Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Gaeta, 11 Maggio 2013 La vaccinazione per il Meningococco e la Pertosse: quali strategie attuali e future Rocco Russo pediatra “Quando penso a una malattia non è per trovarvi rimedio ma, invece, per prevenirla” (Louis Pasteur)
")
2
Mi è molto difficile esprimere con le parole il dolore per la scomparsa di un Grande Maestro come il Prof. Giorgio Bartolozzi, ma sono sicuro che ciò che ha seminato in noi sicuramente porterà buoni frutti! I Grandi non muoiono MAI! (e Lui è anche di più...) Rocco Russo
 Rocco Russo.")
3
“Contro la meningite P. U. O. I
“Contro la meningite P.U.O.I. fare la differenza: Previeni, Unisciti, Osserva, Informati”

4
Neisseria meningitidis
Classificazione A B C Y W Presenti 13 sierogruppi distinti in base alla capsula polisaccaridica Più del 90% dei casi di malattia invasiva son causati dai suddetti 5 sierogruppi

5
Review Emergence of serogroup X meningococcal disease in Africa: Need for a vaccine
Ouli Xie, Andrew Pollard, Judith E. Mueller, Gunnstein Norheima Countries in Africa with laboratory-confirmed outbreaks or larger clustersof cases of meningococcal disease in the sub-Saharan meningitis belt involving serogroup X meningococci. The coloured areas indicate the different defined levelsof risk of epidemic meningitis Cases of suspected bacterial meningitis cases reported in Niger in the period and laboratory confirmed cases of MenX reported to the national menin-gitis surveillance laboratory Centre de Recherche sur les Médicale et Sanitaire(CERMES), Niamey, Niger. Data on suspected meningitis cases extracted from WHO Global Health Observatory data repository
, Niamey, Niger. Data on suspected meningitis cases extracted from WHO Global Health Observatory data repository.")
6
Lancet Vol 380 November 10, : 1703–11 Estimates of global disease burden for meningitis attributable to Neisseria meningitidis (all ages), by organism and region (modificata) Data are n per population per year (95% CI) unless otherwise specifi ed. Mean proportion of survivors with major long-term sequelae for all organisms combined in the highest incidence regions is 25% (95% CI 19–32), and in the lowest incidence regions is 9% (7–12).1 *African meningitis belt. †Low incidence regions for invasive meningococcal disease—Europe, USA, and Australia. *African meningitis belt †Low incidence regions for invasive meningococcal disease - Europe, USA, and Australia
, by organism and region (modificata) Data are n per population per year (95% CI) unless otherwise specifi ed. Mean proportion of survivors with. major long-term sequelae for all organisms combined in the highest incidence regions is 25% (95% CI 19–32), and in the. lowest incidence regions is 9% (7–12).1 *African meningitis belt. †Low incidence regions for invasive meningococcal. disease—Europe, USA, and Australia. *African meningitis belt †Low incidence regions for invasive meningococcal disease - Europe, USA, and Australia.")
7
Neisseria meningitidis: sierogruppo per gruppo di età e anno (2007-2013)
TOTALE n.i. 1-4 5-9 10-14 15-24 25-64 >64 2007 B 81 2 14 17 7 1 20 15 5 C 43 13 3 12 Altro 8 Non tipizzato 52 11 2008 78 10 6 55 4 37 2009 92 23 9 22 46 21 28 2010 74 18 39 2011 75 19 24 34 2012 16 31 2013*

8
Mandatory and recommended vaccination in the EU, Iceland and Norway: results of the VENICE 2010 survey on the ways of implementing national vaccination programmes M Haverkate, F D’Ancona, C Giambi, K Johansen, P L Lopalco, V Cozza, E Appelgren published on 31 May 2012 Modality of implementation of childhood vaccination programme by vaccine in the E.U. countries, 2010 Vaccination Considering vaccination Recommended (RA or RR) Mandatory (MA or MR) Mixed Diphtheria 29 16 11 2 Haemophilus influenzae type B 21 8 Hepatitis A 25 22 1 Hepatitis B 17 10 Human papillomavirus 23 Influenza 28 NM Invasive disease caused by Neisseria Meningitides C Invasive pneumococcal disease 4 Measles-mumps-rubella Polio 12 Pertussis Rotavirus 9 Tetanus Tuberculosis (with Bacillus Calmette-Guérin) 15 7 Varicella 20 19 MA: mandatory for all; MR: mandatory for people at risk; NM: not mandatory in any of the countries in the study; RA: recommended for all; RR: recommended for people at risk
 Mandatory. (MA or MR) Mixed. Diphtheria Haemophilus influenzae type B Hepatitis A Hepatitis B Human papillomavirus. 23. Influenza. 28. NM. Invasive disease caused by Neisseria Meningitides C. Invasive pneumococcal disease. 4. Measles-mumps-rubella. Polio. 12. Pertussis. Rotavirus. 9. Tetanus. Tuberculosis (with Bacillus Calmette-Guérin) Varicella MA: mandatory for all; MR: mandatory for people at risk; NM: not mandatory in any of the countries in the study; RA: recommended for all; RR: recommended for people at risk.")
9
Meningococcal C vaccine in EU
Mandatory and recommended vaccination in the EU, Iceland and Norway: results of the VENICE 2010 survey on the ways of implementing national vaccination programmes M Haverkate, F D’Ancona, C Giambi, K Johansen, P L Lopalco, V Cozza, E Appelgren published on 31 May 2012 (modificata) Meningococcal C vaccine in EU Austria RA Belgium Bulgaria A Cyprus Czech Rep. RR Denmark Estonia RRe Finland France Germany Greece Hungary Iceland Ireland Italy RA/RRk Latvia RR Lithuania Luxembourg RA Malta A Netherlands Norway Poland Portugal Romania Slovakia Slovenia Spain Sweden U.K. A: Absence of recommendation, MA: Mandatory for all; MR: M. for people at risk; R: Recommended; RA: R. for all; RR: R. for people at risk e Not included in the national immunisation programme, but recommended by the Ministry of Social Affairs k Regional variability.
 Meningococcal C vaccine in EU. Austria. RA. Belgium. Bulgaria. A. Cyprus. Czech Rep. RR. Denmark. Estonia. RRe. Finland. France. Germany. Greece. Hungary. Iceland. Ireland. Italy. RA/RRk. Latvia. RR. Lithuania. Luxembourg. RA. Malta. A. Netherlands. Norway. Poland. Portugal. Romania. Slovakia. Slovenia. Spain. Sweden. U.K. A: Absence of recommendation, MA: Mandatory for all; MR: M. for people at risk; R: Recommended; RA: R. for all; RR: R. for people at risk. e Not included in the national immunisation programme, but recommended by the Ministry of Social Affairs. k Regional variability.")
10
NOVITA’: DUE VACCINI CALENDARIZZATI
Gazzetta Ufficiale - Serie Generale - n. 60 del 12 marzo 2012 Piano Nazionale Prevenzione Vaccinale NOVITA’: DUE VACCINI CALENDARIZZATI VACCINO CONTRO LO PNEUMOCOCCO VACCINO CONTRO LO IL MENINGOCCOCO C

11
Gazzetta Ufficiale - Serie Generale -
n. 60 del 12 marzo 2012 Calendario nazionale delle vaccinazioni offerte attivamente a tutta la popolazione PNPV 5) Dose singola. La somministrazione a anni va considerata nei soggetti non vaccinati nell’infanzia.
 Dose singola. La somministrazione a anni va considerata nei soggetti non vaccinati nell’infanzia.")
12
Current MenC vaccination schedule
Current vaccination schedules with the MenC conjugate vaccine in European countries Country Number of doses Current MenC vaccination schedule Source Andorra 3 2, 4, and 18 months WHO Austria 2 13 months (MenC) and years (MenACWY) The Federal Ministry of Health, Belgium 1 15 months Cyprus 12-13 months France 12-24 months Ministry of labour, health Germany 11-23 months Greece 2, 4, and months Iceland 6 and 8 months Ireland 4, 6, and 13 months Italy 12-13 months and risk groups Ministry of Health Luxembourg 13 months Monaco 2 years Netherlands 14 months Portugal 3, 5, 15 months Slovenia - risk groups Spain 2, 4-6, months Vaccine Advisory Committe Switzerland 12-15 months and years United 3, 4, months Department of Health a bhttp:// chttp:// dhttp://vacunasaep.org/profesionales/calendario-de-vacunaciones-de-la-aep-2011 ehttp:// Kaaijk et al. BMC Infectious Diseases 2012, 12:35 (modificata)
 and years (MenACWY) The Federal Ministry of Health, Belgium months. Cyprus months. France months. Ministry of labour, health. Germany months. Greece. 2, 4, and months. Iceland. 6 and 8 months. Ireland. 4, 6, and 13 months. Italy months and risk groups. Ministry of Health. Luxembourg. 13 months. Monaco. 2 years. Netherlands. 14 months. Portugal. 3, 5, 15 months. Slovenia. - risk groups. Spain. 2, 4-6, months. Vaccine Advisory Committe. Switzerland months and years. United. 3, 4, months. Department of Health. a bhttp:// chttp:// dhttp://vacunasaep.org/profesionales/calendario-de-vacunaciones-de-la-aep ehttp:// Kaaijk et al. BMC Infectious Diseases 2012, 12:35 (modificata)")
13
Is a single dose of meningococcal serogroup C conjugate vaccine sufficient for protection? Experience from the Netherlands Patricia Kaaijk, Arie van der Ende, Guy Berbers, Germie PJM van den Dobbelsteen and Nynke Y Rots Kaaijk et al. BMC Infectious Diseases 2012, 12:35 MenC disease cases a in the Netherlands per year, age group, and among vaccinees Summary: A single dose of MenC conjugate vaccine at the age of 14 months in combination with a catch up vaccine campaign appeared to be a successful strategy to prevent MenC disease in the Netherlands, there by confirming that a single dose of the vaccine could sufficiently protect against disease. Nevertheless, this approach can only be justified in countries with a relatively low incidence of serogroup C meningococcal disease in the first year of life. Furthermore, a good surveillance programme is recommended for timely detection of vaccine breakthroughs and outbreaks among non-vaccineessince long-term protection after a single dose in the second year of life cannot currently be guaranteed.

14
Cosa possiamo aspettarci da un vaccino MenC coniugato?
Herd Protection Solo i Vaccini coniugati determinano questo effetto Oltre all’effetto diretto sui vaccinati, una riduzione delle infezioni nella popolazione non vaccinata del 67%. Trotter CL, et al. Lancet. 2004;364: Introduzione del vaccino Gruppi d’età 0 -19 anni ≥20 anni Effetto di herd protection dimostrato Number of laboratory confirmed serogroup C meningococcal cases in England and Wales, Source: Health Protection Agency

15
EPIDEMIOLOGIA DELLE MALATTIE INVASIVE DA MENINGOCOCCO IN EMILIA-ROMAGNA (dicembre 2012)
(fonte: F. D’Ancona) Numero di casi di MIB da meningococco C nella fascia d’età 0-4 anni e copertura vaccinale (%)al 24° mese per anno. Emilia-Romagna, Casi di MIB da meningococco C per abitanti notificati prima e dopo l’introduzione del vaccino per classi di età. Emilia-Romagna, vs 8,5 casi (range: 4-14) 2,6 casi (range: 1-5) si passa in termini assoluti da una media annuale di 8,5 casi di meningococco C (range: 4-14) ( ) ad una media annuale di 2,6 casi (range: 1-5) nel periodo post-vaccinazione ( * dati non definitivi
 Numero di casi di MIB da meningococco C nella fascia. d’età 0-4 anni e copertura vaccinale (%)al 24° mese per anno. Emilia-Romagna, Casi di MIB da meningococco C per abitanti notificati prima e dopo l’introduzione del vaccino per classi di età. Emilia-Romagna, vs ,5 casi. (range: 4-14) 2,6 casi. (range: 1-5) si passa in termini assoluti da una media annuale di 8,5 casi di meningococco C (range: 4-14) ( ) ad. una media annuale di 2,6 casi (range: 1-5) nel periodo post-vaccinazione ( * dati non definitivi.")
16
Garantire l’offerta attiva e gratuita delle vaccinazioni prioritarie per la popolazione generale al fine del raggiungimento e del mantenimento dei livelli di copertura sotto indicati necessari a prevenire la diffusione delle specifiche malattie infettive (PNPV ): Raggiungimento e mantenimento di coperture vaccinali ≥ 95% per le vaccinazioni anti DTPa, Poliomielite, Epatite B, Hib, nei nuovi nati e delle vaccinazioni anti DTPa e Poliomielite a 5-6 anni; Raggiungimento e mantenimento di coperture vaccinali ≥ 90% per la vaccinazione dTpa negli adolescenti all’età di 14-15° anni (5° dose), (range anni); Raggiungimento e mantenimento di coperture vaccinali per 2 dosi di MPR ≥ 95% nei bambini di 5-6 anni di età e negli adolescenti (11-18 anni); Riduzione della percentuale delle donne in età fertile suscettibili alla rosolia a meno del 5%; Raggiungimento di coperture per la vaccinazione antinfluenzale del 75% come obiettivo minimo perseguibile e del 95% come obiettivo ottimale negli ultrasessantacinquenni e nei gruppi a rischio; Raggiungimento e mantenimento nei nuovi nati di coperture vaccinali ≥ 95% per la vaccinazione antipneumococcica; 7. Raggiungimento e mantenimento nei nuovi nati e negli adolescenti (11-18 anni) di coperture vaccinali ≥ 95% per la vaccinazione antimeningococcica; 8. Offerta attiva della vaccinazione antivaricella agli adolescenti suscettibili (11 – 18 anni) e alle donne suscettibili in età fertile e ai soggetti a elevato rischio individuale e professionale; 9. Raggiungimento di coperture vaccinali per 3 dosi HPV: ≥ 70% nelle dodicenni a partire dalla coorte 2001, ≥ 80% nelle dodicenni a partire dalla coorte del 2002, ≥ 95% nelle dodicenni a partire dalla coorte del Raggiungimento e mantenimento di coperture vaccinali per 1 dose di vaccinazione antivaricella ≥ 95% entro i 2 anni di età, a partire dalla coorte Raggiungimento e mantenimento di coperture vaccinali per 2 dosi di vaccinazione antivaricella ≥ 95% nei bambini di 5-6 anni di età e negli adolescenti, a partire dalla coorte Raggiungimento e mantenimento di coperture vaccinali per 1 dose di MPR ≥ 95% entro i 2 anni di età
, (range anni); Raggiungimento e mantenimento di coperture vaccinali per 2 dosi di MPR ≥ 95% nei bambini di 5-6 anni di età e negli adolescenti (11-18 anni); Riduzione della percentuale delle donne in età fertile suscettibili alla rosolia a meno del 5%; Raggiungimento di coperture per la vaccinazione antinfluenzale del 75% come obiettivo minimo perseguibile e del 95% come obiettivo ottimale negli ultrasessantacinquenni e nei gruppi a rischio; Raggiungimento e mantenimento nei nuovi nati di coperture vaccinali ≥ 95% per la vaccinazione antipneumococcica; 7. Raggiungimento e mantenimento nei nuovi nati e negli adolescenti (11-18 anni) di coperture vaccinali ≥ 95% per la vaccinazione antimeningococcica; 8. Offerta attiva della vaccinazione antivaricella agli adolescenti suscettibili (11 – 18 anni) e alle donne suscettibili in età fertile e ai soggetti a elevato rischio individuale e professionale; 9. Raggiungimento di coperture vaccinali per 3 dosi HPV: ≥ 70% nelle dodicenni a partire dalla coorte 2001, ≥ 80% nelle dodicenni a partire dalla coorte del 2002, ≥ 95% nelle dodicenni a partire dalla coorte del Raggiungimento e mantenimento di coperture vaccinali per 1 dose di vaccinazione antivaricella ≥ 95% entro i 2 anni di età, a partire dalla coorte Raggiungimento e mantenimento di coperture vaccinali per 2 dosi di vaccinazione antivaricella ≥ 95% nei bambini di 5-6 anni di età e negli adolescenti, a partire dalla coorte Raggiungimento e mantenimento di coperture vaccinali per 1 dose di MPR ≥ 95% entro i 2 anni di età")
17
Il vaccino contro il meningococco C
Il vaccino contro il meningococco C coniugato con la proteina CRM197 venne sviluppato agli inizi degli anni ’90

18
Licensed meningococcal vaccines — United States, 1981–2012
Formulation Type Trade name Manufacturer Licensed Age group Dose(s) Serogroups MPSV4 Polysaccharide Menomune Sanofi Pasteur 1981 ≥ 2 yrs Single dose A, C, W, and Y MenACWY-D Conjugate Menactra 2005 11-55 yrs 2007 2-10 yrs 2011 9-23 mos 2-dose series MenACWY-CRM Menveo Novartis 2010 Hib-MenCY-TT MenHibrix GlaxoSmithKline 2012 6 wks-18 mos 4-dose series C and Y
 Serogroups. MPSV4. Polysaccharide. Menomune. Sanofi Pasteur ≥ 2 yrs. Single dose. A, C, W, and Y. MenACWY-D. Conjugate. Menactra yrs yrs mos. 2-dose series. MenACWY-CRM Menveo. Novartis Hib-MenCY-TT MenHibrix. GlaxoSmithKline wks-18 mos. 4-dose series. C and Y.")
19
Il Meningococco B possiede molti diversi sottotipi
Vaccino contro il Meningococco B Il Meningococco B possiede un polisaccaride di parete a base di acido sialico, che è un antigene self, verso il quale già nel feto si osserva un fenomeno di tolleranza Il Meningococco B possiede molti diversi sottotipi

20
Reverse Vaccinology Figure 2. Application of Reverse Vaccinology in Development of a Vaccine for Group B Neisseria meningitidis Infection. Reverse vaccinology has been so named because it depends on genome mining with the use of computer-based algorithms as the initial step rather than on the time-consuming conventional methods that involve culturing the live microorganism. Most of the antigens used in current vaccines (e.g., capsular polysaccharide or modified toxins) are also involved in pathogenesis. Reverse vaccinology involves the unbiased selection of vaccine candidates from the genome and includes those which would not be easily identified by conventional methods. Interestingly, N. meningitidis adhesin A (NadA) and factor H–binding protein (fHbp), which are also involved in meningococcal pathogenesis, were both identified by reverse vaccinology. ELISA denotes enzyme-linked immunosorbent assay, FACS fluorescenceactivated cell sorting, NMB N. meningitidis group B, PCR polymerasechain- reaction assay, and SBA serum bactericidal antibody. N Engl J Med 2010;362:
 are also involved in pathogenesis. Reverse vaccinology involves the unbiased selection of vaccine candidates. from the genome and includes those which would not be easily identified. by conventional methods. Interestingly, N. meningitidis adhesin A. (NadA) and factor H–binding protein (fHbp), which are also involved in. meningococcal pathogenesis, were both identified by reverse vaccinology. ELISA denotes enzyme-linked immunosorbent assay, FACS fluorescenceactivated. cell sorting, NMB N. meningitidis group B, PCR polymerasechain- reaction assay, and SBA serum bactericidal antibody. N Engl J Med 2010;362:")
21
Identificazione nuove proteine Espressione di nuove proteine
Reverse Vaccinology Analisi al computer Sequenza dell’intero genoma batterico Identificazione nuove proteine Espressione di nuove proteine Saggio di immunogenicità in topolini Sviluppo di un vaccino 1-2 anni Tettelin H, et al. Science. 2000;287:1809–1815. Rappuoli R. Vaccine. 2001;19:2688–2691. Pizza M, et al. Science. 2000;287:1816–1820.

22
Combinazioni antigeniche proteiche nel nuovo vaccino contro il sierogruppo B
Vescicole della membrana esterna (OMV) di Neisseria meningitidis gruppo B ceppo NZ98/254 misurate come quantità di proteina totale contenente PorA P1.4 3 antigeni proteici Proteina di fusione ricombinante NHBA PorA LPS PorB Class 4 Class 5 OMV GNA2132 GNA1030 N C Proteina di fusione ricombinante fHbp GNA2091 GNA1870 N C Proteina ricombinante NadA NadA N C
 di Neisseria meningitidis gruppo B ceppo NZ98/254 misurate come quantità di proteina totale contenente PorA P antigeni proteici. Proteina di fusione ricombinante NHBA. PorA. LPS. PorB. Class 4. Class 5. OMV. GNA2132. GNA1030. N. C. Proteina di fusione ricombinante fHbp. GNA2091. GNA1870. N. C. Proteina ricombinante NadA. NadA. N. C.")
23
Componenti antigenici del 4CMenB
(Ogni antigene è importante per la sopravvivenza, fisiologia o virulenza del batterio) NadA: neisserial adhesin A - Promuove l’aderenza e l’invasione delle cellule epiteliali umane - Probabile importaza nel “carriage” fHbp: factor H binding protein - Lega il fattore H consentendo la sopravvivenza del batterio NHBA: neisserial heparin-binding antigen - Presente virtualmente in tutti i cepppi - Il legame all’eparina puo’ aumentare la resisetnza al batterio nel siero NZ PorA 1.4: porin A - Principale proteina delle Outer Membrane Vesicles (OMV) - Produce una robusta risposta anticorpale Key Point: The 3 main protein antigens were selected for inclusion in the Novartis 4CMenB vaccine—fHbp, NadA, and NHBA—based on their importance for the survival, function, virulence, or pathogenicity of the meningococci. Adding the PorA component of the New Zealand vaccine expands coverage to include important clonal complexes. Slide Overview: NadA: neisserial adhesin A is important for 2 reasons: Novel bacterial invasin that promotes adhesion to and invasion into human epithelial cells1-3 Possible importance in carriage fHbp: factor H binding protein was historically thought to primarily bind to factor H, which enables bacterial survival.5,6 However, new evidence suggests its true primary function is bacterial siderophore enterobactin binding (shown in vitro).4 Furthermore, it was recently shown that NspA, another protein, binds human factor H with higher affinity and specificity than fHbp, thus supporting the possibility for this newly identified primary function.7 NHBA: neisserial heparin-binding antigen Present in virtually all strains and binds heparin, which may increase the serum resistance of bacteria8-10 NZ PorA 1.4: porin A Major outer membrane vesicles protein—produces robust antibody response References: Comanducci M, et al. NadA, a novel vaccine candidate of Neisseria meningitidis. J Exp Med. 2002;195: Capecchi B, et al. Neisseria meningitidis NadA is a new invasin which promotes bacterial adhesion to and penetration into human epithelial cells. Mol Microbiol. 2005;55: Mazzon C, et al. IFN-gamma and R-848 dependent activation of human monocyte-derived dendritic cells by Neisseria meningitidis adhesin A. J Immunol. 2007;179: Veggi D, et al. Presented at IPNC. Banff, Canada. September 11-16, 2010. Madico G, et al. The meningococcal vaccine candidate GNA1870 binds the complement regulatory protein factor H and enhances serum resistance. J Immunol. 2006;177: Schneider MC, et al. Functional significance of factor H binding to Neisseria meningitidis. J Immunol. 2006;176: Lewis LA, et al. The meningococcal vaccine candidate neisserial surface protein A (NspA) binds to factor H and enhances meningococcal resistance to complement. PLoS Pathog. 2010;6:e Serruto D, et al. Neisseria meningitidis GNA2132, a heparin-binding protein that induces protective immunity in humans. Proc Natl Acad Sci U S A. 2010;107: Welsch JA, et al. Antibody to genome-derived neisserial antigen 2132, a Neisseria meningitidis candidate vaccine, confers protection against bacteremia in the absence of complement-mediated bactericidal activity. J Infect Dis. 2003;188: Plested JS, Granoff DM. Vaccine-induced opsonophagocytic immunity to Neisseria meningitidis group B. Clin Vaccine Immunol. 2008;15: 23 23
 NadA: neisserial adhesin A. - Promuove l’aderenza e l’invasione delle cellule epiteliali umane. - Probabile importaza nel carriage fHbp: factor H binding protein. - Lega il fattore H consentendo la sopravvivenza del batterio. NHBA: neisserial heparin-binding antigen. - Presente virtualmente in tutti i cepppi. - Il legame all’eparina puo’ aumentare la resisetnza al batterio nel siero. NZ PorA 1.4: porin A. - Principale proteina delle Outer Membrane Vesicles (OMV) - Produce una robusta risposta anticorpale. Key Point: The 3 main protein antigens were selected for inclusion in the Novartis 4CMenB vaccine—fHbp, NadA, and NHBA—based on their importance for the survival, function, virulence, or pathogenicity of the meningococci. Adding the PorA component of the New Zealand vaccine expands coverage to include important clonal complexes. Slide Overview: NadA: neisserial adhesin A is important for 2 reasons: Novel bacterial invasin that promotes adhesion to and invasion into human epithelial cells1-3. Possible importance in carriage. fHbp: factor H binding protein was historically thought to primarily bind to factor H, which enables bacterial survival.5,6 However, new evidence suggests its true primary function is bacterial siderophore enterobactin binding (shown in vitro).4 Furthermore, it was recently shown that NspA, another protein, binds human factor H with higher affinity and specificity than fHbp, thus supporting the possibility for this newly identified primary function.7. NHBA: neisserial heparin-binding antigen. Present in virtually all strains and binds heparin, which may increase the serum resistance of bacteria8-10. NZ PorA 1.4: porin A. Major outer membrane vesicles protein—produces robust antibody response. References: Comanducci M, et al. NadA, a novel vaccine candidate of Neisseria meningitidis. J Exp Med. 2002;195: Capecchi B, et al. Neisseria meningitidis NadA is a new invasin which promotes bacterial adhesion to and penetration into human epithelial cells. Mol Microbiol. 2005;55: Mazzon C, et al. IFN-gamma and R-848 dependent activation of human monocyte-derived dendritic cells by Neisseria meningitidis adhesin A. J Immunol. 2007;179: Veggi D, et al. Presented at IPNC. Banff, Canada. September 11-16, Madico G, et al. The meningococcal vaccine candidate GNA1870 binds the complement regulatory protein factor H and enhances serum resistance. J Immunol. 2006;177: Schneider MC, et al. Functional significance of factor H binding to Neisseria meningitidis. J Immunol. 2006;176: Lewis LA, et al. The meningococcal vaccine candidate neisserial surface protein A (NspA) binds to factor H and enhances meningococcal resistance to complement. PLoS Pathog. 2010;6:e Serruto D, et al. Neisseria meningitidis GNA2132, a heparin-binding protein that induces protective immunity in humans. Proc Natl Acad Sci U S A. 2010;107: Welsch JA, et al. Antibody to genome-derived neisserial antigen 2132, a Neisseria meningitidis candidate vaccine, confers protection against bacteremia in the absence of complement-mediated bactericidal activity. J Infect Dis. 2003;188: Plested JS, Granoff DM. Vaccine-induced opsonophagocytic immunity to Neisseria meningitidis group B. Clin Vaccine Immunol. 2008;15:")
24
a La prima dose deve essere somministrata all’età di 2 mesi
a La prima dose deve essere somministrata all’età di 2 mesi. La sicurezza e l’efficacia di Bexsero nei lattanti di età inferiore alle 8 settimane di vita non sono state stabilite. Non vi sono dati disponibili. b Vedere paragrafo 5.1. La necessità e la tempistica per ulteriori dosi di richiamo non sono ancora state determinate. c Vedere paragrafo 5.1. * Non sono disponibili dati in adulti di età pari o superiore ai 50 anni.

25
Pertosse

26
La pertosse è sotto-diagnosticata negli adulti e negli adolescenti
La diagnosi di pertosse negli adulti è difficile da porre La reale incidenza della malattia è maggiore di quanto non sia effettivamente notificato Il reservoir di infezione e il potenziale di trasmissione è maggiore di quanto stimato La sintomatologia è simile a quella di altre infezioni respiratorie Le infezioni reali potrebbero essere fino a 160 volte maggiori di quelle notificate

27
Malattie che possono essere confuse con la pertosse
Adenovirus Mycoplasma pneumoniae Clamidia Virus Respiratorio Sinciziale Polmoniti Bronchioliti Corpi estranei nell’albero respiratorio Asma Malattia Polmonare Cronico-ostruttiva

28
Pertussis vaccine in EU
Mandatory and recommended vaccination in the EU, Iceland and Norway: results of the VENICE 2010 survey on the ways of implementing national vaccination programmes M Haverkate, F D’Ancona, C Giambi, K Johansen, P L Lopalco, V Cozza, E Appelgren published on 31 May 2012 (modificata) Pertussis vaccine in EU Austria RA Belgium Bulgaria MA Cyprus Czech Rep. Denmark Estonia Finland France Germany Greece Hungary Iceland Ireland Italy RA Latvia MA Lithuania Luxembourg Malta Netherlands Norway Poland Portugal Romania Slovakia Slovenia Spain Sweden U.K. A: Absence of recommendation, MA: Mandatory for all; MR: M. for people at risk; R: Recommended; RA: R. for all; RR: R. for people at risk
 Pertussis vaccine in EU. Austria. RA. Belgium. Bulgaria. MA. Cyprus. Czech Rep. Denmark. Estonia. Finland. France. Germany. Greece. Hungary. Iceland. Ireland. Italy. RA. Latvia. MA. Lithuania. Luxembourg. Malta. Netherlands. Norway. Poland. Portugal. Romania. Slovakia. Slovenia. Spain. Sweden. U.K. A: Absence of recommendation, MA: Mandatory for all; MR: M. for people at risk; R: Recommended; RA: R. for all; RR: R. for people at risk.")
29
29

30
Duration of Immunity Against Pertussis After Natural Infection or Vaccination
Wendelboe Aaron M., Van Rie Annelies, Salmaso Stefania, Englund Janet A. malattia vaccinazione 4-12 anni 4-20 anni The Pediatric Infectious Disease Journal • Volume 24, Number 5, May 2005 30

31
2, 4, 6, 15-18, 4-6 a, 11-12 a Figure 1. Annual Rate of Pertussis and Vaccination History in the Entire Health-Plan Population, According to Age, during the Pertussis Outbreak from January 2010 through June 2011. The annual rate of pertussis (the number of cases per 100,000 person-years) for each age was calculated as follows: all cases of pertussis confirmed by a positive polymerase-chain-reaction (PCR) assay were divided by all personyears at risk and then multiplied by 100,000. Age was calculated on the date of the PCR test (for persons counted in the numerator) and on the last date of each month (for persons counted in the denominator). The percentage of members as of August 14, 2010, who were likely to have received diphtheria, tetanus, and acellular pertussis (DTaP) vaccine for all five doses (i.e., none of the doses were whole-cell pertussis vaccines) was calculated from population-based data on the timing of the transition in the health plan from diphtheria, tetanus, and whole-cell pertussis vaccines to DTaP vaccine. August 14, 2010, was the midpoint of cases (the median diagnosis date) during the 18-month period. Annual Rate of Pertussis and Vaccination History in the Entire Health-Plan Population, According to Age, during the Pertussis Outbreak from January 2010 through June 2011
 for each age was calculated as follows: all cases of pertussis confirmed by a positive polymerase-chain-reaction (PCR) assay were divided by all personyears at risk and then multiplied by 100,000. Age was calculated on the date of the PCR test (for persons counted in the numerator) and on the last date of each month (for persons counted in the denominator). The percentage of members as of August 14, 2010, who were likely to have received diphtheria, tetanus, and acellular pertussis (DTaP) vaccine for all five doses (i.e., none of the doses were whole-cell pertussis vaccines) was calculated from population-based data on the timing of the transition in the health plan from diphtheria, tetanus, and whole-cell pertussis vaccines to DTaP vaccine. August 14, 2010, was the midpoint of cases (the median diagnosis date) during the 18-month period. Annual Rate of Pertussis and Vaccination History in the Entire Health-Plan Population, According to Age, during the Pertussis Outbreak from January 2010 through June")
32
Antigeni della Bordetella pertussis considerati efficaci nel conferire difese contro la pertosse
Pertactina (P) Tossina della pertosse (TP) Emoagglutinina filamentosa (EF) Antigene delle fimbrie 2 (F2) Antigene delle fimbrie 3 (F3)
 Tossina della pertosse. (TP) Emoagglutinina filamentosa. (EF) Antigene delle fimbrie 2. (F2) Antigene delle fimbrie 3. (F3)")
33
COMPOSIZIONE QUALITATIVA E QUANTITATIVA
Infanrix hexa Polio Infanrix (DTPa) Boostrix (dTpa)/Polioboostrix Dopo ricostituzione, 1 dose (0,5 ml): Tossoide difterico ≥ 30 UI Tossoide tetanico ≥ 40 UI Bordetella pertussis: Tossoide pertossico : 25 mcg Emoagglutinina filamentosa: 25 mcg Pertactina: 8 mcg Epatite B : 10 mcg Polisaccaride Haemophilus tipo b: 10 mcg Poliomielite (inattivati) : tipo 1 (ceppo Mahoney) 40 D- unità antig. tipo 2 (ceppo MEF-1) 8 D- unità antig. tipo 3 (ceppo Saukett) 32 D- unità antig. vaccinazione primaria e di richiamo (booster). Non deve essere somministrato in bambini con età superiore ai 36 mesi. Tossoide pertossico: 25 mcg Assente Poliomielite (inattivati): tipo 1 (ceppo Mahoney) 40 D-unità antig. tipo 2 (ceppo MEF-1) 8 D-unità antig. tipo 3 (ceppo Saukett) 32 D-unità antig. richiamo a partire dai 16 mesi a 13 anni età inclusa Tossoide difterico ≥ 2 UI Tossoide tetanico ≥ 20 UI Tossoide pertossico: 8 mcg Emoagglutinina filamentosa: 8 mcg Pertactina: 2,5 mcg richiamo a partire dai 4 anni età
 Boostrix (dTpa)/Polioboostrix. Dopo ricostituzione, 1 dose (0,5 ml): Tossoide difterico ≥ 30 UI. Tossoide tetanico ≥ 40 UI. Bordetella pertussis: Tossoide pertossico : 25 mcg. Emoagglutinina filamentosa: 25 mcg. Pertactina: 8 mcg. Epatite B : 10 mcg. Polisaccaride Haemophilus tipo b: 10 mcg. Poliomielite (inattivati) : tipo 1 (ceppo Mahoney) 40 D- unità antig. tipo 2 (ceppo MEF-1) 8 D- unità antig. tipo 3 (ceppo Saukett) 32 D- unità antig. vaccinazione primaria e di richiamo (booster). Non deve essere somministrato in bambini con età superiore ai 36 mesi. Tossoide pertossico: 25 mcg. Assente. Poliomielite (inattivati): tipo 1 (ceppo Mahoney) 40 D-unità antig. tipo 2 (ceppo MEF-1) 8 D-unità antig. tipo 3 (ceppo Saukett) 32 D-unità antig. richiamo a partire dai 16 mesi a 13 anni età inclusa. Tossoide difterico ≥ 2 UI. Tossoide tetanico ≥ 20 UI. Tossoide pertossico: 8 mcg. Emoagglutinina filamentosa: 8 mcg. Pertactina: 2,5 mcg. richiamo a partire dai 4 anni età.")
34
Queenan AM et al. 368;6: february 7, 2013
Pertactin-Negative Variants of Bordetella pertussis in the United States Queenan AM et al. 368;6: february 7, 2013 * IS denotes insertion sequence, PFGE pulsed-field gel electrophoresis, and STOP stop codon.

35
Reduced Risk of Pertussis Among Persons Ever Vaccinated With Whole Cell Pertussis Vaccine Compared to Recipients of Acellular Pertussis Vaccines in a Large US Cohort Maxwell A. Witt, Larry Arias, Paul H. Katz, Elizabeth T. Truong, and David J. Witt Clinical Infectious Diseases 2013 (1 May);56(9):1248–54 3.2 milion population person 8-20 years 904 cases of pertussis identificated In the combined 5 and 6 dose groups, those who received only acellular vaccines had a 5.47 Relative Risk of disease compared to those with 1 or more whole cell dose (p= .001). Relative Risk 8.57 (p<.0001) Relative Risk 3.55 (p<.0001) Methods. Kaiser Permanente (KP) is an integrated healthcare system with complete electronic records and a centralized laboratory. Cases of laboratory-confirmed pertussis and vaccination data for members aged 8–20 years were retrieved. Results. Among persons aged 8–20 years, 904 cases of pertussis were identified. In patients with a full history of vaccinations administered by KP, those with 5 total doses of only aP had an 8.57 relative risk (RR) of pertussis (P < .0001) contrasted to those with ≥1 wP dose. With 6 doses of aP, the RR of disease was 3.55 (P < .0001). When external vaccine records were included, the results were similar. This would temporally correlate to the introduction of the aP vaccine in 1991, which had completely supplanted vaccination with wP vaccine in the United States by 2001. Mean time since last dose of vaccine among cases, with 95% confidence interval shown
;56(9):1248– milion population person 8-20 years. 904 cases of pertussis identificated. In the combined 5 and 6 dose. groups, those who received only acellular vaccines had a Relative Risk of disease compared to those with 1 or more whole cell dose. (p= .001). Relative Risk (p<.0001) Relative Risk (p<.0001) Methods. Kaiser Permanente (KP) is an integrated healthcare system with complete electronic records and a. centralized laboratory. Cases of laboratory-confirmed pertussis and vaccination data for members aged 8–20 years. were retrieved. Results. Among persons aged 8–20 years, 904 cases of pertussis were identified. In patients with a full. history of vaccinations administered by KP, those with 5 total doses of only aP had an 8.57 relative risk (RR) of. pertussis (P < .0001) contrasted to those with ≥1 wP dose. With 6 doses of aP, the RR of disease was (P < .0001). When external vaccine records were included, the results were similar. This would temporally correlate to the introduction of the aP vaccine in 1991, which had completely supplanted vaccination with wP vaccine in the United States by Mean time since last dose of vaccine among cases, with 95% confidence interval shown.")
36
Il ruolo fondamentale di una valida sorveglianza epidemiologica
L’importanza di condividere il sistema di monitoraggio delle coperture vaccinali Il ruolo fondamentale di una valida sorveglianza epidemiologica la conoscenza dei germi etiologicamente implicati, è molto utile, infatti, per valutare l’impatto della vaccinazione sia per indicare, eventualmente, ulteriori misura preventive

37
Grazie PNV 2005-2007 Non tutte le Regioni per la vaccinazione
In offerta attiva Efficacia e sicurezza Postumi gravemente invalidanti Borgo S Lorenzo Veneto e Liguria 1 dose

39
Meningococcal vaccines: WHO position paper
For monovalent MenC conjugate vaccine one single intramuscular dose is recommended for children aged ≥12 months, teenagers and adults. Children 2–11 months of age require 2 doses administered at an interval of at least 2 months and a booster about 1 year thereafter. If the primary series is interrupted, vaccination should be resumed without repeating the previous dose.

40
Advisory Committee on Immunization Practices (ACIP) Recommended Immunization Schedules for Persons Aged 0 Through 18 Years and Adults Aged 19 Years and Older — United States, 2013 13. Meningococcal conjugate vaccines (MCV). (Minimum age: 6 weeks for Hib-MenCY, 9 months for Menactra [MCV4-D], 2 years for Menveo [MCV4-CRM]). Routine vaccination: • Administer MCV4 vaccine at age 11–12 years, with a booster dose at age 16 years. • Adolescents aged 11 through 18 years with human immunodeficiency virus (HIV) infection should receive a 2-dose primary series of MCV4, with at least 8 weeks between doses. See MMWR 2011; 60:1018–1019 available at: • For children aged 9 months through 10 years with high-risk conditions, see below. Catch-up vaccination: • Administer MCV4 vaccine at age 13 through 18 years if not previously vaccinated. • If the first dose is administered at age 13 through 15 years, a booster dose should be administered at age 16 through 18 years with a minimum interval of at least 8 weeks between doses. • If the first dose is administered at age 16 years or older, a booster dose is not needed.
. (Minimum age: 6 weeks for Hib-MenCY, 9 months for Menactra [MCV4-D], 2 years for Menveo [MCV4-CRM]). Routine vaccination: • Administer MCV4 vaccine at age 11–12 years, with a booster dose at age 16 years. • Adolescents aged 11 through 18 years with human immunodeficiency virus (HIV) infection should receive a 2-dose primary series of MCV4, with at least 8 weeks between doses. See MMWR 2011; 60:1018–1019 available at: • For children aged 9 months through 10 years with high-risk conditions, see below. Catch-up vaccination: • Administer MCV4 vaccine at age 13 through 18 years if not previously vaccinated. • If the first dose is administered at age 13 through 15 years, a booster dose should be administered at age 16 through 18 years with a minimum interval of at least 8 weeks between doses. • If the first dose is administered at age 16 years or older, a booster dose is not needed.")
41
Raccomandazioni in Italia Molise (BUR Molise 1/2/2012)
Offerta attiva e gratuita di 1 dose di MenACWY-CRM per i soggetti a rischio (>12 anni di età). In questa categoria rientrano soggetti a rischio perchè affetti da patologie o per le condizioni di vita (es. situazione epidemiologica ad alto rischio, stili di vita o altre indicazioni).
. In questa categoria rientrano soggetti a rischio perchè affetti da patologie o per le condizioni di vita (es. situazione epidemiologica ad alto rischio, stili di vita o altre indicazioni).")
42
Raccomandazioni in Italia Sicilia (D.A.0820/12)
Informazione attiva e Offerta in co-payment di 1 dose di MenACWY-CRM: Adolescenti nella coorte anni Offerta attiva e gratuita di 1 dose di MenACWY-CRM: Soggetti a rischio di malattia meningococcica Viaggiatori internazionali

43
Raccomandazioni per categorie a rischio
Emilia Romagna 26 Marzo 2012 Offerta gratuita di MenACWY-CRM per i soggetti a rischio con la schedula: 2 dosi somministrare con 2 mesi di intervallo

44
Raccomandazioni per categorie a rischio Veneto
6 Agosto 2012 Offerta gratuita di MenACWY-CRM per i soggetti a rischio con la schedula: 2 dosi somministrare con 2 mesi di intervallo + dosi booster ogni 5 anni

46
Riduzione del rischio di pertosse nei nuovi nati mediante la
strategia del “cocooning”: consiste nella vaccinazione massiccia di tutti coloro che vivono o hanno contatti con il lattante e che non sono in regola con le scadenze vaccinali es.: madri, padri, fratelli e sorelle e persino i nonni e le nonne

47
Pertussis vaccines: WHO position paper

48
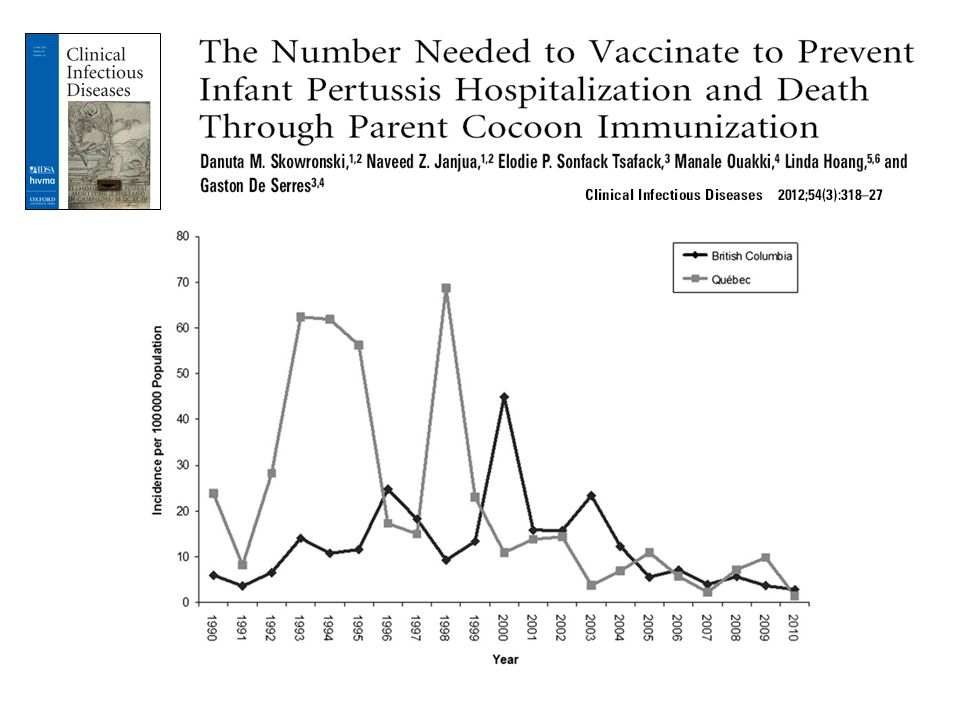
Background. Parental immunization has been recommended as a ‘‘cocoon’’ strategy to prevent serious pertussis outcomes in early infancy. We illustrate the high number needed to vaccinate (NNV) for this program based on recent epidemiologic data from the provinces of Que´bec and British Columbia (BC), Canada. Methods. Surveillance trends were summarized for the period 1990–2010. Hospitalization, intensive care unit (ICU) admission, and mortality data were compiled from 2000 to The proportion of infant pertussis attributed to a parent was estimated at 35%, explored up to 55%. Adult vaccine efficacy (VE) was estimated at 85%. The NNV was calculated as [2 parents/(parent-attributable infant risk 3 parent VE)]. To capture at least 1 recent cyclical peak, NNV was derived for the period 2005–2009 and explored for peak/trough years.
 admission, and mortality data were compiled from 2000 to The proportion of infant pertussis attributed to a parent was estimated at 35%, explored up to 55%. Adult vaccine efficacy (VE) was estimated at 85%. The NNV was calculated as [2 parents/(parent-attributable infant risk 3 parent VE)]. To capture at least 1 recent cyclical peak, NNV was derived for the period 2005–2009 and explored for peak/trough years.")
50
The NNV for parental immunization was:
Conclusions. In the context of low pertussis incidence, the parental cocoon program is inefficient and resource intensive for the prevention of serious outcomes in early infancy. Regions contemplating the cocoon program should consider the NNV based on local epidemiology. Result: For the period 2005–2009, the risk of infant hospitalization and ICU admission was 57 and 7, respectively, per in Que´bec and 33 and 7, respectively, per in BC. In both provinces the risk of infant pertussis-related death over that period was 0.5 per The NNV for parental immunization was: at least 1 million to prevent 1 infant death, approximately for ICU admission, and for hospitalization.

Presentazioni simili