.Ridolo, modificata.")
10
ITS NEI POLISENSIBILI: il punto di vista inglese
BSACI guidelines for the management of allergic and non-allergic rhinitis. Scadding GK et al; British Society for Allergy and Clinical Immunology. Clin Exp Allergy Jan;38(1):19-42. da E.Ridolo, modificata
: da E.Ridolo, modificata.")
11
Standards for practical allergen-specific immunotherapy
ITS NEI POLISENSIBILI: il punto di vista europeo Standards for practical allergen-specific immunotherapy Alvarez-Cuesta E, Bousquet J, Canonica GW, Durham SR, Malling HJ, Valovirta E EAACI, Immunotherapy Task Force. Allergy. 2006;61 Suppl 82:1-20 Patients with multiple allergic sensitivity may be effectively treated with several individual allergen products according to their individual sensitivities. In general this approach is limited to two or at most three allergens, which should be injected at 30-min intervals. da E.Ridolo, modificata

12
Diagnostica molecolare e immunoterapia specifica
Utile Inutile Inevitabile

13
Diagnostica molecolare e immunoterapia specifica
Utile Inutile (salvo eccezioni) Inevitabile
 Inevitabile.")
14
Diagnostica molecolare e immunoterapia specifica:
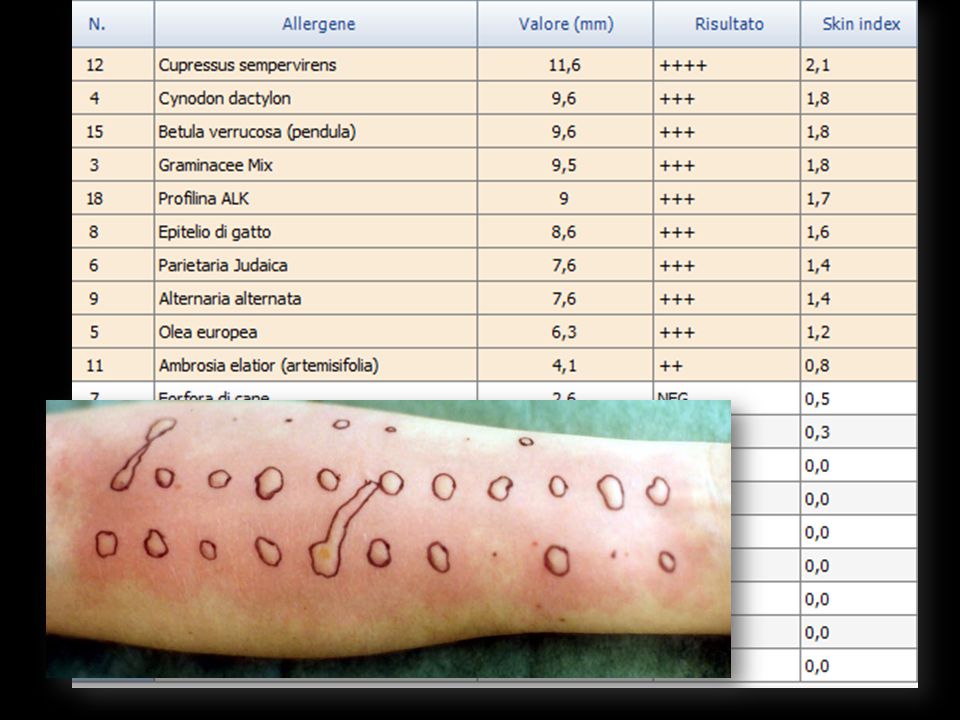
Inutile (salvo eccezioni) Francesco, 9 aa RCA persistente moderata severa dall’età di 8 anni Periodo: Maggio-Giugno
 Francesco, 9 aa. RCA persistente moderata severa dall’età di 8 anni. Periodo: Maggio-Giugno.")
15
Valenta R. The future of antigen-specific immunotherapy of allergy.
Nat Rev Immunol. 2002;2:

16
Appropriatezza Prescrittiva ITS Impatto sull’efficacia
retrospettivo e analisi soggettiva di dati personali Studiati 746 pazienti trattati con la SCIT per graminacee e valutata l’efficacia della ITS rispetto alla presenza o meno di IgE per gli allergeni Maggiori e/o minori Component-resolved diagnosis of allergies allows disease-specific patterns of sensitization in some conditions such as allergic bronchopulmonary aspergillosis ABPA). By determination of IgE against important pollen allergens such as Bet v 1, Ole e 1 or Phl p1/Phl p 5, more precise guidance for allergen-specific immunotherapy may be achieved, as pollen extracts contain mostly these major allergens. Sensitizations against minor allergens such as profilins or polcalcins influence the outcome of IgE measurements against full allergen sources, but are often of limited clinical relevance. In food allergy, frequent cross reactivity between pollens such as birch pollen via Bet v 1/PR10 proteins can be identified. Sensitization against some storage proteins such as peanut (Ara h 2) or lipid transfer proteins of peach (Pru p 3) or hazelnut (Cor a 8) may indicate an increased risk of severe anaphylactic reactions. Exercise-induced anaphylaxis, unclear sensitizations against latex or double-positivity in insect allergy are other useful indications for component-resolved diagnosis. Microarray-based allergen chip diagnosis makes possible today the detection of IgE against more than 100 allergens in tiny amounts of serum and is very promising, but still needs evaluation and optimization in regard to allergen selection and sensitivity.
. By determination of IgE against important pollen allergens such as Bet v 1, Ole e 1 or Phl p1/Phl p 5, more precise guidance for allergen-specific immunotherapy may be achieved, as pollen extracts contain mostly these major allergens. Sensitizations against minor allergens such as profilins or polcalcins influence the outcome of IgE measurements against full allergen sources, but are often of limited clinical relevance. In food allergy, frequent cross reactivity between pollens such as birch pollen via Bet v 1/PR10 proteins can be identified. Sensitization against some storage proteins such as peanut (Ara h 2) or lipid transfer proteins of peach (Pru p 3) or hazelnut (Cor a 8) may indicate an increased risk of severe anaphylactic reactions. Exercise-induced anaphylaxis, unclear sensitizations against latex or double-positivity in insect allergy are other useful indications for component-resolved diagnosis. Microarray-based allergen chip diagnosis makes possible today the detection of IgE against more than 100 allergens in tiny amounts of serum and is very promising, but still needs evaluation and optimization in regard to allergen selection and sensitivity.")
17
n. IgE specifiche per: Efficacia SCIT P. Schmid-Grendelmeier. Hautarzt 2010 · 61:946–953

18
(studio pilota Laziale)
PANALLERGENS IN PAEDIATRICS (studio pilota Laziale) J Allergy Clin Immunol. 2011 Dec 30. [Epub ahead of print]
 J Allergy Clin Immunol Dec 30. [Epub ahead of print]")
19
G G G G G G Are patients „allergic to grass pollens“ all the same
from an immunological point-of-view? G G G G G G i.e. is one grass pollen preparation good for everybody? cortesia P. Matricardi

20
Molecular weight (kD)° Biological Function^ Phl p 1 33-36 Expansin
Allergenic molecules of Phleum pratense most frequently used in diagnostic tests Structure* Molecular weight (kD)° Biological Function^ IgE positivity among Europeans sensitized to grass pollen (%) ^ Phl p 1 33-36 Expansin Phl p 4 55-60 Berberine Bridge Enzyme Phl p 5 29-38 Ribonuclease Phl p 2 11-12 Unknown Phl p 6 13 Phl p 11 20 Trypsin inhibitor Phl p 12 14 Profilin ,2 Phl p 7 6 Calcium binding protein 5 - 8 cortesia P. Matricardi * (June 2012) °Andersson K, Lidholm J . IAAI 2003 ^ (June 2012)
° Biological Function^ IgE positivity among Europeans sensitized to grass pollen (%) ^ Phl p Expansin Phl p Berberine Bridge Enzyme Phl p Ribonuclease Phl p Unknown Phl p Phl p Trypsin inhibitor Phl p Profilin ,2. Phl p Calcium binding protein cortesia P. Matricardi. * (June 2012) °Andersson K, Lidholm J . IAAI ^ (June 2012)")
21
175 pazienti IgEs per Phleum ben 39 profili diversi
di IgE specifiche (≥ 0,35 kU/L) per le 8 molecole del Phleum: Phl p 1 Phl p 2 Phl p 4 Phl p 5 Phl p 6 Phl p7 Phl p 11 Phl p 12 15 profili Tripodi S et Al, JACI 2011
 per le 8 molecole del Phleum: Phl p 1. Phl p 2. Phl p 4. Phl p 5. Phl p 6. Phl p7. Phl p 11. Phl p profili. Tripodi S et Al, JACI")
22
È efficace l’AIT? 175 pazienti IgEs per Phleum ben 39 profili diversi
di IgE specifiche (≥ 0,35 kU/L) per le 8 molecole del Phleum: 11/175 (6,3%) Phl p 1 e Phl p 5= assenti È efficace l’AIT? Tripodi S et Al, JACI 2011
 per le 8 molecole del Phleum: 11/175 (6,3%) Phl p 1 e Phl p 5= assenti. È efficace l’AIT Tripodi S et Al, JACI")
23
Diagnostica molecolare e immunoterapia specifica
Utile Inutile Inevitabile (ma non sempre sufficiente)
")
25
„Panallergeni in Pediatria“
“RICERCARE INSIEME PER CURARE MEGLIO” Studio multicentrico „Panallergeni in Pediatria“

26
„Panallergens in Pediatrics“ CLINICAL HISTORY IS ESSENTIAL
(PAN-PED) 16 centers in 14 Italian cities Recruitment 1360 children (4-18) with SAR Questionnaire ARIA classification SPT tests (extracts) IgE tests (molecules) Roma Ascolii Piceno Genova Iglesias Milano Parma Bologna Verona Empoli Benevento Napoli Palermo Crotone Figure 1 – Map of Italy showing differences across the country regarding: a) clnical features (left); b) sensitization against major pollens, LTP and profiline (right). AR = allergic rhinitis. OAS = oral allergy syndrome. LTP = lipid transfer protein. DOBBIAMO RAPPRESENTARE GRAFICAMENTE ANCHE I CENTRI? CLINICAL HISTORY IS ESSENTIAL Clinically relevant sensitization: SPT >3 mm & nasal/eye symptoms during local pollen season Dondi A.,Tripodi et Al. PAI (2013)
 16 centers in 14 Italian cities. Recruitment children (4-18) with SAR. Questionnaire. ARIA classification. SPT tests (extracts) IgE tests (molecules) Roma. Ascolii. Piceno. Genova. Iglesias. Milano. Parma. Bologna. Verona. Empoli. Benevento. Napoli. Palermo. Crotone. Figure 1 – Map of Italy showing differences across the country regarding: a) clnical features (left); b) sensitization against major pollens, LTP and profiline (right). AR = allergic rhinitis. OAS = oral allergy syndrome. LTP = lipid transfer protein. DOBBIAMO RAPPRESENTARE GRAFICAMENTE ANCHE I CENTRI CLINICAL HISTORY IS ESSENTIAL. Clinically relevant sensitization: SPT >3 mm & nasal/eye symptoms. during local pollen season. Dondi A.,Tripodi et Al. PAI (2013)")
27
Advanced disease stage

28
Tripodi et Al. PAI (2013)
")
29
Probability of having moderate to severe allergic rhinitis, asthma, polysensitization, and longer extension of symptoms during a year among children with AR, by the duration since onset of their AR Tripodi et Al. PAI (2013)
")
30
The Journal of Allergy and Clinical Immunology - 02 May 2014

31
Changes in decision? guidelines/doctors
Roma Ascolii Piceno Genova Iglesias Milano Parma Bologna Verona Empoli Benevento Napoli Palermo Crotone Impact of CRD on SIT prescription in 651 children with moderate to severe AR how often the information obtained with CRD would modify the decision of SIT prescription or its composition based on SPT only? 1360 children (4-18) with AR Figure 1 – Map of Italy showing differences across the country regarding: a) clnical features (left); b) sensitization against major pollens, LTP and profiline (right). AR = allergic rhinitis. OAS = oral allergy syndrome. LTP = lipid transfer protein. DOBBIAMO RAPPRESENTARE GRAFICAMENTE ANCHE I CENTRI? first Evaluation SPT only then Re-evaluation SPT + CRD 651children with moderate-severe AR Changes in decision? guidelines/doctors Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
 with AR. Figure 1 – Map of Italy showing differences across the country regarding: a) clnical features (left); b) sensitization against major pollens, LTP and profiline (right). AR = allergic rhinitis. OAS = oral allergy syndrome. LTP = lipid transfer protein. DOBBIAMO RAPPRESENTARE GRAFICAMENTE ANCHE I CENTRI first. Evaluation. SPT only. then. Re-evaluation. SPT + CRD. 651children with. moderate-severe AR. Changes in decision guidelines/doctors. Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)")
32
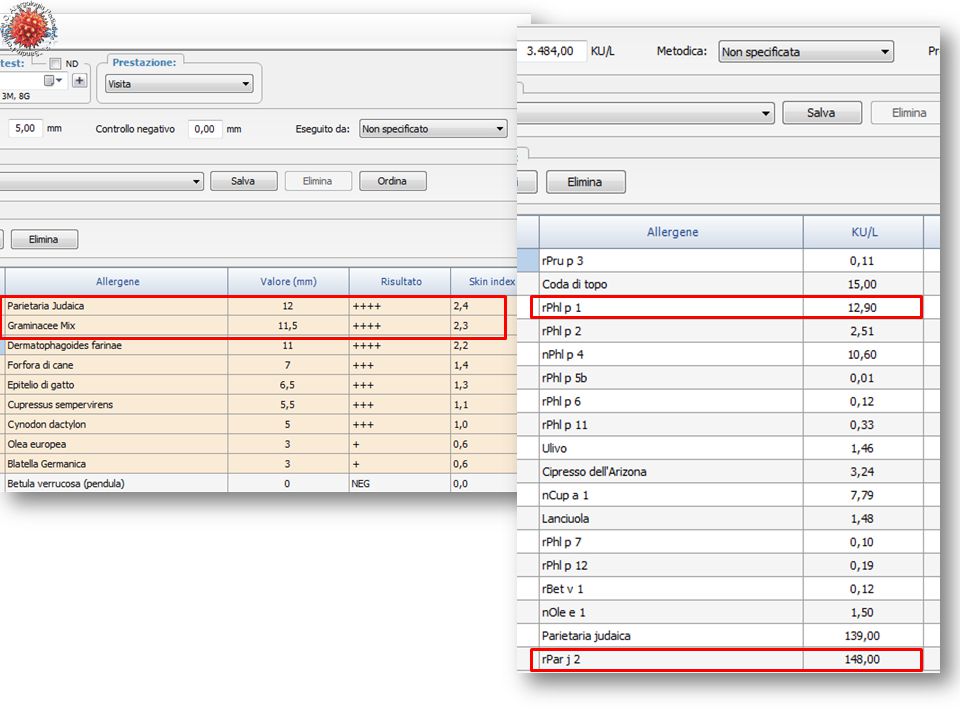
vs CRD positivo cut-off IgEs ≥ 0,7 kU/L
Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
")
33
Based on EAACI-GA2LEN guidelines mismatch SPT+ SIT+ SIT-
Phl p 1, Phl p 5 neg Ole e 1 neg Par j 2 neg Domanda: in che modo la CRD influisce sulla prescrizione della SIT effettuata sulla base di SPT >3 mm e sulla sintomatologia moderata-grave presente durante il periodo dell´anno rilevante per un determinato polline in base al modello teorico per cui venie prescritta immunoterapia al max per 3 allergeni? Risultati: nei pazienti con rinite da moderata a grave viene prescritta SIT soprattutto per graminacee e oleaceae e in minor misura per parietaria, cipresso, betullaceae e artemisia. Dopo l´esecuzione della CRD tale prescrizione non viene confermata nel 10% dei casi per quanto riguarda le graminaceae e il cipresso, nel 30% per parietaria e oleaceae e in misura ancora maggiore per artemisia e betullaceae. Le prescrizioni che non vengono effettuate in accordo con il risultato degli SPT vengono modificate dalla CRD in una percentuale minore di casi per tutte le famiglie allergeniche. Cup a 1 neg Bet v 1 neg Art v 1 neg Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
")
34
n. 1271 Anni 10.4 + 3.4 25% SPT + profilina 23% Phl p 12 +
Asero R., Tripodi S. et Al. Prevalence and clinical relevance of IgE sensitization to profilin in childhood. A multicenter study. (submitted)
")
35
Presenza di IgEs per profilina (Phl p 12) e/o polcalcina (Phl p 7)
vs tale discrepanza è tutta spiegabile con la presenza di IgEs per profillina e/o polcalcina? Presenza di IgEs per profilina (Phl p 12) e/o polcalcina (Phl p 7) nei casi discordanti Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
 e/o polcalcina (Phl p 7) nei casi discordanti. Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)")
36
Changing decision on SIT: in how many patients?
42% patients 19% American European Monoallergen Monoesensitized GUIDELINES Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
")
37
OK, ma i modelli possono alterare la realtà
Come si comportano dei Medici realmente? Decisioni di Medici (n=14) partecipanti allo studio (cluster randomizzazione) (circa 90 pazienti/medico) Prima vs Dopo aver visto i risultati della CRD
 partecipanti allo studio. (cluster randomizzazione) (circa 90 pazienti/medico) Prima vs Dopo aver visto i risultati della CRD.")
38
Storia clinica SPT ITS CRD Modifica ITS ?

39
14 allergists CLINICIANS about 90 patients each Randomly assigned
by climatic area CLINICIANS Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
")
40
Prescrizione ITS prima della CRD
CLINICIANS 14 allergists about 90 patients each Randomly assigned by climatic area Prescrizione ITS prima della CRD

41
+ Modifica della prescrizione della ITS dopo i risultati della CRD
Prescrizione ITS + Modifica della prescrizione della ITS dopo i risultati della CRD

42
Fig 4 – Discordance rate between SIT prescription based on SPT or on SPT and CRD in 651children with AR, according to doctors‘ decision CLINICIANS Doctors have changed their SIT prescription in 47% of the 651patients after IgE molecular tests The number of SIT prescritions increased from 508 to 539 out of 651patients (83 no to yes) (52 yes to no) (170 modified composition) 14 allergists about 90 patients each Randomly assigned by climatic area Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)
 (52 yes to no) (170 modified composition) 14 allergists. about 90 patients each. Randomly assigned. by climatic area. Stringari G, Tripodi S, Caffarelli C. et al. (JACI, 02 May 2014)")
43
Impact of in vitro Molecular Diagnosis on
prescription of specific immunotherapy

44
Diagnostica molecolare e immunoterapia specifica
Utile Inutile Inevitabile (ma non sempre sufficiente)
")
46
@llergymonitor periodo maggio-giugno 2011 (circa 60 gg)
Pazienti gruppo I-PAN (dr.ssa A. Bianchi) Totali pazienti 120 Monit. sufficiente 90 75% Monitor. Insufficiente 2 2% Monitor. tardivo 4 3% No monitoraggio 24 20% Storia clinica SPT CRD ITS @M Modifica ITS ?
 Totali pazienti Monit. sufficiente % Monitor. Insufficiente. 2. 2% Monitor. tardivo. 4. 3% No monitoraggio % Storia clinica. SPT. CRD. Modifica ITS")
47
Modifica della prescrizione della ITS
Prescrizione ITS + Modifica della prescrizione della ITS dopo

49
ITS solo per parietaria
graminacee sintomi sintomi parietaria ITS solo per parietaria

50
Condizione più frequente: “Paziente polisensibile vero”
Esempi di influenza la prescrizione dell’ITS ITS NON prescritta dopo CRD prescritta ITS prescritta dopo CRD Modificata 8% Condizione più frequente: “Paziente polisensibile vero” in cui grazie si sono potuti identificare gli allergeni clinicamente rilevanti da scegliere per un’ITS e controllare in maniera più efficace la sua sintomatologia cortesia di a. bianchi

51
Polisensibilizzazione
Niccolò, 11 anni, RCA primaverile Polisensibilizzazione Olivo, graminacee, parietaria, ma anche cipresso, fagales, artemisia cortesia di a. bianchi

52
Polisensibile vero per Graminacee, olivo, parietaria
ma anche Art v1, Bet v1, Cup a 1 + cortesia di a. bianchi

53
AIT graminacee AIT olivo
RTSS AIT graminacee olivo + parietaria AIT olivo cortesia di a. bianchi

54
cipresso olivo SMS graminacee parietaria

55
Paolo Matricardi, Giovanna Stringari, Arianna Dondi
Carlo Caffarelli, Riccardo Asero, Mario Plebani

56
grazie per l’attenzione

Presentazioni simili


,>")

 devices receive FDA approval annually 3500 medium-risk (class II) products are approved for marketing.>")














