Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Riabilitazione Neurologica (2)
PROGETTO FORMATIVO SPECIALE / C.L. FISIOTERPIA Riabilitazione Neurologica (2)
")
2
Cosa è la riabilitazione neurologica?
Barnes, J Neurol Neurosurg Psychiat, 2003

3
Due principi sono fondamentali:
RIABILITAZIONE NEUROLOGICA Due principi sono fondamentali: La riabilitazione è un processo attivo, distinto dal miglioramento spontaneo (recupero o convalescenza) e dal trattamento terapeutico (a pazienti non partecipanti). Gli obbiettivi perseguiti dalla riabilitazione sono centrati sulla persona
 e dal trattamento terapeutico (a pazienti non partecipanti). Gli obbiettivi perseguiti dalla riabilitazione sono centrati sulla persona.")
4
What is a model of illness?
Illness refers to all aspects of ill health personal, family, society, etc Need a framework to analyse illness To describe it Need a model To plan rational interventions

5
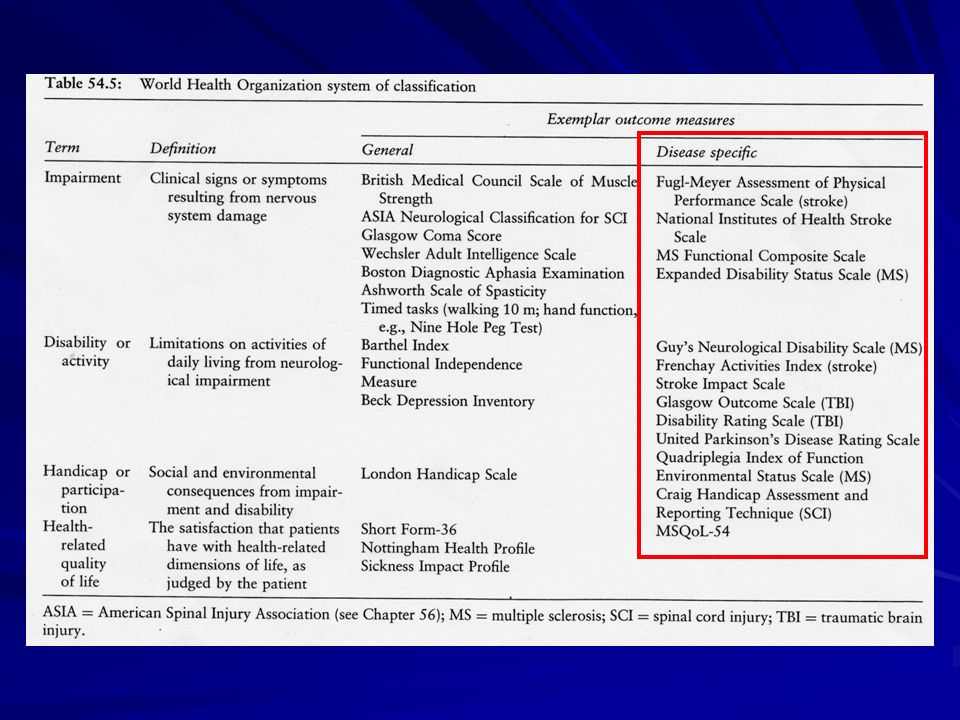
WHO ICF model of illness
The framework can be seen as a systems analytic approach, considering illness as a hierarchy of systems A MODEL In this model, illness comprises interacting systems which may have emergent properties

6
Rivisitata ICIDH ICF:
WHO ICF International Classification of Functioning, Disability and Health Rivisitata ICIDH ICF: Aggiunta fattori di contesto : fisici (archittetonici, vestiti, etc) personali (experienze, attitudini, etc) sociali (familgia/amicizie, cultura, etc) Cambio parole (e concetti ?) disabilità -> attività handicap -> participazione Concetto globale di ‘functioning’
 personali (experienze, attitudini, etc) sociali (familgia/amicizie, cultura, etc) Cambio parole (e concetti ) disabilità -> attività. handicap -> participazione. Concetto globale di ‘functioning’")
7
Interactions between the components of ICF (WHO 2001)
")
8
Well-being WHO ICF Model of illness Four Levels Three Contexts
Organ (pathology) Personal Person (impairment) Physical Person in environment Behaviour (activities) Social Person in society Social position (Participation) Well-being
 Personal. Person (impairment) Physical. Person in environment. Behaviour (activities) Social. Person in society. Social position (Participation) Well-being.")
9
Riabilitazione neurologica: elementi per la definizione
Scopi della riabilitazione Processo della riabilitazione Caratteristiche di un servizio di riabilitazione

10
Riabilitazione neurologica: elementi per la definizione
Scopi della riabilitazione Processo della riabilitazione Caratteristiche di un servizio di riabilitazione

11
Rehabilitation of patients with cognitive deficits
Dr Derick T Wade * Professor in Community Rehabilitation Faculteit der Geneeskunde, Universiteit Maastricht * Professor in Neurological Disability Oxford Centre for Enablement Windmill Road, Oxford OX3 7LD Effectiveness of Rehabilitation for Cognitive Deficits Cardiff 17 – 19 September, 2002

12
Rehabilitation aims (outcome)
To maximise patient participation in society maximise role function in community maximise status in community To maximise patient well-being somatic and emotional achieving satisfaction (adaptation) To minimise stress on & distress of relatives
 To minimise stress on & distress of relatives.")
13
ICF e Obiettivi della Riabilitazione
Massimizzare il repertorio comportamentale Ottimizzando i contesti personale, fisico, sociale Minimizzando le menomazioni tutte, ma specialmente quelli con impatto sulle attività Minimizzando il danno d’organo (pathology) Ottimizzando le opportunità di interazione sociale
 Ottimizzando le opportunità di interazione sociale.")
14
ICF e Interventi Danno d’organo Impairments
Diagnosi e trattamento della malattia Diagnosi e trattamento delle complicanze Diagnosi e trattamento di malattie incidentali Impairments Cognitivi (neglect, word finding) Altro deficit (motorio scrittura) Impedire peggioramenti (eccesso di farmaci!!)
 Altro deficit (motorio scrittura) Impedire peggioramenti (eccesso di farmaci!!)")
15
ICF e Interventi Attività Partecipazione
Esercizio delle funzioni colpite, secondo gli obiettivi del paziente, in rapporto all’ambiente quotidiano Partecipazione Organizzare opportunità per inserimento sociale

16
ICF e Interventi Contesto personale Contesto fisico Contesto sociale
Aumentare la fiducia in se stesso Ridurre i timori di insuccesso Contesto fisico Uso di ausili cognitivi (diari, sistemi di allarme-ricordo, post-it) Contesto sociale Lavoro stabile Inserimentonella comunità
 Contesto sociale. Lavoro stabile. Inserimentonella comunità.")
17
Aims of the rehabilitation process
Maximise patients’ participation in their social setting Minimise the risk of medical complication (e.g. contractures) Minimise the pain and distress experienced by the patient (maximise quality of life) Minimise the distress of and stress on the patient's family and/or carers DT Wade e BA de Jong, BMJ 2000;320:
 Minimise the pain and distress experienced by the patient (maximise quality of life) Minimise the distress of and stress on the patient s family and/or carers. DT Wade e BA de Jong, BMJ 2000;320:")
18
Approaches of the rehabilitation process
Approaches that reduce disability Approaches designed to acquire new skills and strategies, which will maximise activity Approaches that help to alter the environment, both physical and social, so that a given disability carries with it minimal consequent handicap Barnes, J Neurol Neurosurg Psychiat, 2003

19
Riabilitazione neurologica: elementi per la definizione
Scopi della riabilitazione Processo della riabilitazione Caratteristiche di un servizio di riabilitazione

20
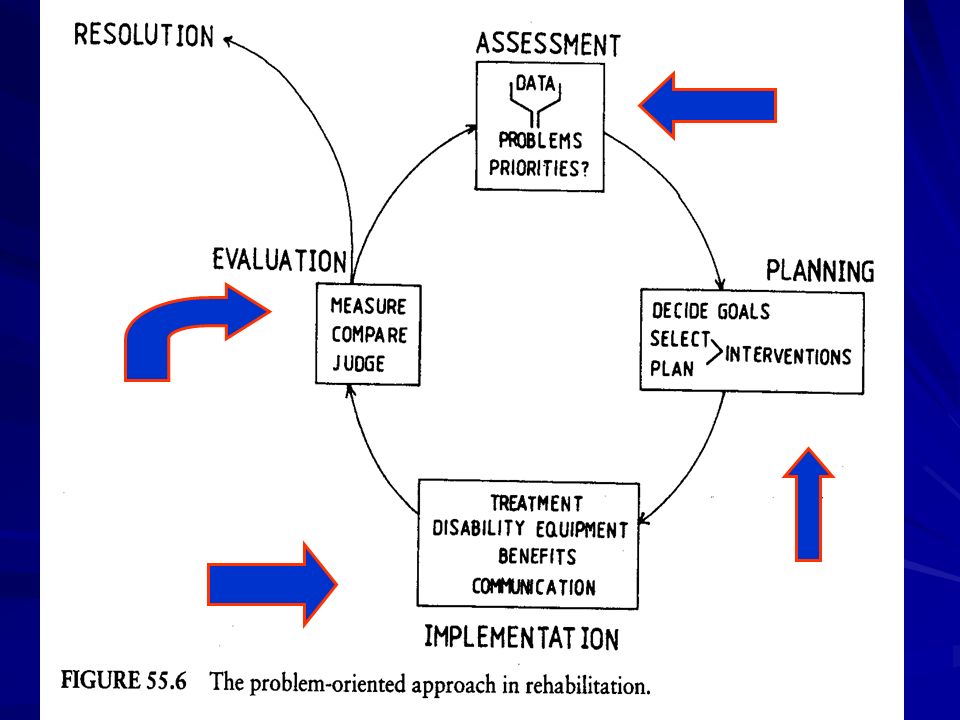
Rehabilitaton Process
Rehabilitation is a reiterative, active, educational, problem solving process focused on a patient's behaviour (disability/activity), with the following components: Assessment: the identification of the nature and extent of the patient's problems and the factors relevant to their resolution Goal setting Intervention, which may include either or both of treatments, which affect the process of change; support, which maintains the patient's quality of life and his or her safety Evaluation: to check on the effects of any intervention DT Wade e BA de Jong, BMJ 2000;320:
, with the following components: Assessment: the identification of the nature and extent of the patient s problems and the factors relevant to their resolution. Goal setting. Intervention, which may include either or both of. treatments, which affect the process of change; support, which maintains the patient s quality of life and his or her safety. Evaluation: to check on the effects of any intervention. DT Wade e BA de Jong, BMJ 2000;320:")
22
Rehabilitaton Process
To work in partnership with the disabled person and their family To give accurate information and advice about the nature of the disability, natural history, prognosis, etc To listen to the needs and perceptions of the disabled person and their family To work with other professional colleagues in an interdisciplinary fashion To liaise as necessary with key carers and advocates To assist with the establishment of realistic rehabilitation goals, which are both appropriate to that person’s disability and their family, social, and employment needs Barnes, J Neurol Neurosurg Psychiat, 2003

23
ICF e misure di risultato

25
ICF e assessment

26
MISURE DI DISABILITA’/ATTIVITA’
Indice di Barthel (BI) Misura di Indipenza Funzionale (FIM)
 Misura di Indipenza Funzionale (FIM)")
27
MISURA DI INDIPENDENZA FUNZIOALE

29
Le scale, come “misuratori di risultato” (outcome measure), devono soddisfare i seguenti criteri:
Validità: deve essere una scala che misura ciò che si vuole misurare; Affidabilità: lo strumento deve essere accurato, stabile nel tempo, riproducibile; Sensibilità: la scale deve essere in grado di cogliere variazioni clinicamente significative; Semplicità: semplice da impiegarsi; Comunicabilità: lo strumento deve essere facilmente compreso anche dai non specialisti; Utilità clinica

30
Goal setting The process of rehabilitation is set around the establishment of goals. The first goal to be set is the long term strategic aim. Once a realistic and achievable long term goal has been established then the smaller steps needed to achieve that goal are determined. The goals must be precise and should be: Specific Measurable Achievable Relevant Time limited SMART

31
Riabilitazione neurologica: elementi per la definizione
Scopi della riabilitazione Processo della riabilitazione Caratteristiche di un servizio di riabilitazione

32
Characteristics of a rehabilitation service
It comprises a multi-disciplinary group (team) of people who focus their attention on a patient's disability, and: Work together towards common goals with each patient; Involve and educate the patient and family in the process; Have relevant expertise and experience (knowledge and skills); and Can, between them, resolve most of the common problems faced by their patients
 of people who focus their attention on a patient s disability, and: Work together towards common goals with each patient; Involve and educate the patient and family in the process; Have relevant expertise and experience (knowledge and skills); and. Can, between them, resolve most of the common problems faced by their patients.")
33
The multidisciplinary team centered around patient and caregiver

34
Recent advances in rehabilitation DT Wade, BA de Jong
Recent advances in rehabilitation DT Wade, BA de Jong BMJ 2000;320;

35
Outcome measures for clinical rehabilitation trials: Impairment, function, quality of life, or value? Wade DT: Am J Phys Med Rehabil, 2003;82(Suppl):S26–S31. Outcome: What Is It? Nel campo della ricerca riabilitativa il termine “outcome” indica è una “variazione attesa” in un parametro o in uno “stato”. Outcome è il nuovo stato in cui il paziente si viene a trovare come risultato di un intervento (programma riabilitativo). Nella riabilitazione vi sono spesso molti inteverventi nel tempo e i relativi “outcomes” non sono sempre ovvi.
. Nella riabilitazione vi sono spesso molti inteverventi nel tempo e i relativi outcomes non sono sempre ovvi.")
36
Outcome measures for clinical rehabilitation trials: Impairment, function, quality of life, or value? In un paziente con ictus, tutti gli “outcomes” della tabella possono essere pertinenti in ragione di cosa si vuole valutare e perché.

37
Outcome measures for clinical rehabilitation trials: Impairment, function, quality of life, or value? Wade DT: Am J Phys Med Rehabil, 2003;82(Suppl):S26–S31. In rehabilitation, outcome is more difficult to measure because usually several outcomes are relevant, relevant outcomes are affected by multiple factors in addition to treatment, and even good measures rarely reflect the specific interest of any individual patient or member of the rehabilitation team, leading to some dissent.

38
Comparison of physician outcome measures and patients' perception of benefits of inpatient neurorehabilitation BMJ 2002; 324:1493 Rating scales of impairment, disability, and handicap are often used but only partially reflect the rehabilitation process, tending to be "physician oriented." Physician outcome measures relate poorly with patients' perceived benefit from inpatient neurorehabilitation as measured on a visual analogue scale. The low correlation of visual analogue scale with the functional outcome measures indicates that these measures reflect only a small part of patients' perceived benefit.

39
Measurement in the Neurorehabilitation based on the ICF

40
Determine if the measures you find
- are self completed by the patient (patient reported outcomes) or - performance-based, rated by a therapist
 or. - performance-based, rated by a. therapist.")
41
Are costs associated with the use of the measure?
How long does it take to complete/ administer the measure? How much equipment is required? Is the measure available in the language of the patient?

42
General Standards for Use of Measures
Validity Reliability Responsiveness Practicability

43
Validity If the test does indeed measure what it is intended to measure, then we can say that the test is valid Psychology Glossary Most important consideration, when selecting a measure Is regarded as the extent to which a test measures what it is intended to measure? Gold standard

44
Reliability It refers to the extent to which a test or other instrument is consistent in its measures Psychology Glossary Maybe defined as "the degree to which a measure is free from random error" Guidelines for how much is "good enough" are suggested to range from ccorrelations of 0.70 and more S. Schädler 2007

45
Reliability Intrarater reliability Interrater reliability
is the degree to which scores on a measure obtained by one trained observer agree with the scores obtained when the same observer reapplies the measure at another time Interrater reliability is the degree to which scores on a measure obtained by one trained observer agree with the scores obtained by another observer

46
Threads of Reliability
Fatigue Boredom Distraction Untrained raters Sh. Wood-Dauphinee 2005

47
Responsiveness Sensitivity to change
The ability of the measure to assess and quantify clinically important change Two things are very important: - the minimal detectable change (MDC) - the minimal clinical important difference (MCID)
 - the minimal clinical important. difference (MCID)")
48
Practicability For which population? Easy to complete
Manual (test instruction) Costs (material, license) Education (time, costs)
 Costs (material, license) Education (time, costs)")
49
What kind of outcome measures should be chosen?
For assessment/ problem analysis For treatment planning For outcome measure For prognosis

50
Recent advances in rehabilitation DT Wade, BA de Jong
Recent advances in rehabilitation DT Wade, BA de Jong BMJ 2000;320;

51
Medicina basata sulle evidenze e Riabilitazione

52
La medicina basata sulle prove (evidenze scientifiche) è:
Integrazione di: Esperienza clinica individuale Miglior evidenza clinica esterna derivata da una ricerca sistematica della letteratura esistente Risorse disponibili Valori ed attese del paziente (Sackett 1997)
")
53
Archie Cochrane ( ) “It is surely a great criticism of our profession that we have not organized a critical summary, by specialty or subspecialty, adapted periodically, of all relevant randomized controlled trials.”

54
Archie Cochrane ( ) Monografia “Effectiveness and Efficiency” (1971) Randomized clinical trials (RCT) Evidence-based Medicine (EBM)
")
55
Evidence-based practice for stroke
The conventional evidence-based practice approach to evaluate interventions has been divided into three components: efficacy : has it been shown to work in ideal circumstances?; effectiveness : has it been shown to have an important effect across a range of settings and circumstances?; and efficiency : has it been shown to provide value for money? The lancet neurology Vol 8 April 2009

56
Efficacia versus Efficienza

57
Basic elements of clinical decision making

58
Quali sono le caratteristiche degli RCTs inclusi nella revisione?
Metodi: Randomizzazione, Cecità Partecipanti: tipo di pazienti, Storia di malattia Interventi: Dose, durata del trattamento, Co-trattamenti Outcomes

59
AAN evidence classification scheme for a therapeutic article
Class II Class III Class IV

60
The Validity of Cognitive Rehabilitation
Strategies for Evaluating Effectiveness and Translating Research to Clinical Practice Keith D. Cicerone, Ph.D.

61
REVIEW ARTICLE Evidence-Based Cognitive Rehabilitation: Recommendations for Clinical Practice Keith D. Cicerone et al., Arch Phys Med Rehabil 2000; 81:

62
Levels of Evidence Class I
Well designed, prospective, randomized controlled trials Well designed, prospective studies with ‘quasi-random’ assignment to treatment conditions (Ia)
")
63
Levels of Evidence Class II Prospective, non-randomized cohort studies
Retrospective, non-randomized case control studies Clinical series with well-designed controls allowing between-subject comparisons

64
Levels of Evidence Class III
Clinical series without concurrent controls Case studies with appropriate single-subject methodology and measurements

65
Practice Parameters Practice Standard
Based on at least one, well-designed Class I study with adequate sample, or Overwhelming Class II evidence, that provides good evidence to support the effectiveness of the intervention

66
Practice Parameters Practice Guideline
Based on well-designed Class II studies that provide fair evidence to support the effectiveness of the intervention

67
AAN system for translation of evidence to recommendations
Rating of recommendations Translation of evidence to recommendations A = Established as useful/predictive or not useful/predictive for the given condition in the specified population Level A rating requires at least one convincing class I study or at least two consistent, convincing class II studies B = Probably useful/predictive or not useful/predictive for the given condition in the specified population Level B rating requires at least one convincing class II study or overwhelming class III evidence C = Possibly useful/predictive or not useful/predictive for the given condition in the specified population Level C rating requires at least two convincing class III studies U = Data inadequate or conflicting. Given current knowledge, test, predictor is unproven.

68
Practice Parameters Practice Option
Based on Class II or Class III studies, with additional grounds to support the effectiveness of the intervention, but with unclear clinical certainty

69
BIF/AIFA, 2006

70
META-ANALISI: combinare cosa con cosa ?
DIVERSITA’ CLINICA Gli studi affrontano lo stesso problema? Gli studi sono diversi? Es. per: - luogo di ricovero e tipo di assistenza prestata - tipo di pazienti (età, sesso, gravità,…) - trattamenti (farmaco, dose, durata, frequenza,…) - definizione e misure degli esiti - durata del follow-up
 - trattamenti (farmaco, dose, durata, frequenza,…) - definizione e misure degli esiti. - durata del follow-up.")
71
META-ANALISI: combinare cosa con cosa ?
DIVERSITA’ METODOLOGICA RCT a gruppi paralleli o crossover Qualità degli studi (per es. randomizzazione e modalità di assegnazione ai gruppi di trattamento, oppure cecità della misurazione degli outcomes Analisi (per es. ‘intenzione al trattamento’ vs. ‘trattati’ )
")
72
ETEROGENEITA’ STATISTICA
META-ANALISI: combinare cosa con cosa ? ETEROGENEITA’ STATISTICA Vi è una diversità dei risultati degli studi maggiore di quella che ci si potrebbe aspettare per effetto del caso

73
Questa linea orizzontale è la scala che misura l’effetto del
Questi titoli indicano quale confronto è stato fatto e qual’è l’outcome di interesse Questa linea verticale nel centro è dove il trattamento e il controllo hanno lo stesso effetto- non vi è differenza tra i due Copyright © Mediss 2001 All rights reserved Questa linea orizzontale è la scala che misura l’effetto del trattamento. A destra la scala è <1 e significa che il trattamento ha reso meno probabile la morte.

74
Per ogni studio vi è un id I dati di ogni studio sono qui, divisi nel
gruppo dei trattati e dei controlli Questo è il peso % assegnato a questo studio nell’analisi aggregata Statistica utilizzata Dati numerici del grafico Ad ogni studio è assegnato un quadrato posto dove i dati misurano l’effetto. L’area del quadrato è proporzionale al peso % dello studio. La % di peso assegnata dipende dalla varianza dello studio (dimensioni e numero di eventi osservati). La linea orizzontale rappresenta l’intervallo di confidenza, una misura che ci indica di quanto il risultato può variare per effetto del caso. Quanto più l’intervallo di confidenza è ampio, tanto meno siamo confidenti nell’effetto osservato. Confidence intervals are calculated from a number known as a standard error. Standard errors are companions of all estimates. They describe the extent to which an estimate might be wrong due to random error. The smaller the standard error the more certain we are about the estimate. To get a feel for standard errors it is helpful to know that 95% confidence intervals are obtained by taking the estimate and creating limits that are 1.96 standard errors below it and 1.96 standard errors above it. Thus an estimate may be wrong by about a standard error, but to be 95% confident about where the true effect lies, we go roughly 2 standard errors either side. La varianza è il quadrato dello standard errore Copyright © Mediss 2001 All rights reserved
. La linea orizzontale rappresenta l’intervallo di confidenza, una misura che ci indica di quanto il risultato può variare per effetto del caso. Quanto più l’intervallo di confidenza è ampio, tanto meno siamo confidenti nell’effetto osservato. Confidence intervals are calculated from a number known as a standard error. Standard errors are companions of all estimates. They describe the extent to which an estimate might be wrong due to random error. The smaller the standard error the more certain we are about the estimate. To get a feel for standard errors it is helpful to know that 95% confidence intervals are obtained by taking the estimate and creating limits that are 1.96 standard errors below it and 1.96 standard errors above it. Thus an estimate may be wrong by about a standard error, but to be 95% confident about where the true effect lies, we go roughly 2 standard errors either side. La varianza è il quadrato dello standard errore. Copyright © Mediss All rights reserved.")
75
L’analisi aggregata dei risultati di tutti gli studi è rappresentata con un diamante (media pesata).
Se l’intervallo di confidenza include l’unità significa che non abbiamo trovato una differenza statisticamente significativa tra i due trattamenti. Copyright © Mediss 2001 All rights reserved

76
Evidence-Based PM&R? Arch Phys Med Rehabil Vol78, November 1997

77
PM&R journals 9 major impact factor–rated Physical Medicine and Rehabilitation (PM&R) journals: Archives of Physical Medicine and Rehabilitation, American Journal of Physical Medicine and Rehabilitation, Physical Therapy, Scandinavian Journal of Rehabilitation Medicine, Journal of Rehabilitation Research and Development, Supportive Care in Cancer, Prosthetics and Orthotics International, Journal of Orthopaedic and Sports Physical Therapy, Journal of Manipulative and Physiological Therapeutics

78
Evidence-Based Practice and the Limits of Rational Rehabilitation Keith D. Cicerone, Ph.D Arch Phys Med Rehabil 2005; 86: E’ difficile applicare i principi della “evidence-practice-medicine” alla ricerca in riabilitazione (contemporaneità di interventi e di diversi “outcome”, problemi etici nella randomizzazione) ma è una via “obbligata”. Vanno rispettati 3 “pilastri”: attenta considerazione delle migliori “prove” scientifiche disponibili esperienza clinica e valutazione personale considerazione dei valori e delle convinzioni del paziente. Il “rispetto” del paziente pone comunque dei problemi da risolvere
 ma è una via obbligata . Vanno rispettati 3 pilastri : attenta considerazione delle migliori prove scientifiche disponibili. esperienza clinica e valutazione personale. considerazione dei valori e delle convinzioni del paziente. Il rispetto del paziente pone comunque dei problemi da risolvere.")
79
GRAZIE PER L’ATTENZIONE

Presentazioni simili

 064825120 - fax.>")







>")








>")
