Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Highlights in the management of renal cell carcinoma
Mediterranean School of Oncology Highlights in the management of renal cell carcinoma Criteria for defining resistance to TKIs: Are RECIST appropriate? G. Cartenì Direttore U.O.S.C. di Oncologia Medica A.O.R.N. A. Cardarelli Napoli Roma, 22 febbraio 2013

2
Routes to longer-term survival in mRCC
Efficacious first-line agents Effective therapy management Longer-term survival However…. ….despite the benefits observed with targeted first-line agents and the application of therapy management, resistance eventually develops in mRCC and the disease progresses

3
When to start second-line therapy?
‘Progression’ incorporates a wide range of clinical scenarios Progression will be observed in patients with primary resistance within 2-3 months of targeted therapy Patients with evasive resistance to targeted therapy may be: Early progressors (6-12 months of treatment) Late progressors (12+ months) Clinicians need to use a combination of pathologic data and clinical assessment to decide whether disease progression has occurred and, consequently, whether and when to start a second-line treatment Rini BI, and Flaherty K, Urol Oncol 2008; Négrier S. Oncol 2012;82:189–96
 Late progressors (12+ months) Clinicians need to use a combination of pathologic data and clinical assessment to decide whether disease progression has occurred and, consequently, whether and when to start a second-line treatment. Rini BI, and Flaherty K, Urol Oncol 2008; Négrier S. Oncol 2012;82:189–96.")
6
Nella ricerca Risposta obiettiva misurata Durata della risposta
Tempo alla progressione Criteri Recist per la misurazione

7
“Non tante risposte molte stabilità”
Considerazioni “Non tante risposte molte stabilità” “Il beneficio clinico del paziente”

8
Necessario fare riferimento a criteri:
Valutazione dello stato di malattia in corso di trattamento con targeted therapies Necessario fare riferimento a criteri: Diagnostica strumentale Clinici Laboratorio

10
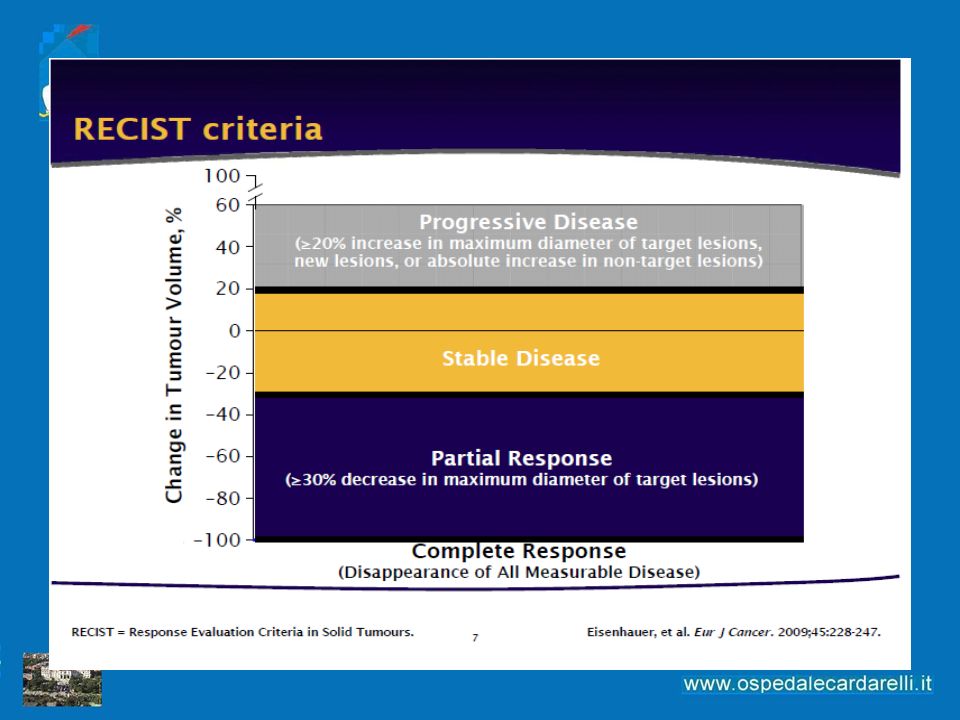
Criteri di risposta (RECIST) - Criticità
I criteri RECIST rappresentano lo standard di valutazione di risposta al trattamento in studi clinici su farmaci antitumorali1 La risposta parziale è definita come tumor shrinkage pari al 30% Un tumor shrinkage del < 30% è un risultato positivo per il paziente. Il controllo del tumore potrebbe essere un endpoint clinicamente più rilevante2 Potrebbe non essere appropriato per valutare la risposta alle targeted therapies (differente meccanismo d’azione) Le targeted therapies possono determinare necrosi tumorale piuttosto che tumor shrinkage3 Si basa sulle risposte agli agenti antitumorali citotossici Non si misurano le necrosi tumorali 1. Therasse P, et al. J Natl Cancer Inst 2000; 92:205–16 2. Nygren P, et al Acta Oncologia 2008; 47:316–29 3. Abou-Alfa G, et al. J Clin Oncol 2006;24:4293–300
 Le targeted therapies possono determinare necrosi tumorale piuttosto che tumor shrinkage3. Si basa sulle risposte agli agenti antitumorali citotossici. Non si misurano le necrosi tumorali. 1. Therasse P, et al. J Natl Cancer Inst 2000; 92:205– Nygren P, et al Acta Oncologia 2008; 47:316–29 3. Abou-Alfa G, et al. J Clin Oncol 2006;24:4293–300.")
11
Revisione criteri di risposta (RECIST v. 1.1)
Principali modifiche proposte: Numero delle lesioni valutabili; Dimensioni dei linfonodi patologici; Conferma della risposta; Supporto FDG-PET per valutare le progressioni.

12
I criteri RECIST e la loro più recente revisione non tengono conto di:
Come valutare la risposta al trattamento nell’era delle targeted therapies? I criteri RECIST e la loro più recente revisione non tengono conto di: Tecniche di imaging funzionale come la PET o la RMN Valutazione anatomica volumetrica del tumore Necessità di nuove metodiche di immagine atte a studiare la vascolarizzazione e la necrosi tumorale MRI DCE-US = dynamic contrast enhanced-ultrasonography FDG-PET DCE-US DCE-MRI

13
Imaging funzionale con DCE-US Valutazione della risposta a sorafenib
Abdominal lymph node from an RCC in a 37 year-old woman (good responder) treated with sorafenib DCE-US before treatment shows contrast uptake throughout the tumour estimated at 81% Lamuraglia et al. “In the group of good responders, mean contrast uptake was 92% before treatment and decreased to 60% at 3 weeks. The mean volume was 115 cm3 before treatment, 107 cm3 at 3 weeks and 104 cm3 at 6 weeks for the good responders”. DCE-US after 3 weeks of treatment shows contrast uptake throughout the tumour estimated at 48% DCE-US after 6 weeks of treatment shows contrast uptake throughout the tumour estimated at 31% Lamuraglia et al.EJC 2006
 treated with sorafenib. DCE-US. before treatment shows contrast uptake throughout the tumour estimated at 81% Lamuraglia et al. In the group of good responders, mean contrast uptake was 92% before treatment and decreased to 60% at 3 weeks. The mean volume was 115 cm3 before treatment, 107 cm3 at 3 weeks and 104 cm3 at 6 weeks for the good responders . DCE-US after 3 weeks of treatment. shows contrast uptake throughout the tumour estimated at 48% DCE-US after 6 weeks of treatment shows contrast uptake. throughout the tumour estimated at 31% Lamuraglia et al.EJC")
15
identifying patients with progression-free survival of >250 days
sensitivity specificity MASS criteria 86% 100% SACT criteria 75% OBJECTIVE: The objective of our study was to evaluate response assessment and predict clinical outcome in patients with metastatic renal cell carcinoma (RCC) receiving antiangiogenic targeted therapy. Target lesions were assessed on routine contrast-enhanced CT (CECT) images obtained during the portal venous phase using new response criteria. MATERIALS AND METHODS: Standard CECT examinations of patients with metastatic clear cell RCC on first-line sunitinib or sorafenib therapy (n = 84) were retrospectively evaluated using Mass, Attenuation, Size, and Structure (MASS) Criteria; Response Evaluation Criteria in Solid Tumors (RECIST); Size and Attenuation CT (SACT) Criteria; and modified Choi Criteria. The objective response to therapy was compared with clinical outcomes including time to progression (TTP) and disease-specific survival. The Kaplan-Meier method was used to estimate survival functions. RESULTS: A favorable response according to MASS Criteria had a sensitivity of 86% and specificity of 100% in identifying patients with a good clinical outcome (i.e., progression-free survival of > 250 days) versus 17% and 100%, respectively, for RECIST partial response. The objective categories of response used by MASS Criteria-favorable response, indeterminate response, and unfavorable response-differed significantly from one another with respect to TTP (p < , log-rank test) and disease-specific survival (p < , log-rank test). CONCLUSION: Assessment of metastatic RCC target lesions on CECT for changes in morphology, attenuation, size, and structure by MASS Criteria is more accurate than response assessment by SACT Criteria, RECIST, or modified Choi Criteria. Furthermore, the use of MASS Criteria for imaging response assessment showed high interobserver agreement and may predict disease outcome in patients with metastatic RCC on targeted therapy Smith AD, Shah SN, Rini BI, Lieber ML, Remer EM. Morphology, Attenuation, Size, and Structure (MASS) criteria: assessing response and predicting clinical outcome in metastatic renal cell carcinoma on antiangiogenic targeted therapy. AJR Am J Roentgenol Jun;194(6):1470-8
 receiving antiangiogenic targeted therapy. Target lesions were assessed on routine contrast-enhanced CT (CECT) images obtained during the portal venous phase using new response criteria. MATERIALS AND METHODS: Standard CECT examinations of patients with metastatic clear cell RCC on first-line sunitinib or sorafenib therapy (n = 84) were retrospectively evaluated using Mass, Attenuation, Size, and Structure (MASS) Criteria; Response Evaluation Criteria in Solid Tumors (RECIST); Size and Attenuation CT (SACT) Criteria; and modified Choi Criteria. The objective response to therapy was compared with clinical outcomes including time to progression (TTP) and disease-specific survival. The Kaplan-Meier method was used to estimate survival functions. RESULTS: A favorable response according to MASS Criteria had a sensitivity of 86% and specificity of 100% in identifying patients with a good clinical outcome (i.e., progression-free survival of > 250 days) versus 17% and 100%, respectively, for RECIST partial response. The objective categories of response used by MASS Criteria-favorable response, indeterminate response, and unfavorable response-differed significantly from one another with respect to TTP (p < , log-rank test) and disease-specific survival (p < , log-rank test). CONCLUSION: Assessment of metastatic RCC target lesions on CECT for changes in morphology, attenuation, size, and structure by MASS Criteria is more accurate than response assessment by SACT Criteria, RECIST, or modified Choi Criteria. Furthermore, the use of MASS Criteria for imaging response assessment showed high interobserver agreement and may predict disease outcome in patients with metastatic RCC on targeted therapy. Smith AD, Shah SN, Rini BI, Lieber ML, Remer EM. Morphology, Attenuation, Size, and Structure (MASS) criteria: assessing response and. predicting clinical outcome in metastatic renal cell carcinoma on antiangiogenic targeted therapy. AJR Am J Roentgenol Jun;194(6):")
16
“An agent which does not produce an appreciable objective clinical improvement … cannot be expected to prolong life…” Karnofsky and Burchenal, 1949

17
Change from baseline in tumour measurement (%)*
Sorafenib - phase III TARGET 76% Tumour shrinkage in patients treated with sorafenib 150 100 50 –50 –100 –150 Placebo Sorafenib Tumour growth Change from baseline in tumour measurement (%)* No change 76% 25% Il grafico evidenzia per ogni paziente i cambiamenti dal basale delle dimensioni del tumore secondo i criteri RECIST. La riduzione della massa tumorale è stata osservata nel 76% dei pazienti trattati con sorafenib e nel 25% dei pazienti con placebo. Sorafenib riduce la massa tumorale tre volte di più rispetto a placebo. Tumour shrinkage The data presented here are based on a May 2005 analysis, and differ from data presented at ASCO 2005 *Investigator-assessed measurements Escudier B, et al. N Engl J Med 2007;356:125–34
* No change. 76% 25% Il grafico evidenzia per ogni paziente i cambiamenti dal basale delle dimensioni del tumore secondo i criteri RECIST. La riduzione della massa tumorale è stata osservata nel 76% dei pazienti trattati con sorafenib e nel 25% dei pazienti con placebo. Sorafenib riduce la massa tumorale tre volte di più rispetto a placebo. Tumour shrinkage. The data presented here are based on a May 2005 analysis, and differ from data presented at ASCO *Investigator-assessed measurements. Escudier B, et al. N Engl J Med 2007;356:125–34.")
18
Maximum % Change in Target Lesions and Objective Response Rate*
100% Everolimus Placebo 75% 50% 25% 0% −25% Best Response n (%) PR (2) Stable (67) PD (21) NE (11) Best Response n (%) PR Stable (32) PD (53) NE (14) −50% −75% −100% NE = not evaluable * Central Radiology Review
 PR 5 (2) Stable 185 (67) PD 57 (21) NE 30 (11) Best Response n (%) PR 0 Stable 45 (32) PD 74 (53) NE 20 (14) −50% −75% −100% NE = not evaluable. * Central Radiology Review.")
19
Necessario fare riferimento a criteri:
Valutazione dello stato di malattia in corso di trattamento con targeted therapies Necessario fare riferimento a criteri: Diagnostica strumentale Clinici Laboratorio

20
Criteri clinici Esame obiettivo Performance status
Sintomi tumore-correlati Perdita di peso Consumo di analgesici Qualità di vita del paziente

21
Key Factors for Successful Therapy Management in mRCC
Dosing Side-effect Management Optimum Efficacy Treatment Duration Therapy management Specific clinical management strategies have emerged as being essential for the optimal use of targeted agents for mRCC1–3 Therapy management describes the implementation of these strategies, which focus on three key interlinked areas:1–3 Dosing Treatment duration Proactive side effect management References 1. Hutson TE, et al. Oncologist 2008 2. Négrier S, Ravaud A. Eur J Cancer Suppl 2007 3. Bhojani N, et al. Eur Urol 2008 Schedule 21

22
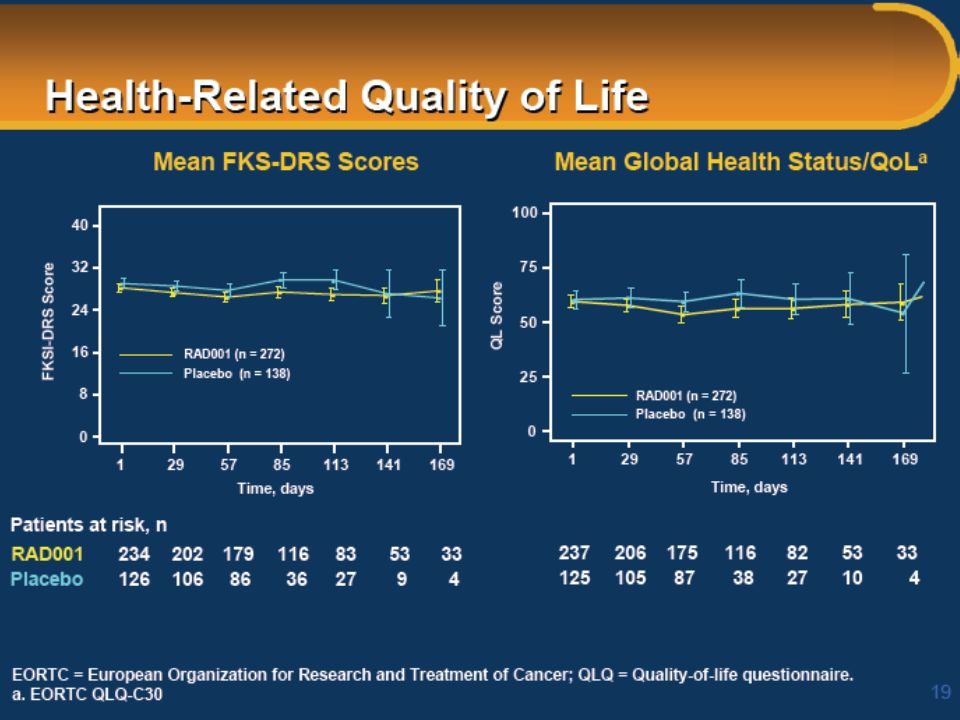
Proportion of patients not yet deteriorated (%)
Sorafenib Significantly Prolongs Time To Health-Status Deterioration vs Placebo (TARGET Trial) 100 75 50 25 Sorafenib Placebo Censored observation Proportion of patients not yet deteriorated (%) Median time to health status deterioration: 91 vs 60 days; p<0.0001 Treatment days from randomisation Bukowski R, et al. Am J Clin Oncol 2007;30:220–7 22 22
 Sorafenib. Placebo. Censored observation. Proportion of patients not yet deteriorated (%) Median time to health status deterioration: 91 vs 60 days; p< Treatment days from randomisation. Bukowski R, et al. Am J Clin Oncol 2007;30:220–")
24
Criteri di laboratorio
Emocromo completo Funzionalità epatica Funzionalità renale LDH Calcemia Tossicità o progressione di malattia?

25
Quando finisce una prima linea di trattamento ?

26
In assenza di una sicura progressione obiettiva, i criteri clinici che depongono per un beneficio per il paziente, devono sempre orientare verso la prosecuzione del trattamento con l’agente target in corso E viceversa….

27
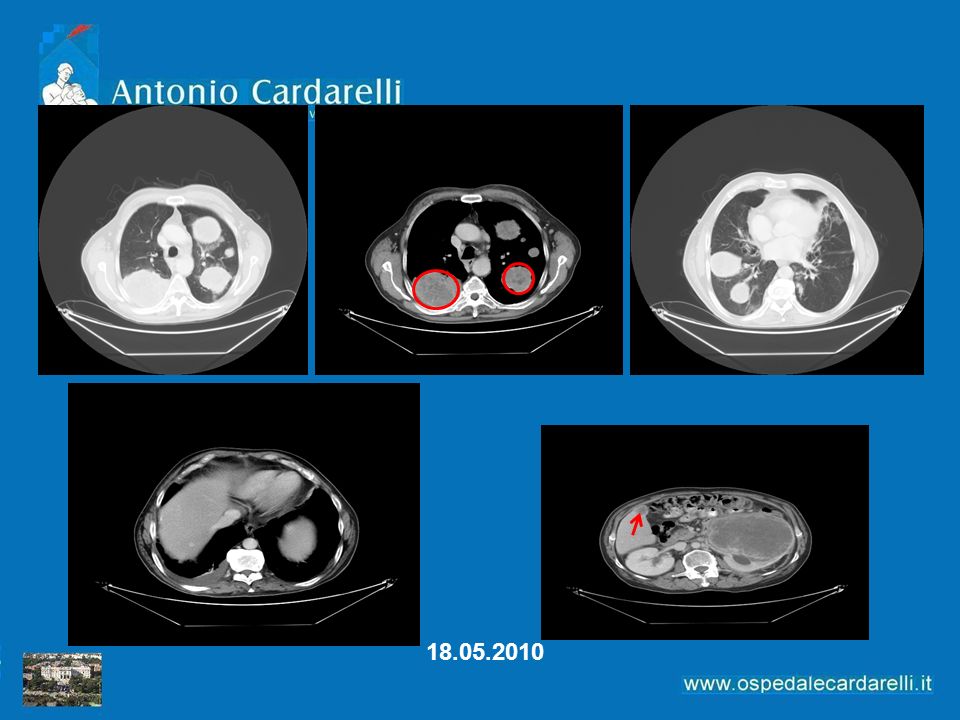
Case Study Sintomi all’esordio Ematuria Anemia Dolori addominali
Calo ponderale Astenia Dispnea Il paziente viene trasportato a braccia alla visita

28
Emoglobina: 9.0 gr/dl LDH 920 PS: sec Karnofsky 70% Pluri-metastatico

30
PET TOTAL BODY

31
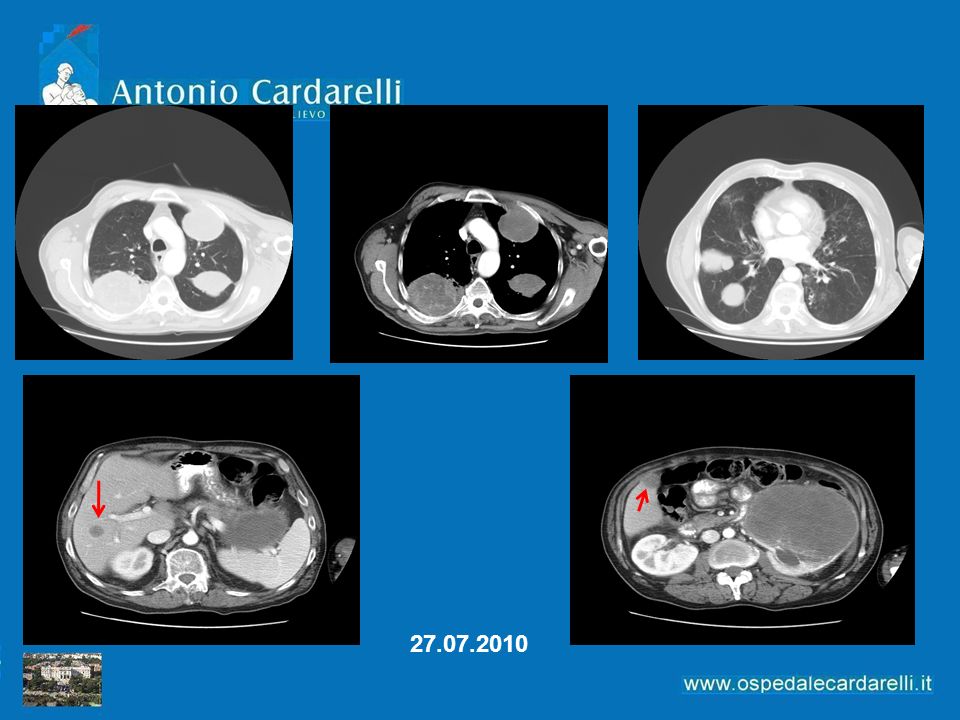
Maggio 2010 Praticati due cicli di Sutent Netto miglioramento delle condizioni cliniche Molto ridotto il dolore addominale Astenia quasi assente Hgb 11 g/dl Calcemia 8.6 mg/dl LDH 650 Karnofsky 80%

34
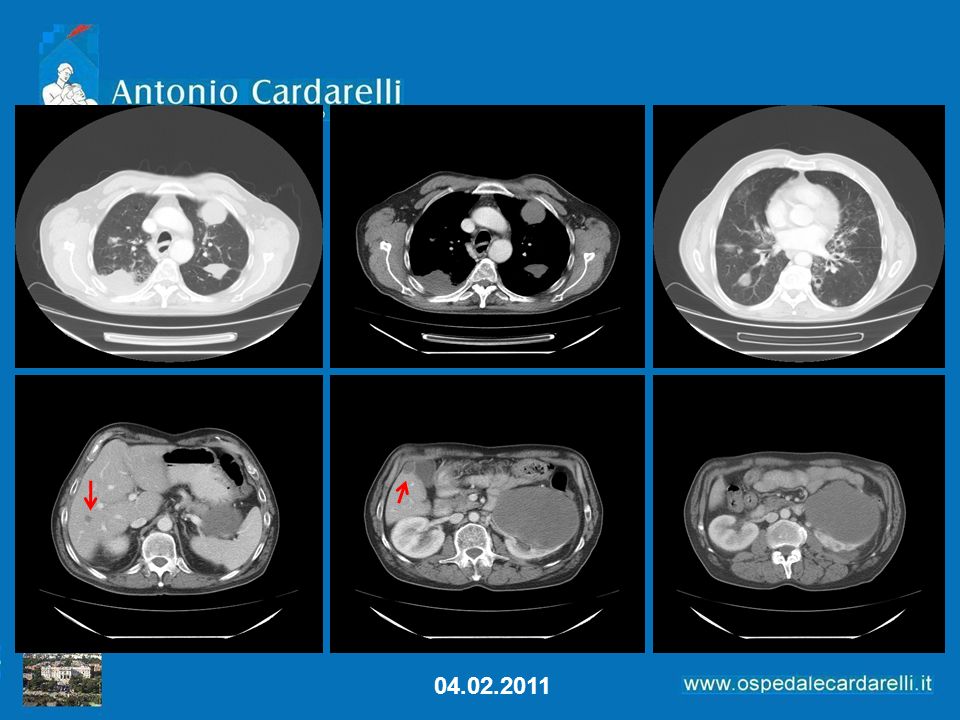
Inizia la riduzione

Presentazioni simili