Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
BIOPSIA DELLE MASSE RENALI
Come, quando e perché ?

2
RUOLO TRADIZIONALE DELLA BIOPSIA DELLE MASSE RENALI
Diagnosi di malattia metastatica in pazienti con una nota neoplasia primitiva extrarenale Diagnosi di ascesso renale o linfoma Conferma istologica di un tumore primitivo renale in presenza di malattia metastatica disseminata o di una massa retroperitoneale non resecabile chirurgicamente Because treatment is nonsurgical in these cases.

3
BIOPSIA DELLA MASSE RENALI
INCERTEZZE STORICHE SICUREZZA Rischio di sanguinamento Rischio di seeding TECNICA Rischio di prelievo non diagnostico Errori di campionamento (eterogeneità intratumorale) EFFICACIA Accuratezza diagnostica Impatto sulle decisioni cliniche
 EFFICACIA. Accuratezza diagnostica. Impatto sulle decisioni cliniche.")
4
GUIDA ECOGRAFICA/TC

5
ADEGUATO STRUMENTARIO
Da destra a sinistra: Cannula guida da 17 gauge Ago sottile da 22 gauge per citologia Pistola automatica con ago da 18 gauge per prelievo bioptico

6
TECNICA COASSIALE

8
CONTROLLO QUALITA’ DEL CAMPIONE

9
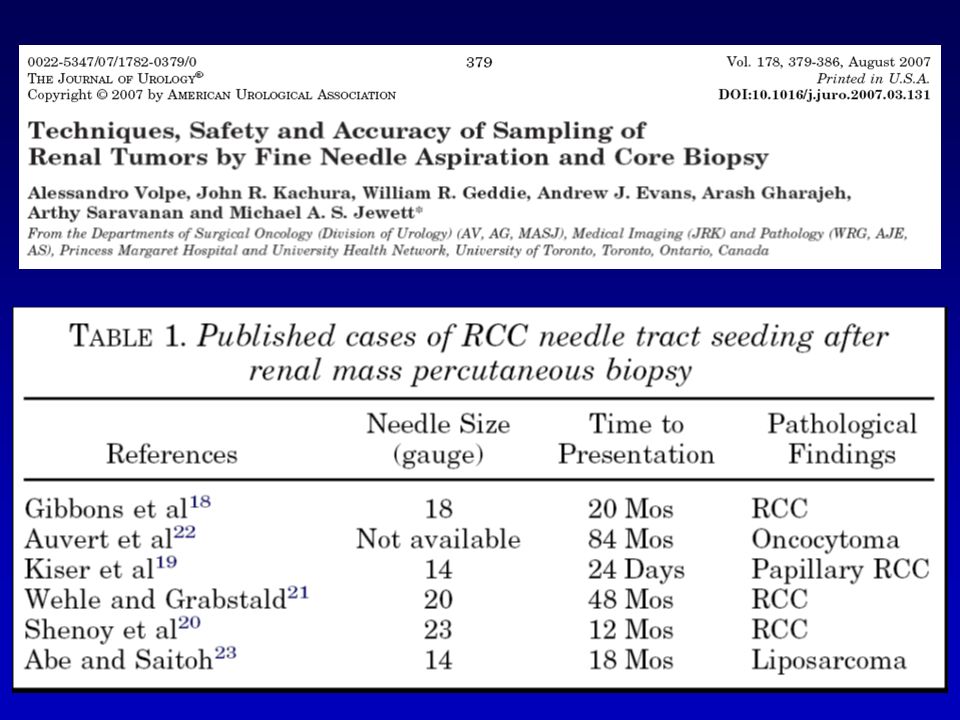
COMPLICANZE Autore No. Diametro ago Sanguinamento Neuzillet, 2004 88
Vasudevan, 2006 100 16 G 1 (1%) Somani, 2007 70 16-18 G 1 (1.4%) Maturen, 2007 152 2 (1.3%) Lebret, 2007 119 Volpe, 2008 Veltri, 2010 150 18-22 G 1 (0.7%)
 Somani, G. 1 (1.4%) Maturen, (1.3%) Lebret, Volpe, Veltri, G. 1 (0.7%)")
11
EFFICACIA DIAGNOSTICA
Autore No. Biopsie diagnostiche Biopsie benigne Wood, 1999 100 94% 32% Neuzillet, 2004 88 91% 16% Lebret, 2007 119 79% 20% Somani, 2007 70 87% 24% Maturen, 2007 152 96% 40% Volpe, 2008 84% 21% Wang, 2009 110 35% Veltri, 2010 150 93% 25%

12
325 risposte analizzabili
139 (43%) urologi non utilizzano mai le biopsie renali 111 (34%) utilizzano sempre le biopsie per le masse renali 75 (23%) utilizzano le biopsie solo in casi selezionati
 urologi non utilizzano mai le biopsie renali. 111 (34%) utilizzano sempre le biopsie per le masse renali. 75 (23%) utilizzano le biopsie solo in casi selezionati.")
13
INDAGINI RADIOLOGICHE
Accuratezza elevata ma non ottimale per la diagnosi di malignità Scarsa capacità nella identificazione di oncocitomi ed angiomiolipomi epitelioidi “fat free” A careful evaluation of outside imaging needs to be done. A surgeon should not operate on a renal mass without a noncontrast CT image to exclude the possibility of detecting macroscopic fat indicative of angiomyolipoma [16]. At our centre, we use ‘renal protocol’ CT imaging, which consists of three imaging sequences including precontrast, corticomedullary phase, and late nephrogenic excretory phase. A high degree of diagnostic accuracy in diagnosing renal cortical tumours is achieved with this technique (100% specificity, 95% sensitivity) [17]. The degree to which a renal mass enhances is dependent on the CT scanner being used. For a single-detector scanner 10 HU was considered suspicious for a renal cortical tumour but with more modern multidetector scanners, ‘pseudo enhancement’ of renal cysts secondary to volume averaging and beam hardening effects, particularly in smaller lesions, could lead to operation for a benign cyst. Enhancement of 10–20 HU in this setting may lead the radiologist to ask for further imaging, in which case I rely on renal ultrasound (US) with Doppler imaging to assess for vascular flow within the mass. US, as a complementary study, can also more fully characterize cystic lesions, and serves as an effective template for intraoperative US, which can be highly effective in locating small subcortical renal tumours. None of the current imaging methods can determine if a solid renal mass is benign or malignant. Usually at a second office visit after the completion of the medical and imaging evaluations, a frank discussion with the patient and their family ensues. This discussion reviews the diagnostic possibilities of the renal mass (benign, indolent cancer, more potentially aggressive conventional clear cell carcinoma), addresses the likelihood of executing a PN, estimates postoperative renal functional status, carefully reviews the major potential complications related to PN (bleeding, infection, urinary fistula and the need for a prolonged urinary drain) and discusses the likelihood of conversion to RN if, for technical reasons, a PN can not be executed. A discussion is also had concerning the likelihood of ipsilateral ( < 5%) or contralateral ( < 5%) tumour recurrence (new tumour formation) in a patient’s lifetime. In the face of a small renal mass, if medical comorbidities seem great, renal functional reserve minimal, and or the patient is elderly, the rationale for active surveillance can also be readily expressed during this consultation
 [17]. The degree to which a renal mass enhances is dependent on the CT scanner being used. For a single-detector scanner 10 HU was considered suspicious for a renal cortical tumour but with more modern multidetector scanners, ‘pseudo enhancement’ of renal cysts secondary to volume averaging and beam hardening effects, particularly in smaller lesions, could lead to operation for a benign cyst. Enhancement of 10–20 HU in this setting may lead the radiologist to ask for further imaging, in which case I rely on renal ultrasound (US) with Doppler imaging to assess for vascular flow within the mass. US, as a complementary study, can also more fully characterize cystic lesions, and serves as. an effective template for intraoperative US, which can be highly effective in locating small subcortical renal tumours. None of the current imaging methods can determine if a solid renal mass is benign or malignant. Usually at a second office visit after the completion of the medical and imaging evaluations, a frank discussion with the patient and their family ensues. This discussion reviews the diagnostic possibilities of the renal mass (benign, indolent cancer, more potentially aggressive conventional clear cell carcinoma), addresses the likelihood of executing a PN, estimates postoperative renal functional status, carefully reviews the major potential complications related to PN (bleeding, infection, urinary fistula and the need for a prolonged urinary drain) and. discusses the likelihood of conversion to RN if, for technical reasons, a PN can not be executed. A discussion is also had concerning the likelihood of ipsilateral ( < 5%) or contralateral ( < 5%) tumour recurrence (new tumour formation) in a patient’s lifetime. In the face. of a small renal mass, if medical comorbidities seem great, renal functional reserve minimal, and or the patient is elderly, the rationale for active surveillance can also be readily. expressed during this consultation.")
14
Renal oncocytoma and chromophobe RCC showed no significant difference in
size or any of 16 qualitative imaging features (p = –1.0, reader 1; p = –1.0, reader 2). Microscopic fat, hemorrhage, cysts, infiltrative margins, perinephric fat invasion, renal vein invasion, enhancement homogeneity, and hypervascularity were each observed in less than 20% of cases by both readers. A central scar and segmental enhancement inversion (a recently described finding in which early contrast-enhanced images show relatively more enhanced and less enhanced intralesional components with inversion of their relative enhancement on later images) were observed by both readers in at least 10% of cases of both renal oncocytoma and of chromophobe RCC with no significant difference between the two entities (p = –0.2960). CONCLUSION. We have presented the largest series to date of the MRI features of both renal oncocytoma and chromophobe RCC. These related entities exhibited similar findings, and no MRI features were reliable in distinguishing between them.
. Microscopic fat, hemorrhage, cysts, infiltrative margins, perinephric fat invasion, renal vein. invasion, enhancement homogeneity, and hypervascularity were each observed in less than 20% of cases by both readers. A central scar and segmental enhancement inversion (a recently described. finding in which early contrast-enhanced images show relatively more enhanced and less. enhanced intralesional components with inversion of their relative enhancement on later images) were observed by both readers in at least 10% of cases of both renal oncocytoma and of chromophobe. RCC with no significant difference between the two entities (p = –0.2960). CONCLUSION. We have presented the largest series to date of the MRI features of both. renal oncocytoma and chromophobe RCC. These related entities exhibited similar findings, and no MRI features were reliable in distinguishing between them.")
15
AJR 2010 Renal oncocytoma and chromophobe RCC showed no significant difference in size or any of 16 qualitative imaging features (p = –1.0, reader 1; p = –1.0, reader 2). Microscopic fat, hemorrhage, cysts, infiltrative margins, perinephric fat invasion, renal vein invasion, enhancement homogeneity, and hypervascularity were each observed in less than 20% of cases by both readers. A central scar and segmental enhancement inversion (a recently described finding in which early contrast-enhanced images show relatively more enhanced and less enhanced intralesional components with inversion of their relative enhancement on later images) were observed by both readers in at least 10% of cases of both renal oncocytoma and of chromophobe RCC with no significant difference between the two entities (p = –0.2960). CONCLUSION. We have presented the largest series to date of the MRI features of both renal oncocytoma and chromophobe RCC. These related entities exhibited similar findings, and no MRI features were reliable in distinguishing between them.
. Microscopic fat, hemorrhage, cysts, infiltrative margins, perinephric fat invasion, renal vein. invasion, enhancement homogeneity, and hypervascularity were each observed in less than 20% of cases by both readers. A central scar and segmental enhancement inversion (a recently described. finding in which early contrast-enhanced images show relatively more enhanced and less. enhanced intralesional components with inversion of their relative enhancement on later images) were observed by both readers in at least 10% of cases of both renal oncocytoma and of chromophobe. RCC with no significant difference between the two entities (p = –0.2960). CONCLUSION. We have presented the largest series to date of the MRI features of both. renal oncocytoma and chromophobe RCC. These related entities exhibited similar findings, and no MRI features were reliable in distinguishing between them.")
16
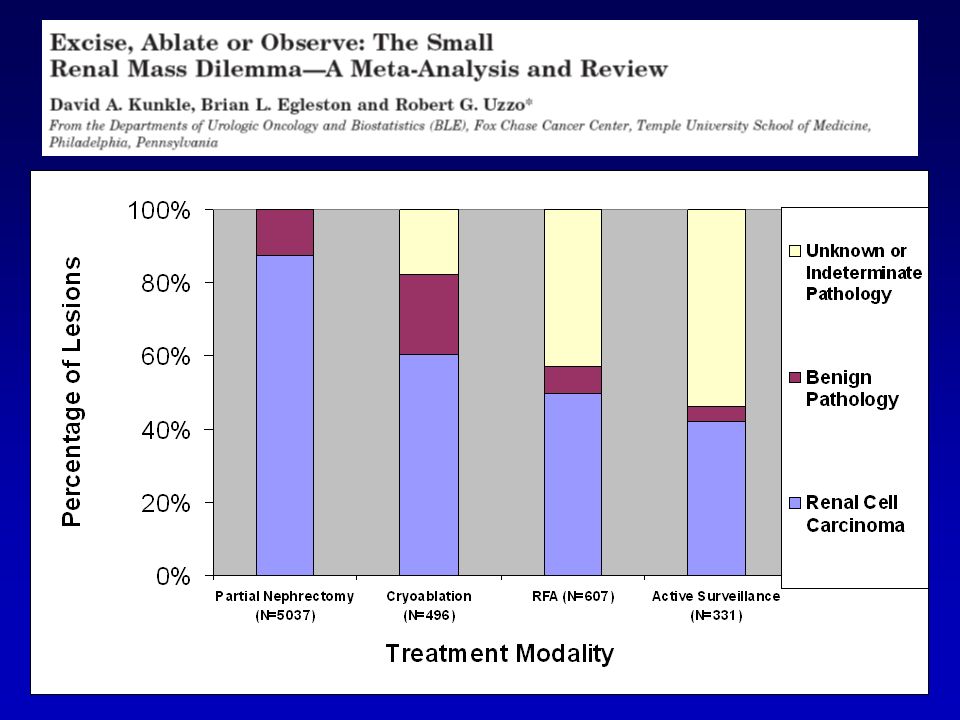
PICCOLE MASSE RENALI IMAGING ACCURATO, MA… Autore No.
Diametro medio (cm) Istologia benigna Gill, 2007 771 2.7 215 (28%) Moinzadeh, 2007 100 3.1 32 (32%) Link, 2005 217 2.6 73 (34%) Venkatesh, 2006 123 37 (31%) Bollens, 2007 39 2.3 17 (44%)
 Istologia benigna. Gill, (28%) Moinzadeh, (32%) Link, (34%) Venkatesh, (31%) Bollens, (44%)")
17
BIOPSIA PICCOLE MASSE RENALI
QUALE RUOLO? Riduzione del numero di chirurgie non necessarie per patologia benigna Supporto nella scelta terapeutica in pazienti con PMR candidati a trattamento conservativo Migliore definizione dei risultati oncologici delle terapie ablative mini-invasive Supporto nella scelta della terapia più adeguata per pazienti con RCC metastatico

18
INDAGINI RADIOLOGICHE
Nessuna significativa capacità di differenziazione di istotipo tumorale ed aggressività della neoplasia A careful evaluation of outside imaging needs to be done. A surgeon should not operate on a renal mass without a noncontrast CT image to exclude the possibility of detecting macroscopic fat indicative of angiomyolipoma [16]. At our centre, we use ‘renal protocol’ CT imaging, which consists of three imaging sequences including precontrast, corticomedullary phase, and late nephrogenic excretory phase. A high degree of diagnostic accuracy in diagnosing renal cortical tumours is achieved with this technique (100% specificity, 95% sensitivity) [17]. The degree to which a renal mass enhances is dependent on the CT scanner being used. For a single-detector scanner 10 HU was considered suspicious for a renal cortical tumour but with more modern multidetector scanners, ‘pseudo enhancement’ of renal cysts secondary to volume averaging and beam hardening effects, particularly in smaller lesions, could lead to operation for a benign cyst. Enhancement of 10–20 HU in this setting may lead the radiologist to ask for further imaging, in which case I rely on renal ultrasound (US) with Doppler imaging to assess for vascular flow within the mass. US, as a complementary study, can also more fully characterize cystic lesions, and serves as an effective template for intraoperative US, which can be highly effective in locating small subcortical renal tumours. None of the current imaging methods can determine if a solid renal mass is benign or malignant. Usually at a second office visit after the completion of the medical and imaging evaluations, a frank discussion with the patient and their family ensues. This discussion reviews the diagnostic possibilities of the renal mass (benign, indolent cancer, more potentially aggressive conventional clear cell carcinoma), addresses the likelihood of executing a PN, estimates postoperative renal functional status, carefully reviews the major potential complications related to PN (bleeding, infection, urinary fistula and the need for a prolonged urinary drain) and discusses the likelihood of conversion to RN if, for technical reasons, a PN can not be executed. A discussion is also had concerning the likelihood of ipsilateral ( < 5%) or contralateral ( < 5%) tumour recurrence (new tumour formation) in a patient’s lifetime. In the face of a small renal mass, if medical comorbidities seem great, renal functional reserve minimal, and or the patient is elderly, the rationale for active surveillance can also be readily expressed during this consultation
 [17]. The degree to which a renal mass enhances is dependent on the CT scanner being used. For a single-detector scanner 10 HU was considered suspicious for a renal cortical tumour but with more modern multidetector scanners, ‘pseudo enhancement’ of renal cysts secondary to volume averaging and beam hardening effects, particularly in smaller lesions, could lead to operation for a benign cyst. Enhancement of 10–20 HU in this setting may lead the radiologist to ask for further imaging, in which case I rely on renal ultrasound (US) with Doppler imaging to assess for vascular flow within the mass. US, as a complementary study, can also more fully characterize cystic lesions, and serves as. an effective template for intraoperative US, which can be highly effective in locating small subcortical renal tumours. None of the current imaging methods can determine if a solid renal mass is benign or malignant. Usually at a second office visit after the completion of the medical and imaging evaluations, a frank discussion with the patient and their family ensues. This discussion reviews the diagnostic possibilities of the renal mass (benign, indolent cancer, more potentially aggressive conventional clear cell carcinoma), addresses the likelihood of executing a PN, estimates postoperative renal functional status, carefully reviews the major potential complications related to PN (bleeding, infection, urinary fistula and the need for a prolonged urinary drain) and. discusses the likelihood of conversion to RN if, for technical reasons, a PN can not be executed. A discussion is also had concerning the likelihood of ipsilateral ( < 5%) or contralateral ( < 5%) tumour recurrence (new tumour formation) in a patient’s lifetime. In the face. of a small renal mass, if medical comorbidities seem great, renal functional reserve minimal, and or the patient is elderly, the rationale for active surveillance can also be readily. expressed during this consultation.")
19
RCC – MIGRAZIONE DI STADIO
STAGE I SIZE 4.1 cm 3.6 cm NATIONAL CANCER DATABASE ( ) Kane et al., Cancer 2007
 Kane et al., Cancer")
20
RCC – INCIDENZA ETÀ SPECIFICA 1998-2002
SEER database, 2005

21
SRMs are therefore frequently benign or low grade RCCs
SRMs are therefore frequently benign or low grade RCCs. Furthermore as we have seen most SRMs are diagnosed in elderly patients who are at higher risk of mortality for other causes, as brilliantly shown by this competing cause analysis that shows that about 40% of patients over the age of 70 with <4 cm tumors die of other causes by 5 years after surgical removal of the renal tumor

22
The presence of comorbidities has a significant impact on overall survival for patients with localized RCC. This study has shown that patients with a CCI >2 is significantly correlated with poorer OS

23
537 clinical T1 renal tumors
Lane and coll from CCF analyzed the predictors of OS in a cohort of 537 patients older than 75 yo with clinical T1 renal tumors and observed at multivariate analysis that only increasing age and CCI correlated with OS, while surgical treatment was not statistically associated with better outcomes as opposed to AS.

24
CARATTERISTICHE DELLA NEOPLASIA
Piccole masse renali Quale trattamento? CARATTERISTICHE DELLA NEOPLASIA DIMENSIONI SEDE TIPO DI CRESCITA PERCENTUALE DI SVILUPPO ESOFITICO POSSIBILE BENIGNITA’ DELLA LESIONE AGGRESSIVITA’ DELLA LESIONE INDICAZIONE Assoluta Relativa Elezione CARATTERISTICHE DEL PAZIENTE Età Comorbilità NSS OPEN NSS VLP Tecniche ablative VIGILE ATTESA

25
J Urol 2006

26
Crescita media 2.74 cc / anno - 0.1 cm / anno
We observed a slow growth rate of the renal tumors at 0.1 cm/year and no progression to metastatic disease Crescita media 2.74 cc / anno cm / anno

27
209 PMR incidentali (<4 cm) Diametro medio 2.1 cm (0.4-4)
Follow-up medio 28 mesi (1-60) Crescita media 0.13 cm/year 27
 Crescita media 0.13 cm/year. 27.")
28
crescita non può predire con accuratezza la malignità di una piccola
La sola velocità di crescita non può predire con accuratezza la malignità di una piccola massa renale in sorveglianza However, tumor growth kinetics can help in the management of SRMs, but we know that…

29
PICCOLE MASSE RENALI E’ necessaria una migliore definizione istologica mediante biopsia percutanea Malignità Grado tumorale

30
Diametro Basso grado (%) Alto grado (%) Totale < 4 cm 4-7 cm
7729 (86) 1250 (14) 8979 4-7 cm 5015 (79) 1361 (21) 6376 > 7 cm 2439 (70) 1024 (30) 3463 Totals 15,183 (81) 3635 (19) 18,818 Furthermore the probability of aggressive, high grade RCC, decreases with decreasing tumor size and the vast majority of SRMs <4cm are actually low grade, relatively indolent cancers
 1250 (14) cm (79) 1361 (21) > 7 cm (70) 1024 (30) Totals. 15,183 (81) 3635 (19) 18,818. Furthermore the probability of aggressive, high grade RCC, decreases with decreasing tumor size and the vast majority of SRMs <4cm are actually low grade, relatively indolent cancers.")
31
BIOPSIA PICCOLE MASSE RENALI
QUALE RUOLO? Riduzione del numero di chirurgie non necessarie per patologia benigna Supporto nella scelta terapeutica in pazienti con PMR candidati a trattamento conservativo Migliore definizione dei risultati oncologici delle terapie ablative mini-invasive Supporto nella scelta della terapia più adeguata per pazienti con RCC metastatico

32
Diametro (cm) N Grado III-IV pT3a M+ 0-3.0 129 4.7% 10.9% 2.4% 3.1-4.0
98 25.5% 35.7% 8.4% This is particularly true for SRMs between 3-4 cm in size that have a higher risk of harbouring high grade disease and therefore higher risk of local and metastatic progression.

37
BIOPSIA PICCOLE MASSE RENALI
QUALE RUOLO? Riduzione del numero di chirurgie non necessarie per patologia benigna Supporto nella scelta terapeutica in pazienti con PMR candidati a trattamento conservativo Migliore definizione dei risultati oncologici delle terapie ablative mini-invasive Supporto nella scelta della terapia più adeguata per pazienti con RCC metastatico

38
Quale ruolo della biopsia?
RCC METASTATICO Quale ruolo della biopsia? Diagnosi di malattia metastatica renale in pazienti con una nota neoplasia primitiva extrarenale Conferma del tumore primitivo renale in presenza di sospetti tumori primitivi in altri organi Conferma istologica di un tumore primitivo renale in presenza di malattia metastatica disseminata o di una massa retroperitoneale non resecabile chirurgicamente

39
BIOPSIA PICCOLE MASSE RENALI
QUALE RUOLO? Riduzione del numero di chirurgie non necessarie per patologia benigna Supporto nella scelta terapeutica in pazienti con PMR candidati a trattamento conservativo Migliore definizione dei risultati oncologici delle terapie ablative mini-invasive Supporto nella scelta della terapia più adeguata per pazienti con RCC metastatico

40
We identified 166 patients who underwent percutaneous biopsy of the
primary tumor before cytoreductive nephrectomy between 1991 and 2007, and had data available for review. Median pathological tumor size was 9.1 cm (range 3 to 32). Median time from biopsy to surgery was 46 days (range 6 to 717). Of 104 patients in whom biopsy was assigned a Fuhrman nuclear grade 33 (31.7%) had the same grade in the nephrectomy specimen, including 74 of 109 (67.9%) when considering only high or low grade. Grade change by more than 2 points was seen in 18 of 104 patients (17.3%). Sarcomatoid features were present in 34 of 166 nephrectomy specimens (20.5%) but only 4 (11.8%) were identified preoperatively.
. Median time from biopsy to surgery was 46 days (range 6 to 717). Of 104. patients in whom biopsy was assigned a Fuhrman nuclear grade 33 (31.7%) had. the same grade in the nephrectomy specimen, including 74 of 109 (67.9%) when. considering only high or low grade. Grade change by more than 2 points was seen. in 18 of 104 patients (17.3%). Sarcomatoid features were present in 34 of 166. nephrectomy specimens (20.5%) but only 4 (11.8%) were identified preoperatively.")
41
RCC METASTATICO

42
RCC METASTATICO Sorafenib: first targeted therapy licensed in the US.5 Sunitinib followed, then both licensed in the EU High-dose IL-2 FDA approved Cytotoxic chemotherapy experiments performed IFN-a shows improved survival versus hormonal therapy Temsirolimus and bevacizumab + IFN licensed 1980s / 1940s IFN-a and high-dose IL-2 used for treatment of RCC in early 1980s Everolimus licensed in the US and EU TARGET: first evidence of PFS benefit with targeted therapy Pazopanib licensed in the US

43
Patients with ARCC including clear cell and other types such as papillary and chromophobe histologies received either IFN (3 million units [MU] subcutaneously three times weekly, escalating to 18 MU) or temsirolimus (25 mg intravenously weekly). Results Approximately 80%of patients had clear cell and 20% of patients had other histologies, the majority of which werepapillary. Patients with clear cell and other RCC histologies, treated with temsirolimus, demonstrated comparable median overall and progression-free survival. In contrast, patients with other RCC histologies, treated with IFN, demonstrated shorter median overall and progression-free survival than patients with clear cell RCC. Hazard ratios for death for treatment with temsirolimus versus IFN were less than 1 for patients regardless of tumor histology. For patients treated with temsirolimus, 59% with clear cell and 68% with other RCC histologies experienced tumor reductions. For patients treatedwith IFN, 35%with clear cell and 14%with otherRCC histologies had tumor reductions. However, temsirolimus did not appear to improve the objective response rate compared to IFN. Temsirolimus resulted in a superior clinical benefit rate compared with IFN, regardless of tumor histology. Conclusion Temsirolimus appears to be efficacious in patients with clear cell and non-clear cell histologies and can, therefore, be used for the treatment of all types of RCC.
 or temsirolimus (25 mg intravenously weekly). Results Approximately 80%of patients had clear cell and 20% of patients had other histologies, the majority of which werepapillary. Patients with clear cell and other RCC histologies, treated with temsirolimus, demonstrated comparable median. overall and progression-free survival. In contrast, patients. with other RCC histologies, treated with IFN, demonstrated. shorter median overall and progression-free survival than. patients with clear cell RCC. Hazard ratios for death for. treatment with temsirolimus versus IFN were less than 1 for. patients regardless of tumor histology. For patients treated. with temsirolimus, 59% with clear cell and 68% with other. RCC histologies experienced tumor reductions. For patients. treatedwith IFN, 35%with clear cell and 14%with otherRCC. histologies had tumor reductions. However, temsirolimus did. not appear to improve the objective response rate compared to. IFN. Temsirolimus resulted in a superior clinical benefit rate. compared with IFN, regardless of tumor histology. Conclusion. Temsirolimus appears to be efficacious in patients with. clear cell and non-clear cell histologies and can, therefore, be. used for the treatment of all types of RCC.")
44
Exploratory subgroup analyses
Phase 3 global advanced renal cell carcinoma (ARCC) trial Patients with ARCC including clear cell and other types such as papillary and chromophobe histologies received either IFN (3 million units [MU] subcutaneously three times weekly, escalating to 18 MU) or temsirolimus (25 mg intravenously weekly). Results Approximately 80%of patients had clear cell and 20% of patients had other histologies, the majority of which werepapillary. Patients with clear cell and other RCC histologies, treated with temsirolimus, demonstrated comparable median overall and progression-free survival. In contrast, patients with other RCC histologies, treated with IFN, demonstrated shorter median overall and progression-free survival than patients with clear cell RCC. Hazard ratios for death for treatment with temsirolimus versus IFN were less than 1 for patients regardless of tumor histology. For patients treated with temsirolimus, 59% with clear cell and 68% with other RCC histologies experienced tumor reductions. For patients treatedwith IFN, 35%with clear cell and 14%with otherRCC histologies had tumor reductions. However, temsirolimus did not appear to improve the objective response rate compared to IFN. Temsirolimus resulted in a superior clinical benefit rate compared with IFN, regardless of tumor histology. Conclusion Temsirolimus appears to be efficacious in patients with clear cell and non-clear cell histologies and can, therefore, be used for the treatment of all types of RCC.
 trial. Patients with ARCC. including clear cell and other types such as papillary and. chromophobe histologies received either IFN (3 million units. [MU] subcutaneously three times weekly, escalating to. 18 MU) or temsirolimus (25 mg intravenously weekly). Results Approximately 80%of patients had clear cell and 20% of patients had other histologies, the majority of which werepapillary. Patients with clear cell and other RCC histologies, treated with temsirolimus, demonstrated comparable median. overall and progression-free survival. In contrast, patients. with other RCC histologies, treated with IFN, demonstrated. shorter median overall and progression-free survival than. patients with clear cell RCC. Hazard ratios for death for. treatment with temsirolimus versus IFN were less than 1 for. patients regardless of tumor histology. For patients treated. with temsirolimus, 59% with clear cell and 68% with other. RCC histologies experienced tumor reductions. For patients. treatedwith IFN, 35%with clear cell and 14%with otherRCC. histologies had tumor reductions. However, temsirolimus did. not appear to improve the objective response rate compared to. IFN. Temsirolimus resulted in a superior clinical benefit rate. compared with IFN, regardless of tumor histology. Conclusion. Temsirolimus appears to be efficacious in patients with. clear cell and non-clear cell histologies and can, therefore, be. used for the treatment of all types of RCC.")
45
Patients with ARCC including clear cell and other types such as papillary and chromophobe histologies received either IFN (3 million units [MU] subcutaneously three times weekly, escalating to 18 MU) or temsirolimus (25 mg intravenously weekly). Results Approximately 80%of patients had clear cell and 20% of patients had other histologies, the majority of which werepapillary. Patients with clear cell and other RCC histologies, treated with temsirolimus, demonstrated comparable median overall and progression-free survival. In contrast, patients with other RCC histologies, treated with IFN, demonstrated shorter median overall and progression-free survival than patients with clear cell RCC. Hazard ratios for death for treatment with temsirolimus versus IFN were less than 1 for patients regardless of tumor histology. For patients treated with temsirolimus, 59% with clear cell and 68% with other RCC histologies experienced tumor reductions. For patients treatedwith IFN, 35%with clear cell and 14%with otherRCC histologies had tumor reductions. However, temsirolimus did not appear to improve the objective response rate compared to IFN. Temsirolimus resulted in a superior clinical benefit rate compared with IFN, regardless of tumor histology. Conclusion Temsirolimus appears to be efficacious in patients with clear cell and non-clear cell histologies and can, therefore, be used for the treatment of all types of RCC.
 or temsirolimus (25 mg intravenously weekly). Results Approximately 80%of patients had clear cell and 20% of patients had other histologies, the majority of which werepapillary. Patients with clear cell and other RCC histologies, treated with temsirolimus, demonstrated comparable median. overall and progression-free survival. In contrast, patients. with other RCC histologies, treated with IFN, demonstrated. shorter median overall and progression-free survival than. patients with clear cell RCC. Hazard ratios for death for. treatment with temsirolimus versus IFN were less than 1 for. patients regardless of tumor histology. For patients treated. with temsirolimus, 59% with clear cell and 68% with other. RCC histologies experienced tumor reductions. For patients. treatedwith IFN, 35%with clear cell and 14%with otherRCC. histologies had tumor reductions. However, temsirolimus did. not appear to improve the objective response rate compared to. IFN. Temsirolimus resulted in a superior clinical benefit rate. compared with IFN, regardless of tumor histology. Conclusion. Temsirolimus appears to be efficacious in patients with. clear cell and non-clear cell histologies and can, therefore, be. used for the treatment of all types of RCC.")
46
BIOPSIA PICCOLE MASSE RENALI
QUALE RUOLO? Riduzione del numero di chirurgie non necessarie per patologia benigna Supporto nella scelta terapeutica in pazienti con PMR candidati a trattamento conservativo Migliore definizione dei risultati oncologici delle terapie ablative mini-invasive Supporto nella scelta della terapia più adeguata per pazienti con RCC metastatico

47
Impatto sulla terapia (%)
IMPATTO CLINICO No. Diametro medio (cm) Impatto sulla terapia (%) Wood, 1999 79 3.3 44% Neuzillet, 2004 88 2.8 48% Rybilowski, 2008 66 <4 6% Thullier, 2008 53 2.5 25% Volpe, 2008 100 2.4 43% Shannon, 2008 222 2.9 34%
 Impatto sulla terapia (%) Wood, % Neuzillet, % Rybilowski, <4. 6% Thullier, % Volpe, % Shannon, %")
48
J Urol 2008 We know today that renal biopsies are safe and can provide an accurate diagnosis in >90% of cases in centres with experience. In such centres the information provided have a significant impact on treatment decision making and allow a potentially better and safer selection of patients who are good candidates for an AS approach.

49
BIOPSIA DELLA MASSE RENALI
INCERTEZZE STORICHE SICUREZZA Rischio di sanguinamento Rischio di seeding TECNICA Rischio di prelievo non diagnostico Errori di campionamento (eterogeneità intratumorale) EFFICACIA Accuratezza diagnostica Impatto sulle decisioni cliniche x x x
 EFFICACIA. Accuratezza diagnostica. Impatto sulle decisioni cliniche. x. x. x.")
50
BIOPSIA DELLA MASSE RENALI ATTUALI PUNTI DI DISCUSSIONE
Utilità dell’agoaspirato Definizione del miglior schema bioptico Eterogeneità intratumorale Istotipo (tumori ibridi cromofobo – oncocitoma) Grado
 Grado.")
51
BIOPSIA DELLA MASSE RENALI PROSPETTIVE DI RICERCA
Variabilità interosservatore nella valutazione istologica/citologica Accuratezza del grading tumorale su biopsia Diagnosi differenziale tra oncocitoma e carcinoma cromofobo

52
CONCLUSIONI Le attuali indagini radiologiche non hanno un’accuratezza ottimale e forniscono scarse indicazioni per la selezione dei pazienti per un trattamento non chirurgico La biopsia percutanea è sicura e prelievi di adeguata qualità sono in grado di fornire una diagnosi istologica accurata nella maggioranza dei casi

53
CONCLUSIONI La biopsia percutanea ha oggi indicazioni crescenti nella diagnostica delle masse renali per stabilirne malignità, istotipo e grading Deve essere sempre considerata nei casi con imaging dubbio, nei pazienti con piccole masse renali candidati a trattamento non chirurgico e nei pazienti con tumore renale metastatico non candidati a nefrectomia citoriduttiva

54
CONCLUSIONI Ulteriori studi sono necessari per ottimizzare il tasso diagnostico e l’accuratezza della biopsia nella determinazione di istotipo e grado tumorale L’applicazione di citogenetica, biologia molecolare, microarrays rappresentano il presupposto per un ulteriore aumento dell’utilità clinica della biopsia delle masse renali

Presentazioni simili






>")







>")






