Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Azienda Ospedaliera Sant’Andrea
Paolo Marchetti Oncologia Medica II Facoltà di Medicina e Chirurgia Sapienza Università di Roma Azienda Ospedaliera Sant’Andrea Roma La terapia di supporto

2
Azienda Ospedaliera Sant’Andrea
Paolo Marchetti Oncologia Medica II Facoltà di Medicina e Chirurgia Sapienza Università di Roma Azienda Ospedaliera Sant’Andrea Roma La simultaneous care!

3
Oggi… La tutela della salute = prodotto
L’assistenza sanitaria = servizio il malato = utente l’ospedale = azienda lo Stato, definisce, eroga, paga e controlla le prestazioni. ma è corretto definire la salute come un prodotto o servizio e la persona malata come cliente o utente?

4
Significant unmet needs
Significant unmet needs are those needs that patients identify as both important and unsatisfied. The range of unmet need, and the kinds of patients who are more likely to claim unmet need, should be carefully identified. K. Soothill et al., Supportive Care in Cancer, 2001

5
Simultaneous care in oncology
Unmet needs in cancer patients

6
Significant unmet needs
The NHS Cancer Plan [2000] has highlighted the need to streamline cancer services ‘around the needs of the patient’ and to provide ‘the right professional support and care as well as the best treatments’. However, the real question is whether the overall needs of cancer patients are actually being met. K. Soothill et al., Supportive Care in Cancer, 2001

7
Number of unmet needs K. Soothill et al., Supportive Care in Cancer, 2001

8
Significant need and unmet need Top 18 items
K. Soothill et al., Supportive Care in Cancer, 2001

10
Ministero della Salute PIANO ONCOLOGICO NAZIONALE 2010/2012

11
WHAT IS PERSONALIZED HEALTHCARE?
Medical practices that are targeted to individuals based on their specific genetic code in order to provide a tailored approach. The goal of personalized health care is to improve health outcomes and the health care delivery system, as well as the quality of life of patients everywhere.

12
Every Tumor is Unique! Mutations Are Random.
Every tumor develops a unique antigenic fingerprint. 10-8 per bp per cell division cycle on 6 x 109 bp = thousands to millions of unique mutations

13
Every Patient is Unique! Problems Are Random.
Every patient develops a unique individual fingerprint. thousands of unique problems!

14
Leaving the era of the “median results”, but targeting … what?
Patient: Genotype and polymorphisms: role of SNPs (CYP2D6) Tumor: refining the population target Proliferation gene Index (PGI): the best ? RE+/PG- population: does it mean something? EGFR: is or is not ? Triple negative BC: time for separating ?
 Tumor: refining the population target. Proliferation gene Index (PGI): the best RE+/PG- population: does it mean something EGFR: is or is not Triple negative BC: time for separating")
15
Tamoxifen activity is related to its metabolic pathway
80 variant alleles of cytocrome p450 2D6 Alleles 3,4 5 6 account for 99% of the variants Catalyzes metabolism of many common drugs Inhibited by flouxetina and paroxetina, frequently used by women assuming tamoxifen Tamoxifen metabolites have different anti-estrogenic power.

16
Practical implication
Very important remind: we deal not only with the tumor, but also with the host Similar observation with other anti-hormonal drugs (i.e. CYP19 and Letrozole, ASCO 2004) Confirmatory and prospective studies needed In the meanwhile, pay attention to all drugs you administer in combination with TAM, particularly new antidepressant implication in some type of drug resistance?
 Confirmatory and prospective studies needed. In the meanwhile, pay attention to all drugs you administer in combination with TAM, particularly new antidepressant. implication in some type of drug resistance")
17
Leaving the era of the “median results”, but targeting … what?
Patient: Genotype and polymorphisms: role of SNPs (CYP2D6) Tumor: refining the population target
 Tumor: refining the population target.")
18
Histologically they look like, but…
Pt 39 yrs, pre-menopausal T 2.2 cm, N (-), G1 ER (±)/PR(+), HER-2 (-) 09/2000: QUART FEC100 x LHRH-Tam Pt 47 yrs, pre-menopausal T 2.4 cm, N (-), G1 ER (±)/PR(+), HER-2 (-) 12/2003: QUART FEC100 x LHRH-Tam 10/2004: Metastatic disease 09/2005: NED Topoisomerase II By courtesy of S. Iacobelli, 2006
, G1. ER (±)/PR(+), HER-2 (-) 09/2000: QUART. FEC100 x 6 LHRH-Tam. Pt 47 yrs, pre-menopausal. T 2.4 cm, N (-), G1. ER (±)/PR(+), HER-2 (-) 12/2003: QUART. FEC100 x 6 LHRH-Tam. 10/2004: Metastatic disease. 09/2005: NED. Topoisomerase II By courtesy of S. Iacobelli,")
19
Cancer Biology Diversity of tumor subtypes: time for separating patients and treatments? Going inside to cancer biology can help clinicians?

20
Targeting Dysregulated Pathways With Novel Agents

21
Circulating Tumor Cells at First Follow-Up Predict Progression-Free Survival
100% 90 % 80 % 70 % 60 % 50 % 40 % 30 % 20 % 10 % 0 % <5 CTC (n=114), ~7.0 months ≥5 CTC (n=49), ~2.1 months First follow-up (3-4 wk), n=163, Logrank p < 0.001 Percent probability of progression-free survival ~2.1 months ~7.0 months Slide 4.30 Ideally, we would like to not only predict progression-free survival at baseline but also be able to predict whether therapy affected this progression-free survival. To test whether this was viable, the Hayes group drew blood at various intervals throughout therapy. They found that at about one month after the initiation of new systemic therapy, patients with greater than five circulating tumor cells had a progression-free survival rate of 2.1 months, suggesting that their initial therapy was probably not going to work. However, participants with five or less circulating tumor cells had a progression-free survival rate of about seven months. Time from baseline (weeks) CTC = circulating tumor cells Cristofanilli M et al. N Engl J Med 2004;351(8):
, ~7.0 months. ≥5 CTC (n=49), ~2.1 months. First follow-up (3-4 wk), n=163, Logrank p < Percent probability of progression-free survival. ~2.1 months. ~7.0 months. Slide Ideally, we would like to not only predict progression-free survival at baseline but also be able to predict whether therapy affected this progression-free survival. To test whether this was viable, the Hayes group drew blood at various intervals throughout therapy. They found that at about one month after the initiation of new systemic therapy, patients with greater than five circulating tumor cells had a progression-free survival rate of 2.1 months, suggesting that their initial therapy was probably not going to work. However, participants with five or less circulating tumor cells had a progression-free survival rate of about seven months Time from baseline (weeks) CTC = circulating tumor cells. Cristofanilli M et al. N Engl J Med 2004;351(8):")
23
Challenges of cancer treatment
The key goals of cancer treatment remain to Cure patients Improve overall survival Improve quality of life Identify novel targets and therapeutics Provide more tailored, individualized treatment

25
Leaving the era of the “median results”, but targeting … what?
Patient Tumor The patient with a cancer!

26
How Accurate Is Clinician Reporting of Chemotherapy Adverse Effects?
100 38 65 77 65 70 17 30 60 80 60 Percentage 40 20 It is quite accurate, however, for nausea, vomiting, and diarrhea, which are expected after chemotherapy. By comparison, 77% of patients reporting dyspnea were not identified by the physician as having it. To understand some of this cardiotoxicity, more vigilance is needed toward the symptoms that could relate to it. Fatigue Pain Dyspnea Insomnia Anorexia Nausea/ Vomiting Diarrhea Constipation Physician identified Physician missed J Clin Oncol. 2004; 22: Slamon D. SABCS General Session I.

27
Percezione dei sintomi: un obiettivo comune?

28
ESMO takes a stand on supportive and palliative care
Make alleviation of pain and other symptoms a high priority Medical oncologist must be expert with the evaluation and management of pain and other symptoms Cancer center should provide supportive and palliative care as part of the basic basket of services. Sottolineare i termini usati “takes a stand” “must be expert” (Ann Oncol 14: 1335, 2003)
")
29
Bridging the Divide: Integrating Cancer-Directed Therapy and Palliative Care
We must take symptom management a priority at diagnosis, throughout treatment, during periods without treatment, and finally, at the end of life We need all of these effort and more to traverse the divide that now exists between palliative care and cancer-directed therapy. Sottolineare Tutte le fasi della malattia Unire ciò che ora è diviso Integrazione piuttosto che sequenza Continuità piuttosto che separazione (JL Malin, JCO 22: 3438, 2004)
")
30
“Doc, I’m tired…”

31
Fatigue Agreement and disagreement between patients and clinicians. E. Basch et al., Lancet Oncol 2006

32
Survival According to the Underlying Cause of Cardiomyopathy
1.00 Peripartum 0.75 1% Idiopathic Due to doxorubicin therapy Proportion of Patients Surviving 0.50 Due to ischemic heart disease As of 2002, the most common therapeutics associated with cardiomyopathy are the anthracyclines. They account for only approximately 1% of adult cardiomyopathy with a particularly adverse outcome of approximately 50% at 2 years. Due to infiltrative myocardial disease 0.25 Due to HIV infection 0.00 5 10 15 Years Felker GM, et al. N Engl J Med. 2000;342:

33
43. 7% of Medical Oncologists used multiple symptoms tools and 37
43.7% of Medical Oncologists used multiple symptoms tools and 37.9% used symptom specific tools; 58.9% used some instrument to assess pain. More than a third of the respondents (35.5%) used patient-tailored protocols. No statistical differences were found regarding region of residency, availability of consultants in pain therapy and/or palliative care, colleagues with main interest on palliative care, and beds dedicated to palliative care.
 used patient-tailored protocols. No statistical differences were found regarding region of residency, availability of consultants in pain therapy and/or palliative care, colleagues with main interest on palliative care, and beds dedicated to palliative care.")
36
BreakThrough Cancer Pain (BTcP)
")
37
Prevalence of BTcP The prevalence of BTcP may differ due to the stage of the cancer and the methodology of the different studies, but it remains an important problem in cancer patients who are already receiving treatment for their pain. Up to 95% of patients with cancer suffer from BTcP. Zeppetella G, Ribeiro MD. Pharmacotherapy of cancer-related episodic pain. Expert Opin Pharmacother 2003

38
Terapia dei sintomi

39
Nutrition assessment Weight loss at the time of diagnosis has been associated with decreased survival and reduced response to treatment. Dewys WD, Am J Med, 1980 Treatment of nutrition-related symptoms reverse weight loss in in 50-88% of cancer patients. Ottery FD, Proc Am Soc Clin Oncol, 1998 Assessment with Patient-Generated Subjective Global Assessment (PG-SGA), anthropometric and laboratory data or Bioelectrical Impedance Analysis (BIA– unavailable in most ambulatory settings) Sungurtekin H, Nutrition, 2004 Lukaski HC, Ann N Y Acad Sci, 1999
, anthropometric and laboratory data or Bioelectrical Impedance Analysis (BIA– unavailable in most ambulatory settings) Sungurtekin H, Nutrition, Lukaski HC, Ann N Y Acad Sci,")
40
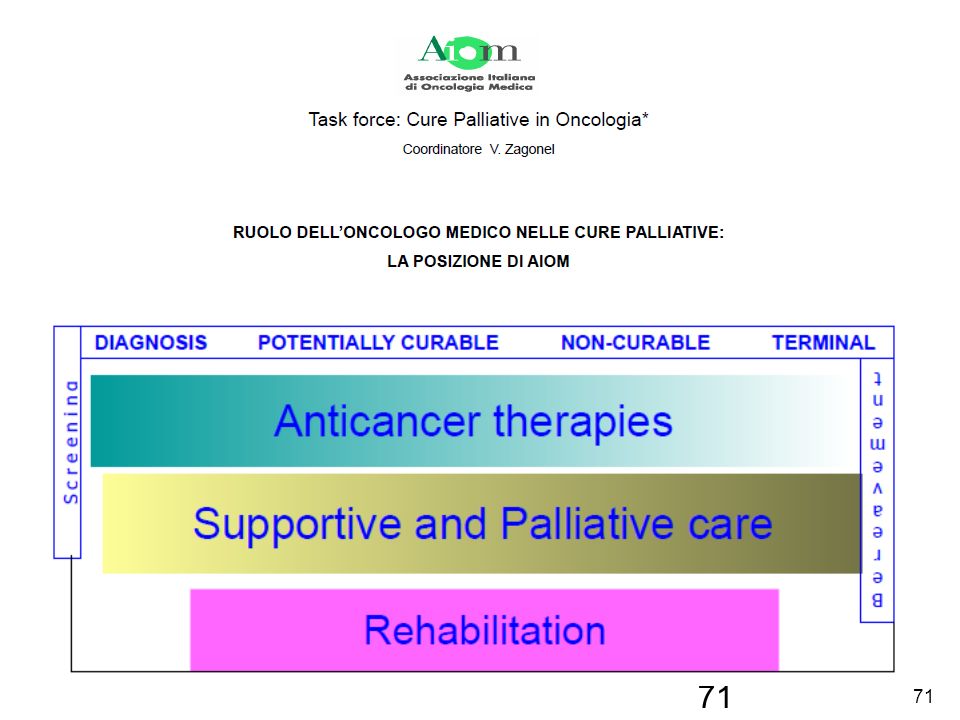
Cancer rehabilitation is the process that assists the cancer patients to obtain maximal physical, social, psychological and vocational functioning within the limits created by the disease and its treatment

41
Optimization of physical functioning Vocational counselling
The rehabilitation approach to cancer treatment originates with National Cancer Act (NCA) of 1971 In 1972, the NCI sponsored the National Cancer Rehabilitation Planning Conference and developed training programs and research projects to identify 4 objectives in cancer rehabilitation: Psychosocial support Optimization of physical functioning Vocational counselling Optimization of social functioning
 of In 1972, the NCI sponsored the National Cancer Rehabilitation Planning Conference and developed training programs and research projects to identify 4 objectives in cancer rehabilitation: Psychosocial support. Optimization of physical functioning. Vocational counselling. Optimization of social functioning.")
42
why do women fear breast cancer more than any other health risk?
One out of two women in the United States will die from heart disease or stroke. Women also believe ovarian cancer is their biggest "cancer" threat when it is actually lung cancer that kills 70,000 women a year.

43
The risk was perceived three times higher than it actually was.
Breast Cancer Risk:Perception vs Reality Nearly 90% of Women Overestimate Breast Cancer Risk When asked to estimate the average lifetime chance of developing breast cancer, nine out of 10 women overestimated the risk. The risk was perceived three times higher than it actually was. P. Ubel et al., Patient Education and Counseling, 2005

44
Breast Cancer Risk:Perception vs Reality Nearly 90% of Women Overestimate Breast Cancer Risk
Estimating Risk Roughly one in eight women will eventually develop breast cancer. In other words, a woman has a 13% chance of developing breast cancer at some point during her life. Numbers don't give context: asking the patients to estimate their own risk can help put the actual risk in perspective. We shouldn't just throw numbers at patients without giving them some context for those numbers! P. Ubel et al., Patient Education and Counseling, 2005

45
One Size Doesn't Fit All!

46
Comprendere ilPaziente!
Quanto è grave la sua malattia? Quanto è curabile la sua malattia?

47
The risk perception attitude (RPA) framework
Four attitudinal groups based on their perceptions of risk and beliefs of personal efficacy. Responsive (high risk, high efficacy) Avoidance (high risk, low efficacy) Proactive (low risk, high efficacy) Indifference (low risk, low efficacy) These groups differ from each other in their self-protective motivations and behaviors.
 Avoidance (high risk, low efficacy) Proactive (low risk, high efficacy) Indifference (low risk, low efficacy) These groups differ from each other in their self-protective motivations and behaviors.")
48
Comunicare in oncologia Cosa?
Il tipo di trattamento Gli effetti collaterali Le risposte attese La prognosi

49
… ma anche I risultati delle rivalutazioni clinico-strumentali
Assenza di tumore o non evidenza di ripresa di malattia? Angoscia per i prossimi controlli o falsa tranquillità per i successivi 6/12 mesi?

50
… ma anche Variazioni nel tipo di farmaco usato
Paziente asintomatica, senza progressione di malattia, preoccupata di eventuali nuovi effetti collaterali. Paziente sintomatica, preoccupata che il cambio di farmaco sia dovuto ad un fallimento della precedente terapia

51
Caso clinico Paziente di 70 anni, operata per un ca della mammella da 2 anni, in trattamento adiuvante (precauzionale) con tamoxifen. Sulla base dei risultati con gli IA, deve sostituire il tamoxifen con un IA. La Paziente non ha avuto alcun effetto collaterale con il tamoxifen. Informata dei possibili effetti collaterali degli IA, è spaventata. Rinuncerà ai benefici della nuova terapia?

52
l’informazione sulla diagnosi di tumore secondo le risposte dei caregiver
Al paziente è stato detto che aveva un tumore? % (95% CI) SI 37 (34-40) NO, ma lo sapevano 29 (27-32) NO e non lo sapevano 26 (24-29) NO, non so se sapevano 7 (6-10) M. Costantini et al., Ann Oncol, 2006
 SI. 37. (34-40) NO, ma lo sapevano. 29. (27-32) NO e non lo sapevano. 26. (24-29) NO, non so se sapevano. 7. (6-10) M. Costantini et al., Ann Oncol,")
53
l’informazione sulla diagnosi di tumore secondo le risposte dei caregiver
Quando la prognosi è diventata sfavorevole, è stato comunicato al paziente? % (95% CI) SI 13 (10-15) NO, ma lo sapevano 50 (46-54) NO e non lo sapevano 27 (24-30) NO, non so se sapevano 10 (8-14) M. Costantini et al., Ann Oncol, 2006
 SI. 13. (10-15) NO, ma lo sapevano. 50. (46-54) NO e non lo sapevano. 27. (24-30) NO, non so se sapevano. 10. (8-14) M. Costantini et al., Ann Oncol,")
54
ricevono più informazione
l’informazione sulla diagnosi di tumore secondo le risposte dei caregiver chi sono i pazienti che ricevono più informazione residenti nel nord Italia più giovani con titolo di studio elevato con tumori testa-collo o mammario con aspettativa di vita lunga alla diagnosi M. Costantini et al., Ann Oncol, 2006

55
Il punto di vista dei pazienti
Il punto di vista dell’opinione pubblica M. Costantini, 2008

56
% di pazienti oncologici a cui è stata comunicata la diagnosi di tumore nei diversi studi italiani
dal 1985 al 2005! M. Costantini, 2008

57
Comunicare in oncologia Quando?
Al momento della prima visita, delineando tutte le varie possibilità terapeutiche in funzione dei possibili risultati? In maniera continuativa, durante le diverse fasi dela evoluzione clinica della malattia?

58
Comunicare in oncologia A chi?
Ogni tipo di comunicazione deve essere attuata tenendo ben presente la persona malata, nella sua complessità ed interezza, valutando le sue specifiche caratteristiche umane, i suoi problemi e le sue preoccupazioni familiari, le sue incertezze e le sue paure sociali, insieme alle caratteristiche cliniche della neoplasia.

59
Caso clinico Paziente di 41 anni, importante dirigente di industria.
Viene operata per una carcinoma della mammella ad alto rischio e deveessere sottoposta a chemioterapia e ad ormonoterapia per 5 anni. … ma aveva deciso di avere dei figli con il suo nuovo compagno!

60
A chi? La familiarità e la predisposizione genetica.

61
Caso clinico Donna di 36 anni, 3 figlie, M5 e O3, viene operata per un carcinoma ovarico. Paura per le figlie. Interessi conflittuali con i familiari.

62
Comunicare in oncologia Come?
Numeri, percentuali, numeri… Facile, poco coinvolgente, apparentemente molto tecnico. Ma le percentuali si riferiscono a popolazioni e non al singolo paziente che sied di fronte a noi!

63
La comunicazione in oncologia
La comunicazione in oncologia. Necessità clinica o inutile complicazione assistenziale?

64
Study of unmet needs in symptomatic veterans with advanced cancer
The total number of unmet needs was predictive of QOL. Shirley S. Hwang et al., 2004

65
End of life issues and spiritual histories
Patients facing end-of-life issues have spiritual concerns that may have an impact on their medical decision-making. Conclusion: Spiritual concerns of many patients facing end-of-life decisions are not being addressed. King DE e al (2003) End of life issues and spiritual histories South medical Journal 96:
 End of life issues and spiritual histories South medical Journal 96:")
66
Religious struggle as a predictor of mortality among medically ill elderly patients.
Although church attendance has been associated with a reduced risk of mortality, no study has examined the impact of religious struggle with an illness on mortality. Certain forms of religiousness may increase the risk of death. Elderly ill men and women who experience a religious struggle with their illness appear to be at increased risk of death, even after controlling for baseline health, mental health status, and demographic factors. Pargament Kl e al (2001) Religious struggle as a predictor of mortality among medically ill elderly patients. Archives Internal Medicine. 161:
 Religious struggle as a predictor of mortality among medically ill elderly patients. Archives Internal Medicine. 161:")
67
Breast cancer in the family
Children's perceptions of their mother's cancer and its initial treatment .

68
Breast cancer in the family
Family fatigue

69
Cancer survivors with unmet needs were more likely to use complementary and alternative medicine.
Despite advancements in cancer care, cancer survivors continue to experience a substantial level of physical and emotional unmet needs. Cancer survivors who experienced unmet needs within the existing cancer treatment and support system were more likely to use CAM to help with cancer problems. JJ Mao et al., J Cancer Surviv. 2008

70
Simultaneous care Terapia di supporto

Presentazioni simili





 Università degli Studi, Pavia (founder) IRCCS Fondazione.>")
 064825120 - fax.>")
















