Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Il bioterrorismo e la biosicurezza. Analisi e prospettive bioetiche.
R. Sinno Docente di Bioetica ISSR di Benevento Facoltà Teologica Italia meridionale. Docente di Bioetica Master Università di Bari.

2
Il controllo dei danni alla popolazione, indotti dagli attacchi del bioterrorismo, ha generato una maggiore attenzione internazionale riguardo i programmi della biosicurezza.

3
“Sadly the world has changed. The threat of bioterrorism
is real and growing.” Il mondo è tristemente cambiato. La minaccia del bioterrorismo è reale ed è in crescita. Margaret Hamburg M.D., Conference of Department of Health and Human Services, F.D.A., “The bioterrorism today”, N.Y., 2009.

4
Biological Terrorism Use of biological agents to intentionally produce disease or intoxication in susceptible populations: humans, animals, or plants - to meet terrorist aims. E’ l’uso intenzionale di agenti biologici capaci di generare malattie o intossicazioni in popolazioni umane sensibili, in animali o piante- con lo scopo di generare terrore.

5
Physician Bioterrorism Training, v2
Wednesday, March 29, 2017 Biological Terrorism Intentional or threatened use of viruses, bacteria, fungi or toxins from living organisms to produce death or disease in humans, animals or plants. Bioterrorism definition of the Centers for Disease Control and Prevention. Senza minaccia non si parla di bioterrorismo Biosgna notare la varietà di agenti che possono essere usati : virus, batteri , funghi e tossine che possono essere prodotti in laboratorio. UCLA Center for Public Health and Disasters,

6
ATTACCO? PREVENZIONE!

7
Biological Terrorism – Why?

8
Primo traguardo: effetti devastanti;
Agenti invisibili,rapidamente letali; Possibilmente insapori ed inodori; Da reperire con facilità; Con tracce difficili da testare; Capaci di aggredire la popolazione inerme; Capaci di generare effetti ritardati; terrore e caos incontrollabili. Z.Tamiza Teja , MD., Cordinator Project Bioterrorism and Health Preparedness, CDC,in Bioterrorism Training for Physician, Updated March 2003.

9
The CDC classifies bioterrorist agents into 3 categories: A, B and C based on the combined factors of availability of the agent, potential for morbidity and mortality, and easy of dissemination. La classificazione CDC degli agenti capaci di generare bioterrismo è di tre tipi A B C si basa sulla combinazione della disponibiltà degli agenti, sulla potenza nel generaare morbilità e mortalità e sulla facilità della disseminazione.

10
Gli agenti della Classe A sono internazionalmente riconosciuti essere quelli con la maggiore potenza d’uso di armi biologiche.

11
Caratteristiche degli Agenti Classe A
Alta priorità nella loro pericolosità globale ; possono essere areorolizzaati e hanno un alta trasmissibilità determinano sovvertimento

12
Facile trasmissione e disseminazione
Alta pericolosità globale Facile trasmissione e disseminazione Alta mortalita’ Causa di distruzione sociale Incapacita’ di difesa

13
Agenti della classe A Anthrax Botulism Plague Smallpox Tularemia
Viral Hemorrhagic Fevers Ebola infection’s Argentine hemorrhagic fever ALTA’ MORTALITA’ Bacillus antracis, clostridium botulinum, yersina pestis, variola major,

14
Caratteristiche degli Agenti Classe B

15
FACILE DISSEMINAZIONE
RIDOTTO RISCHIO DI MORTALITA’ ELEVATA MORBILITA’ DANNI CRONICI DEVASTANTI

16
Agenti della classe B Q Fever Brucellosi Febbre Equina
Encefalopatie virali Tetano(clostridium perfigens) Dissenterie da Salmonella-shigella E. Coli Vibrione cholera Enterotossine streppococciche ALTA’ MORBILITA’
 Dissenterie da Salmonella-shigella. E. Coli. Vibrione cholera. Enterotossine streppococciche. ALTA’ MORBILITA’")
17
Caratteristiche degli Agenti Classe C

18
DETERMIANANO EMERGENZE
PATOGENI COMUNI CHE DETERMIANANO EMERGENZE UTILIZZO IMPROPRIO DI MATERIALE BIOLOGICO SINTETICO O SEMISINTETICO.

19
Agenti della classe C Virus influenzali modificati
Febbre emorragica da zecca tifo Febbre gialla Tubercolosi Infezioni fungine resisenti Enfefalite da zecca dei castori. CO- MORBILITA’

20
DI UN AGENTE BIOLOGICO:
POTENZA IDEALE DI UN AGENTE BIOLOGICO: Produzione a basso costo; Elevata mortalità; Può essere areosolizzato (1- 10 mµ); Sopravvivenza giornaliera; Facile trasmissibilità; Profilassi e trattamenti non efficaci.
; Sopravvivenza giornaliera; Facile trasmissibilità; Profilassi e trattamenti non efficaci.")
21
Bioterrorism – Early historY!

22
Gli Assiri usavano l’Ergotamina
sui prigionieri a dosi tossiche .

23
I Romani infettavano le acque dei nemici con animali morti.
Tale pratica si estese a tutto il Medio-evo.

24
the Tartars catapulted dead bubonic plague victims.
L. Kallus, MD, Bioterrorism, Emergency Medicine Department Suny, Conference “The Bioterrorism today”, NY, 2009.

25
per l’uso di coperte infette
Guerra Franco - Inglese (1763). Gli indiani furono sterminati per l’uso di coperte infette di vaiolo.
. Gli indiani furono sterminati. per l’uso di coperte infette. di vaiolo.")
26
BIOTERRORISMO MODERNO

27
Nella Prima guerra mondiale,
, fu istituito un programma di attacco-difesa (somministrazione di antrace) Sia da parte dell’esercito Tedesco, sia francese.
 Sia da parte dell’esercito. Tedesco, sia francese.")
28
NEL 1931 FU ISTITUITA L’UNITA’ 731 DELL’ESERCITO GIAPPONESE,
DEDICATO ALLA GUERRA BATTERIOLOGICA.

29
Nel 1931 i giapponesi usarono
Sui prigionieri inoculazioni Batteriche a scopo di ricerca.

30
Nel periodo della II guerra Mondiale, l’esercito inglese
Studiò la possibilità di Dispersione di antrace.

31
L’esercito tedesco contaminò Le isole gruinard, vicino alla
Scozia, con un infezione di Spore di antrace.

32
NEL 1942 SI AVVIA IL PROGRAMMA DEGLI U.S.A.
NEL 1956 L’URSS ACCUSA GLI USA DI AVER USATO ARMI BIOLOGICHE IN COREA.

33
NEL 1950 SI AVVIA IL PROGRAMMA DI DIFESA TERRITORIALE DEGLI U.S.A.
NEL 1960 ATTACCO CON MICROSFERE DI SERRATIA. NELLA CITTA’ DI S. FRANCISCO SI CONTANO DECINE DI INTOSSICATI CON 1 MORTO

34
Di b. subtilis Nella S.W. Della città Di N.Y.
Nel 1966 Dispersione Di b. subtilis Nella S.W. Della città Di N.Y.

35
NEL 1970 INCIDENTE A SVERDLOSK
MENTRE SI PRODUCEVA ANTRACE. VI FURONO 66 VITTIME E CENTINAIA DI INTOSSICATI

36
NEL 1992 L’URSS DICHIARAVA DI INTERROMPERE LA PRODUZIONE DI ANTRACE.

37
I MEMBRI DEL CULTO RAJNEESHEE
INFETTANO, CON SPORE DI SALMONELLA, CIBI IN UN RISTORANTE DELL’OREGON. SI VERIFICA UN INFEZIONE GRAVE IN 700 PERSONE.

38
Rajneeshee Cult, Salmonella Oregon, 1984

39
SI STIMA UN CENTINAIO DI INTOSSICATI DAL CAFFE.
NEL 1991 ATTACCO DA PARTE DEI MILIZIANI DEL MOVIMENTO PATRIOTTICO DEL MINESSOTA CON SOLUZIONE DI ESTRATTI DI OLIO DI RICINO. SI STIMA UN CENTINAIO DI INTOSSICATI DAL CAFFE.

40
MN Patriots Council, Douglas County, 1991.

41
Sarin Gas Attack, Tokyo Subway, 1995

42
ATTACCO POSTALE CONTEMPORANEO NEL 2001. SPORE DI ANTRACE.
STATI FL.,W. D.C., N.Y., NJ.

43
FURONO CONTAMINATI CIRCA UN CENTINAIO DI PERSONE, 25
INTOSSICATI GRAVI, CON 5 DECEDUTI PER SINDROME PNEUMONICA DA ANTRACE E 20 CON LESIONI CUTANEE GRAVI E PERMANENTI(PERDITA DELLA VISTA, LESIONI INVALIDANTI ARTI SUPERIORI).
.")
44
NEL 2010 NUOVO ATTACCO POSTALE
CON SPORE DI ANTRACE IN U.K. L’ATTENTA SORVEGLIANZA RIDUCE I CONTAMINATI AD UNA DECINA. SI CONTANO DUE CASI INVALIDANTI

45
ARE YOU PREPARED?

47
SITUAZIONI FUNZIONALI-OPERATIVE DIFFERENTI.
ATTACCO CONCLAMATO IN ATTO ATTACCO NON CONCLAMATO E NASCOSTO.

48
OVERT ATTACK

49
Un attacco conclamato si realizza quando il rilascio di un agente
è annunciato. La comunicazione tra le forze dell'ordine, della salute pubblica, l’ assistenza sanitaria, e donatori, è fondamentale per fornire un trattamento adeguato delle vittime potenziali.

50
UN ATTACCO CONCLAMATO DETERMINA:
COORDINAZIONE E VALIDITA’ DEL SISTEMA DI RISPOSTA ATTIVAZIONE DELLA RETE OSPEDALIERA E SANITARIA INFORMAZIONE SOCIALE, INTERVENTO DELLE FORZE SPECIALI

51
OVERT ATTACK

52
Problemi: Verificare se l’attacco è stato realmente condotto in quel luogo; Se ha generato caos e paura; Il numero delle vittime reali e quelle prevedibili; Mettere in atto le procedure della decontaminazione e isolamento della popolazione civile; Attuare I piani sanitari quali sistemi di profilassi e ulteriore prevenzione.

53
REALTA’ O INGANNO ?

54
LA CREDIBILITA’ DI OGNI PIANO DI DIFESA DAGLI ATTACCHI
BIOLOGICI, DIPENDE DALLA CAPACITA’ DI RISPOSTA, E COORDINAZIONE, ALL’EVENTO, IN UN PERIDO MASSIMO DI h.

55
COVERT ATTACK

56
sembra direttamente collegato ad un’azione annunciata o resa pubblica.
Si definisce attacco bioterroristico non conclamato, quello in cui l’evento non sembra direttamente collegato ad un’azione annunciata o resa pubblica. Tale situazione determina una risposta non specifica delle forze di bio-difesa, con riduzione della rete d’emergenza.

57
COVERT ATTACK

58
Problemi: Difficile identificazione dell’agente; Piccoli gruppi colpiti possono simulare infezioni aspecifiche; La trasmissione da contatto secondario (cibo-acqua-altre sostanze), determina difficile rintranciabilita’ della sostanza; Una sottostima iniziale e’ elemento devastante del covert attack; Difficolta’ di catalogazione da parte delle agenzie.
, determina difficile rintranciabilita’ della sostanza; Una sottostima iniziale e’ elemento. devastante del covert attack; Difficolta’ di catalogazione da parte. delle agenzie.")
59
Strategia nazionale per contrastare le minacce biologiche Consiglio nazionale per la sicurezza 2009

60
“ Quando una sostanza non è ancora riconosciuta quale effettivo mezzo
di un atto terroristico, devono essere attivate contemporaneamente tutti i dipartimenti e le agenzie federali, le strutture universitarie di ricerca, gli ospedali, per una pronta bio-difesa nazionale”.

62
INDICATORI E ASPETTI CLINICI ED
EDEPIDEMIOLOGICI DEL BIOTERRORISMO

63
Indicatori di un attacco B.T.
MORTE O MALATTIE DI BRANCHI DI ANIMALI MANIFESTAZIONI CLINICHE STAGIONALI ATIPICHE MALATTIE NON USAULMENTE ENDEMICHE PATOGENI RESISTENTI AI FARMACI.

64
Physician Bioterrorism Training, v2
Wednesday, March 29, 2017 Anthrace Origine : Bacillus anthracis; Produzione di spore e tossine; Effetti cutanei, inalatori , intestinali. Anthrax is the most notorious agent because it was used in the mail-related cases in fall of 2001 Caused by the bacterium Bacillus anthracis Note the ‘boxcar’ appearance of the bacilli in this picture. The bacteria produce spores which then enter the body in three ways forming the three forms of illness. The same bacteria is the cause of 3 forms of illness: cutaneous, inhalational, and intestinal The spores can stay dormant in the body, but illness will result once the toxins produced by activated spores are released. Anthrax is highly stable in the environment. It forms spores that are resistant to drying and sunlight. Therefore they could be aerosolized and distributed effectively (Gordon, 1999). Article References: Inglesby TV, O’Toole T, Henderson DA, et al. Anthrax as a biological weapon, JAMA 2002;287: Gordon SM. The threat of bioterrorism: A reason to learn more about anthrax and smallpox. Cleveland Clinic J of Medicine ;66(10): Dixon TC, Meselson M, Guillemin J, Hanna PC. Anthrax. New Engl J Med 1999; 341: Friedlander AM, Pittman PR, Parker GW. Anthrax vaccine. JAMA 1999;282: CDC. Update: Investigation of anthrax related to intentional exposure and interim public health guidelines. MMWR October 19, 2001;50(41): CDC. Update: Investigation of Bioterrorism-Related Anthrax and Interim Guidelines for Exposure Management and Antimicrobial Therapy. MMWR October 26, 2001;50(42): CDC. Update: Investigation of Bioterrorism-Related Anthrax and Interim Guidelines for Clinical Evaluation of Persons with Possible Anthrax. MMWR November 02, 2001;50(43):941-8. UCLA Center for Public Health and Disasters,
. Article References: Inglesby TV, O’Toole T, Henderson DA, et al. Anthrax as a biological weapon, JAMA 2002;287: Gordon SM. The threat of bioterrorism: A reason to learn more about anthrax and smallpox. Cleveland Clinic J of Medicine. 1999;66(10): Dixon TC, Meselson M, Guillemin J, Hanna PC. Anthrax. New Engl J Med 1999; 341: Friedlander AM, Pittman PR, Parker GW. Anthrax vaccine. JAMA 1999;282: CDC. Update: Investigation of anthrax related to intentional exposure and interim public health guidelines. MMWR October 19, 2001;50(41): CDC. Update: Investigation of Bioterrorism-Related Anthrax and Interim Guidelines for Exposure Management and Antimicrobial Therapy. MMWR October 26, 2001;50(42): CDC. Update: Investigation of Bioterrorism-Related Anthrax and Interim Guidelines for Clinical Evaluation of Persons with Possible Anthrax. MMWR November 02, 2001;50(43): UCLA Center for Public Health and Disasters,")
65
Bacillus Antracis

66
Physician Bioterrorism Training, v2
Wednesday, March 29, 2017 ANTRACE CUTANEO. Cutaneous anthrax is the most common form that occurs naturally, presents with skin ulcers, fever, adenopathy Cutaneous form occurs naturally through inoculation of skin lesions Few cases occur each year in the US, mostly in the southwest Usually responds well to treatment Photo source: Binford CH, Connor DH, eds. Pathology of Tropical and Extraordinary Diseases. Vol 1. Washington, DC: AFIP :119. UCLA Center for Public Health and Disasters,

67
INALAZIONE DI SPORE DI ANTRACE.
Physician Bioterrorism Training, v2 Wednesday, March 29, 2017 INALAZIONE DI SPORE DI ANTRACE. INCUBAZIONE : 1 – 6 GIORNI ( Raramente oltre i 60) Prodomi: 1-2 giorni di febbre elevata, malessere, disidratazione progressiva. Severo distress respiratorio, shock settico, si possono verificare forme di meningite fulminante; diagnosi Mediastinite emorragica con Rx , Tc, Pet. Di tipo standard( ricerca batteriologica e laboratorio) Bioterrorism attack would most likely use aerosol exposure as was the situation in the eastern United States in Fall, 2001 Inhalational Anthrax = Intentional Infection Clinical diagnosis: The most common incubation period for inhalation anthrax is less than one week but there have been cases with incubation periods of 30 days. Presents as vague viral-type illness progressing to severe sepsis. The patient may also have meningitis. Hemorrhagic mediastinitis is a hallmark for clinical diagnosis. Definitive lab identification: Diagnosis with a culture or gram stain of blood may be positive, but usually this only occurs late in the course of the illness. Notify a lab immediately if this agent is suspected because special tests must be done. ELISA may be better for early diagnosis, but it is not available in most labs. Isolation: This disease is not communicable from person to person; use routine Universal Precautions of gloves and mask Cues to a covert attack: The rapid fulminating course in a patient who presents with what seemed like an ordinary respiratory infection. Multiple cases in your institution, and in other health care institutions UCLA Center for Public Health and Disasters,
 Prodomi: 1-2 giorni di febbre elevata, malessere, disidratazione progressiva. Severo distress respiratorio, shock settico, si possono verificare forme di meningite fulminante; diagnosi. Mediastinite emorragica con Rx , Tc, Pet. Di tipo standard( ricerca batteriologica e laboratorio) Bioterrorism attack would most likely use aerosol exposure as was the situation in the eastern United States in Fall, Inhalational Anthrax = Intentional Infection. Clinical diagnosis: The most common incubation period for inhalation anthrax is less than one week but there have been cases with incubation periods of 30 days. Presents as vague viral-type illness progressing to severe sepsis. The patient may also have meningitis. Hemorrhagic mediastinitis is a hallmark for clinical diagnosis. Definitive lab identification: Diagnosis with a culture or gram stain of blood may be positive, but usually this only occurs late in the course of the illness. Notify a lab immediately if this agent is suspected because special tests must be done. ELISA may be better for early diagnosis, but it is not available in most labs. Isolation: This disease is not communicable from person to person; use routine Universal Precautions of gloves and mask. Cues to a covert attack: The rapid fulminating course in a patient who presents with what seemed like an ordinary respiratory infection. Multiple cases in your institution, and in other health care institutions. UCLA Center for Public Health and Disasters,")
69
PRIMA DIFESA DALL’ANTRACE

70
TRATTAMENTO DELL’ANTRACE
Physician Bioterrorism Training, v2 Wednesday, March 29, 2017 TRATTAMENTO DELL’ANTRACE ALLONTANAMENTO IMMEDIATO DALLA FONTE; SOMMINISTRAZIONE DI CIPROFLOXACINA SOMMINISTRAZIONE DI VANCOCINA, IMIPENEM, CLARITROMICINA; VIGLIANZA PARAMETRI VITALI IN UTIR; DOPO ESPOSIZIONE CIPROFLOXACINA PER 60 GIORNI , VACCINO-PROFILASSI. It was previously believed that the mortality of inhalation anthrax approached 100% even with treatment, but based on the experience in fall of 2001 we now believe that treatment may be effective if started early—Six of eleven inhalation anthrax patients survived. Prophylactic treatment can prevent patients from becoming sick if started soon after exposure. Terrorists may be likely to use strains that are resistant to penicillin or doxycycline, so quinolones would be preferred until susceptibility is known (there are no known quinolone-resistant strains) Because spores can persist in tissues for a long time, prophylactic antibiotics must be given for 60 days. This can be shortened to 30 days if vaccine is given also. However, anthrax vaccine is currently in short supply. Although ciprofloxacin is the only drug with an FDA indication for prophylaxis against aerosol anthrax, other quinolones (e.g., Levofloxacin, Moxifloxacin, Gatifloxacin) would probably also be effective. There is much debate about the safety and efficacy of anthrax vaccine in the setting of intentional aerosol exposure. Although we do not have good data on anthrax vaccine safety in large numbers of people, the incidence of systemic adverse reactions appears to be about – 0.5%. In the setting of a known or strongly suspected anthrax exposure, the potential benefit of the vaccine would likely exceed the risk. The risk/benefit balance for pre-exposure vaccination for large numbers of people is debatable, since the probability of exposure is very low for most. No randomized trials have been done in humans for intentional exposure to aerosol anthrax. A single-blind, placebo-controlled trial using the less potent form of the vaccine was conducted in goat hair mill workers in New Hampshire from The vaccine conferred statistically significant reduction in the incidence of anthrax overall (cutaneous plus inhalational) and suggested a reduction in the incidence of inhalational anthrax, but the numbers of cases of inhalational disease were too small to attain statistical significance. In addition, trials on non-human primates and guinea pigs have shown that the vaccine is effective against fatal disease due to infection by the aerosol route. Ref: Inglesby TV, O’Toole T, Henderson DA, et al. Anthrax as a biological weapon, Updated recommendations for management. JAMA May 1, 2002;287: UCLA Center for Public Health and Disasters,
 Because spores can persist in tissues for a long time, prophylactic antibiotics must be given for 60 days. This can be shortened to 30 days if vaccine is given also. However, anthrax vaccine is currently in short supply. Although ciprofloxacin is the only drug with an FDA indication for prophylaxis against aerosol anthrax, other quinolones (e.g., Levofloxacin, Moxifloxacin, Gatifloxacin) would probably also be effective. There is much debate about the safety and efficacy of anthrax vaccine in the setting of intentional aerosol exposure. Although we do not have good data on anthrax vaccine safety in large numbers of people, the incidence of systemic adverse reactions appears to be about 0.06 – 0.5%. In the setting of a known or strongly suspected anthrax exposure, the potential benefit of the vaccine would likely exceed the risk. The risk/benefit balance for pre-exposure vaccination for large numbers of people is debatable, since the probability of exposure is very low for most. No randomized trials have been done in humans for intentional exposure to aerosol anthrax. A single-blind, placebo-controlled trial using the less potent form of the vaccine was conducted in goat hair mill workers in New Hampshire from The vaccine conferred statistically significant reduction in the incidence of anthrax overall (cutaneous plus inhalational) and suggested a reduction in the incidence of inhalational anthrax, but the numbers of cases of inhalational disease were too small to attain statistical significance. In addition, trials on non-human primates and guinea pigs have shown that the vaccine is effective against fatal disease due to infection by the aerosol route. Ref: Inglesby TV, O’Toole T, Henderson DA, et al. Anthrax as a biological weapon, Updated recommendations for management. JAMA May 1, 2002;287: UCLA Center for Public Health and Disasters,")
71
Physician Bioterrorism Training, v2 Il Botulismo.
Wednesday, March 29, 2017 Sindrome Paralitica: Il Botulismo. UCLA Center for Public Health and Disasters,

72
Physician Bioterrorism Training, v2
Wednesday, March 29, 2017 BOTULINO ORIGINE : Clostridium botulinum neurotoxin TIPI A, B, E, and F LA PIU’ POTENTE TOSSINA CONOSCIUT DOSE LETALE 1 ng/kg 100,000 VOLTE PIU’ TOSSICA DI QUELLA DEL SARIN Terrorists using botulism would probably not be spreading the bacterium itself. It is more likely they would be using the purified toxin. The most potent toxin known, botulinum is 100,000 times more toxic than sarin, the agent that was used in the Tokyo subway attacks by the Aum Shinrikyo cult in 1995 (Franz, 1997). The endospores of C. botulinum, when stained using the Malachite Green staining method, will appear as green spheres, while the bacilli themselves will turn purple in color. Article References: Arnon SS, et al. Botulinum toxin as a biological weapon. JAMA 2001; 285: Franz DR et al. Clinical recognition and management of patients exposed to biological warfare agents. JAMA ;278(5): Photo Reference: CDC Public Health Image Library, Clostridium botulinum spores stained with Malachite Green Stain. Photo by: CDC/Courtesy of Larry Stauffer, Oregon State Public Health Laboratory. UCLA Center for Public Health and Disasters,
. The endospores of C. botulinum, when stained using the Malachite Green staining method, will appear as green spheres, while the bacilli themselves will turn purple in color. Article References: Arnon SS, et al. Botulinum toxin as a biological weapon. JAMA 2001; 285: Franz DR et al. Clinical recognition and management of patients exposed to biological warfare agents. JAMA. 1997;278(5): Photo Reference: CDC Public Health Image Library, Clostridium botulinum spores stained with Malachite Green Stain. Photo by: CDC/Courtesy of Larry Stauffer, Oregon State Public Health Laboratory. UCLA Center for Public Health and Disasters,")
73
Physician Bioterrorism Training, v2
Wednesday, March 29, 2017 BOTULINO INCUBAZIONE: 1-5 GIORNI; SINTOMI BLOCCO DELLE SINAPSI COLINERGIHE DIPOLIDIA, DISPFAGIA, IRRIGIDIMENTO MUSCOLARE SUCCESSIVA PARALISI FLACCIDA DIAGNOSI CLINICA TITOLAZIONE DELLA TOSSINA SIERICA. Patients are afebrile, awake and alert. Paralysis develops over hours and can last for weeks or months. Death is due to respiratory paralysis. If patients are intubated and ventilated, they will most likely have full recovery barring any other complications. Symptoms will persist for weeks to months, because synapses are permanently damaged, and patients must grow new synapses to recover Recovery may be prolonged (Franz, 1997). Article References: Arnon SS, et al. Botulinum toxin as a biological weapon. JAMA 2001; 285: Franz DR et al. Clinical recognition and management of patients exposed to biological warfare agents. JAMA ;278(5): Photo Reference: CDC Public Health Image Library, Six week old infant with botulism, which is evident as a marked loss of muscle tone, especially in the region of the head and neck, Photo by: CDC. UCLA Center for Public Health and Disasters,
. Article References: Arnon SS, et al. Botulinum toxin as a biological weapon. JAMA 2001; 285: Franz DR et al. Clinical recognition and management of patients exposed to biological warfare agents. JAMA. 1997;278(5): Photo Reference: CDC Public Health Image Library, Six week old infant with botulism, which is evident as a marked loss of muscle tone, especially in the region of the head and neck, Photo by: CDC. UCLA Center for Public Health and Disasters,")
74
SPORE DI BOTULINO AL M.E.

75
Physician Bioterrorism Training, v2
Wednesday, March 29, 2017 IL VAIOLO MAIOR Most physicians today in the United States have not seen this disease. This slide is to help familiarize physicians with what smallpox looks like. Note the concentration of the rash on the face, and less so on the trunk. The smallpox rash tends to be more peripherally distributed. Smallpox is probably the most feared bioterrorist agent. This is because of the risk of secondary spread, the lack of effective known treatment, the large portion of the population that no longer has antibodies to it, and because of the disease’s visibility and disfiguring nature. It is highly contagious, affecting about 1 in 12 people exposed. It is estimated that each case of the disease could infect 10 to 12 new contacts. A large portion of the population is susceptible because immunity wanes with time. The last known natural case was in Somalia in Since then, the only known cases were caused by a laboratory accident in 1978 in Birmingham, England, which killed one person and caused a limited outbreak. Smallpox was officially declared eradicated in 1979. Vaccinations were stopped in the United States in 1972. Smallpox could easily become reestablished in the world if it were released as a bioterrorist agent. Source: World Health Organization Communicable Disease Surveillance and Response. Frequently asked questions on smallpox, 26 October Available at: Photo Source: World Health Organization Communicable Disease Surveillance and Response Slide Set on Diagnosis of Smallpox, UCLA Center for Public Health and Disasters,

77
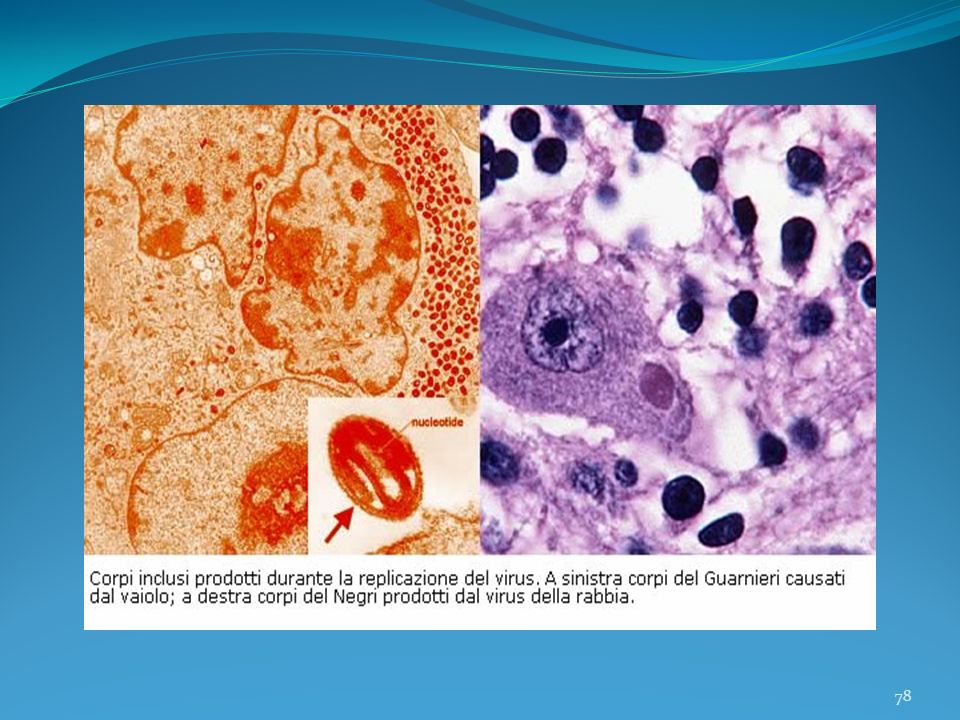
VIRUS DEL VAIOLO ALLA M. E.

79
TEAM DI ISOLAMENTO CDC

80
Laboratory Response Network for Bioterrorism
Physician Bioterrorism Training, v2 Wednesday, March 29, 2017 Laboratory Response Network for Bioterrorism This diagram shows the laboratory response network for bioterrorist agents and the referral pattern for lab specimens. Specimens first go to the on-site lab (hospital, clinic), which is usually a Level A lab. If further testing is needed or required, specimens are then referred to the local public health labs. The next level is state public health labs (typically level C) And then, if necessary, the CDC (Khan 2000). The only other Level D lab is at the United States Army Medical Research Institute for Infectious Diseases (USAMRIID). Article Reference: Khan AS, Morse S, Lillibridge S. Public-health preparedness for biological terrorism in the USA. Lancet. September 30, 2000;356: UCLA Center for Public Health and Disasters,
, which is usually a Level A lab. If further testing is needed or required, specimens are then referred to the local public health labs. The next level is state public health labs (typically level C) And then, if necessary, the CDC (Khan 2000). The only other Level D lab is at the United States Army Medical Research Institute for Infectious Diseases (USAMRIID). Article Reference: Khan AS, Morse S, Lillibridge S. Public-health preparedness for biological terrorism in the USA. Lancet. September 30, 2000;356: UCLA Center for Public Health and Disasters,")
82
Il BIOTERRORIMO PREVEDE
UNA MODERNA BIODIFESA.

83
L’APPLICAZIONE DI CONOSCENZE TECNICHE, SCIENTIFICHE ED
EQUIPAGGIAMENTI PER PREVENIRE I DANNI DA ESPOSIZIONE AD AGENTI BIOLOGICI POTENZIALMENTE LETALI. L’OBIETTIVO DELLA BIOSICUREZZA E’ RIDURRE I RISCHI DELLA CONTAMINAZIONE INDIVIDUALE E DELLA POPOLAZIONE. ISTITUTIONAL BIOSAFETY COMMITEE USA, 2009.

84
ASPETTI OPERATIVI Organizzare una formazione permanente del personale che opera nei laboratori di ricerca; Controllo e responsabilità delle autorità sanitarie, preposte alla collaborazione dei programmi di biosicurezza; Informazione della popolazione civile con successivo addestramento in caso di pericoli della salute pubblica; Verifica dei casi o incidenti nel corso degli ultimi decenni, con successiva e specifica difesa internazionale. (Indicazioni già espresse negli articoli 15 “Gestione dei rischi”, art. 17 “Misure di emergenza”, art. 20 “Scambio di informazioni”, del protocollo di Cartagena).
.")
85
the CARTAGENA PROTOCOL ON Biosafety to the Convention on Biological diversity Adopted on 29 january 2000 and entred in to The force on 11 september 2003.

86
Modern Biosafety. Dinamicità; Adattabilità; Validità internazionale; Programmazione di verifica; Una ricerca scientifica conforme alle norme internazionali di difesa della popolazione civile.

87
Il Protocollo di Ginevra redatto il 17 giugno 1925 proibiva l’uso di
gas asfissianti, veleni, antisettici, e altre sostanze biologiche quali mezzi di distruzione di massa e vietava la guerra batteriologica.

88
I limiti del protocollo di Ginevra riguardavano la possibilità che
gli stati potevano continuare le ricerche in tale settore. Si consentiva l’uso di rivalsa in caso di attacco batteriologico.

89
Ratificata a Londra, Mosca e Washington
CONVENZIONE SUL DIVIETO DELLE ARMI BIOLOGICHE DEL 1972. Tale Convenzione vieta la messa a punto, la fabbricazione e lo stoccaggio delle armi batteriologiche (biologiche) o a tossine e che disciplina la loro distruzione. Ratificata a Londra, Mosca e Washington il 10 aprile 1972.
 o a tossine e che disciplina la loro distruzione. Ratificata a Londra, Mosca e Washington. il 10 aprile")
90
PREAMBOLO Decisi di operare per l’attuazione di progressi effettivi sulla via dei disarmo completo, compreso il divieto e la soppressione di tutti i tipi d’armi di distruzione di massa, e convinti che il divieto della messa in punto, della fabbricazione e della giacenza di armi chimiche e batteriologiche (biologiche), come anche la loro distruzione con provvedimenti efficaci contribuiranno all’attuazione del disarmo generale completo sotto uno stretto ed efficace controllo internazionale......
, come anche la loro distruzione con provvedimenti efficaci contribuiranno all’attuazione del disarmo generale completo sotto uno stretto ed efficace controllo internazionale")
91
Art. I Ciascuno Stato partecipe della presente Convenzione s’impegna a mai e in nessuna circostanza mettere in punto, fabbricare, tenere in deposito o acquistare in un modo o nell’altro né conservare: 1. agenti microbiologici e altri agenti biologici come anche tossine, qualunque ne sia l’origine o il modo di produzione, di tipo e in quantità non destinati a fini profilattici, di protezione o ad altri fini pacifici; 2. armi, equipaggiamento e vettori destinati all’impiego di tali agenti o tossine a fini ostili e in conflitti armati.

92
CONVENZIONE DELLA PROIBIZIONE
DELLE ARMI CHIMICHE (PARIGI 1993)
")
93
PREVEDE LA MESSA A BANDO DI TUTTE LE SOSTANZE CHIMICHE
ENTRO IL 2007, CON PROROGA ENTROIL 2012.

95
RISOLUZIONE ONU CONTRO IL BIOTERRORIMO MAGGIO 2007.
APPROVAATA NELL’ASSEMBLEA GENERLE DEL 2008.

96
PUNTI SALIENETI DELLA RISOLUZIONE:
Esplorazione degli strumenti innovativi per la prevenzione verso obiettivi particolarmente sensibili; Rafforzamento della cooperazione per il controllo del riciclaggio di fondi che finanziano gruppi terroristici.

98
BIOTERRORISMO E BIOETICA?
Why?

99
ARE YOU PREPARED?

100
EFFETTI DIRETTI E INDIRETTI

101
EFFETTI DIRETTI PAURA INCONTROLLATA; ANGOSCIA; TERRORE.

102
LA PAURA INCONTROLLATA RIGUARDA IL RAPPORTO TRA
LA COSCIENZA (COMPORTAMENTI- SCELTE-OBIETTIVI), E LA PERCEZIONE DEL GRADO EFFETTIVO DI DIFESA ATTUABILE.
, E LA PERCEZIONE. DEL GRADO EFFETTIVO. DI DIFESA ATTUABILE.")
103
L’ANGOSCIA DI UN ATTACCO BIOTERRORISTICO RIDUCE LA FIDUCIA
NELL’ORGANIZZAZIONE SOCIALE.

104
IL TERRORE DELLE ARMI BIOLOGICHE FA EMERGERE UN SENSO DI IMPOTENZA COLLETTIVA.

105
GLOBALE QUALE PRINCIPIO DI ALLEANZA E TUTELA DEL VALORE DELLA VITA.
UNA VULNERABILTA’ GLOBALE QUALE PRINCIPIO DI ALLEANZA E TUTELA DEL VALORE DELLA VITA.

107
GLI EFFETTI INDIRETTI INDAGANO
I PERCORSI PRECAUZIONALI NELLA RICERCA E PRODUZIONE DEL MATERIALE BIOLOGICO.

108
GLI EFFETTI DIRETTI E INDIRETTI COMPORTANO UN NECESSARIO E
DELICATO EQUILIBRIO TRA INFORMAZIONE AL CITTADINO E MOTIVAZIONI DI DIFESA GLOBALE.

109
ABBIAMO IN MENTE UNA NON REALE
IDEA DI SICUREZZA GLOBALE. SI DEVE CONSIDERARE CHE NON POTREMO MAI ESSERE protetti SOLO TENENDO CONTO DEI DATI SCIENTIFICI O POLITICI. SERVE UNA PRESA D’ATTO DELLE NOSTRE LIBERE COSCIENZE DELLA REALE MINACCIA DI DISTRUZIONE DI TUTTO IL NOSTRO SISTEMA.

110
RICERCA DELLA BIODIFESA COMPORTA UN INCREMENTO,
“OGNI PROGRAMMA NELLA RICERCA DELLA BIODIFESA COMPORTA UN INCREMENTO, IN QUELLA DELLA BIO-OFFESA”. J. M. Haas , Ethical Challanges of Bioterrorism in “ Ethics and Medicine”, 2002, 27(1), 1.
, 1.")
111
LA QUESTIONE DEL BIOTERRORISMO
PONE LE BASI PER UNA RICERCA DI EQUILIBRIO TRA LIBERTA’ INDIVIDUALE E BENE COMUNE.

112
RISORSA E APPRODO DI OGNI
UN BENE COMUNE CHE SIA RISORSA E APPRODO DI OGNI PERCORSO UMANO.

113
UNA LIBERTA’ CHE SIA SVINCOLATA DALLE DERIVE IDEOLOGICHE,
CHE EVITI LE DRAMMATICHE SOPRAFFAZIONI DELL’UOMO SU OGNI SUO SIMILE.

Presentazioni simili