Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Il Disturbo d’Ansia Indotto da Sostanze nel DSM IV-TR e nell’ICD-10
Scuola Superiore di Formazione in Medicina. “Terza Scuola Invernale di Psichiatria sull’analisi del DSM IV.TR – I Disturbi d’Ansia” Zafferana Etnea (CT), MASSIMO CLERICI Dipartimento di Neuroscienze e Tecnologie Biomediche Università degli studi di Milano BIcocca
, MASSIMO CLERICI. Dipartimento di Neuroscienze. e Tecnologie Biomediche. Università degli studi di Milano BIcocca.")
2
….l’evoluzione del problema
Calves' Heads and Brains, or A Phrenological Lecture (London: Published for the Artist, 1826) Henry Thomas Alken ( )
 Henry Thomas Alken ( )")
3
…aree di confine in psichiatria… la “doppia diagnosi”, oggi
Abuso e Dipendenza da sostanze devono, inevitabilmente, essere considerati un disturbo del cervello, quanto ogni altro disturbo mentale Organizzazione Mondiale della Sanità (WHO), 2004
,")
4
COMORBIDITY AND SUBSTANCE USE DISORDERS (Clark & MCClanahan, 1998)
NEGLI ULTIMI VENTI ANNI LA NOZIONE DI “DOPPIA DIAGNOSI” E’ STATA COMUNEMENTE IMPIEGATA PER INDICARE UN GENERICO CONCETTO DI “DISTURBO CORRELATO A SOSTANZE SOVRAPPOSTO AD ALTRI DISTURBI PSICHIATRICI, O VICEVERSA” SCARSAMENTE APPROFONDITO RIMANEVA - NELLA CONDIZIONE DI DD - LO STUDIO DI ASPETTI RILEVANTI QUALI: LE EVENTUALI DIFFERENZE TRA EFFETTI PSICHICI DELLE SOSTANZE E SINTOMI DEL/DEI DISTURBI PSICHIATRICI CONCOMITANTI - LE QUESTIONI EZIOPATOGENETICHE GLI EFFETTI A LUNGO TERMINE DELL’USO DI SOSTANZE NEI DISTURBI MENTALI

5
LE POLITICHE IN MATERIA DI SOSTANZE IN EUROPA
LE POLITICHE IN MATERIA DI SOSTANZE IN EUROPA. LA SITUAZIONE DALL’OSSERVATORIO DI LISBONA IL CONSUMO DI DROGHE NON ACCENNA A DIMINUIRE: NEI GIOVANI RISULTA, IN PERCENTUALE, DOPPIO RISPETTO AGLI ADULTI SI STIMA CHE UNA PERSONA SU CINQUE IN EUROPA ABBIA PROVATO ALMENO UNA VOLTA NELLA SUA VITA UNA DROGA ILLECITA I TOSSICODIPENDENTI “CRONICI” RAPPRESENTANO SOLO LO 0,5% DELLA POPOLAZIONE EUROPEA

6
Are Alcohol Figures Comparable between E-U Countries?

7
Studi epidemiologici di popolazione
EPIDEMIOLOGICAL CATCHMENT AREA SURVEY (ECA, anni 80-92) Il 20% di chi ha assunto almeno una volta una droga ha poi sviluppato un DCS A partire da una diagnosi primaria di disturbo psichiatrico il 15% circa mostra co-diagnosi di disturbo correlato a sostanze (DCS) per droghe e il 30% circa per alcool
 Il 20% di chi ha assunto almeno una volta una droga ha poi sviluppato un DCS. A partire da una diagnosi primaria di disturbo psichiatrico il 15% circa mostra co-diagnosi di disturbo correlato a sostanze (DCS) per droghe e il 30% circa per alcool.")
8
Progress in Addiction Medicine and Psychiatry (el-Guebaly, 2005; Section on Addiction Psychiatry – WPA) NEGLI ULTIMI 20 ANNI, L’ALLARGAMENTO DEL MERCATO HA SENZA DUBBIO FACILITATO L’INGRESSO NEI SERVIZI DI POPOLAZIONI CLINICHE A MAGGIORE VULNERABILITA’ BIOPSICOSOCIALE IN PRECEDENZA NON INTERESSATE DAL PROBLEMA: CIO’ HA SENSIBILMENTE COMPLICATO LE COSE

9
BACKGROUND L’esperienza italiana nel campo dei disturbi correlati a sostanze è abbastanza diversa da quella della maggior parte degli altri paesi One of the most peculiar elements of Italian health culture in the addiction field has been an ideologically oriented approach to addiction as a phenomenon, and to the organization of related services (Carrà G. & Clerici M, 2003; 2006) Addiction; Am J Addiction
 Addiction; Am J Addiction.")
10
…. l’organizzazione diagnostica attuale e i suoi limiti
Calves' Heads and Brains, or A Phrenological Lecture (London: Published for the Artist, 1826) Henry Thomas Alken ( )
 Henry Thomas Alken ( )")
11
Lo spettro dell’ansia comorbidità disturbo sintomi
Ansia fisiologica Uso di sostanze e malattie organiche In campo psichiatrico nessun sintomo è patognomonico di uno specifico disturbo 11

12
13 categorie diagnostiche
I disturbi d’ansia nel DSM IV DSM II (1968): 3 categorie diagnostiche DSM IV TR (2000): 13 categorie diagnostiche 12
: 3 categorie diagnostiche. DSM IV TR (2000): 13 categorie diagnostiche. 12.")
13
I disturbi d’ansia (DSM IV-TR)
Attacco di panico Agorafobia Disturbo di panico senza agorafobia Agorafobia senza anamnesi di disturbo di panico Fobia specifica (semplice) Fobia sociale Disturbo ossessivo - compulsivo Disturbo post-traumatico da stress Disturbo acuto da stress Disturbo d’ansia generalizzato Disturbo d’ansia dovuto a una condizione medica Disturbo d’ansia indotto da sostanze Disturbo d’ansia non altrimenti specificato 13
 Fobia sociale. Disturbo ossessivo - compulsivo. Disturbo post-traumatico da stress. Disturbo acuto da stress. Disturbo d’ansia generalizzato. Disturbo d’ansia dovuto a una condizione medica. Disturbo d’ansia indotto da sostanze. Disturbo d’ansia non altrimenti specificato. 13.")
14
Sindromi nevrotiche, legate a stress e somatoformi (ICD-10)
SINDROMI FOBICHE (agorafobia, fobie speciali, fobie specifiche/isolate, altre, non specificate) ALTRE SINDROMI ANSIOSE (sindrome da attacchi/ansia episodica parossistica, sindrome ansiosa generalizzata, sindrome mista ansioso-depressiva, altre sindromi ansiose miste, altre specificate, non specificate) SINDROME OSSESSIVO-COMPULSIVA (prevalenti ruminazioni e pensieri ossessivi, prevalenti atti compulsivi/rituali ossessivi, associazione di pensieri ossessivi ed atti compulsivi, altra, non specificata) REAZIONE A GRAVI STRESS E SINDROMI DA DISADATTAMENTO (reazione acuta da stress, sindrome post-traumatica da stress, sindromi da disadattamento, altra, non specificata) 14
 ALTRE SINDROMI ANSIOSE (sindrome da attacchi/ansia episodica parossistica, sindrome ansiosa generalizzata, sindrome mista ansioso-depressiva, altre sindromi ansiose miste, altre specificate, non specificate) SINDROME OSSESSIVO-COMPULSIVA (prevalenti ruminazioni e pensieri ossessivi, prevalenti atti compulsivi/rituali ossessivi, associazione di pensieri ossessivi ed atti compulsivi, altra, non specificata) REAZIONE A GRAVI STRESS E SINDROMI DA DISADATTAMENTO (reazione acuta da stress, sindrome post-traumatica da stress, sindromi da disadattamento, altra, non specificata) 14.")
15
Sindromi nevrotiche, legate a stress e somatoformi (ICD-10)
SINDROMI DISSOCIATIVE (da conversione: amnesia dissociativa, fuga dissociativa, stupore dissociativo, sindrome di trance e di possessione, sindromi dissociative motorie, convulsioni dissociative, anestesia e perdita sensoriale dissociative, sindromi dissociative/da conversione miste, altre, non specificate) SINDROMI SOMATOFORMI (sindrome di somatizzazione, sindrome somatoforme indifferenziata, sindrome ipocondrica, disfunzione vegetativa somatoforme, sindrome somatoforme da dolore persistente, altra, non specificata) ALTRE SINDROMI NEVROTICHE (nevrastenia, sindrome di depersonalizzazione-derealizzazione, altre specificate, non specificate) 15
 SINDROMI SOMATOFORMI (sindrome di somatizzazione, sindrome somatoforme indifferenziata, sindrome ipocondrica, disfunzione vegetativa somatoforme, sindrome somatoforme da dolore persistente, altra, non specificata) ALTRE SINDROMI NEVROTICHE (nevrastenia, sindrome di depersonalizzazione-derealizzazione, altre specificate, non specificate) 15.")
16
Sindromi e disturbi psichici e comportamentali dovuti all’uso di sostanze psicoattive (ICD-10)
SINDROMI E DISTURBI PSICHICI E COMPORTAMENTALI DOVUTI ALL’USO DI…. un quarto e quinto elemento vanno aggiunti al codice per specificare la condizione clinica: Intossicazione acuta Uso dannoso Sindrome di dipendenza Stato di astinenza Stato di astinenza con delirium Sindrome psicotica Sindrome amnesica Sindrome o disturbo psichico residuo o ad esordio tardivo Sindromi e disturbi psichici e comportamentali di altro tipo Sindromi e disturbi psichici e comportamentali non specificati 16

17
Quali sistemi di classificazione per la DD?
ICD-10 Viene classificata nel gruppo diagnostico denominato”Sindromi e Disturbi psichici e comportamentali dovuti all’uso di sostanze psicoattive” Prevede per ogni sostanza 10 sottoclassi, descrittive delle caratteristiche del quadro clinico Viene inquadrata sulla base di un principio eziopatogenetico, dove l’assunzione di sostanze sarebbe primaria e il disturbo psicopatologico secondario CRITICHE stabilisce a priori un nesso di causalità; l’abuso/dipendenza non viene considerato di per se stesso come disturbo psichiatrico indipendente DSM IV: il sistema più usato in campo di ricerca Disturbi da uso di sostanze (abuso, dipendenza) Disturbi indotti da sostanze (intossicazione, astinenza, disturbi sindromici secondari) Entrambi questi tipi di disturbo possono coesistere con qualsiasi altro disturbo di asse I CRITICHE tende a produrre diagnosi multiple; la doppia diagnosi finisce per avere un approccio eccessivamente medico e psichiatrico.
 Disturbi indotti da sostanze (intossicazione, astinenza, disturbi sindromici secondari) Entrambi questi tipi di disturbo possono coesistere con qualsiasi altro disturbo di asse I. CRITICHE. tende a produrre diagnosi multiple; la doppia diagnosi finisce per avere un approccio eccessivamente medico e psichiatrico.")
18
Considerazioni sui disturbi come presenti dal DSM IV
Positive: Migliorate conoscenze sui disturbi da un punto di vista fisiopatologico Negative: Alto livello di comorbidità tra le varie forme Overlapping dei sintomi Frammentazione delle forme cliniche Gradi di risposta terapeutica non specifici 18

19
PER QUANTO STABILE LA DIAGNOSI?
• 44.3% mantengono la diagnosi di DCS • 40.2% hanno un disturbo dell’umore o d’ansia attuale • 66% mantengono la loro diagnosi di Asse II Verheul, R. Kranzler, H.R., Poling, J et al, (2000) Axis 1 and Axis II disorders in alcoholics and drug addicts: fact or artifact? J. Stud Alcohol 61,
 Axis 1 and Axis II disorders in alcoholics and drug addicts: fact or artifact J. Stud Alcohol 61,")
20
Europ - ASI ASI – Addiction Severity Index European Official Version (Kokkevi & Hartgers, 1995; Pozzi & Tempesta, 1995) of Addiction Severity Index ASI McLellan AT, Kusher H, Metzger D, Peters R, Smith I, Grisson G, & Pettinati H (1992) The fifth edition of the Addiction Severity Index: Historical critique and normative data; Journal of Substance Abuse Treatment, 9,
 of Addiction Severity Index ASI. McLellan AT, Kusher H, Metzger D, Peters R, Smith I, Grisson G, & Pettinati H (1992) The fifth edition of the Addiction Severity Index: Historical critique and normative data; Journal of Substance Abuse Treatment, 9,")
21
Maudsley Addiction Profile-MAP
MAP - European Official Version Marsden, J., Nizzoli, U., Corbelli, C., Margaron, H., Torres, M., Prada De Castro, I., Stewart, D. & Gossop, M. (2000) New European instruments for treatment outcome research: reliability of the Maudsley Addiction Profile and treatment perceptions questionnaire in Italy, Spain and Portugal. European Addiction Research, 6, 115–122
 New European instruments for treatment outcome research: reliability of the Maudsley Addiction Profile and treatment perceptions questionnaire in Italy, Spain and Portugal. European Addiction Research, 6, 115–122.")
22
….la rilevanza epidemiologica
Calves' Heads and Brains, or A Phrenological Lecture (London: Published for the Artist, 1826) Henry Thomas Alken ( )
 Henry Thomas Alken ( )")
23
Percent of persons with mental illnesses who also will develop a substance use disorder
Co-occurring disorder Up to 50%

24
Disturbi indotti da sostanze
I: Intossicazione A: Astinenza P: probabile I Disturbi indotti da sostanze delirium demenza amnesia psicotici umore ansia sessuali sonno Alcol I/A P I Amfetam. - Cannabis Cocaina Allucinog. Inalanti Oppiacei PCP Ansiolitici A DSM IV, TR

25
Structured clinical interviews
Co-occurrence between psychiatric disorders and substance use disorders in the general population Structured clinical interviews US ECA 20.291 DSM III NCS 8.098 DSM III R NLAES 42.826 DSM IV NESARC 43.093 EUROPE NEMESIS 1996 7.076 OSLO 2.066

26
Life-time prevalence – ECA-study N = 20.000
II Substance use disorders Bipolar disorders 61% Schizofrenia 47% Panic disorders 36% Compulsive disorders 33% Affective disorders 32% Anxiety disorders 15%

27
Pazienti psichiatrici che utilizzano sostanze
III Lifetime Prevalence and Odds Ratios of Mental Disorders by Substance Use Disorder: ECA Alcohol Drug Comorbid Disorder % O.R. % O.R. Any mental Schizophrenia Affective Anxiety Antisocial Merikangas, 2004

28
Independent disorder (DSM IV)
National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) 12-month prevalence, n = Comorbidity substance use disorders and independent mood and anxiety disorders Independent disorder (DSM IV) Persist more than 4 weeks after intoxication or Psychiatric disorder established before abuse. Grant et al., Arch Gen Psychiatry 2004
 12-month prevalence, n = Comorbidity substance use disorders and independent mood and anxiety disorders. Independent disorder (DSM IV) Persist more than 4 weeks after intoxication or. Psychiatric disorder established before abuse. Grant et al., Arch Gen Psychiatry")
29
NESARC 12-month prevalence
Mood disorders % Anxiety disorders % SUD (Substance Use Disorders) % alcohol dependence % alcohol abuse % drug dependence % drug abuse % Grant et al., Arch Gen Psychiatry 2004
 9.4 % alcohol dependence 3.8 % alcohol abuse 4.7 % drug dependence 0.6 % drug abuse 1.4 % Grant et al., Arch Gen Psychiatry")
30
NESARC 12-month prevalence Independent mood and anxiety disorders and substance use disorders
SUD YES No OR Mood disorders 8% 20% 2.8 ( ) Anxiety disorders 10% 18% 1.9 ( ) Grant et al., Arch Gen Psychiatry 2004
 Anxiety disorders. 10% 18% 1.9 ( ) Grant et al., Arch Gen Psychiatry")
31
Prevalence of SUD among persons with independent anxiety disorders
Any anxiety disorder 15% Panic disorder (with agoraphobia) 24% Social phobia % Specific phobia 14% Generalized anxiety syndrome 19%
 24% Social phobia 16% Specific phobia 14% Generalized anxiety syndrome 19%")
32
Prevalence of SUD among respondents seeking treatment for mood and anxiety disorders
Mood disorders Anxiety disorders Any SUD Alcohol use disorder Drug use disorder 21% 17% 8% 13% 7% Grant et al., Arch Gen Psychiatry 2004

33
Prevalence of mood or anxiety disorders among respondents seeking treatment for SUD
Alcohol use disorders Drug use disorders Mood disorders Anxiety disorders 41% 33% 60% 43% Grant et al., Arch Gen Psychiatry 2004

34
Conclusions Population studies
The life-time risk for having a substance use disorder is 2-4 times increased among persons with a life-time mental disorder Clinical studies In general, comorbidiy is more common among those seeking treatment than in population samples

35
Prevalence of Current Axis-I Disorders (Jellinek sample)
Depression Dysthymia Panic/Agoraphobia Social phobia Obsessive Compulsive Disorder Post Traumatic Stress Disorder Generalized Anxiety Disorder ADHD 18,5 % 31,9 % 21,0 % 16,0 % 3,4 % 5,9 % 25,2 % 15,8 % Kraanen et al., 2007

36
Prevalence of Co-morbidity (Jellinek sample)
High prevalence of co-current psychiatric disorders - 47% of schizophrenics % of anxiety disorders - 30% of in-patients in psychiatric hospitals 50% of patients treated for alcohol or drug dependence has a other psychiatric disorder (Axis-I and/or Axis-II) The numbers presented on this slide are from a current and standard textbook. Different figures are often presented by different sources due to issues such as the difference between lifetime and current prevalence, the clinical setting and the method of screening employed. There has been an increase in multiple diagnoses of alcohol, drug and mental disorders by physicians over the past two decades. It is felt that this increase is due to enhanced awareness by clinicians, deinstitutionalization and changing patterns of drug use in society. The most important message is that all physicians will see patients with addictions. These patients will have altered mental status and will require diagnostic clarification and appropriate management. THIS MUST BECOME COMMON PRACTICE!
 The numbers presented on this slide are from a current and standard textbook. Different figures are often presented by different sources due to issues such as the difference between lifetime and current prevalence, the clinical setting and the method of screening employed. There has been an increase in multiple diagnoses of alcohol, drug and mental disorders by physicians over the past two decades. It is felt that this increase is due to enhanced awareness by clinicians, deinstitutionalization and changing patterns of drug use in society. The most important message is that all physicians will see patients with addictions. These patients will have altered mental status and will require diagnostic clarification and appropriate management. THIS MUST BECOME COMMON PRACTICE!")
37
Are Specific Psychiatric Disorders Associated with Specific Substances
Are Specific Psychiatric Disorders Associated with Specific Substances? Percent of Patients Using Substance (Jellinek sample) Depression Panic/ Social phob ADHD Agoraphob
 Depression Panic/ Social phob ADHD. Agoraphob.")
38
Co-current Psychiatric Disorder (Jellinek sample)
Panic disorder/ agoraphobia and social phobia primarily associated with tranquilizers ADHD primarily associated with cocaine and opiate

39
Co-Occurring Disorders (Jellinek sample)
Health and social problems requiring costly care At risk for homelessness and incarceration Women are at risk of being victims of sexual abuse and domestic violence Parents with co-occurring problems risk encounters with child welfare

41
Relazione al Parlamento “sullo stato delle Tossicodipendenze in Italia” – anno 2006

42
Studio epidemiologico sulla comorbidità tra disturbi mentali e disturbi correlati all’uso di sostanze (droghe e/o alcool) nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy Allo stato attuale il tasso di risposta dei DSM è del 55%. La prevalenza di doppia diagnosi è 2,4 per 100 utenti. L’età media dei pazienti è 42 anni (range 19-75), l’80% di essi è maschio; la diagnosi psichiatrica principale più frequente è il disturbo di personalità (37%), seguito da psicosi schizofrenica (31%), psicosi affettiva (17%), disturbo nevrotico (9%) e altre diagnosi (6%). La droga principale di abuso è l’alcool; il 63 % dei pazienti è inoltre dipendente da almeno un’altra sostanza.
, l’80% di essi è maschio; la diagnosi psichiatrica principale più frequente è il disturbo di personalità (37%), seguito da psicosi schizofrenica (31%), psicosi affettiva (17%), disturbo nevrotico (9%) e altre diagnosi (6%). La droga principale di abuso è l’alcool; il 63 % dei pazienti è inoltre dipendente da almeno un’altra sostanza.")
43
Distribuzione DSM e prevalenza utenti con comorbidità per
Studio epidemiologico sulla comorbidità tra disturbi mentali e disturbi correlati all’uso di sostanze (droghe e/o alcool) nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy) Distribuzione DSM e prevalenza utenti con comorbidità per area geografica Area n° DSM aderenti Utenti DD per 100 utenti Nord 12 3.5 Centro 1 0.6 Sud 5 2.3 Totale 18 2.4
 nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy) Distribuzione DSM e prevalenza utenti con comorbidità per. area geografica. Area. n° DSM aderenti. Utenti DD per 100 utenti. Nord Centro Sud Totale")
44
Distribuzione per diagnosi psichiatrica
Studio epidemiologico sulla comorbidità tra disturbi mentali e disturbi correlati all’uso di sostanze (droghe e/o alcool) nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy) Distribuzione per diagnosi psichiatrica Diagnosi Totale % Psicosi schizofreniche ( ) e stati paranoidi ( ) 50 28.1 Psicosi affettive ( ) Altre psicosi non organiche ( ) 6 3.3 Disturbi nevrotici e somatoformi ( , 307) 22 12.4 Disturbi di personalità ( ) 178 100.0
 nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy) Distribuzione per diagnosi psichiatrica. Diagnosi. Totale. % Psicosi schizofreniche ( ) e stati paranoidi ( ) Psicosi affettive ( ) Altre psicosi non organiche ( ) Disturbi nevrotici e somatoformi ( , 307) Disturbi di personalità ( )")
45
Distribuzione per diagnosi e profili di utilizzo delle sostanze [1]
Studio epidemiologico sulla comorbidità tra disturbi mentali e disturbi correlati all’uso di sostanze (droghe e/o alcool) nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy) Distribuzione per diagnosi e profili di utilizzo delle sostanze [1] Profilo di utilizzo Psic. schizofreniche ( ) e stati paranoidi ( ) n=49 Psicosi affettive ( ) n=50 Altre psicosi non org. ( ) n=6 D. nevrotici e somatoformi ( , 307) n=22 D. Personalità ( ) n=50 Uso 23 (46.0) 25 (50.0) 1 (16.7) 2 (9.1) Abuso 44 (88.0) 38 (76.0) 8 (133.3) 18 (81.8) 63 (126.0) Dipendenza 19 (38.0) 28 (56.0) 7 (116.0) 35 (159.1) 25 (50.0) [1] Tra parentesi è riportata la percentuale del profilo di utilizzo calcolato sul totale di ogni diagnosi psichiatrica (è possibile che tale percentuale sia maggiore del 100% nei casi in cui il soggetto abusi contemporaneamente di più di una sostanza o sia dipendente da altre sostanze)
![Distribuzione per diagnosi e profili di utilizzo delle sostanze [1]](http://slideplayer.it/slide/590890/2/images/45/Distribuzione+per+diagnosi+e+profili+di+utilizzo+delle+sostanze+%5B1%5D.jpg "Studio epidemiologico sulla comorbidità tra disturbi mentali e disturbi correlati all’uso di sostanze (droghe e/o alcool) nei DSM italiani (PADDI Study - Psychiatric and Addictive Dual Disorders in Italy) Distribuzione per diagnosi e profili di utilizzo delle sostanze [1] Profilo di utilizzo. Psic. schizofreniche ( ) e stati paranoidi ( ) n=49. Psicosi affettive. ( ) n=50. Altre psicosi non org. ( ) n=6. D. nevrotici e somatoformi ( , 307) n=22. D. Personalità ( ) n=50. Uso. 23. (46.0) 25 (50.0) 1. (16.7) 2. (9.1) Abuso. 44. (88.0) 38. (76.0) 8. (133.3) 18. (81.8) 63. (126.0) Dipendenza. 19. (38.0) 28. (56.0) 7. (116.0) 35. (159.1) 25. (50.0) [1] Tra parentesi è riportata la percentuale del profilo di utilizzo calcolato sul totale di ogni diagnosi psichiatrica (è possibile che tale percentuale sia maggiore del 100% nei casi in cui il soggetto abusi contemporaneamente di più di una sostanza o sia dipendente da altre sostanze)")
46
Distribuzione per sostanza utilizzata (abuso o dipendenza) in base alla diagnosi [1]
Sostanza Utilizzata Psicosi schizofreniche ( ) e stati paranoidi ( ) n=49 Psicosi affettive ( ) n=50 Altre psicosi non organiche ( ) n=6 Disturbi nevrotici e somatoform ( , 307) n=22 Disturbi Person. ( ) n=50 Alcool 37 (74.0) 38(76.0) 4 (66.7) 17 (77.3) 33(66.0) Oppioidi 7 (14.0) 11 (22.0) 1 (16.7) 5 (22.7) 10(20.0) Cann.oidi 9 (18.0) 10 (20.0) 3 (50.0) 15 (30.0) Cocaina e Stimol. 5 (10.0) 4 (8.0) 2 (9.1) 13 (26.0) Allucinog. 1 (2.0) 0 (0.0) 1 (4.5) Barbitur. 2 (4.0) Altro [1] Tra parentesi è riportata la percentuale di uso della specifica sostanza all’interno di ciascun sottogruppo diagnostico
![Distribuzione per sostanza utilizzata (abuso o dipendenza) in base alla diagnosi [1]](http://slideplayer.it/slide/590890/2/images/46/Distribuzione+per+sostanza+utilizzata+%28abuso+o+dipendenza%29+in+base+alla+diagnosi+%5B1%5D.jpg "Sostanza. Utilizzata. Psicosi schizofreniche ( ) e stati paranoidi. ( ) n=49. Psicosi affettive. ( ) n=50. Altre psicosi non organiche ( ) n=6. Disturbi nevrotici e somatoform ( , 307) n=22. Disturbi. Person. ( ) n=50. Alcool. 37 (74.0) 38(76.0) 4 (66.7) 17 (77.3) 33(66.0) Oppioidi. 7 (14.0) 11 (22.0) 1 (16.7) 5 (22.7) 10(20.0) Cann.oidi. 9 (18.0) 10 (20.0) 3 (50.0) 15 (30.0) Cocaina e Stimol. 5 (10.0) 4 (8.0) 2 (9.1) 13 (26.0) Allucinog. 1 (2.0) 0 (0.0) 1 (4.5) Barbitur. 2 (4.0) Altro. [1] Tra parentesi è riportata la percentuale di uso della specifica sostanza all’interno di ciascun sottogruppo diagnostico.")
47
….gli aspetti clinici Calves' Heads and Brains, or
A Phrenological Lecture (London: Published for the Artist, 1826) Henry Thomas Alken ( )
 Henry Thomas Alken ( )")
48
DIAGNOSI E TRATTAMENTO
…le complesse relazioni tra psicopatologia e disturbi correlati a sostanze: un altro esempio “dell’uovo e della gallina”… from “evolutionistic ornithology” to treatment Meyer RE (ed), Psychopathology and Addictive Disorders, Guilford, New York, 1986
, Psychopathology and Addictive Disorders, Guilford, New York,")
49
Etiology of dual diagnosis: possible explanations
A causal relationship of the disorders: Are psychiatric symptoms cause or consequence of substance use problems? Disorders share common etiologic or risk factors, e.g. genetic predisposition, childhood trauma or neglect Self-medication of psychological symptoms that are related to previous trauma or neglect Use of ‘numbing’ substances to self-medicate emotional dysregulation - intense emotions and hyperarousal symptoms - associated with life-events exposure or mental disorders 49

50
L’auto-medicazione nei Disturbi di Asse I e II: fattori di rischio psicopatologici per i DCS?
Schizofrenia: riduzione dei sintomi negativi e positivi (stimolanti, cannabinoidi) Depressione, in particolare disturbo bipolare: stabilizzazione o amplificazione del tono dell’umore e “manipolazione delle sensazioni (oppiacei, cocaina) Disturbi di Personalità: superamento dell’isolamento e dell’insoddisfazione, vissuti a seguito dell’impairment psicosociale correlato al dp, mediante ricerca di alterazioni comportamentali e supporto fornito dall’inserimento in gruppi di pari più tolleranti (poliabuso) PTSD: Decremento dell’attivazione spontanea (alcool) ADHD: Incremento della concentrazione e “rallentamento” delle performance (cocaina) 2
 Depressione, in particolare disturbo bipolare: stabilizzazione o amplificazione del tono dell’umore e manipolazione delle sensazioni (oppiacei, cocaina) Disturbi di Personalità: superamento dell’isolamento e dell’insoddisfazione, vissuti a seguito dell’impairment psicosociale correlato al dp, mediante ricerca di alterazioni comportamentali e supporto fornito dall’inserimento in gruppi di pari più tolleranti (poliabuso) PTSD: Decremento dell’attivazione spontanea (alcool) ADHD: Incremento della concentrazione e rallentamento delle performance (cocaina) 2.")
51
DOPPIA DIAGNOSI: LA SFIDA
L’emergenza e la diffusione ubiquitaria della doppia diagnosi rappresentano un elemento “catastrofico” che segna una crisi profonda ed impone una svolta alle consolidate modalita’ di presa in carico e di assistenza alla popolazione tossicomane e psichiatrica da parte del sistema dicotomico dipendenze/salute mentale

52
“DD”: CONFIGURAZIONI CLINICHE POSSIBILI
Condizione psichiatrica reversibile/temporanea indotta da sostanze; Slatentizzazione di fenomeni psicopatologici da parte delle sostanze stesse; Paziente psichiatrico che usa sostanze; Consumo cronico di sostanze che determina una patologia psichiatrica persistente;

53
Quadrant Model for Dual Diagnosis treatment
53

54
Overlap of comorbid disorders
54

55
Quadrant Model for Dual Diagnosis treatment
QI (low/low): out-patient addiction services QII (high psych/low addict): in-patient psychiatric services QIII (low psych/high addict): in-patient addiction services QIV (high psych/high addict): specialized dual diagnosis unit Psychotic: DD unit in psychiatric service Non-psychotic: DD unit in addiction service 55
: out-patient addiction services. QII (high psych/low addict): in-patient psychiatric services. QIII (low psych/high addict): in-patient addiction services. QIV (high psych/high addict): specialized dual diagnosis unit. Psychotic: DD unit in psychiatric service. Non-psychotic: DD unit in addiction service. 55.")
56
Main comorbid disorders
Depression Anxiety disorders Chronic psychotic disorders ADHD Borderline PD 56

57
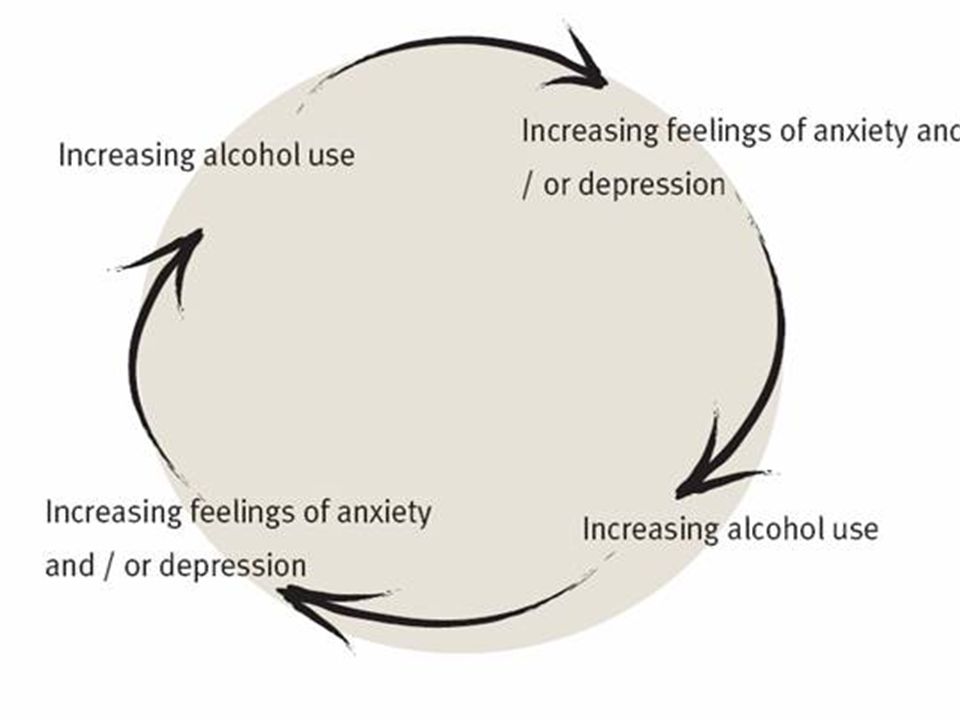
Anxiety & alcohol Mainly social phobia: Anxiety after abstinence:
Alcohol initially eases social contact In long-run alcohol dependence increases level of anxiety Anxiety after abstinence: strong reduction for majority within first 2-3 weeks 57

58
Anxiety & cannabis Chronic/ daily users report: anxiety, depression, fatigue, reduced motivation Cross sectional studies support association between use and depression/ anxiety (up to 5 x increase in anxiety/ depression disorders vs non users) Depression and anxiety in teenagers does not appear to increase risk of regular cannabis use 58
 Depression and anxiety in teenagers does not appear to increase risk of regular cannabis use. 58.")
59
Ecstasy and mental disorders
59

60
Anxiety Disorders in Substance Abusers
Post-Traumatic Stress Disorder Panic Disorder, Agorafhobia & Social Phobia

61
Post-Traumatic Stress Disorder (PTSD)
Symptoms are often grouped into three main categories: Re-living Avoiding Increased arousal

62
PTSD: Re-living and avoiding
People with PTSD repeatedly re-live the trauma through thoughts and memories of the trauma. They may also feel great distress when certain things remind them of the trauma – such as the anniversary date of the event. AVOIDANCE The person may avoid people, places, or thoughts or situations that may remind them of the trauma. This can lead to: feelings of detachment and isolation from family and friends, as well as a loss of interest in activities that they once enjoyed.

63
PTSD: Increased arousal
Difficulty falling or staying asleep Irritability, outbursts of anger The person may also suffer physical symptoms such as increased blood pressure and heart rate, rapid breathing, muscle tension, nausea and diarrhea. difficult to differentiate from substance induced arousal (e.g. cocaine)
")
64
PTSD and Substance Abuse
Used primarily to numb the painful memories of past experiences. Heavy use of alcohol, nicotine, caffeine, and other drugs. The “cure” often becomes a bigger problem than the problem it was supposed to help … dependency. Increased tolerance to alcohol and drugs

65
Prevalence of PTSD and Substance Use Disorders
Community samples of addicts: % life-time PTSD In-patients: 39% current PTSD Problem: most clinicians misdiagnose PTSD and/or ignore the problem

66
Etiological models of PTSD-SUD
Victims of violence are often under influence of alcohol/drug Alcohol/drugs are used as self-medication Co-occurrence of PTSD and SUD is due to ’third’ factor: Common genetic pathway Early childhood trauma Most evidence for ‘self-medication’ model

67
Simple vs. Complex PTSD Simple PTSD typically develops from one incident, usually experienced as an adult. Complex PTSD is associated with repeated incidents (domestic violence or ongoing childhood abuse). Broader range of symptoms: self-harm, suicide, dissociation (“losing time”); problems with relationships, memory, sexuality, health, anger, shame, guilt, numbness, loss of faith and trust, feeling damaged.
. Broader range of symptoms: self-harm, suicide, dissociation ( losing time ); problems with relationships, memory, sexuality, health, anger, shame, guilt, numbness, loss of faith and trust, feeling damaged.")
68
Relationships between Trauma and Substance Abuse
Traumatic experiences increase likelihood of substance abuse, especially if PTSD develops Childhood trauma increases risk of PTSD, especially if it is multiple trauma Substance abuse increases the risk of victimization Need for linkages between systems: medical, shelters, social services, mental health, criminal justice, addiction treatment (Zweben et al 1994)
")
69
Pathways Between Trauma-related Disorders and Substance Use
SUD PTSD TRAUMA 3

70
Panic disorder, Agoraphobia and Social Phobia

71
Substance Abuse and Anxiety Disorders
High comorbidity in community studies especially alcohol abuse (e.g. Kessler et al., 1997; NEMESIS, 1998) One third of alcohol dependent males co-current anxiety disorder More than half of alcohol dependent females co-current anxiety disorder Most prevalent anxiety disorders: Social phobia Panic disorder/agoraphobia
 One third of alcohol dependent males co-current anxiety disorder. More than half of alcohol dependent females co-current anxiety disorder. Most prevalent anxiety disorders: Social phobia. Panic disorder/agoraphobia.")
72
Substance Dependence / Anxiety Interface
Substance-induced anxiety Self-medication Common aetiology Common risk factors Common neurobiology

73
A representative general population sample (n = 7,076)
Origin of the comorbidity of anxiety disorders and alcohol dependence Marquenie et al. (2007) European Addiction Research,13, A representative general population sample (n = 7,076) Different models were tested: (1) anxiety disorders increase the risk of alcohol dependence; (2) alcohol dependence increases the risk of anxiety disorders; (3) family history or childhood traumatisation increase the risk of both alcohol dependence and anxiety disorders.
 European Addiction Research,13, A representative general population sample (n = 7,076) Different models were tested: (1) anxiety disorders increase the risk of alcohol dependence; (2) alcohol dependence increases the risk of anxiety disorders; (3) family history or childhood traumatisation increase the risk of both alcohol dependence and anxiety disorders.")
74
Origin of the comorbidity of anxiety disorders and alcohol dependence Marquenie et al. (2007) European Addiction Research,13, The data show that alcohol dependence does not precede the onset of anxiety disorders, anxiety disorders do precede the onset of alcohol dependence, that family history is not very likely to be the third factor explaining the elevated comorbidity, and that in women childhood trauma might be partially responsible for the association between both disorders

76
….gli aspetti terapeutici
Calves' Heads and Brains, or A Phrenological Lecture (London: Published for the Artist, 1826) Henry Thomas Alken ( )
 Henry Thomas Alken ( )")
77
LINEE-GUIDA: si o no... Come/dove realizzare un trattamento integrato per la “doppia diagnosi”? - Come/dove integrare trattamenti già esistenti? - Quali Servizi coinvolgere (DSM, SerT, Privato accreditato, Servizi specialistici DD, etc.)? - Quali percorsi attivare (territorio, ospedale, residenzialità comunitaria, rete informale, etc.)? - Quale intensità dare al programma?
 - Quali percorsi attivare (territorio, ospedale, residenzialità comunitaria, rete informale, etc.) - Quale intensità dare al programma")
78
Treatment: anxiety & alcohol
Wait 2-3 weeks Psychoeducation & social competency training If insufficient reduction of anxiety: More intensive psychotherapeutic intervention If no reduction or increase of anxiety: Combine with AD 78

79
Treatment: anxiety & cannabis
Withhold treatment for several weeks of abstinence Use benzodiazepines during withdrawal period Cognitive-behavioral interventions If symptoms persist or increase, start SSRI treatment (initiate with lower dose, i.e. citalopram 10mg) 79
 79.")
80
Personality Disorders Affect Treatment Outcome
Higher drop out Reduced effect of treatment Less adequate social functioning Enhanced criminality figures Higher prevalence of Axis-I disorders

81
Challenges in the Treatment of Traumatic Stress and Addiction
Abstinence may not resolve comorbid trauma-related disorders for many patients the PTSD worsens Individuals with PTSD abuse the most severe substances and are vulnerable to relapse for both conditions, as well as repeated trauma Confrontational approaches typical in addictions settings frequently exacerbate mood and anxiety disorders Phase of Illnesses of chronic recurrent disorders is critical. 4 4

82
Challenges in the Treatment of Traumatic Stress and Addiction
12-Step Models often do not acknowledge the need for pharmacological interventions Treatment programs often do not offer integrated treatments for Substance Use and PTSD Treatments developed for PTSD alone may not be advisable to treat individuals with addictions

83
What Disorder to Treat First?
Dual PTSD-SUD disorders are difficult to treat Mental health centers refer to addiction centers Addiction centers refer to mental health centers Alternative: integrated treatment of PTSD and addiction?

84
Integrated Intervention PTSD-Substance Abuse
Particip. Dually diagnosed Sequential vs. contemporaneous Timing Attend to one or both problems Therapist Interventions designed to address both problem areas Context

85
Naturalistic follow-up study:
Comorbid phobic disorders do not influence outcome of alcohol dependence treatment. (Marquenie et al., Alcohol & Alcoholism, 2006, 41(2):168-73) Do social and agoraphobic patients alcohol dependent patients have an increased chance of relapse? Naturalistic follow-up study: 81 alcohol-dependent patients with comorbid social phobia or agoraphobia 88 alcohol-dependent patients without anxiety disorders Alcohol-dependent patients who have undergone alcohol-dependence treatment are not at greater risk of a relapse if they have a comorbid anxiety disorder.
:168-73) Do social and agoraphobic patients alcohol dependent patients have an increased chance of relapse Naturalistic follow-up study: 81 alcohol-dependent patients with comorbid social phobia or agoraphobia. 88 alcohol-dependent patients without anxiety disorders. Alcohol-dependent patients who have undergone alcohol-dependence treatment are not at greater risk of a relapse if they have a comorbid anxiety disorder.")
86
The additional therapy clearly reduced the anxiety symptoms
The effectiveness of anxiety treatment on co-morbid patients (Schade et al., Alcohol Clin Exp Res. 2005, 29(5): ) RCT with patients with double diagnosis of alcohol dependence and agoraphobia or social phobia. Psychosocial relapse-prevention program (RPP) on its own (n = 49) or RPP plus an anxiety treatment program comprising cognitive behavioral therapy (CBT) and optional pharmacotherapy consisting of an SSRI (n = 47). The additional therapy clearly reduced the anxiety symptoms It had no significant effect on the alcohol relapse rates.
: ) RCT with patients with double diagnosis of alcohol dependence and agoraphobia or social phobia. Psychosocial relapse-prevention program (RPP) on its own (n = 49) or. RPP plus an anxiety treatment program comprising cognitive behavioral therapy (CBT) and optional pharmacotherapy consisting of an SSRI (n = 47). The additional therapy clearly reduced the anxiety symptoms. It had no significant effect on the alcohol relapse rates.")
87
Concluding Remarks on Anxiety Disorders
Phobic disorders do not enhance risk of relapse in substance abuse. Although CBT focusing on anxiety results in less anxiety this does not affect the rate of relapse after cognitive behaviour therapy for substance abuse.

88
Integrated models of intervention
New integrated models have been developed during the last 15 years with several common features Patient engagement and retention Persuasion about the relevance of substance abuse to psychiatric disturbances Assessment (distinguishing primary from secondary disorders) Concomitant treatment of both disorders Training in relapse prevention in an aftercare setting Ridgely et al. 1991
 Concomitant treatment of both disorders. Training in relapse prevention in an aftercare setting. Ridgely et al")
89
Integrated models of intervention

90
Psychopathology and addictive disorders are not linked
Possible Relationships Between Addictive Behavior and Coexisting Psychopathology. Guide-lines Axis I and II Psychopathology May Serve as a Risk factor for addictive disorders Psychopathology may modify the course of an addictive disorder in terms of rapidity of course, response to treatment, symptom picture, and long term outcome Psychiatric symptoms may develop in the course of chronic intoxication, acute withdrawal, or prolonged abstinence Psychopathology and addictive disorders are not linked 5

91
Psychopharmacological treatment - any effect on alcohol dependence?
Anxiety (Buspirone): 5 studies Effect anxiety, not SUD Bipolar (Valproate): lithium+valproate vs lithium Effect SUD, not mood Schizophrenia (Clozapine): no RCT-study Effect SUD + psychosis Fauve et al., Alc Clin Exp Res 2004
: 5 studies. Effect anxiety, not SUD. Bipolar (Valproate): lithium+valproate vs lithium. Effect SUD, not mood. Schizophrenia (Clozapine): no RCT-study. Effect SUD + psychosis. Fauve et al., Alc Clin Exp Res")
92
Anxiety Disorders: What Medications to Use?
SSRI’s Venlafaxine MAOI’s Similar to other psychiatric disorders, it has not been demonstrated that treating anxiety disorder helps reduce substance use 15

93
Pharmacologic Treatments for Anxiety Disorders: Conclusions
Much less empirical data compared to depression Some evidence that anxiety symptoms more likely to improve with buspirone or SSRI (paroxetine). No clear evidence that alcohol or drug use is reduced Again, abstinence from drugs prior to initiation of trial may reduce placebo response rates and increase likelihood of finding drug-placebo differences
. No clear evidence that alcohol or drug use is reduced. Again, abstinence from drugs prior to initiation of trial may reduce placebo response rates and increase likelihood of finding drug-placebo differences.")
94
Conclusions Very little data to guide clinicians regarding what pharmacologic strategies are the most efficacious to treat alcoholics/substance abusers with bipolar disorder, anxiety disorders, ADHD or schizophrenia At present, prudent to use medications that are safer, long-acting, and less abuse liability for dually-diagnosed patients since they tend to be less treatment compliant and more impulsive More research is needed.

95
Centrate sulle priorità: - del sintomo, - dei compiti istituzionali,
Che fare? il paziente in “doppia diagnosi” (DD), specie se poliabusatore, generalmente tende a essere assistito ma non curato, rimane una presenza continua e pressante per il Servizio e costituisce lo zoccolo duro dei pazienti definiti come “cronici”: le risposte usuali degli operatori rischiano pertanto di rinforzare le problematiche che costui porta Caratteristiche DD Polimorfismo sintomatologico Richieste pressanti e caotiche a Servizi e professionisti diversi Fallimento dialettico Autoinvalidazione Passività Tendenza all’evitamento Difficoltà nel problem solving Risposte usuali Divise tra più Servizi Centrate sulle priorità: - del sintomo, - dei compiti istituzionali, - della domanda esplicita, - del contenimento della crisi
, specie se poliabusatore, generalmente tende a essere assistito ma non curato, rimane una presenza continua e pressante per il Servizio e costituisce lo zoccolo duro dei pazienti definiti come cronici : le risposte usuali degli operatori rischiano pertanto di rinforzare le problematiche che costui porta. Caratteristiche DD. Polimorfismo sintomatologico. Richieste pressanti e caotiche a Servizi e professionisti diversi. Fallimento dialettico. Autoinvalidazione. Passività. Tendenza all’evitamento. Difficoltà nel problem solving. Risposte usuali. Divise tra più Servizi. Centrate sulle priorità: - del sintomo, - dei compiti istituzionali, - della domanda esplicita, - del contenimento della crisi.")
96
come intervenire modificando l’approccio al problema
Cambiare “mitologie” e modelli di riferimento operativi Intervenire sulle resistenze al cambiamento Migliorare la definizione degli obbiettivi Aumentare la percezione della trattabilità dei pazienti Addestrare correttamente su evoluzione/prognosi e sul progetto terapeutico

97
come organizzare un Servizio terapeutico
Il Servizio può avere due impostazioni generali: - essere un’organizzazione che mette gli operatori “solo” nella condizione di svolgere il proprio lavoro - avere una connotazione terapeutica nella sua architettura organizzativa

98
come organizzare un Servizio terapeutico
nella prima ipotesi, il Servizio si modella sulle esigenze dei professionisti e sulle risorse (quantitative e qualitative) disponibili nella seconda ipotesi, il Servizio si costruisce sulla visione della patologia (filosofia del Servizio)
 disponibili. nella seconda ipotesi, il Servizio si costruisce sulla visione della patologia (filosofia del Servizio)")
99
….per una possibile prevenzione
Calves' Heads and Brains, or A Phrenological Lecture (London: Published for the Artist, 1826) Henry Thomas Alken ( )
 Henry Thomas Alken ( )")
100
Antecedents of substance use in adolescence
Sensation seeking temperament Aggressiveness Impulsivity Conduct problems Cognitive difficulties Deviant peers affiliation Poor parenting Maladaptation to stress Social anxiety Mood problems Poikolainen, Current Opinion in Psychiatry Gerra et al., Subst. Use Misuse

101
Predictors at the age of 11-years (Gerra, 2006)
EARLY ONSET SUBSTANCE USE IS NOT CASUAL OR OCCASIONAL Poor self control (Wills et al., 2001) Present orientation (Wills et al., 2001) Risk taking tendency (Wills et al., 2000) Negative life events (Wills et al., 1998) Low academic competence (Wills et al., 1998) Low parental support (Wills et al., 1998) Negative mood (Wills et al., 1995)
 Present orientation (Wills et al., 2001) Risk taking tendency (Wills et al., 2000) Negative life events (Wills et al., 1998) Low academic competence (Wills et al., 1998) Low parental support (Wills et al., 1998) Negative mood (Wills et al., 1995)")
102
Adverse Childhood Experiences (ACEs)
Abuse variables Emotional, Physical , Sexual Neglect variables Emotional, Physical Household dysfunction variables Battered mother Parental separation or divorce Mental illness in a family member Substance abuse in a family member Incarcerated family member Dube et al., 2003

103
Weak social competence Lack of interest Insecure identity
NON SOLO DSM IV Gerra, 2006) Low self esteem Weak social competence Lack of interest Insecure identity No long term vocation No ideological values Immature relationships Peer rejection Lack of family monitoring Poor family bonding Lack of school engagement
 Low self esteem. Weak social competence. Lack of interest. Insecure identity. No long term vocation. No ideological values. Immature relationships. Peer rejection. Lack of family monitoring. Poor family bonding. Lack of school engagement.")
104
PREDICTORS OF SUBSTANCE USE DISORDERS
Social phobia and panic disorder (Zimmerman et al., 2003) Persistence of ADHD and adolescent CD (Molina and Pelham, 2003; Wilens et al., 1997) - ADHD and CD (Flory et al., 2003; Whitmore et al., 1997) ADHD adolescents more vulnerable to peers influences (Marshal et al., 2003) ADHD, anxiety, disruptive behavior (Hahesy et al., 2002)
 Persistence of ADHD and adolescent CD. (Molina and Pelham, 2003; Wilens et al., 1997) - ADHD and CD. (Flory et al., 2003; Whitmore et al., 1997) ADHD adolescents more vulnerable to peers influences (Marshal et al., 2003) ADHD, anxiety, disruptive behavior. (Hahesy et al., 2002)")
105
PREDICTORS OF SUBSTANCE USE DISORDERS
MOOD DISORDER (Depression and Bipolar Disorder) FOLLOWED THE ONSET OF SUBSTANCE USE DISORDERS (SUD)(Hahesy et al., 2002) DEPRESSIVE SYMPTOMS IN ADOLESCENCE PREDICTED PROBLEM DRINKING (Aalto-Setala et al., 2002) ADOLESCENT-ONSET BIPOLAR DISORDER IS ASSOCIATED WITH HIGHER RISK FOR SUD (Wilens et al., 1999) SOCIAL ANXIETY PREDICT NICOTINE DEPENDENCE (Sonntag et al., 2000)
 FOLLOWED THE ONSET OF SUBSTANCE USE. DISORDERS (SUD)(Hahesy et al., 2002) DEPRESSIVE SYMPTOMS IN ADOLESCENCE. PREDICTED PROBLEM DRINKING. (Aalto-Setala et al., 2002) ADOLESCENT-ONSET BIPOLAR DISORDER. IS ASSOCIATED WITH HIGHER RISK FOR SUD. (Wilens et al., 1999) SOCIAL ANXIETY PREDICT NICOTINE. DEPENDENCE. (Sonntag et al., 2000)")
106
Sintomi psichiatrici antecedenti l’esordio dei disturbi da
uso di sostanze: Ansia 60% Disturbi dell’umore 51% ADHD 47% Disturbo della condotta 19% …Mania …Disturbi dell’alimentazione Tra gli adolescenti SU non-problematici già presenti i sintomi Crescente % di sintomi nei SUP e SUD (Shrier et al., 2003)
")
107
Identification of temperamental risk factors
for child psychopathologies - Behavioral inhibition (social anxiety disorder) - Behavioral disinhibition (disruptive behavior - mood disorders) SUBSTANCE USE DISORDERS
 - Behavioral disinhibition. (disruptive behavior - mood disorders) SUBSTANCE USE DISORDERS.")
108
“Doppia Diagnosi”…in molti casi, certamente, una “clinica della confusione”
Quadri sovrapposti Quadri misti Stati misti Cicli rapidi Depressione agitata Mania disforica Decorsi rallentati Associazioni spurie o composite Patomorfosi eterogenea Cronicizzazione di elementi misti Intossicazione o astinenza Influenza di: terapia sostitutiva, NL, stabilizzanti, AD, BDZ Condizioni organiche e terapie mediche

109
“DOPPIA DIAGNOSI”: “NON DIAGNOSI” O “NUOVA DIAGNOSI” ?
La DD si configura come un potente “disorganizzatore nosografico” Nella DD si verifica un’alterazione della processualità temporale dei Disturbi Mentali classicamente descritti (acuzie, cronicità, ciclicità, remissione, scompenso, ricaduta, recidiva) Che fare, allora, nella DD?
 Che fare, allora, nella DD")
Presentazioni simili

 Valutazione quantitativa dei pazienti sofferenti di (HAE) in Francia, Germania, Italia, Spagna e UK Condotto.>")

 Brussels, 26 settembre 2013.>")

 064825120 - fax.>")














