Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Alberto Braghiroli Centro di Medicina del Sonno ad Indirizzo Respiratorio Divisione di Pneumologia Riabilitativa Istituto Scientifico di Veruno - Novara - Italia 1

3
LA PROCEDURA DIAGNOSTICA
Linee Guida di Procedura Diagnostica nella Sindrome delle Apnee Ostruttive nel Sonno dell'Adulto Documento AIMS-AIPO Rass. di Patologia dell’Apparato Respiratorio 2001;16:

6
OSA (grave) sintomatica
3 % OSA (grave) sintomatica 3 % OSA grave asintomatica Inoltre il ragionamento che giustifica una diagnosi precoce sta in piedi se si ammette che ci sia una progressione nella storia naturale della malattia dai casi 23 % ( 15%) OSA lieve moderata Data source: Vitoria Gasteiz study 6 6
 sintomatica. 3 % OSA grave asintomatica. Inoltre il ragionamento che giustifica una diagnosi precoce sta in piedi se si ammette che ci sia una progressione nella storia naturale della malattia dai casi. 23 % ( 15%) OSA lieve moderata. Data source: Vitoria Gasteiz study")
7
Kaplan-Meier estimates of the probability of event-free survival
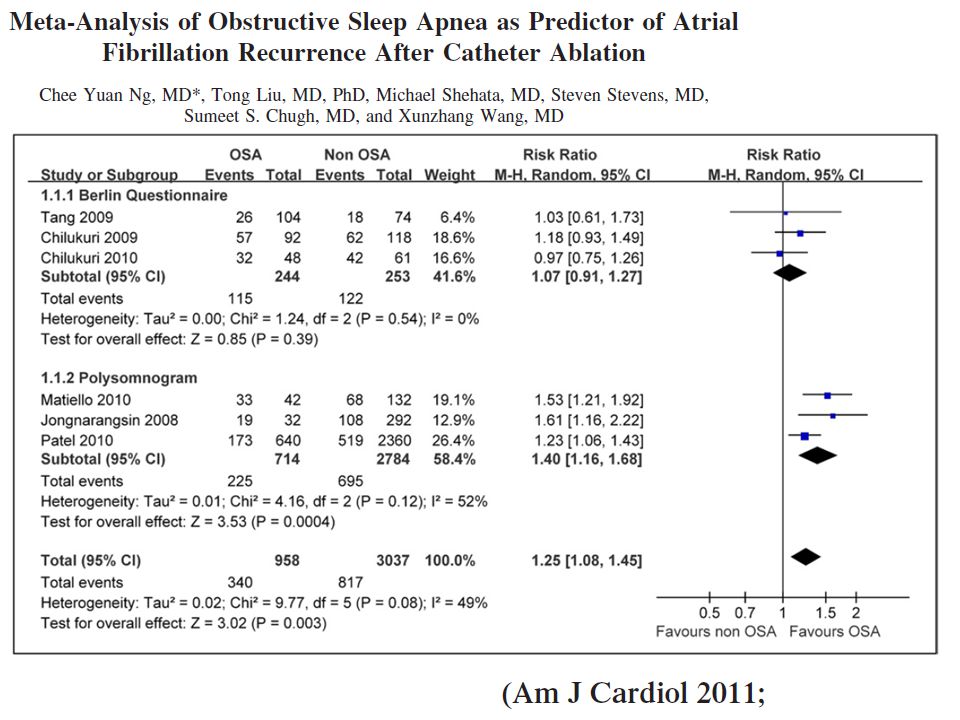
Rationale: Obstructive sleep apnea (OSA) is linked to increased cardiovascular risk, but the impact of mild forms of OSA and their treatment on cardiovascular outcomes remains controversial. Objectives: To prospectively investigate cardiovascular outcomes in treated versus untreated patients with OSA. Methods: Consecutive sleep laboratory patients with all degrees of OSAwere included. Endpointswere nonfatal (myocardial infarction, stroke, and acute coronary syndrome requiring revascularization procedures) and fatal (death from myocardial infarction or stroke) cardiovascular events. Measurements and Main Results: Comparison of event-free survival rates in treated versus untreated patients (Kaplan-Meier estimates, log-rank test).Of 449 patients enrolled (age, years; body mass index, kg/m2), 364 patients received OSA treatment, and 85 patients remained untreated. Median follow-up was 72.0 months (range, 1–156). Mean apnea–hypopnea index before treatment was /hour in treated and /hour in untreated patients, but there were no differences in cardiovascular comorbidities or risk factors. In patients with mild–moderate OSA (n 5 288), events were more frequent in untreated patients (estimated event-free survival at 10 yr, 51.8 vs. 80.3% [P , 0.001]; absolute risk reduction, 28.5%; number needed to treat to prevent one event/10 yr, 3.5). After adjustment for age, gender, cardiovascular risk factors, and comorbidities at baseline, OSA treatment was an independent predictor for events (hazard ratio, 0.36; 95% confidence interval, 0.21–0.62; P , 0.001). Conclusions: OSA treatmentwas associatedwith a cardiovascular risk reduction of 64%independent fromage and preexisting cardiovascular comorbidities. OSA treatment should be considered for primary and secondary cardiovascular prevention, even inmilder OSA. Conclusions This observational study shows benefits of OSA treatment on cardiovascular outcome in mild-moderate OSA. OSA treatment is associated with a marked cardiovascular risk reduction of at least 38%(upper end of 95%CI) independent from age, gender, and preexisting cardiovascular comorbidities. As a component of primary or secondary prevention, OSA therapy should be considered even in mild forms of OSA. In patients with mild–moderate OSA, more events occurred in untreated (25.3% [n 5 20]) than in treated patients (14.4% [n 5 30]; P ). The estimated event-free survival after 10 years was 51.8% in untreated and 80.3% in treated patients (log-rank test, P , 0.001; absolute risk reduction, 28.5%; number needed to treat to prevent one event over 10 yr, 3.5) (Figure 2B). In treated patients who were compliant to CPAP, the estimated event-free survival after 10 years was 83.1% (log- rank test, P , for comparison with untreated patients). The first event tended to occur earlier in untreated than in treated patients (46.3 vs mo), but this difference was statistically not significant. OSA treatment was associated with a cardiovascular risk reduction of 64% independent from age and preexisting cardiovascular comorbidities. OSA treatment should be considered for primary and secondary cardiovascular prevention, even in milder OSA Am J Respir Crit Care Med 176: 1274–1280; 2007 7
 is linked to increased cardiovascular risk, but the impact of mild forms of OSA and their treatment on cardiovascular outcomes remains controversial. Objectives: To prospectively investigate cardiovascular outcomes in treated versus untreated patients with OSA. Methods: Consecutive sleep laboratory patients with all degrees of OSAwere included. Endpointswere nonfatal (myocardial infarction, stroke, and acute coronary syndrome requiring revascularization procedures) and fatal (death from myocardial infarction or stroke) cardiovascular events. Measurements and Main Results: Comparison of event-free survival rates in treated versus untreated patients (Kaplan-Meier estimates, log-rank test).Of 449 patients enrolled (age, years; body mass index, kg/m2), 364 patients received OSA treatment, and 85 patients remained untreated. Median follow-up was 72.0 months (range, 1–156). Mean apnea–hypopnea index before treatment was /hour in treated and /hour in untreated patients, but there were no differences in cardiovascular comorbidities or risk factors. In patients with mild–moderate OSA (n 5 288), events were more frequent in untreated patients (estimated event-free survival at 10 yr, 51.8 vs. 80.3% [P , 0.001]; absolute risk reduction, 28.5%; number needed to treat to prevent one event/10 yr, 3.5). After adjustment for age, gender, cardiovascular risk factors, and comorbidities at baseline, OSA treatment was an independent predictor for events (hazard ratio, 0.36; 95% confidence interval, 0.21–0.62; P , 0.001). Conclusions: OSA treatmentwas associatedwith a cardiovascular risk reduction of 64%independent fromage and preexisting cardiovascular comorbidities. OSA treatment should be considered for primary and secondary cardiovascular prevention, even inmilder OSA. Conclusions. This observational study shows benefits of OSA treatment on cardiovascular outcome in mild-moderate OSA. OSA treatment is associated with a marked cardiovascular risk reduction of at least 38%(upper end of 95%CI) independent from age, gender, and preexisting cardiovascular comorbidities. As a component of primary or secondary prevention, OSA therapy should be considered even in mild forms of OSA. In patients with mild–moderate OSA, more events occurred in untreated (25.3% [n 5 20]) than in treated patients (14.4% [n 5 30]; P ). The estimated event-free survival after 10 years was 51.8% in untreated and 80.3% in treated patients (log-rank test, P , 0.001; absolute risk reduction, 28.5%; number needed to treat to prevent one event over 10 yr, 3.5) (Figure 2B). In treated patients who were compliant to CPAP, the estimated event-free survival after 10 years was 83.1% (log- rank test, P , for comparison with untreated patients). The first event tended to occur earlier in untreated than in treated patients (46.3 vs mo), but this difference was statistically not significant. OSA treatment was associated with a cardiovascular risk reduction of 64% independent from age and preexisting cardiovascular comorbidities. OSA treatment should be considered for primary and secondary cardiovascular prevention, even in milder OSA. Am J Respir Crit Care Med 176: 1274–1280;")
11
BERLIN QUESTIONNAIRE: ITALIAN TRANSLATION
6. Qualcuno ha mai notato che lei smette di respirare durante il sonno? quasi quotidianamente 3-4 volte a settimana 1-2 volte la settimana 1-2 volte al mese mai o quasi mai 7. Quante volte si sente stanco o affaticato dopo aver dormito 8. Durante la giornata, si sente stanco, affaticato o non in forma? 9. Le è mai capitato di avere un colpo di sonno o di essersi addormentato alla guida di un veicolo? Sì No Se sì, quante volte le succede? 10. Soffre di pressione alta? non so Medicina del sonno in Medicina Generale Valutazione del sonno Cognome, Nome Data Altezza (m) Peso (kg) Età Maschio Circonferenza del collo (cm) Femmina 1. Il suo peso si è modificato negli ultimi 5 anni? aumentato diminuito invariato 2. Russa? Sì No non so 3. Il suo russamento è poco più forte del respiro forte come quando parla un po’ più forte di quando parla molto forte. Si può sentire dalla camera a fianco 4. Quante volte russa? quasi quotidianamente 3-4 volte a settimana 1-2 volte la settimana 1-2 volte al mese mai o quasi mai 5. Il suo russare ha mai dato fastidio ad altre persone? No Categoria 1 Categoria 2
 Peso (kg) Età Maschio. Circonferenza del collo (cm) Femmina. 1. Il suo peso si è modificato negli ultimi 5 anni aumentato. diminuito. invariato. 2. Russa Sì. No non so. 3. Il suo russamento è. poco più forte del respiro. forte come quando parla. un po’ più forte di quando parla. molto forte. Si può sentire dalla camera a fianco. 4. Quante volte russa quasi quotidianamente. 3-4 volte a settimana. 1-2 volte la settimana. 1-2 volte al mese. mai o quasi mai. 5. Il suo russare ha mai dato fastidio ad altre persone No. Categoria 1. Categoria 2.")
12
Risultato: se il punteggio
totalizzato è superiore a: 7 in modalità autosomministrata 10 se eterosomministrata ciò è indicativo di una sonnolenza diurna eccessiva

13
OSA e medicina generale
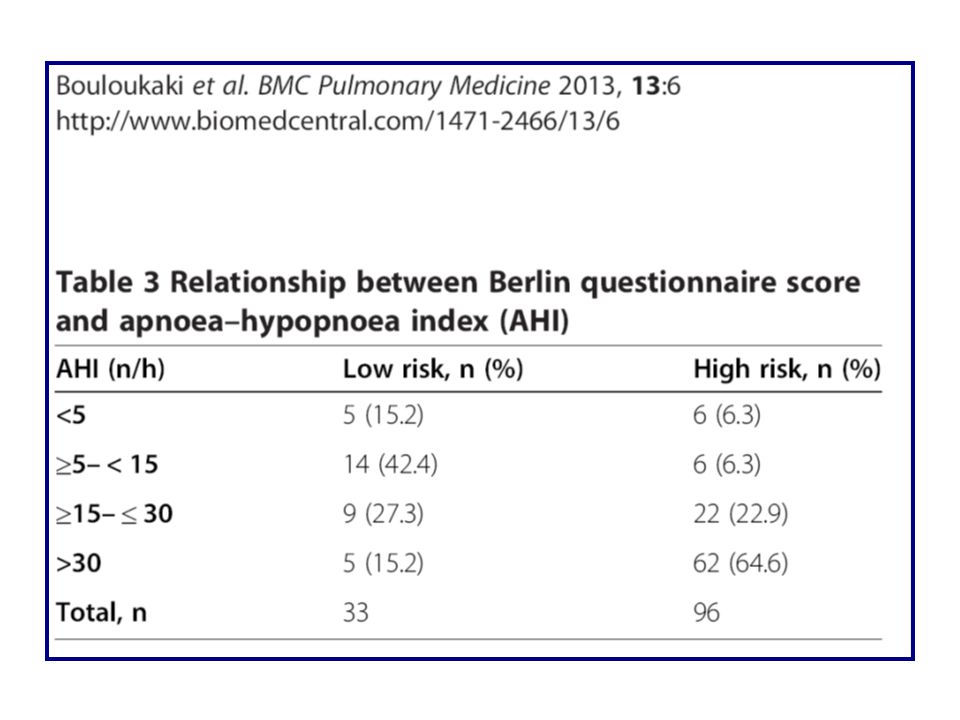
Un semplice questionario che permette di individuare con alta probabilità la presenza di apnee nel sonno è stato somministrato ai pazienti consecutivi che si recavano nell’ambulatorio del proprio medico di famiglia. In totale sono stati forniti questionari, il 78% dei quali compilati e restituiti, con i risultati seguenti

14
RISK FACTORS AND FUNCTIONAL SLEEPINESS (Netzer - AJRCCM 2003)
")
15
Casistica: 549 OSA vs 549 controlli
Otake et al. Cardiovascular medication use in patients with undiagnosed obstructive sleep apnoea. Thorax 2002; 57: Casistica: 549 OSA vs 549 controlli OSA 3.3 volte più prescrizioni di farmaci cardiovascolari dei controlli OSA dosi giornaliere più dei controlli 36.6% OSA vs 19.7% controlli in trattamento antiipertensivo Trattamento antiipertensivo OR: 2.71 OSA

20
Questionnaires n = 5439 PSG n = 930 PSG+STOP BANG n = 746

24
N = 1,058,710

25
CHEST 2013;144:903-14

26
CHEST 2013;144:903-14

27
CHEST 2013;144:903-14

28
Circulation. 2004;110:

29
JACC 2007; 49:565-71

31
Pacing Clin. Electrophysiol. 32, 1434–1443 (2009).
.")
32
Coumel’s Triangle Trigger AF Sympathetic activity Substrate

33
58% sinus node disease (AHI 19±23)
Garrigue S et al. High prevalence of sleep apnea syndrome in patients with long-term pacing: the European Multicenter Polysomnographic Study. Circulation Apr 3;115(13): 50% CHF (AHI 11±7) 68% A-V block (AHI 24±29) 58% sinus node disease (AHI 19±23) CONCLUSIONS: In paced patients, there is an excessively high prevalence of undiagnosed SAS (59%). Whether treating SAS would have changed the need for pacing is unknown. Treatment effects should be further evaluated particularly because these patients are less symptomatic than typical SAS patients. In any case, SAS should be systematically searched for in paced patients owing to potential detrimental effects on their cardiovascular evolution.
: % CHF (AHI 11±7) 68% A-V block (AHI 24±29) 58% sinus node disease (AHI 19±23) CONCLUSIONS: In paced patients, there is an excessively high prevalence of undiagnosed SAS (59%). Whether treating SAS would have changed the need for pacing is unknown. Treatment effects should be further evaluated particularly because these patients are less symptomatic than typical SAS patients. In any case, SAS should be systematically searched for in paced patients owing to potential detrimental effects on their cardiovascular evolution.")
37
37

38
In che modo il dispositivo registra le apnee notturne?
Utilizzando il sensore di Ventilazione Minuto, ovvero tramite la misura dell’impedenza transtoracica rilevata tra il catetere atriale e la cassa del dispositivo.

39
Monitoraggio della respirazione del paziente…
…e delle pause respiratorie Il Monitoraggio delle Apnee Notturne (SAM, Sleep Apnea Monitoring) mediante il senosre MV è disponibile nel Relpy200 SR e DR
 mediante il senosre MV è disponibile nel Relpy200 SR e DR.")
40
In che modo il dispositivo registra le apnee notturne?
Grazie al sensore di Ventilazione Minuto, il pacemaker è in grado di rilevare sia le apnee sia le ipopnee e di calcolare automaticamente l’indice RDI Numero di Pause & Riduzioni Respiratorie Numero di ore di monitoraggio (5h)
")
41
Respiratory Disturbance Index (RDI) automatically calculated by SAM (Sleep Apnea Monitoring) pacemaker algorithm Respiration reduction Pause Apnea Hypopnea Transthoracic impedance Transthoracic Impedance Measurement (Minute Ventilation) Number of Ventilation Pauses & Reductions Number of Hours of Monitoring RDI = 6 months RDI trend RDI severity threshold AF burden
 Number of Ventilation Pauses & Reductions. Number of Hours of Monitoring. RDI = 6 months RDI trend. RDI severity threshold. AF burden.")
42
Apnea / Hypopnea detection PSG recording and PMK transthoracic impedance signal
A: 2 apnea events concurrent reduction of the amplitude of the thoracic impedance signal from the PMK B: 3 hypopnea events simultaneous reduction of the amplitude of the thoracic impedance signal from the PMK Heart Rhythm 2014; 11:

43
Informazioni al follow-up
Soglia di severità per identificare il numero di notti con pause respiratorie ricorrenti Indice RDI per ogni notte Trend in parallelo con il trend della FA

44
Lo studio clinico DREAM
Obiettivo: sensibilità e valore predittivo di SAM Design: 40 pazienti non selezionati Elevato numero di eventi: gli eventi respiratori sono stati confrontati singolarmente tra Reply 200 e polisonnografia The DREAM Clinical Study was held in 2012 and included 6 centers from France and Spain. 40 patients were enrolled, 3 patients withdrew their consents and one had an adverse event during his polysomnography (PSG) examination (*). Altogether 36 patients had complete PSG recordings which were compared to the Minute Ventilation recordings at the same time. Night respiratory events (apneas and hypopneas) were compared individually between Reply 200 and PSG. Preliminary results are positive and may be presented in a subsequent abstract or journal article. Although the primary objective was to compare individual respiratory events between REPLY 200 and PSG, the secondary objectives include the same comparison at the index level, i.e. for patients. Such a comparison is shown on next slide. (*) not related to the Reply 200 or to the pacemaker therapy.
 examination (*). Altogether 36 patients had complete PSG recordings which were compared to the Minute Ventilation recordings at the same time. Night respiratory events (apneas and hypopneas) were compared individually between Reply 200 and PSG. Preliminary results are positive and may be presented in a subsequent abstract or journal article. Although the primary objective was to compare individual respiratory events between REPLY 200 and PSG, the secondary objectives include the same comparison at the index level, i.e. for patients. Such a comparison is shown on next slide. (*) not related to the Reply 200 or to the pacemaker therapy.")
45
Grado di severità di SAS nella popolazione DREAM (36 pazienti)
The DREAM study enrolled 40 patients. 3 patients later withdrew their consent and did not want to take the polysomnography exam. 1 patient had a heart failure decompensation event during the polysomnography recording, which was invalidated. No a Lieve 8 pazienti Moderata 8 pazienti Severa 20 pazienti

46
Risultati dello studio DREAM
Reply 200 (RDI) Correlazione fra SAM e polisonnografia 70 60 50 40 30 20 10 Note: ogni crocetta corrisponde a un paziente This chart shows preliminary results of the DREAM study. This is not the exact data! RDI = Respiratory Disturbance Index AHI = Apnea Hypopnea Index (Gold Standard) Each patient is represented by a cross on the chart. The horizontal axis corresponds to the value displayed by the polysomnography measurement (or gold standard). The vertical axis corresponds to the value displayed by the pacemaker during the same night. If we use a Severity Threshold to identify patients at risk, we have a good sensitivity and a good positive predictive value: this demonstrate the ability to screen severe SAS patients with Reply 200. Definition of screening: the examination of a group of usually asymptomatic individuals to detect those with a high probability of having or developing a given disease. (source: The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company.) Soglia di Severità Polisonnografia (AHI) No a Lieve Moderata Severa Elevata specificità (85%) e sensibilità (89%)
 Correlazione fra SAM e polisonnografia Note: ogni crocetta corrisponde a un paziente. This chart shows preliminary results of the DREAM study. This is not the exact data! RDI = Respiratory Disturbance Index. AHI = Apnea Hypopnea Index (Gold Standard) Each patient is represented by a cross on the chart. The horizontal axis corresponds to the value displayed by the polysomnography measurement (or gold standard). The vertical axis corresponds to the value displayed by the pacemaker during the same night. If we use a Severity Threshold to identify patients at risk, we have a good sensitivity and a good positive predictive value: this demonstrate the ability to screen severe SAS patients with Reply 200. Definition of screening: the examination of a group of usually asymptomatic individuals to detect those with a high probability of having or developing a given disease. (source: The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company.) Soglia di Severità Polisonnografia (AHI) No a Lieve. Moderata. Severa. Elevata specificità (85%) e sensibilità (89%)")
47
Reliability of SA screening tool: the “DREAM” Study Main findings and conclusions
Prevalence of SA in the DREAM study unselected pacemaker population (evaluated by PSG-AHI) 78% moderate to severe SA 56% severe SA An optimal cut-off of 20 events/hour for SAM-RDI value was validated to identify severe SA with 88.9% Sensitivity – 88.9% PPV 84.6% Specificity The DREAM study showed that a transthoracic impedance sensor with an advanced algorithm (SAM) could be used to identify severe SA in PMK patients
 78% moderate to severe SA. 56% severe SA. An optimal cut-off of 20 events/hour for SAM-RDI value was validated to identify severe SA with. 88.9% Sensitivity – 88.9% PPV. 84.6% Specificity. The DREAM study showed that a transthoracic impedance sensor with an advanced algorithm (SAM) could be used to identify severe SA in PMK patients.")
48
Feasibility of a new model to manage Paced Patients with Sleep Apnea
Al fine di valutare quanto l’indicazione data da un sistema d’impianto fosse utile nell’identificare nell’identificare i soggetti affetti da SAS, il policlinico san donato ha recentemnte pubblicato uno studio clinico pilota monocentrico

49
Feasibility of a new model to manage Paced Patients with Sleep Apnea
Flowchart of patient management to determine the PPV of pacemaker-derived index Primary Endpoint: To determine the PPV of the pacemaker-derived index (minute ventilation sensor on-board) vs Sleep-Lab Polygraphy (PG) outcomes to screen and diagnose paced patients (pts) at risk for sleep apnea. Studied population: n = 61 consecutive pts with dual chamber PM (Talent 3DR, Ela Medical/Sorin Group) Age: ± 10.9 years (50% M) PM indications: 51% SND/BTS, 41% BAV, 8% others FU time: 4.64 ±1.78 years FU visits: n = 609 Lo studio ha valutato un flowchart clinico di gestione (screening e diagnosi di SAS) in un gruppo di n=61 pazienti portatori di PM bicamerale (Talent 3 DR) dotato di sensore ventilazione minuto (VM) per rilevare cicli respiratori anomali. Gli indici SA dati dal PM erano incrociati, quando positivi, con l’esito di un’indagine PGF. Con soglia diagnostica per SAS basata sulla presenza di un indice AHI>30 come rilevato dal PM. This single-centre prospective study has been entirely conducted at the IRCCS Policlinico San Donato. A total of 61 consecutive patients (pts) were included in the database. All pts had received a Talent 3 DR PM implant and were being routinely followed-up at our institution. At the time of enrolment, none of the pts was known for a history of sleep breathing disorders or under treatment with continuous positive airway pressure (CPAP) therapy. The diagnostic feature to detect apnoea/hypopnoea events (based on data from the ventilation sensor) was activated in all devices to compute standard AHI from the information gathered over a programmable seven-hour ‘‘sleep-window’’ within the latest 24 hours, and also to record the total number of apnoea and hypopnoea events over the entire period between two consecutive FU visits. The database comprised 609 FU visits from 61 pts (June 2003 to December 2009), accounting for a mean of 4.64 ± 1.78 years FU time (median 5.06 years; minimum 1 day, maximum years). The average time between FU visits was days. The PM implant indications were: atrio-ventricular block 25/61 (41%), sinus node disease 31/61 (51%), others 5/61 (8%). Patients were aged years at implant time (min 41 years, max 94 years) and 50% were men. At the time of implant, none of the patients had a history of sleep breathing disorders or was under treatment with CPAP. The value of the body mass index (BMI), available for only n = 22 pts (36%), was equal to Kg/m About signs/symptoms of heart failure, none of the included patients was classified into NYHA functional class III or IV, typical finding in the real-world unselected dual-chamber PM recipients (normal or mildly reduced left ventricular ejection fraction). Aimè E & al. – Heart, Lung & Circulation 2014
 vs Sleep-Lab Polygraphy (PG) outcomes to screen and diagnose paced patients (pts) at risk for sleep apnea. Studied population: n = 61 consecutive pts with dual chamber PM (Talent 3DR, Ela Medical/Sorin Group) Age: 71.4 ± 10.9 years (50% M) PM indications: 51% SND/BTS, 41% BAV, 8% others. FU time: 4.64 ±1.78 years. FU visits: n = 609. Lo studio ha valutato un flowchart clinico di gestione (screening e diagnosi di SAS) in un gruppo di n=61 pazienti. portatori di PM bicamerale (Talent 3 DR) dotato di sensore ventilazione minuto (VM) per rilevare cicli. respiratori anomali. Gli indici SA dati dal PM erano incrociati, quando positivi, con l’esito di un’indagine. PGF. Con soglia diagnostica per SAS basata sulla presenza di un indice AHI>30 come. rilevato dal PM. This single-centre prospective study has been entirely conducted at the IRCCS Policlinico San Donato. A total of 61 consecutive patients (pts) were included in the database. All pts had received a Talent 3 DR PM implant and were being routinely followed-up at our institution. At the time of enrolment, none of the pts was known for a history of sleep breathing disorders or under treatment with continuous positive airway pressure (CPAP) therapy. The diagnostic feature to detect apnoea/hypopnoea events (based on data from the ventilation sensor) was activated in all devices to compute standard AHI from the information gathered over a programmable seven-hour ‘‘sleep-window’’ within the latest 24 hours, and also to record the total number of apnoea and hypopnoea events over the entire period between two consecutive FU visits. The database comprised 609 FU visits from 61 pts (June 2003 to December 2009), accounting for a mean of 4.64 ± 1.78 years FU time (median 5.06 years; minimum 1 day, maximum years). The average time between FU visits was days. The PM implant indications were: atrio-ventricular block 25/61 (41%), sinus node disease 31/61 (51%), others 5/61 (8%). Patients were aged years at implant time (min 41 years, max 94 years) and 50% were men. At the time of implant, none of the patients had a history of sleep breathing disorders or was under treatment with CPAP. The value of the body mass index (BMI), available for only n = 22 pts (36%), was equal to Kg/m About signs/symptoms of heart failure, none of the included patients was classified into NYHA functional class III or IV, typical finding in the real-world unselected dual-chamber PM recipients (normal or mildly reduced left ventricular ejection fraction). Aimè E & al. – Heart, Lung & Circulation")
50
SA Screening in PMK pts: impact on SA diagnosis & treatment
40/61 positive screening result 65,6 % of tot enrolled patients 61 paced patients SA screening (pacemaker AHI≥30) 26/40 accepted to undergo a PGF examination 42,6 % 22/26 Confirmed positive by PGF 36% 17/22 treated with CPAP 28% Lo studio ha valutato un flowchart clinico di gestione (screening e diagnosi di SAS) in un gruppo di n=61 pazienti portatori di PM bicamerale (Talent 3 DR) dotato di sensore ventilazione minuto (VM) per rilevare cicli respiratori anomali. Gli indici SA dati dal PM erano incrociati, quando positivi, con l’esito di un’indagine PGF. Con soglia diagnostica per SAS basata sulla presenza di un indice AHI>30 come rilevato dal PM. This single-centre prospective study has been entirely conducted at the IRCCS Policlinico San Donato. A total of 61 consecutive patients (pts) were included in the database. All pts had received a Talent 3 DR PM implant and were being routinely followed-up at our institution. At the time of enrolment, none of the pts was known for a history of sleep breathing disorders or under treatment with continuous positive airway pressure (CPAP) therapy. The diagnostic feature to detect apnoea/hypopnoea events (based on data from the ventilation sensor) was activated in all devices to compute standard AHI from the information gathered over a programmable seven-hour ‘‘sleep-window’’ within the latest 24 hours, and also to record the total number of apnoea and hypopnoea events over the entire period between two consecutive FU visits. The database comprised 609 FU visits from 61 pts (June 2003 to December 2009), accounting for a mean of 4.64 ± 1.78 years FU time (median 5.06 years; minimum 1 day, maximum years). The average time between FU visits was days. The PM implant indications were: atrio-ventricular block 25/61 (41%), sinus node disease 31/61 (51%), others 5/61 (8%). Patients were aged years at implant time (min 41 years, max 94 years) and 50% were men. At the time of implant, none of the patients had a history of sleep breathing disorders or was under treatment with CPAP. The value of the body mass index (BMI), available for only n = 22 pts (36%), was equal to Kg/m About signs/symptoms of heart failure, none of the included patients was classified into NYHA functional class III or IV, typical finding in the real-world unselected dual-chamber PM recipients (normal or mildly reduced left ventricular ejection fraction). Good patient compliance to the proposed model (65% of positive screened patients accepted PGF) High Positive Predictive Value [84,6%] - SA pacemaker index vs PGF 42% of positive screened patients undergo CPAP treatment Aimè E & al. – Heart, Lung & Circulation 2014
 26/40. accepted to undergo a PGF examination. 42,6 % 22/26. Confirmed positive by PGF. 36% 17/22. treated with CPAP. 28% Lo studio ha valutato un flowchart clinico di gestione (screening e diagnosi di SAS) in un gruppo di n=61 pazienti. portatori di PM bicamerale (Talent 3 DR) dotato di sensore ventilazione minuto (VM) per rilevare cicli. respiratori anomali. Gli indici SA dati dal PM erano incrociati, quando positivi, con l’esito di un’indagine. PGF. Con soglia diagnostica per SAS basata sulla presenza di un indice AHI>30 come. rilevato dal PM. This single-centre prospective study has been entirely conducted at the IRCCS Policlinico San Donato. A total of 61 consecutive patients (pts) were included in the database. All pts had received a Talent 3 DR PM implant and were being routinely followed-up at our institution. At the time of enrolment, none of the pts was known for a history of sleep breathing disorders or under treatment with continuous positive airway pressure (CPAP) therapy. The diagnostic feature to detect apnoea/hypopnoea events (based on data from the ventilation sensor) was activated in all devices to compute standard AHI from the information gathered over a programmable seven-hour ‘‘sleep-window’’ within the latest 24 hours, and also to record the total number of apnoea and hypopnoea events over the entire period between two consecutive FU visits. The database comprised 609 FU visits from 61 pts (June 2003 to December 2009), accounting for a mean of 4.64 ± 1.78 years FU time (median 5.06 years; minimum 1 day, maximum years). The average time between FU visits was days. The PM implant indications were: atrio-ventricular block 25/61 (41%), sinus node disease 31/61 (51%), others 5/61 (8%). Patients were aged years at implant time (min 41 years, max 94 years) and 50% were men. At the time of implant, none of the patients had a history of sleep breathing disorders or was under treatment with CPAP. The value of the body mass index (BMI), available for only n = 22 pts (36%), was equal to Kg/m About signs/symptoms of heart failure, none of the included patients was classified into NYHA functional class III or IV, typical finding in the real-world unselected dual-chamber PM recipients (normal or mildly reduced left ventricular ejection fraction). Good patient compliance to the proposed model (65% of positive screened patients accepted PGF) High Positive Predictive Value [84,6%] - SA pacemaker index vs PGF. 42% of positive screened patients undergo CPAP treatment. Aimè E & al. – Heart, Lung & Circulation")
54
Sintomi associati all’OSAS
Notturni Russamento Apnee riferite da partner Choking Eccessivi movimenti Nicturia Diaforesi GER Diurni Sonnolenza Astenia Cefalea mattutina concentrazione libido o impotenza attenzione Depressione Modificazioni personalità destrezza manuale 54

55
Insalaco e Salvaggio – Lung Forum 2015
No Insalaco e Salvaggio – Lung Forum 2015

57
Circulation 2003;107:

58
Figure 2. Adjusted mean hemoglobin A1c (HbA1c) values for
patients with no, mild, moderate and severe obstructive sleep apnea (OSA). Data were adjusted for age, sex, race, body mass index, number of diabetes medications, level of exercise, years of diabetes, and total sleep time on polysomnogram. Bars represent SEM; P , for linear trend.
. Data were adjusted for age, sex, race, body mass. index, number of diabetes medications, level of exercise, years of. diabetes, and total sleep time on polysomnogram. Bars represent. SEM; P , for linear trend.")
59
L’individuazione di pazienti asintomatici in popolazioni con comorbilità passa attraverso il filtro di un’anamnesi strutturata o di sistemi di screening dedicati La diagnostica strumentale a tappeto non rappresenta un modello epidemiologicamente sostenibile

60
Abbiamo bisogno di nuovi paradigmi di gestione
Nuovi mezzi “diagnostici” saranno applicati in popolazioni spesso asintomatiche: non possiamo perdere l’occasione di dimostrare a cardiologi, diabetologi, ecc. che possiamo fare la differenza nella gestione dei pazienti 60

62
Centro di Medicina del Sonno ad Indirizzo Respiratorio Fondazione Salvatore Maugeri, IRCCS, Istituto Scientifico di Veruno, Divisione di Pneumologia 62

Presentazioni simili










>")
e mostra un ritmo irregolare che varia continuamente nella forma. La frequenza ventricolare media.>")











>")


