Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Inquinamento atmosferico e salute dei bambini
Claudia Galassi

2
Inquinamento atmosferico e salute dei bambini
Di cosa parliamo…. Le conoscenze sugli effetti sulla salute dell’inquinamento atmosferico da traffico veicolare Aspetti metodologici Disegno degli studi Esposizione Outcomes

3
Inquinamento atmosferico e salute dei bambini
Di cosa non parliamo…. Effetti di alcune specifiche esposizioni (es. Piombo, Mercurio, inquinanti indoor) Politiche per la salute e sviluppo sostenibile
 Politiche per la salute e sviluppo sostenibile.")
4
From http://www.epa.gov/oar/oaqps/eog/course422/ap3.html

6
Particulate matter - definitions
A complex mixture of airborne solid and liquid particles, including soot, organic material, sulfates, nitrates, other salts, metals, biological materials. PM inhalable particles PM fine particles PM10-PM coarse particles PM ultrafine particles

8
ACUTE health effects (e. g
ACUTE health effects (e.g. asthma attacks, myocardial infarction, acute bronchitis, death..) CHRONIC health effects (e.g. chronic bronchitis, lung cancer, anticipation of death...)
 CHRONIC health effects (e.g. chronic bronchitis, lung cancer, anticipation of death...)")
10
Aspetti metodologici

13
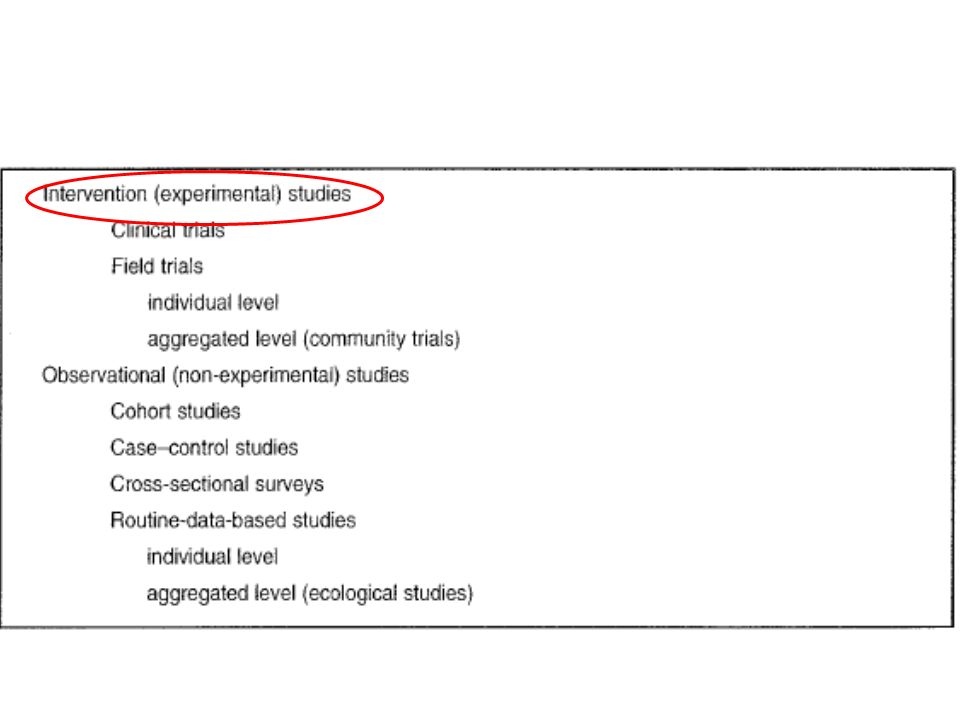
Weaknesses of experimental studies
a small number of, usually healthy, adult volunteer subjects (generalisability of results to the general population may be difficult) “mix” of pollutants difficult to reproduce chronic effects (ex. cancer) cannot be addressed
 mix of pollutants difficult to reproduce. chronic effects (ex. cancer) cannot be addressed.")
14
Types of studies for air pollution
Animal studies Human studies Experimental (chamber studies) Epidemiological (or observational) Cross-sectional Case-control Panel studies Cohort Time series
 Epidemiological (or observational) Cross-sectional. Case-control. Panel studies. Cohort. Time series.")
15
Volume fraction of BrdU-positive AS nuclei in vessels (X10-2 %)
PM and progression of atherosclerosis (rabbits model) Volume fraction of BrdU-positive AS nuclei in vessels (X10-2 %) n=9 n=5 n=9 n=6 Coronary arteries Aorta Suwa et al, 2002
 Volume fraction of BrdU-positive AS nuclei in vessels (X10-2 %) n=9 n=5. n=9 n=6. Coronary arteries. Aorta. Suwa et al,")
16
Ambient Air Pollution and Atherosclerosis in Los Angeles Kunzli et al, EHP 2005 (free access)
carotid intima-media thickness (CIMT), a measure of subclinical atherosclerosis
, a measure of subclinical atherosclerosis.")
17
Exposure Assessment Individual exposure monitoring extremely expensive and complex

18
From: cleanairinitiative
From: cleanairinitiative.org/portal/system/files/presentations/72526_apph.pdf

19
Exposure Assessment Individual exposure monitoring extremely expensive and complex Proxy of exposure (ex. Questionnaires)
 .")
21
Exposure Assessment 2. Generally from fixed site ambient monitors; the best options when large numbers exposed Recent modelling techniques: LUR Models, Dispersion Models, both based on GIS

22
Types of studies for air pollution
Animal studies Human studies Experimental (chamber studies) Epidemiological (or observational) Cross-sectional Case-control Panel studies Cohort Time series
 Epidemiological (or observational) Cross-sectional. Case-control. Panel studies. Cohort. Time series.")
23
Med J Aust Nov 2;169(9): Outdoor air pollution and children's respiratory symptoms in the steel cities of New South Wales. Lewis PR, Hensley MJ, Wlodarczyk J, Toneguzzi RC, Westley-Wise VJ, Dunn T, Calvert D. Open access

24
Objective: To investigate the relationship between outdoor air pollution and the respiratory health of children aged 8 to 10 years Methods: A cross-sectional survey (between October 1993 and December 1993) of children's health and home environment. Summary measures of particulate pollution [PM10] and SO2 were estimated for each area (using air quality monitoring station data from July 1993 to June 1994). Nine areas included.
 of children s health and home environment. Summary measures of particulate pollution [PM10] and SO2 were estimated for each area (using air quality monitoring station data from July 1993 to June 1994). Nine areas included.")
25
Types of studies for air pollution
Animal studies Human studies Experimental (chamber studies) Epidemiological (or observational) Cross-sectional Case-control Panel studies Cohort Time series
 Epidemiological (or observational) Cross-sectional. Case-control. Panel studies. Cohort. Time series.")
26
Types of studies for air pollution
Animal studies Human studies Experimental (chamber studies) Epidemiological (or observational) Cross-sectional Case-control Panel studies Cohort Time series
 Epidemiological (or observational) Cross-sectional. Case-control. Panel studies. Cohort. Time series.")
27
Panel studies Panel of subjects keeping daily diaries (ex. asthma diaries) (‘diary studies’) Exposures measured at the ecological level measured individually Outcomes measured at the individual level (not necessarily with diaries)
")
28
Types of studies for air pollution
Animal studies Human studies Experimental (chamber studies) Epidemiological (or observational) Cross-sectional Case-control Panel studies Cohort Time series
 Epidemiological (or observational) Cross-sectional. Case-control. Panel studies. Cohort. Time series.")
29
Time Series Studies Recently proposed (late 1980s)
Availability of advances in statistical techniques and in computing technology Useful to investigate short term/acute effects of air pollution Outcome and exposure are aggregated over 1 day

30
O3 Mortality November

31
Time series studies Uses routinely collected data for both exposure and outcome Outcomes studied can be: mortality, hospitalisations, emergency department admissions, GP visits Both exposure and outcome measured at the ecological level Confounding: seasonal trends

33
Types of studies for air pollution
Animal studies Human studies Experimental (chamber studies) Epidemiological (or observational) Cross-sectional Case-control Panel studies Cohort Time series
 Epidemiological (or observational) Cross-sectional. Case-control. Panel studies. Cohort. Time series.")
34
Long-term health effects
Chronic exposure studies evaluate health end points across communities or neighborhoods with different levels of average pollution over longer time periods (usually 1 year or more). Pope CA, Environ Health Perspect 108(suppl 4): (2000).
. Pope CA, Environ Health Perspect 108(suppl 4): (2000).")
35
Figure 3. Estimated Adjusted Mortality-Rate Ratios and Pollution Levels in the Six Cities.
Mean values are shown for the measures of air pollution. P denotes Portage, Wisconsin; T Topeka, Kansas; W Watertown, Massachusetts; L St. Louis; H Harriman, Tennessee; and S Steubenville, Ohio.

36
Lung Cancer, Cardiopulmonary Mortality, and Long-term Exposure to Fine Particulate Air Pollution C. Arden Pope III, PhD; Richard T. Burnett, PhD; Michael J. Thun, MD; Eugenia E. Calle, PhD; Daniel Krewski, PhD; Kazuhiko Ito, PhD; George D. Thurston, ScD JAMA. 2002;287:

37
Methods 500,000 subjects, as Part of Cancer Prevention II Study, enrolled in 1982 Study population from 157 cities throughout the USA (157 data points of exposure) Baseline questionnaire collected individual information (age, sex, weight, height, smoking history, etc) Subjects’ risk factors linked to air pollution data and cause of death through to 1998
 Baseline questionnaire collected individual information (age, sex, weight, height, smoking history, etc) Subjects’ risk factors linked to air pollution data and cause of death through to")
38
Birth cohorts

39
Criteria for assessing causality of associations
Strength of association Strong association considered to be more likely causal than weak associations Temporality Exposure precedes effect Specificity A cause is associated with a single effect Biologic gradient An exposure-response relationship is present Plausibility Coherence Experimental evid. The association should be consistent with relevant biologic data Hill (1965), Rothman (1986, 1998).
, Rothman (1986, 1998).")
40
Effetti sulla salute dell’inquinamento atmosferico da traffico nei bambini

41
Effetti studiati: Patologie respiratorie
Infezioni (alte /basse vie respiratorie) Asma (aggravamento/insorgenza) Esiti riproduttivi (nascite pre-termine) Tumori infantili Mortalità neonatale/infantile
 Asma (aggravamento/insorgenza) Esiti riproduttivi (nascite pre-termine) Tumori infantili. Mortalità neonatale/infantile.")
42
Effetti respiratori acuti

45
Association of Low-Level Ozone and Fine Particles With Respiratory Symptoms in Children With Asthma
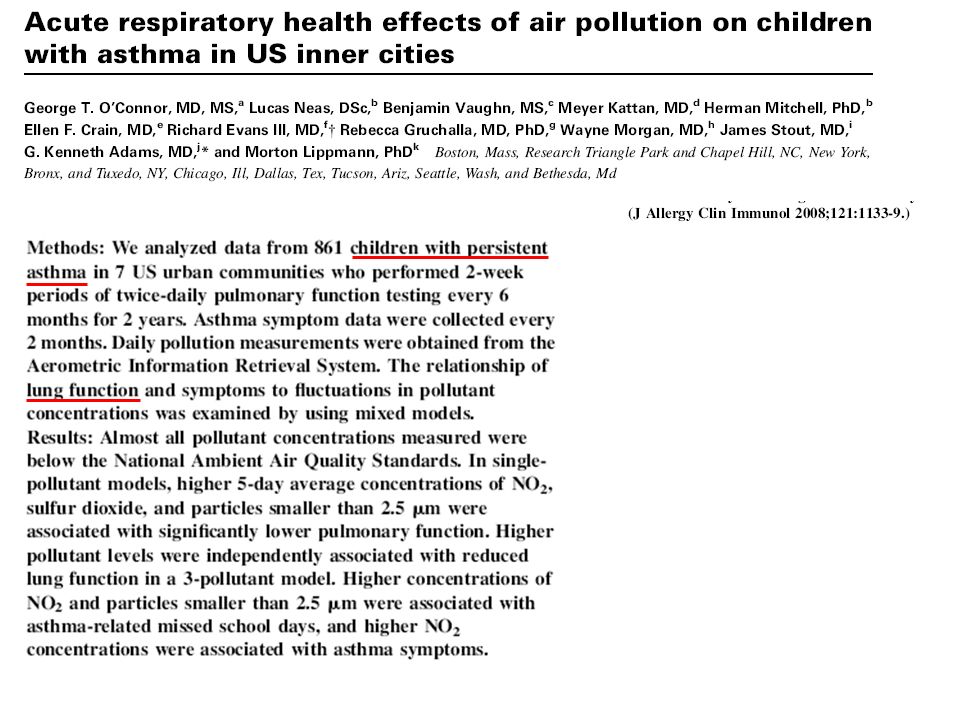
JAMA. 2003;290(14): Design, Setting, and Participants Daily respiratory symptoms and medication use were examined prospectively for 271 children younger than 12 years with physician-diagnosed, active asthma residing in southern New England. Main Outcome Measures Respiratory symptoms and rescue medication use recorded on calendars by subjects' mothers. Results Mean (SD) levels were 59 (19) ppb (1-hour average) and 51 (16) ppb (8-hour average) for ozone and 13 (8) µg/m3 for PM2.5. In copollutant models, ozone level but not PM2.5 was significantly associated with respiratory symptoms and rescue medication use among children using maintenance medication; a 50-ppb increase in 1-hour ozone was associated with increased likelihood of wheeze (by 35%) and chest tightness (by 47%). The highest levels of ozone (1-hour or 8-hour averages) were associated with increased shortness of breath and rescue medication use. No significant, exposure-dependent associations were observed for any outcome by any pollutant among children who did not use maintenance medication. Conclusion Asthmatic children using maintenance medication are particularly vulnerable to ozone, controlling for exposure to fine particles, at levels below EPA standards.
: Design, Setting, and Participants Daily respiratory symptoms and medication use were examined prospectively for 271 children younger than 12 years with physician-diagnosed, active asthma residing in southern New England. Main Outcome Measures Respiratory symptoms and rescue medication use recorded on calendars by subjects mothers. Results Mean (SD) levels were 59 (19) ppb (1-hour average) and 51 (16) ppb (8-hour average) for ozone and 13 (8) µg/m3 for PM2.5. In copollutant models, ozone level but not PM2.5 was significantly associated with respiratory symptoms and rescue medication use among children using maintenance medication; a 50-ppb increase in 1-hour ozone was associated with increased likelihood of wheeze (by 35%) and chest tightness (by 47%). The highest levels of ozone (1-hour or 8-hour averages) were associated with increased shortness of breath and rescue medication use. No significant, exposure-dependent associations were observed for any outcome by any pollutant among children who did not use maintenance medication. Conclusion Asthmatic children using maintenance medication are particularly vulnerable to ozone, controlling for exposure to fine particles, at levels below EPA standards.")
49
Acta Paediatrica 2010

50
2007 Associations are expressed as a percentage change (95% confidence interval) in the number of ER visits for an increase of 10 ug/m3 in NO2, at different lags (0–5),
,")
51
Criteria for assessing causality of associations
Strength of association Strong association considered to be more likely causal than weak associations Temporality Exposure precedes effect Specificity A cause is associated with a single effect Biologic gradient An exposure-response relationship is present Plausibility Coherence Experimental evid. The association should be consistent with relevant biologic data Hill (1965), Rothman (1986, 1998).
, Rothman (1986, 1998).")
52
coherence symptoms lung function decrease
GP visits/use of medications ED presentations hospital admissions

54
particulate matter and ozone)
2005 The available evidence is also sufficient to assume a causal relationship between exposure to air pollution and aggravation of asthma (mainly due to exposure to particulate matter and ozone)
")
55
2005 A significant body of evidence supports the explanation that much of the morbidity and mortality related to air pollution in children occurs via interactions with respiratory infections, which are very frequent among children. Evidence suggests a causal relationship between exposure to ambient air pollution and increased incidence of upper and lower respiratory symptoms (many of which are likely to be symptoms of infections).
.")
56
Effetti sulla funzionalità polmonare

57
Gaudermann et al, NEJM 2004 Community specific proportion of 18 year old with a FEV1 below 80% of the Predicted Value Plotted against the average levels of PM10 from 1994 through 2000.

58
Gaudermann et al, Lancet 2007

59
Studies of lung function in children suggest that:
2005 Studies of lung function in children suggest that: • living in areas of high air pollution is associated with lower lung function; • chronically elevated air pollution is associated with lower rates of lung function growth; • improvement in air pollution leads to improvements in lung function level and/or growth rate; • acute exposures to air pollution are associated with apparently reversible deficits in lung function; and • children who spend a significant amount of time outdoors in polluted environments or those with poor nutrition may be more strongly affected by air pollution.

60
2005 These effects of air pollution are modest, accounting for only a few per cent of the deficit in average lung function. Nevertheless, the studies suggest that the effects can be cumulative over a 20-year growing period, and there is uncertainty over whether the chronic effects are reversible.

61
Effetti cronici

62
Prevalenza Asma e Allergie 1980-1990: aumento medio 5% /anno

63
1980-1990: aumento medio 14% / anno
Prevalenza della rino-congiuntivite allergica e del tasso di sensibilizzazione : aumento medio 14% / anno aumento medio 6.7% /anno

64
ISAAC, The International Study of Asthma and Allergies in Childhood, is a unique worldwide epidemiological research programme established in 1991 to investigate asthma, rhinitis and eczema in children due to considerable concern that these conditions were increasing in western and developing countries. ISAAC has become the largest worldwide collaborative research project ever undertaken, involving more than 100 countries and nearly 2 million children and its aim is to develop environmental measures and disease monitoring in order to form the basis for future interventions to reduce the burden of allergic and non-allergic diseases, especially in children in developing countries. The ISAAC findings to date have shown that these diseases are increasing in developing countries and that they have little to do with allergy, especially in the developing world. Further population studies are urgently needed to discover more about the underlying mechanisms of non-allergic causes of asthma, rhinitis and eczema and the burden of these conditions.

65
ISAAC : International Study of Asthma and Allergies in Childhood
Obiettivo: Stimare la prevalenza di asma ed allergie nella popolazione di 6/7 anni e 13/14 anni, per effettuare confronti geografici e temporali. Metodo: 2 studi trasversali (campione casuale di almeno 1000 bambini), a distanza di almeno 5 anni; stesso protocollo d’indagine, questionari standardizzati
, a distanza di almeno 5 anni; stesso protocollo d’indagine, questionari standardizzati.")
66
Condizioni considerate
Sibili (12 mesi) Asma (nella vita) Oculorinite (12 mesi) Raffreddore primaverile (nella vita) Segni di dermatite atopica (12 mesi) Eczema (nella vita)
 Asma (nella vita) Oculorinite (12 mesi) Raffreddore primaverile (nella vita) Segni di dermatite atopica (12 mesi) Eczema (nella vita)")
67
ISAAC core questions Sibili 12 mesi: "Have you had wheezing or whistling in the chest in the past 12 months?“ Oculorinite 12 mesi; "In the past 12 months, have you had a problem with sneezing, or a runny, or a blocked nose, accompanied by itchy and watery eyes when you did not have a cold or the flu?" Dermatite atopica 12 mesi:“Have you had an itchy rash, which was coming and going for at least 6 months at any time in the last 12 months, affecting any of the following places: the folds of the elbows, behind the knees, in front of the ankles, under the buttocks, or around the necks, ears, or eyes?"

68
SIDRIA Estensione italiana di ISAAC (International Study on Asthma and Allergies in Childhood) Fase 1 (ISAAC I): 1994/1995 Fase 2 (ISAAC III): 2002 Gruppo Collaborativo SIDRIA-2° fase
: Gruppo Collaborativo SIDRIA-2° fase.")
69
SIDRIA 2° fase Cambiamenti nella prevalenza di asma e allergie tra le due fasi dello studio Gruppo Collaborativo SIDRIA-2° fase

70
Caratteristiche della popolazione
Bambini 94/ Adolescenti (self) 94/ N° di aree 6 8 Rispondenza (%) 95,5 92,5 96,6 92,7 N° di soggetti 16 115 11 287 19 723 10 267 Genere maschile (%) 51,8 51,3 52,2 52,5 Età (media) 6,4 6,7 13,1 13,3 Gruppo Collaborativo SIDRIA-2° fase
 94/ N° di aree Rispondenza (%) 95,5. 92,5. 96,6. 92,7. N° di soggetti Genere maschile (%) 51,8. 51,3. 52,2. 52,5. Età (media) 6,4. 6,7. 13,1. 13,3. Gruppo Collaborativo SIDRIA-2° fase.")
71
Cambiamenti nella prevalenza di fischi/sibili negli ultimi 12 mesi per fasce di età
% Gruppo Collaborativo SIDRIA-2° fase

72
Cambiamenti nella prevalenza di asma (nella vita) per fasce di età
% Gruppo Collaborativo SIDRIA-2° fase

73
Prevalenza di asma e sibili nei 12 mesi per livello di urbanizzazione
Bambini (6-7 anni) – SIDRIA-2
 – SIDRIA-2.")
74
Cambiamenti nella prevalenza di raffreddore primaverile (nella vita) per fasce di età
% Gruppo Collaborativo SIDRIA-2° fase

75
Cambiamenti nella prevalenza nella vita di asma, raffreddore primaverile ed eczema nei GENITORI di bambini di 6-7 anni p < .05

76
SIDRIA II Analisi sensibilità
L’inclusione nel modello di analisi di diversi fattori (istruzione della madre, compilatore del questionario, stagione di rilevazione ) non cambia i risultati in modo sostanziale.
 non cambia i risultati in modo sostanziale.")
79
In sintesi La sintomatologia asmatica è invariata. La crescita sembra essersi fermata Modesto aumento della “diagnosi” di asma, probabilmente in rapporto ad un maggior riconoscimento della malattia Rapido aumento dei sintomi di rinite allergica e della diagnosi di raffreddore allergico nei bambini e nei ragazzi Rapido aumento dei sintomi di dermatite atopica e della diagnosi di eczema nei bambini e nei ragazzi

81
ERJ 2001; 17:881

82
ERJ 2004; 23:407

83
BMJ 2004; 328:1052 -6.4 -3.4 -0.3 -2.2 -3.3 -4.8

84
BMJ 2004; 328:1052 +5.4 +2.6 +3.3 -3.4

85
BMJ 2004; 328:386

87
In the last 8 years, the prevalence of asthma
Allergy, 2004; 59:1301 –1307 L. García-Marcos et al. Stabilization of asthma prevalence among adolescents and increase among schoolchildren (ISAAC phases I and III) in Spain. In the last 8 years, the prevalence of asthma has not changed in year-old Spanish children but has increased substantially in 6-7-year olds
 in Spain. In the last 8 years, the prevalence of asthma. has not changed in year-old Spanish children. but has increased substantially in 6-7-year olds.")
88
Eur Resp J 2005, 26: The prevalence of asthma in children: a reversing trend C.P. van Schayck and H.A. Smit The general practice registration showed that after a five-fold increase in asthma prevalence during the 1980s and 1990s a downward trend seemed to occur around the turn of the century. The public health service confirms a clear decrease in wheezing and dyspnoea in children during the late 1990s. Thus far, there has been no satisfactory explanation for this observation.

89
Key findings di ISAAC Fase III
Modesti cambiamenti della prevalenza totale dei sintomi asmatici Riduzione della prevalenza di asma nei Paesi anglofoni Aumenti in alcuni (ma non in tutti) i Paesi dove precedentemente la prevalenza dell’asma era bassa Aumenti della prevalenza in particolare in Africa, America Latina e alcuni paesi asiatici Le differenze internazionali nella prevalenza dei sintomi asmatici si sono ridotte Aumenti della prevalenza d’asma diagnosticata in quasi tutti i Paesi L’asma non è più una malattia anglofona
 i Paesi dove precedentemente la prevalenza dell’asma era bassa. Aumenti della prevalenza in particolare in Africa, America Latina e alcuni paesi asiatici. Le differenze internazionali nella prevalenza dei sintomi asmatici si sono ridotte. Aumenti della prevalenza d’asma diagnosticata in quasi tutti i Paesi. L’asma non è più una malattia anglofona.")
90
La ricerca delle cause dell’asma

91
Theories of asthma causation: The “hygiene” hypothesis
Strachan, The British National Child Development Study A lower exposure to infections in early childhood is associated with an increased risk of asthma and hay fever This could be occurring through a reduced TH1 and an increased TH2 immune response

92
“L’ipotesi igienistica”
L’aumento a livello globale nella prevalenza dell’asma sarebbe attribuibile ad un aumento della suscettibilità alla sensibilizzazione antigenica e/o allo sviluppo dell’asma Tale aumento potrebbe essere dovuto al fatto che, vivendo in ambienti domestici più puliti, abbiamo perso l’effetto protettivo fornito in passato dalle infezioni contratte in età infantile Questa ipotesi descrive meglio la distribuzione della prevalenza dell’asma a livello globale Esistono però molte eccezioni: per esempio, la prevalenza dell’asma è più alta in America Latina (nonostante gli alti tassi di infezioni pediatriche) che non in Spagna o in Portogallo.
 che non in Spagna o in Portogallo.")
93
Tutto è determinato prima della nascita?

94
US-born Mexicans children were significantly more likely
Eldeirawi K et al, J Allergy Clin Immunol 2005: **Questionnaires with interview to parents of children 0-16 years old (NHANES-NHIS) US-born Mexicans children were significantly more likely to report asthma diagnosis than Mexico-born peers, after accounting for potential confounding variables
 US-born Mexicans children were significantly more likely. to report asthma diagnosis than Mexico-born peers, after accounting for potential confounding variables.")
95
US-born Mexicans had a higher prevalence of asthma
Holguin F et al,Am J Resp Crit Care Med 2005: **Questionnaires with interview (aged => 18 years) in the language spoken in the household (NHANES-NHIS) US-born Mexicans had a higher prevalence of asthma than did Mexican-born Mexicans, independent to access to health care and other potential confounders 2) With prolonged times of residence in the US, the prevalence of asthma increased in Mexican-born participants less than 10yrs of residence = 2%, more than 10yrs of residence = 4%
 in the language spoken in the household (NHANES-NHIS) US-born Mexicans had a higher prevalence of asthma. than did Mexican-born Mexicans, independent to access to health care and other potential confounders. 2) With prolonged times of residence in the US, the. prevalence of asthma increased in Mexican-born participants. less than 10yrs of residence = 2%, more than 10yrs of residence = 4%")
96
Results-1. Prevalence of asthma and wheezing by birthplace – SIDRIA II
*p<0.05, ** p<0.001 by 2 test

97
Results-2. Prevalence (%) of asthma/wheezing by birthplace/parent origin
 of asthma/wheezing by birthplace/parent origin")
98
98

99
Considerazioni I bambini e gli adolescenti nati all’estero hanno una prevalenza significativamente più bassa di asma e wheezing rispetto ai coetanei nati in Italia. Questi risultati sono consistenti con quelli di altri studi che hanno evidenziato come i bambini nati in Paesi più poveri abbiano una minor prevalenza di asma.

100
Considerazioni 2) Tuttavia, la frequenza di asma e sintomi asmatici dei bambini immigrati è risultata diversa a seconda del tempo trascorso dalla migrazione, mostrando un incremento del rischio associato alla permanenza in Italia. Anche questo dato è già stato segnalato in letteratura, e suggerisce che i cambiamenti nell’esposizione a fattori ambientali e l’adozione di uno stile di vita occidentale abbiano un ruolo predominante rispetto a fattori genetici nello sviluppo dell’asma nell’infanzia.
 Tuttavia, la frequenza di asma e sintomi asmatici dei bambini immigrati è risultata diversa a seconda del tempo trascorso dalla migrazione, mostrando un incremento del rischio associato alla permanenza in Italia. Anche questo dato è già stato segnalato in letteratura, e suggerisce che i cambiamenti nell’esposizione a fattori ambientali e l’adozione di uno stile di vita occidentale abbiano un ruolo predominante rispetto a fattori genetici nello sviluppo dell’asma nell’infanzia.")
101
Considerazioni 3) Tutto questo sarebbe a supporto dell’ipotesi secondo la quale nell’espressione della malattia asmatica non giocano un ruolo primario solo i primi anni di vita, ma possono essere rilevanti anche i successivi cambiamenti nelle esposizioni ambientali, come confermato anche da alcuni studi di tipo occupazionale
 Tutto questo sarebbe a supporto dell’ipotesi secondo la quale nell’espressione della malattia asmatica non giocano un ruolo primario solo i primi anni di vita, ma possono essere rilevanti anche i successivi cambiamenti nelle esposizioni ambientali, come confermato anche da alcuni studi di tipo occupazionale.")
102
Asthma epidemiology The future
Genetic factors cannot account for the increase of asthma, but gene-environment interactions may be important. The search for environmental causes of asthma is likely to continue to be primary, while the study of gene-environment interactions will play an important secondary role Pearce, 2001

103
Inquinamento atmosferico e insorgenza dell’asma (new onset asthma)
")
104
2005 There was little evidence for a causal association between the prevalence/incidence of asthma and air pollution in general, though the evidence is suggestive for a causal association between the prevalence/incidence of asthma symptoms and living in close proximity to traffic.

108
Inquinamento atmosferico e birth outcomes

109
2005 Overall, there is evidence implicating air pollution in adverse effects on birth outcomes, but the strength of the evidence differs between outcomes. The evidence is solid for infant mortality: this effect is primarily due to respiratory deaths in the post-neonatal period and it appears to be mainly due to particulate air pollution.

111
2005 Overall, there is evidence implicating air pollution in adverse effects on birth outcomes, but the strength of the evidence differs between outcomes. Studies on birth weight, preterm births and IUGR also suggest a link with air pollution, but there were important inconsistencies in the results that were probably due to differences in design and measurement of exposure(s).
.")
117
Ipotesi sui meccanismi biologici plausibili
Risposta infiammatoria Stress ossidativo Disfunzioni placentari

118
Inquinamento atmosferico e tumori infantili

119
2005 Accumulated epidemiological evidence is insufficient to infer a causal link between childhood cancer and the levels of outdoor air pollution typically found in Europe. However, the number of available studies is limited and their results are not fully consistent. Future studies, considering exposure during different periods from conception to disease diagnosis, may help to support a clearer conclusion about the role of childhood exposures to air pollution in causing cancers in both childhood and adulthood.

121
Levels of evidence for causal relationships were defined as: (i) sufficient—at least one expert group has reviewed the available evidence and published a peer-reviewed report indicating a consensus view that there is a causal relationship, (ii) limited—evidence is suggestive of an association between the agent and the outcome but is limited (and may or may not represent a causal relationship) because chance, bias and confounding cannot be ruled out with confidence, e.g., at least one high-quality study shows a positive association but the results of other studies are inconsistent and, (iii) inadequate—available studies are of insufficient quality (e.g., available studies have failed to adequately control for confounding or have inadequate exposure assessment), consistency or statistical power to permit a conclusion regarding the presence or absence of an association or no studies exist that examine the relationship.
 sufficient—at least one expert group has reviewed the available evidence and published a peer-reviewed report indicating a consensus view that there is a causal relationship, (ii) limited—evidence is suggestive of an association between the agent and the outcome but is limited (and may or may not represent a causal relationship) because chance, bias and confounding cannot be ruled out with confidence, e.g., at least one high-quality study shows a positive association but the results of other studies are inconsistent and, (iii) inadequate—available studies are of insufficient quality (e.g., available studies have failed to adequately control for confounding or have inadequate exposure assessment), consistency or statistical power to permit a conclusion regarding the presence or absence of an association or no studies exist that examine the relationship.")
122
Quali sviluppi di ricerca sugli effetti dell’inquinamento atmosferico?
Migliorare ( e standardizzare) le metodologie di indagine per gli effetti (soprattutto cronici) per i quali l’evidenza è limitata Studi per migliorare le conoscenze sui meccanismi d’azione Studi su effetti relativamente poco studiati (es. effetti sullo sviluppo neurocomportamentale del bambino)
 le metodologie di indagine per gli effetti (soprattutto cronici) per i quali l’evidenza è limitata. Studi per migliorare le conoscenze sui meccanismi d’azione. Studi su effetti relativamente poco studiati (es. effetti sullo sviluppo neurocomportamentale del bambino)")
125
Annual Cases (and %) attributed to Air Pollution Austria, France, and Switzerland
Künzli et al, Lancet 2000; 356: Outcome Cases Attribut. % Death (adults ³ 30yrs.) 40‘600 (24‘600-56'900) ~ 6 % Hospital Admissions (cardio-respiratory causes) 48’000 (17’300–79’100) ~ 2 % Chronic Bronchitis (incidence in adults) 47'100 (4’300-93'500) ~ 12 % Bronchitis Episodes (children) 543'000 (239’ '600) ~ 30 % Restricted Activity Days (adults) 30.5 mill. ( mill) Asthma attacks ~ 6 % 1.04 mill. (0.54–1.54 mill.)
 40‘600. (24‘ ) ~ 6 % Hospital Admissions. (cardio-respiratory causes) 48’000. (17’300–79’100) ~ 2 % Chronic Bronchitis (incidence in adults) (4’ ) ~ 12 % Bronchitis Episodes (children) (239’ ) ~ 30 % Restricted Activity Days (adults) 30.5 mill. ( mill) Asthma attacks. ~ 6 % 1.04 mill. (0.54–1.54 mill.)")
Presentazioni simili




 Brussels, 26 settembre 2013.>")
 064825120 - fax.>")












>")


