Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Le infezioni delle vie urinarie: le nuove linee guida
Giovanni Montini Nefrologia Pediatrica Bologna

3
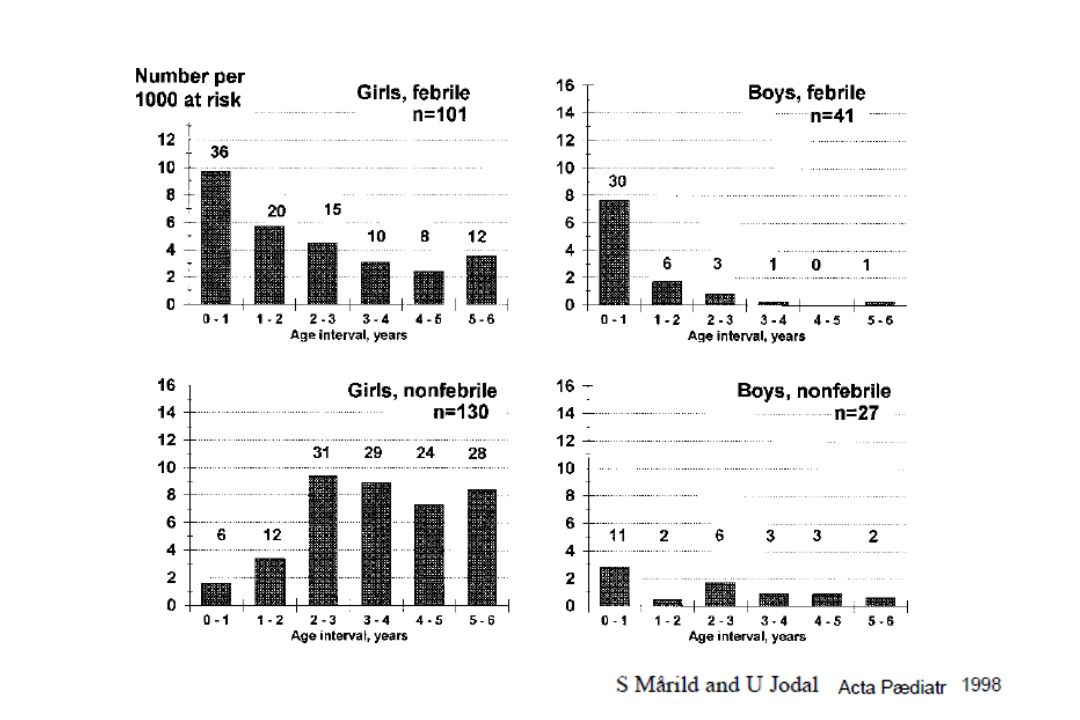
INCIDENCE: 1.7/1000 boys/year
UTI - EPIDEMIOLOGY INCIDENCE: 1.7/1000 boys/year 3.1/1000 girls/year PREVALENCE: girls % (0-6 y) boys 2,5 % (Jodal ESPN 2002) 3
 boys 2,5 % (Jodal ESPN 2002) 3.")
5
Fig 2 Distribution by age (months) and sex of 502 children
Montini, G. et al. BMJ 2007;335:386 Copyright ©2007 BMJ Publishing Group Ltd. 5

9
UTIs: Pathophysiology
Kidneys and urinary tract are germ free When bacteria enter a number of conditions may develop: Bacteriuria Cystitis Febrile UTIs with activation of the inflammatory process Adequate urine flow and intact uroepithelium are key in the prevention of UTI. E. coli have P fimbriae that facilitate uroepithelial attachment

10
Montini G et al. N Engl J Med 2011
Quimiocinas citoquinas Figure 2 Pathophysiology of Acute Pyelonephritis. Acute pyelonephritis occurs when bacteria ascend to the kidneys, causing intrarenal infection. Escherichia coli bacteria with P fimbriae attach to uroepithelial cells and cannot be flushed out. The endotoxin (lipopolysaccharide) of the bacteria binds to CD14 on the cell surface, activating toll-like receptor (TLR) 4. Through subsequent steps, this activates transcription factor nuclear factor κB (NF-κB), which migrates into the cell nucleus, stimulating production of inflammatory factors, including cytokines, chemokines, nitric oxide, and transforming growth factor β. These mediators induce an inflammatory response, which increases vascular permeability and recruitment of neutrophils to resolve the infection, but the mediators are also responsible in part for the ensuing kidney scarring. COX-2 denotes cyclooxygenase-2, I-κB inhibitory protein κB, TGF-β transforming growth factor β, and TNF-α tumor necrosis factor α. Montini G et al. N Engl J Med 2011 10
 of the bacteria binds to CD14 on the cell surface, activating toll-like receptor (TLR) 4. Through subsequent steps, this activates transcription factor nuclear factor κB (NF-κB), which migrates into the cell nucleus, stimulating production of inflammatory factors, including cytokines, chemokines, nitric oxide, and transforming growth factor β. These mediators induce an inflammatory response, which increases vascular permeability and recruitment of neutrophils to resolve the infection, but the mediators are also responsible in part for the ensuing kidney scarring. COX-2 denotes cyclooxygenase-2, I-κB inhibitory protein κB, TGF-β transforming growth factor β, and TNF-α tumor necrosis factor α. Montini G et al. N Engl J Med")
12
Outcome renal function
Recruited children 3479 Prevalence of patients with impaired renal function: 0-56% 1029 children included in 8 prospective studies; of the 55 children with CKD at the end of follow-up, only in 4 (0.4%) renal function was normal at start. Almost all children with a decreased renal function at the end of follow-up showed scars or hypodysplastic kidneys at start.
 renal function was normal at start. Almost all children with a decreased renal function at the end of follow-up showed scars or hypodysplastic kidneys at start.")
13
Febrile Urinary Tract Infections
Vesico- ureteric reflux Renal hypo-dysplasia Post infectious scarring

14
Caso Clinico n° 1 Marco ecografie fetali normali, è sempre stato bene; crescita e sviluppo regolari. All’età di 8 mesi presenta un episodio febbrile. Alla visita presenta: Buone condizioni generali TC 38.7, da circa 24 ore esame obiettivo negativo Eseguite tutte le vaccinazioni consigliate

15
Caso clinico1 Come mi comporto?
Vigile attesa Eseguo stick urine Prescrivo esame urine + urocoltura + esami ematochimici (emocromo, VES, PCR) Ricovero ospedaliero
 Ricovero ospedaliero.")
16
Caso clinico n°1 Come mi comporto?
Eseguo stick urine PS 1015,PH 5, GB ++, Nitriti Positivo

17
Caso clinico1 Come mi comporto?
Ricovero ospedaliero Prescrivo esame urine + urocoltura + esami ematochimici (emocromo, VES, PCR) Prescrivo urocoltura Vigile attesa
 Prescrivo urocoltura. Vigile attesa.")
18
Come mi comporto? Prescrivo urocoltura 106 E. Coli

19
Caso clinico 1 Come ottengo il campione di urine? (stick)
Puntura sovrapubica Cateterismo vescicale Mitto intermedio Sacchetto perineale

20
Caso clinico 1 Come ottengo il campione di urine? (urocoltura)
Mitto intermedio Sacchetto perineale

21
Caso clinico 1bis Come mi comporto?
Ricovero ospedaliero Prescrivo esame urine + urocoltura + esami ematochimici (emocromo, VES, PCR) Prescrivo urocoltura Vigile attesa
 Prescrivo urocoltura. Vigile attesa.")
22
Caso clinico n°1 Marco ecografie fetali normali, è sempre stato bene; crescita e sviluppo regolari. All’età di 8 mesi diagnosi di IVU febbrile da E Coli. Quale accertamento diagnostico ritenete necessario eseguire per primo?

23
Quale accertamento strumentale ritenete necessario eseguire per primo?
ECOGRAFIA CISTOGRAFIA SCINTIGRAFIA CON DMSA SCINTIGRAFIA CON MAG3 UROGRAFIA

24
Quale accertamento ritenete necessario eseguire per primo?
ECOGRAFIA

25
Caso clinico n°1 Marco ecografie fetali normali, è sempre stato bene; crescita e sviluppo regolari. All’età di 8 mesi diagnosi di IVU febbrile da E Coli. Ecografia renale eseguita 15 giorni dopo l’infezione urinaria evidenzia un quadro normale

26
Prescrivo profilassi antibiotica e urinocolture di controllo
Come procedi? Prescrivo profilassi antibiotica e urinocolture di controllo Prescrivo profilassi e richiedo cistografia minzionale Prescrivo profilassi e richiedo scintigrafia con DMSA Osservazione clinica

27
Come procedi? Osservazione clinica

28
Caso clinico n°2 Andrea ecografie fetali normali, è sempre stato bene; crescita e sviluppo regolari. All’età di 8 mesi diagnosi di IVU febbrile da Pseudomonas. Ecografia renale eseguita 15 giorni dopo l’infezione urinaria evidenzia un quadro normale

29
Prescrivo profilassi antibiotica e urinocolture di controllo
Come procedi? Prescrivo profilassi antibiotica e urinocolture di controllo Prescrivo profilassi e richiedo cistografia minzionale Prescrivo profilassi e richiedo scintigrafia con DMSA Osservazione clinica

30
Prescrivo profilassi e richiedo cistografia minzionale
Come procedi? Prescrivo profilassi e richiedo cistografia minzionale

31
Caso clinico n° 2 Andrea ecografie fetali normali, è sempre stato bene; crescita e sviluppo regolari. All’età di 8 mesi diagnosi di IVU febbrile da Pseudomonas. Ecografia renale : normale Cistografia minzionale: RVU di terzo grado a sx

32
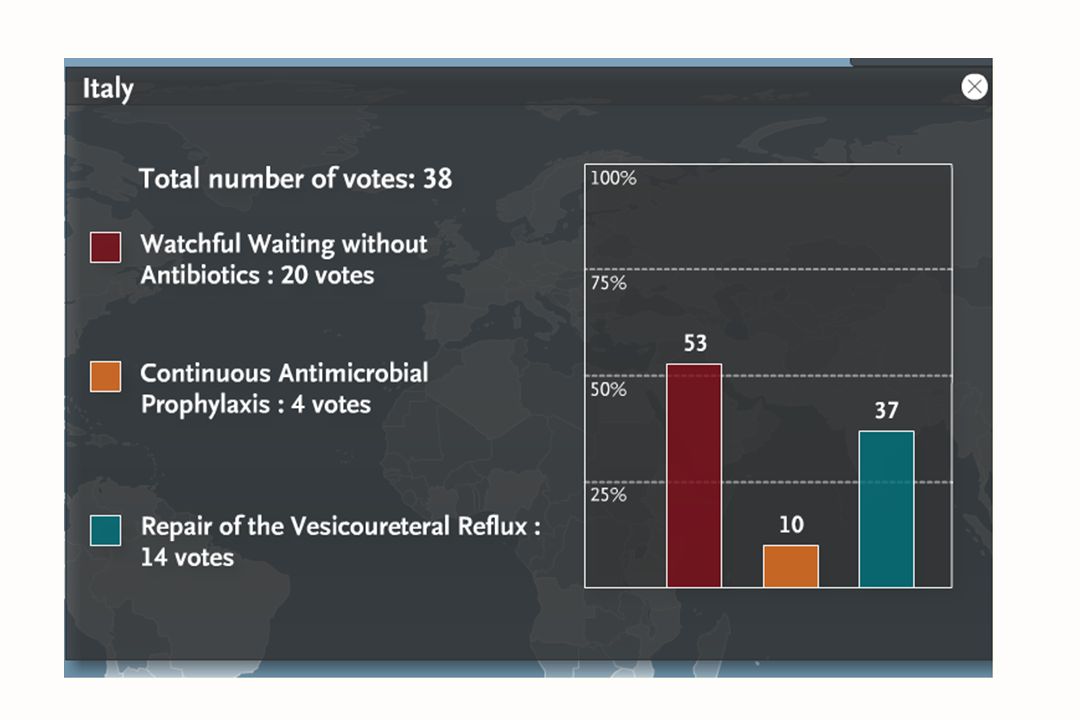
Che programma per questo bambino?
Stop profilassi, urinocolture mensili ed in corso di febbre. Continua profilassi, urinocolture in caso di febbre isolata o sintomi evocativi di IVU Continua profilassi, urinocolture mensili ed in caso di febbre isolata o sintomi evocativi di IVU

33
Che programma per questo bambino?
Continua profilassi, urinocolture in caso di febbre isolata o sintomi evocativi di IVU

35
Febrile UTIs: diagnosis and management
Urinalysis and urine culture Blood inflammatory markers Management Treatment of the acute episode Prophylaxis Imaging investigations Urocultivos imagenes 35

36
When to suspect a UTI ? SINP SINP SINP
Ictericia incircuncidado circuncicion SINP SINP SINP 36

39
SINP

40
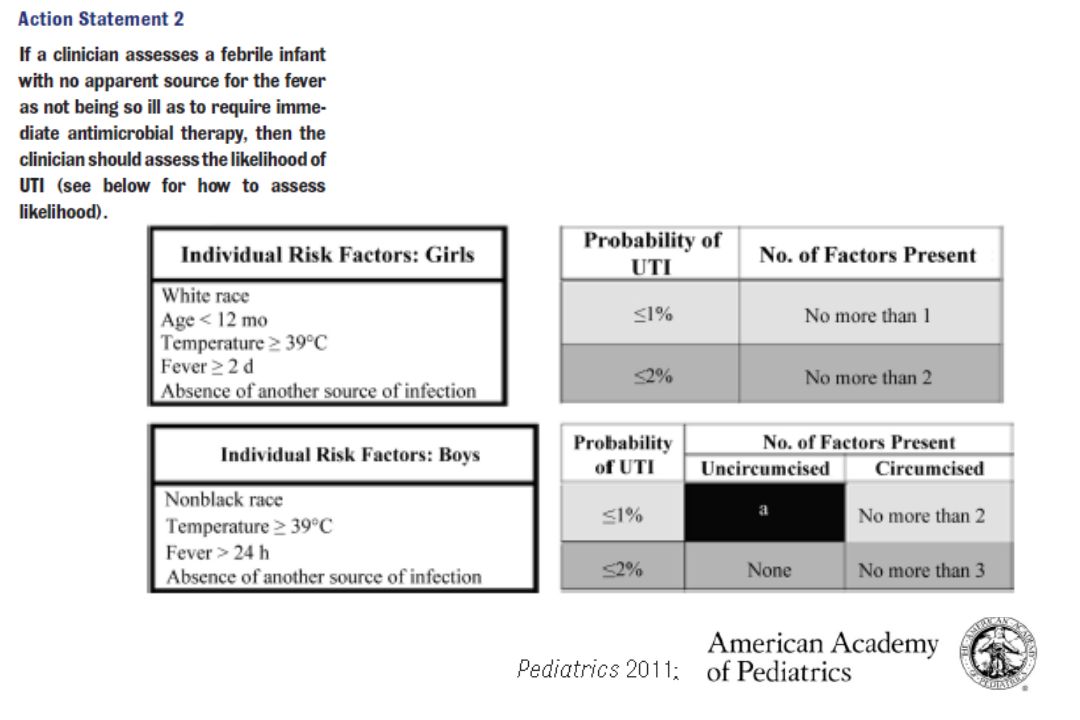
What to do when a UTI is suspected ?
Collectionada cinta reactiva (dipstick) vejiga diagnostico muyenfermos Chorro medio Bolsa recollectora SINP 40
 vejiga diagnostico muyenfermos. Chorro medio. Bolsa recollectora. SINP. 40.")
41
UTI Diagnosis Cateterismo muestra de orina 41

42
Febrile UTIs: diagnosis and management
Urinalysis and urine culture Blood inflammatory markers Management Treatment of the acute episode Prophylaxis Imaging investigations 42

43
Are blood tests necessary if a UTI is suspected ?
In the published guidelines and in the most recent literature C reactive protein and WBC are not considered useful diagnostic tools to identify renal parenchymal involvement, because of a low specificity. If a blood analysis is prescribed, procalcitonin is considered the best test to diagnose the level of infection Especificidad herramienta (tool) SINP 43
 SINP. 43.")
44
PCT CRP Pecile P et al, Pediatrics 2004

45
Febrile UTIs: diagnosis and management
Urinalysis and urine culture Blood inflammatory markers Management Treatment of the acute episode Prophylaxis Imaging investigations 45

46
Primary and Secondary outcomes in the 502 randomised children
Montini, G. et al. BMJ 2007;335:386 46

47
Susceptibility to antimicrobials
IRIS 1 (00-05) Padova 07 Pordenone 07 n (% E. Coli) 490 (94%) 149 (88%) Amoxicillin 32% 49% 33% Co-amoxiclav 6% 14% 1% Sulf-trimetr 12% 17% Cefal (IIIG) <1% Aminoglic 4% Ciproflox 2% 47
 Padova 07. Pordenone 07. n (% E. Coli) 490 (94%) 149 (88%) Amoxicillin. 32% 49% 33% Co-amoxiclav. 6% 14% 1% Sulf-trimetr. 12% 17% Cefal (IIIG) <1% Aminoglic. 4% Ciproflox. 2% 47.")
48
SINP

49
Hewitt 2008

50
Febrile UTIs: diagnosis and management
Urinalysis and urine culture Blood inflammatory markers Management Treatment of the acute episode Prophylaxis Imaging investigations 50

51
Bambina di 6 anni con VUR di III grado, diagnosticato all’età di 1 anno per pielonefrite. Eco normale, DMSA non eseguito a quell’epoca. Cotrimoxazolo per 1 anno senza recidive di pielonefrite Controllo degli sfinteri a 2 anni, no stipsi La famiglia si è trasferita diverse volte e in questo periodo vengono riferiti numerosi episodi febbrili, senza esecuzione di esame urine e urocoltura

52
A 6 anni diventa vostra paziente.
Le fate fare una cistoscintigrafia che conferma la presenza di RVU bilaterale di III grado; ecografia e scintigrafia con DMSA dimostrano reni normali. I genitori vi chiedono cosa fare. Cosa consigliate?

58
International Classification of Vesicoureteral Reflux.
Figure 1 International Classification of Vesicoureteral Reflux. This classification grades vesicoureteral reflux as follows: grade I, reflux into a nondilated ureter only; grade II, reflux into the renal pelvis and calyces without dilatation; grade III, reflux into a mildly to moderately dilated ureter and renal pelvis with no or only slight blunting of fornices; grade IV, moderate dilatation and tortuosity of the ureter and renal pelvis, with obliteration of the sharp angle of the fornices but maintenance of papillary impressions in most calyces; and grade V, gross dilatation and tortuosity of the ureter, renal pelvis, and calyces with loss of papillary impressions.16 Montini G et al. N Engl J Med 2011 58 58

59
6.7% 5.7% 8% 27.5% 42.8%

62
SINP

63
Cranberry juice it acts by inhibiting bacterial adhesion to uroepithelial cells. standardization is lacking, which renders comparison of studies difficult a Cochrane review reported that cranberry products may decrease symptomatic UTIs in women; a recent study suggested similar results in children a randomised placebo controlled trial (Finland) Arandano 63
 Arandano. 63.")
64
Febrile UTIs: diagnosis and management
Urinalysis and urine culture Blood inflammatory markers Management Treatment of the acute episode Prophylaxis Imaging investigations 64

65
First febrile UTI US Abnormal No risk factors and/or Risk factors:
ISPN US Abnormal and/or Risk factors: Abnormal prenatal US First degree relative with VUR Septicemia Chronic kidney disease Age < 6 mo. in a male infant Likely non-compliance of the family Abnormal bladder emptying No clinical response to correct antibiotic treatment within 72 hrs Bacteria other than E.coli Normal No risk factors No necessary further imaging Probable no compliance Falta de apoyo 2nd febrile UTI Further imaging ( cystography, renal radionuclide scan) 65
 65.")
66
UTI Imaging

67
VALUTAZIONE DELL’EFFICACIA DELLE RACCOMANDAZIONI SINP PER LA 1° INFEZIONE URINARIA FEBBRILE IN ETA’ PEDIATRICA. PROTOCOLLO MULTICENTRICO DI STUDIO.

68
Centro pz tot Pazienti arruolati Belluno 52 33 Oderzo 37 30 Treviso 61 57 Messina 29 21 Napoli 139 138 Milano 87 35 Bologna 114 Trieste 64 56 Palermo 26 19 Foggia 50 659 533

69
MODALITÀ RACCOLTA URINE

70
EZIOLOGIA 1°IVU

71
GESTIONE PAZIENTE

72
TERAPIA ANTIBIOTICA: via di somministrazione

73
TERAPIA ANTIBIOTICA: scelta del farmaco

74
TERAPIA ANTIBIOTICA: resistenze antibiotici di E.coli - 1
CO-AMOXICLAV CEFALOSPORINE ORALI CEFALOSPORINE PARENTERALI

75
CARATTERISTICHE PAZIENTI
Centro Pazienti arruolati pz con fatt rischio % pz con fatt rischio pz SENZA fatt rischio % pz SENZA fatt rischio Belluno 33 14 42% 19 58% Oderzo 30 11 37% 63% Treviso 57 27 47% 53% Messina 21 18 86% 3 14% Napoli 138 107 78% 31 22% Milano 35 77% 8 23% Bologna 114 75 66% 39 34% Trieste 56 26 46% 54% Palermo 13 68% 6 32% Foggia 24 80% 20% 533 342 64% 191 36%

76
PAZIENTI A RISCHIO centro pz con fatt rischio CUM eseguite x 1° IVU
NO RVU NO RVU % RVU RVU % Belluno 14 8 4 50% Oderzo 11 3 38% 5 63% Treviso 27 20 16 80% 20% Messina 18 44% 10 56% Napoli 107 101 51 50 Milano 24 15 9 Bologna 75 63 32 51% 31 49% Trieste 26 12 67% 33% Palermo 13 7 70% 30% Foggia 19 68% 6 32% TOT 342 283 157 55% 126 45%

77
PAZIENTI A RISCHIO centro RVU RVU basso grado RVU basso grado %
RVU alto grado % RVU alto grado Belluno 4 0% 100% Oderzo 5 2 40% 3 60% Treviso Messina 10 30% 7 70% Napoli 50 10% 45 90% Milano 9 22% 78% Bologna 31 23% 24 77% Trieste 1 25% 75% Palermo 67% 33% Foggia 6 TOT 126 22 17% 104 83%

78
BAMBINI CON FATTORI DI RISCHIO

79
BAMBINI NON A RISCHIO con 2° IVU: cistografie
TOT 191 bambini senza fattori di rischio 3° grado: 15 4° grado: 6

80
BAMBINI NON A RISCHIO con 2° IVU: scintigrafie DMSA
TOT 42 bambini senza fattori di rischio con 2° IVU

81
Current Understanding of Febrile Urinary Tract Infections and Renal Scarring.
Figure 4 Current Understanding of Febrile Urinary Tract Infections and Renal Scarring. The figure shows the current approach (blue) to febrile urinary tract infection (UTI) in children and highlights the contribution of congenital damage and the importance of immunologic and genetic factors (red). The figure also recognizes the role of infection-related kidney scarring in producing major long-term medical sequelae. Genetic factors influence both the occurrence of dysplasia and the propensity for scar formation. VUR denotes vesicoureteral reflux, and VUR III–V grade III to grade V reflux. The role of antibiotic prophylaxis that is depicted here represents our view. Montini G et al. N Engl J Med 2011 81 81
 to febrile urinary tract infection (UTI) in children and highlights the contribution of congenital damage and the importance of immunologic and genetic factors (red). The figure also recognizes the role of infection-related kidney scarring in producing major long-term medical sequelae. Genetic factors influence both the occurrence of dysplasia and the propensity for scar formation. VUR denotes vesicoureteral reflux, and VUR III–V grade III to grade V reflux. The role of antibiotic prophylaxis that is depicted here represents our view. Montini G et al. N Engl J Med")
Presentazioni simili