Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

2
La biopsia nel carcinoma renale
Department of Emergency and Organ Transplantation Urology, Andrology and Kidney Transplantation Unit University of Bari – Italy La biopsia nel carcinoma renale Michele Battaglia

3
La rimozione chirurgica è il «gold standard» della terapia del tumore del rene
Controversie 2013 nella chirurgia dell’RCC La biopsia renale. Quando e come farla? Il problema della piccole masse renali: cosa fare ? Sono anch’esse «big killer»? Novità in tema di nefrectomia parziale ed i margini chirurgici positivi. Qual è il vero «problema»? Il diabete e l’RCC La nefrectomia radicale in ogni caso? Sorveglianza attiva e trattamenti mininvasivi Novità in tema di terapia neoadiuvante Terapia adiuvante

4
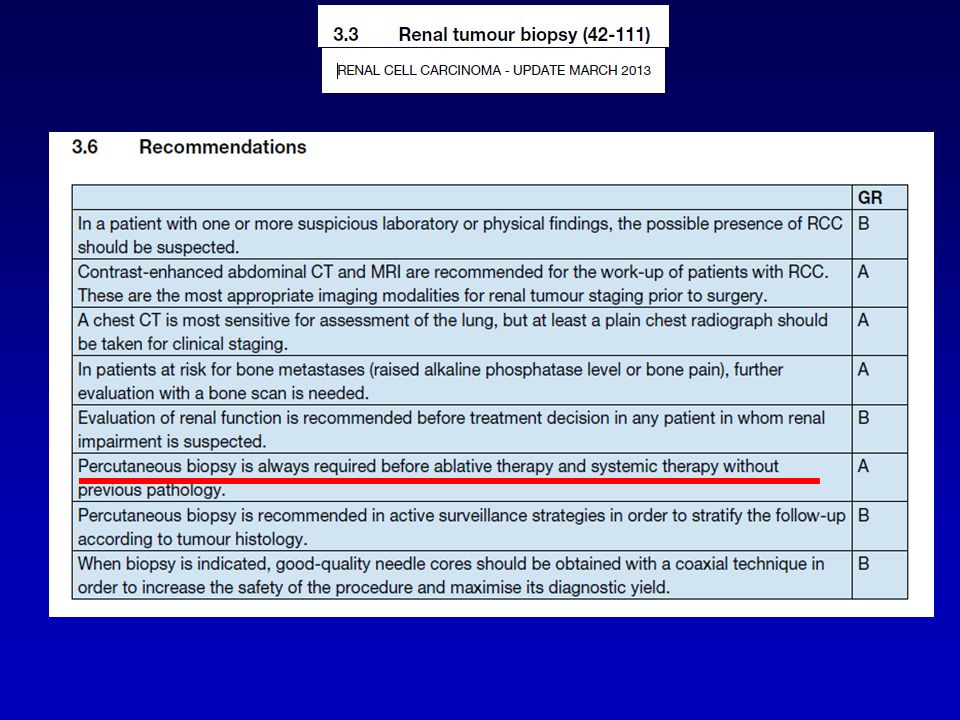
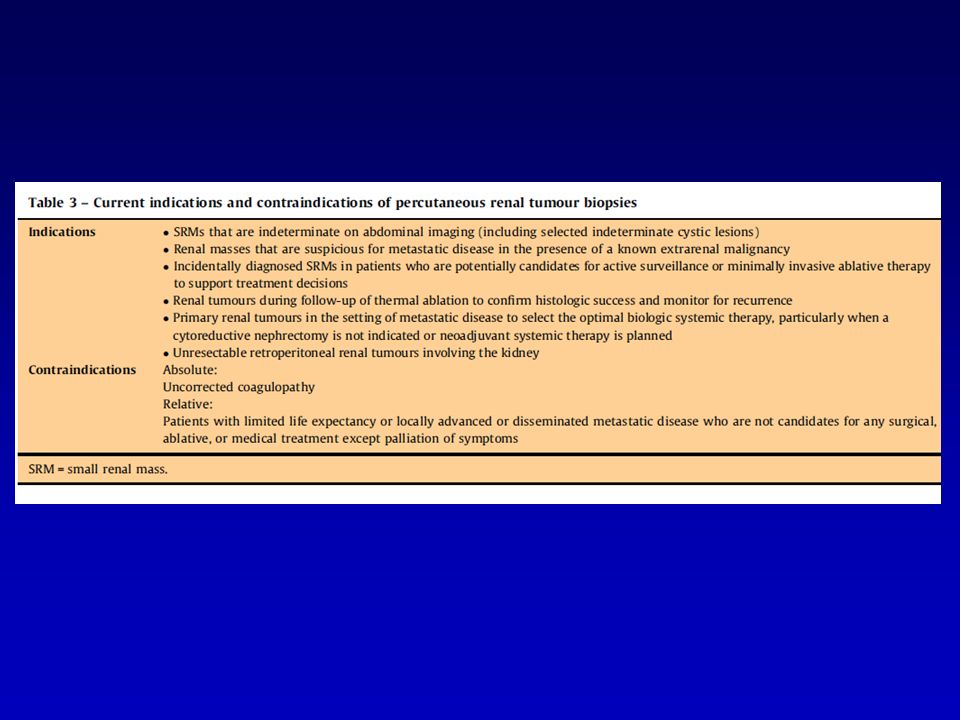
RUOLO TRADIZIONALE DELLA BIOPSIA DELLE MASSE RENALI
Diagnosi di malattia metastatica in pazienti con una nota neoplasia primitiva extrarenale Diagnosi di ascesso renale o linfoma Diagnosi di patologie di competenza “nefrologica” Conferma istologica di un tumore primitivo renale in presenza di malattia metastatica disseminata o di una massa retroperitoneale non resecabile chirurgicamente [6] Herts BR, Baker ME. The current role of percutaneous biopsy in the evaluation of renal masses. Semin Urol Oncol 1995;13: 254–61. Herts BR, Semin Urol Oncol 1995;13:254-61

5
Quando si fa

7
Quando NON si fa Percutaneous sampling of renal masses can be performed under local anesthesia in the majority of cases (42-51) (LE: 3). Depending on the tumour’s location, its echogenic features, and the patient’s physical characteristics, biopsies can be performed with either ultrasound or CT guidance, with a similar diagnostic yield (47,50) (LE: 2b).
 (LE: 3). Depending on the tumour’s location, its echogenic features, and the patient’s physical. characteristics, biopsies can be performed with either ultrasound or CT guidance, with a similar diagnostic. yield (47,50) (LE: 2b).")
8
….NEI GIOVANI? …quasi mai indicata per il rischio della trasformazione in tumore maligno «over time»!

9
COME SI GIUDICA LA BIOPSIA?
-Fallita: quantità di tessuto insufficiente/inadeguato -Indeterminata: il patologo non riesce a fare diagnosi -Inaccurata: falso positivo/falso negativo Lane BR, J Urol 2008;179:20-7 Most authors currently define a biopsy as failed when it does not provide sufficient or adequate tissue for diagnosis, indeterminate when the pathologist cannot make a definitive diagnosis using available tissues, and inaccurate (false negative or false positive) when there is a discrepancy between diagnosis on the biopsy and on the final pathologic specimen [20]. Lane BR, Samplaski MK, Herts BR, Zhou M, Novick AC, Campbell SC. Renal mass biopsy—a renaissance? J Urol 2008;179:20–7
 when there is a discrepancy between diagnosis on. the biopsy and on the final pathologic specimen [20]. Lane BR, Samplaski MK, Herts BR, Zhou M, Novick AC, Campbell SC. Renal mass biopsy—a renaissance J Urol 2008;179:20–7.")
10
ALMENO 2 DI BUONA QUALITA’ (Neuzillet Y, J Urol 2004;171:1802-5)
QUANTI «CORES?» ALMENO 2 DI BUONA QUALITA’ (Neuzillet Y, J Urol 2004;171:1802-5) Ago 18 gauge 1 cm lungo Although no clinical practice guidelines are available, there is agreement that at least two good-quality cores should be obtained in each case [8] [8] Neuzillet Y, Lechevallier E, Andre M, Daniel L, Coulange C. Accuracy and clinical role of fine needle percutaneous biopsy with computerized tomography guidance of small (less than 4.0 cm) renal masses. J Urol 2004;171:1802–5.
 Ago 18 gauge. 1 cm lungo. Although no clinical practice guidelines are available, there is. agreement that at least two good-quality cores should be. obtained in each case [8] [8] Neuzillet Y, Lechevallier E, Andre M, Daniel L, Coulange C. Accuracy. and clinical role of fine needle percutaneous biopsy with computerized. tomography guidance of small (less than 4.0 cm) renal. masses. J Urol 2004;171:1802–5.")
11
AIMS ACHIEVED BY BIOPSY OF RENAL MASSES
HISTOLOGY OF RENAL TUMORS CONFIRM TREATMENT SUCCESS AFTER THERMAL ABLATION SELECT THE MOST SUITABLE TARGETED PHARMACOLOGIC TH. IN METASTATIC DISEASE GROWING INTEREST Immunohistochemical, molecular and genetic assessments Tumor biologic and clinical behaviour Although the indications for biopsy are still generally dictated by local practice patterns and investigative interest, in the past few years, percutaneous biopsies have been increasingly used to clarify the histology of renal tumours to aid with treatment decisions for SRMs, confirm treatment success after thermal ablation of renal lesions, and select the most suitable targeted pharmacologic therapy in the setting of metastatic disease. Furthermore, there has been growing interest in the use of immunohistochemical, molecular, and genetic assessments that can potentially improve our ability to determine renal tumour biologic and clinical behaviour on percutaneous biopsies Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) criteria [7 [7] Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 2009;6:e Alessandro Volpe, Eur Urol 62 (2012)
 criteria [7. [7] Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for. reporting systematic reviews and meta-analyses of studies that. evaluate health care interventions: explanation and elaboration. PLoS Med 2009;6:e Alessandro Volpe, Eur Urol 62 (2012)")
12
BIOPSIA DELLA MASSE RENALI
INCERTEZZE STORICHE SICUREZZA Rischio di sanguinamento Rischio di seeding TECNICA Rischio di prelievo non diagnostico Errori di campionamento (eterogeneità intratumorale) EFFICACIA Accuratezza diagnostica Impatto sulle decisioni cliniche
 EFFICACIA. Accuratezza diagnostica. Impatto sulle decisioni cliniche.")
13
La biopsia delle masse renali non ha avuto una diffusione clinica perché ritenuta non attendibile e incapace di modificare la strategia terapeutica in una grande percentuale di casi (Riscontro di falsi negativi nel 18% dei casi) Questo risulta valido per una grande percentuale di urologi che ritiene sufficiente il dato strumentale di una massa renale con enhancement alla TC o RMN per programmare un intervento dal momento che l’80 % di queste lesioni è rappresentato da un RCC Risultati delle biopsie renali :studi antecedenti il 2001: Falsi negativi : 0-25% (spesso biopsie insufficienti o fallite piuttosto che falsi negativi) Falsi positivi: 0-5% ( prime esperienze di citoaspirato) Overall positive predictive value : 95.7% Overall negative predictive value :82% Sensibilità: 92.1% (range 70% to 100%) Specificità :89.7% (range 60% to 100%) Per confronto - standard imaging (TC): Sensibilità (maligno vs benigno) 60-90% Specificità (maligno vs benigno) 5-50%
 Falsi positivi: 0-5% ( prime esperienze di citoaspirato) Overall positive predictive value : 95.7% Overall negative predictive value :82% Sensibilità: 92.1% (range 70% to 100%) Specificità :89.7% (range 60% to 100%) Per confronto - standard imaging (TC): Sensibilità (maligno vs benigno) 60-90% Specificità (maligno vs benigno) 5-50%")
14
EFFICACIA DIAGNOSTICA
Autore No. Biopsie diagnostiche Biopsie benigne Wood, 1999 100 94% 32% Neuzillet, 2004 88 91% 16% Lebret, 2007 119 79% 20% Somani, 2007 70 87% 24% Maturen, 2007 152 96% 40% Volpe, 2008 84% 21% Wang, 2009 110 35% Veltri, 2010 150 93% 25% L’accuratezza diagnostica va dal 78% al 100%, mentre l’errore diagnostico per una biopsia ben eseguita è raro The diagnostic yield of renal tumour biopsies in the largest recent series ranges from 78% to 100%, and an erroneous diagnosis on adequate biopsy specimens is now rare [8–16]

15
Accuracy of renal tumor biopsy
[20] Lane BR, Samplaski MK, Herts BR, Zhou M, Novick AC, Campbell SC. Renal mass biopsy—a renaissance? J Urol 2008;179:20–7 Recent series - sensitivity: % - specificity: 100% - accuracy: 90% Volpe et al., J Urol 2007 Volpe A, Eur Urol 62 (2012) Lane BR, J Urol 2008;179:20-7
 Lane BR, J Urol 2008;179:20-7.")
16
110 Bx renali per SRM Diametro medio SRM: 2.7 cm 100 casi (90.9%): materiale diagnostico 10 casi (9.1%): materiale insuff. x diagnosi
: materiale insuff. x diagnosi.")
17
ACCURATEZZA DIAGNOSTICA E SIZE DEL TUMORE
-Correla significativamente con le dimensioni del tumore (Volpe A, J Urol 2008;180:2333-7) -Aumenta per 1cm in più delle dimensioni del tumore con OR 2,30 (p=0,002) (Leveridge MJ, Eur Urol 2011;60:578-84) Tumour size. A few authors assessed the influence of tumour dimension on the diagnostic success of percutaneous biopsy and showed that a larger tumour size significantly correlates with diagnostic yield [13,16]. Leveridge et al. analysed a series of 345 percutaneous biopsies and observed that the odds ratio (OR) for a diagnostic result was 2.30 (95% confidence interval [CI], 1.54–6.28) for each 1-cm increase in tumour size ( p = 0.002) [16]. Urologists should be aware of the higher risk of biopsy failure with decreasing tumour size and inform patients accordingly. [16] Leveridge MJ, Finelli A, Kachura JR, et al. Outcomes of small renal mass needle core biopsy, nondiagnostic percutaneous biopsy, and the role of repeat biopsy. Eur Urol 2011;60:578–84. [13] Volpe A, Mattar K, Finelli A, et al. Contemporary results of percutaneous biopsy of 100 small renal masses: a single center experience. J Urol 2008;180:2333–7. Informare il paziente
 -Aumenta per 1cm in più delle dimensioni del tumore. con OR 2,30 (p=0,002) (Leveridge MJ, Eur Urol 2011;60:578-84) Tumour size. A few authors assessed the influence of. tumour dimension on the diagnostic success of percutaneous. biopsy and showed that a larger tumour size significantly. correlates with diagnostic yield [13,16]. Leveridge et al. analysed a series of 345 percutaneous biopsies and observed. that the odds ratio (OR) for a diagnostic result was 2.30 (95% confidence interval [CI], 1.54–6.28) for each 1-cm increase in. tumour size ( p = 0.002) [16]. Urologists should be aware of. the higher risk of biopsy failure with decreasing tumour size. and inform patients accordingly. [16] Leveridge MJ, Finelli A, Kachura JR, et al. Outcomes of small renal. mass needle core biopsy, nondiagnostic percutaneous biopsy, and. the role of repeat biopsy. Eur Urol 2011;60:578–84. [13] Volpe A, Mattar K, Finelli A, et al. Contemporary results of percutaneous. biopsy of 100 small renal masses: a single center experience. J Urol 2008;180:2333–7. Informare il paziente.")
18
ACCURATEZZA DIAGNOSTICA E SEDE TUMORE
Poche informazioni in letteratura Sedi «problematiche»: Faccia anteriore Polo superiore Mediale Peri-ilari Endofitica Sedi «con maggiore accuratezza diagnostica»: Polo superiore vs medio vs inferiore (in analisi univariata solo) (Leveridge MJ, Eur Urol 2011;60:578-84) Tumour location and endophytic/exophytic pattern. Little information is available on the correlation between other tumour characteristics (anterior/posterior, longitudinal and rim location, endophytic/exophytic pattern, proximity to renal sinus and collecting system) and the diagnostic rate of percutaneous biopsies In general, biopsies of anteriorly located, upper-pole, medial, perihilar, and endophytic tumours are considered more challenging. Longitudinal location (upper vs mid vs lower pole) was found to be a significant predictor of diagnostic biopsy in univariable but not multivariable analysis [16]. [16] Leveridge MJ, Finelli A, Kachura JR, et al. Outcomes of small renal mass needle core biopsy, nondiagnostic percutaneous biopsy, and the role of repeat biopsy. Eur Urol 2011;60:578–84.
 (Leveridge MJ, Eur Urol 2011;60:578-84) Tumour location and endophytic/exophytic pattern. Little. information is available on the correlation between other. tumour characteristics (anterior/posterior, longitudinal and. rim location, endophytic/exophytic pattern, proximity to. renal sinus and collecting system) and the diagnostic rate of. percutaneous biopsies. In general, biopsies of anteriorly. located, upper-pole, medial, perihilar, and endophytic. tumours are considered more challenging. Longitudinal. location (upper vs mid vs lower pole) was found to be a. significant predictor of diagnostic biopsy in univariable but. not multivariable analysis [16]. [16] Leveridge MJ, Finelli A, Kachura JR, et al. Outcomes of small renal. mass needle core biopsy, nondiagnostic percutaneous biopsy, and. the role of repeat biopsy. Eur Urol 2011;60:578–84.")
19
ALTRI FATTORI INFLUENZANTI L’ACCURATEZZA DIAGNOSTICA
BMI non valutato (Volpe A, Eur Urol 2012 Imaging Personalizzazione (Leveridge MJ, Eur Urol 2011;60:578-84) Needle size 18 gauge (Breda A, BJU Int 2009;105:940-5) Qualità specimen Periferico > centrale per t.>4cm (Wunderlich H, J Urol 2005;174:44-6) Approccio multidisciplinare Urologo, radiologo e patologo = migliori risultati Needle size. There are indications that a larger needle size correlates with better diagnostic outcomes [20,31]. There is currently agreement that 18-gauge needles are ideal for renal tumour biopsies, allowing a safe procedure and sufficient tissue [32] Breda A, Treat EG, Haft-Candell L, et al. Comparison of accuracy of 14-, 18- and 20-G needles in ex-vivo renal mass biopsy: a prospective, blinded study. BJU Int 2009;105:940–5. Wunderlich et al. observed better diagnostic outcomes of peripheral compared to central biopsies for renal tumours >4 cm [21]. [21] Wunderlich H, HindermannW, Al Mustafa AM, Reichelt O, Junker K, Schubert J. The accuracy of 250 fine needle biopsies of renal tumors. J Urol 2005;174:44–6.
 Needle size 18 gauge (Breda A, BJU Int 2009;105:940-5) Qualità specimen Periferico > centrale per t.>4cm (Wunderlich H, J Urol 2005;174:44-6) Approccio multidisciplinare Urologo, radiologo e patologo = migliori risultati Needle size. There are indications that a larger needle. size correlates with better diagnostic outcomes [20,31]. There is currently agreement that 18-gauge needles are ideal. for renal tumour biopsies, allowing a safe procedure and. sufficient tissue. [32] Breda A, Treat EG, Haft-Candell L, et al. Comparison of accuracy of. 14-, 18- and 20-G needles in ex-vivo renal mass biopsy: a prospective, blinded study. BJU Int 2009;105:940–5. Wunderlich et al. observed better diagnostic outcomes of peripheral compared. to central biopsies for renal tumours >4 cm [21]. [21] Wunderlich H, HindermannW, Al Mustafa AM, Reichelt O, Junker. K, Schubert J. The accuracy of 250 fine needle biopsies of renal. tumors. J Urol 2005;174:44–6.")
20
Assessment of tumour grade on core biopsies is challenging
Assessment of tumour grade on core biopsies is challenging. The accuracy of Fuhrman grading on biopsies is poor (43-75%), but it can be improved using a simplified two-tier system (high-grade vs. low grade) (42-50,54,55,57-75) (LE: 2b).
, but it can be improved using a simplified two-tier system (high-grade vs. low grade) (42-50,54,55,57-75) (LE: 2b).")
21
Accuratezza diagnostica Biopsia vs nefrectomia
ISTOTIPO 86% - 98%* Grado di Fuhrman 63% - 76%* *Accuratezza diagnostica Biopsia vs nefrectomia Diagnostic accuracy for tumour subtyping on core biopsies compared to final nephrectomy is also high in recent series, ranging from 86% to 98% [8–11,13–16]. Fuhrman nuclear grading from biopsies can be determined in 76–94% of cases [8,10,21], with accuracy rates of 63–76% [8,10,11,13,16] (Table 2). [9] Shannon BA, Cohen RJ, de Bruto H, Davies RJ. The value of preoperative needle core biopsy for diagnosing benign lesions among small, incidentally detected renalmasses. J Urol 2008;180:1257–61, discussion 1261. Shannon BA, J Urol 2008;180:
. [9] Shannon BA, Cohen RJ, de Bruto H, Davies RJ. The value of preoperative. needle core biopsy for diagnosing benign lesions among. small, incidentally detected renalmasses. J Urol 2008;180:1257–61, discussion Shannon BA, J Urol 2008;180:")
22
Diagnostic yield for cystic renal masses
Core biopsies Diagnostic yield for cystic renal masses It is low It should not be recommended alone in these cases, unless areas with a solid pattern are present (Bosniak IV cysts) (LE: 2b). Combined FNA and core biopsies can provide complementary results, especially for complex cystic lesions (LE: 3). [27] Lang EK, Macchia RJ, Gayle B, et al. CT-guided biopsy of indeterminate renal cystic masses (Bosniak 3 and 2F): accuracy and impact on clinical management. Eur Radiol 2002;12:2518–24. [28] Harisinghani MG, Maher MM, Gervais DA, et al. Incidence of malignancy in complex cystic renal masses (Bosniak category III): should imaging-guided biopsy precede surgery? AJR Am J Roentgenol 2003;180:755–8. Lang EK, Eur Radiol 2002;12: Harisinghani MG, AJR 2003;180:755-8
 (LE: 2b). Combined FNA and core biopsies can provide complementary results, especially for complex cystic lesions. (LE: 3). [27] Lang EK, Macchia RJ, Gayle B, et al. CT-guided biopsy of indeterminate. renal cystic masses (Bosniak 3 and 2F): accuracy and. impact on clinical management. Eur Radiol 2002;12:2518–24. [28] Harisinghani MG, Maher MM, Gervais DA, et al. Incidence of. malignancy in complex cystic renal masses (Bosniak category III): should imaging-guided biopsy precede surgery AJR Am J Roentgenol. 2003;180:755–8. Lang EK, Eur Radiol 2002;12: Harisinghani MG, AJR 2003;180:")
24
“Biopsy has not been ‘a must’ in the diagnostic algorithm
Da sempre l’urologo ha detto no alle biopsie delle masse renali perché considerate inattendibili (incapaci di modificare la strategia terapeutica) e pericolose. “Fine-needle aspiration or biopsy has traditionally been of limited value in the evaluation of renal masses……. The major problems with this technique are the high incidence of false-negative biopsy findings in patients with renal malignant neoplasms and the difficulty differentiating renal oncocytoma from the common eosinophilic variants of RCC with limited pathologic material “(Herts and Baker, 1995; Schatz and Lieber, 2003). Campbell- Walsh Urology 2010 “Biopsy has not been ‘a must’ in the diagnostic algorithm of the renal masses and it has traditionally been reserved for dubious cases to either exclude or confirm origin in metastatic disease”.
 e pericolose. Fine-needle aspiration or biopsy has traditionally been of limited value in the evaluation of renal masses……. The major problems with this technique are the high incidence of false-negative biopsy findings in patients with renal malignant neoplasms and the difficulty differentiating renal oncocytoma from the common eosinophilic variants of RCC with limited pathologic material (Herts and Baker, 1995; Schatz and Lieber, 2003). Campbell- Walsh Urology Biopsy has not been ‘a must’ in the diagnostic algorithm. of the renal masses and it has traditionally been reserved. for dubious cases to either exclude or confirm origin in. metastatic disease .")
25
All’analisi multivariata la dimensione del tumore ed il tipo tumorale solido correlano significativamente con la probabilità di ottenere una biopsia diagnostica fattori predittivi di affidabilità diagnostica

26
Da sempre l’urologo ha detto no alle biopsie delle masse renali perché considerate inattendibili (incapaci di modificare la strategia terapeutica) e pericolose. Current risk estimated to be about 0.01 %

27
BIOPSIA DELLA MASSE RENALI
INCERTEZZE STORICHE SICUREZZA Rischio di sanguinamento Rischio di seeding

28
Da sempre l’urologo ha detto no alle biopsie delle masse renali perché considerate inattendibili (incapaci di modificare la strategia terapeutica) e pericolose. L’incidenza di emorragia post- biopsia clinicamente significativa è estremamente bassa, (~1% ) L’insorgenza di uno pseudoaneurisma tardivo clinicamente significativo è altrettanto bassa (< 1%) . Maturen K.E. AJR 2007 Il rischio di sanguinamento spontaneo è elevato in presenza di angiomiolipoma , ma i casi da sottoporre a biopsia sono quelli “atipici” o epitelioidi non a rischio emorragico Bissler J.J. Kidney International 2004
 L’insorgenza di uno pseudoaneurisma tardivo clinicamente significativo è altrettanto bassa (< 1%) . Maturen K.E. AJR Il rischio di sanguinamento spontaneo è elevato in presenza di angiomiolipoma , ma i casi da sottoporre a biopsia sono quelli atipici o epitelioidi non a rischio emorragico Bissler J.J. Kidney International")
29
COMPLICANZE Autore No. Diametro ago Sanguinamento Neuzillet, 2004 88
Vasudevan, 2006 100 16 G 1 (1%) Somani, 2007 70 16-18 G 1 (1.4%) Maturen, 2007 152 2 (1.3%) Lebret, 2007 119 Volpe, 2008 Veltri, 2010 150 18-22 G 1 (0.7%)
 Somani, G. 1 (1.4%) Maturen, (1.3%) Lebret, Volpe, Veltri, G. 1 (0.7%)")
30
Alessandro Volpe, Eur Urol 62 (2012) 491-504
")
32
is unusual (0-1.4%) and generally self-limiting (42-111).
Overall, percutaneous biopsies have low morbidity. Spontaneously resolving subcapsular/perinephric haematoma and haematuria are the most frequently reported complications, while clinically significant bleeding is unusual (0-1.4%) and generally self-limiting (42-111). Overall, percutaneous biopsies have low morbidity. Spontaneously resolving subcapsular/perinephric haematoma and haematuria are the most frequently reported complications, while clinically significant bleeding is unusual (0-1.4%) and generally self-limiting (42-111). 42. Neuzillet Y, Lechevallier E, Andre M, et al. Accuracy and clinical role of fine needle percutaneous biopsy with computerized tomography guidance of small (less than 4.0 cm) renal masses. J Urol 2004 May;171(5): 111. Zardawi IM. Renal fine needle aspiration cytology. Acta Cytol 1999 Mar-Apr;43(2):
 and generally self-limiting (42-111). Overall, percutaneous biopsies have low morbidity. Spontaneously resolving subcapsular/perinephric. haematoma and haematuria are the most frequently reported complications, while clinically significant bleeding. is unusual (0-1.4%) and generally self-limiting (42-111). 42. Neuzillet Y, Lechevallier E, Andre M, et al. Accuracy and clinical role of fine needle percutaneous. biopsy with computerized tomography guidance of small (less than 4.0 cm) renal masses. J Urol May;171(5): Zardawi IM. Renal fine needle aspiration cytology. Acta Cytol 1999 Mar-Apr;43(2):")
33
quality cores (nonfragmented, > 10 mm in length) should be obtained, and necrotic areas should be avoided in order to maximize the diagnostic yield (42,44,47,48,50) (LE: 4). Peripheral biopsies are preferable for larger tumours, to avoid areas of central necrosis (56) (LE: 2b). 42. Neuzillet Y, Lechevallier E, Andre M, et al. Accuracy and clinical role of fine needle percutaneous biopsy with computerized tomography guidance of small (less than 4.0 cm) renal masses. J Urol 2004 May;171(5):
 renal masses. J Urol May;171(5):")
34
In recent series from experienced centers, core biopsies of solid renal tumours have shown a
diagnostic yield of 78-97%, high specificity (98-100%), and high sensitivity (86-100%) for the diagnosis of malignancy (42-50,54,55,57-75) (LE: 2b). However, it should be noted that % of core biopsies are nondiagnostic (42-50,54,55,57-75) (LE: 2b). If a biopsy is nondiagnostic, but there are radiologic findings suspicious for malignancy, a further biopsy or surgical exploration should always be considered (LE: 4).
, and high sensitivity (86-100%) for the diagnosis of. malignancy (42-50,54,55,57-75) (LE: 2b). However, it should be noted that % of core biopsies are. nondiagnostic (42-50,54,55,57-75) (LE: 2b). If a biopsy is nondiagnostic, but there are radiologic findings. suspicious for malignancy, a further biopsy or surgical exploration should always be considered (LE: 4).")
35
BIOPSIA DELLA MASSE RENALI
INCERTEZZE STORICHE TECNICA Rischio di prelievo non diagnostico Errori di campionamento (eterogeneità intratumorale)
")
36
Come si può fare Percutaneous sampling of renal masses can be performed under local anesthesia in the majority of cases (42-51) (LE: 3). Depending on the tumour’s location, its echogenic features, and the patient’s physical characteristics, biopsies can be performed with either ultrasound or CT guidance, with a similar diagnostic yield (47,50) (LE: 2b).
 (LE: 3). Depending on the tumour’s location, its echogenic features, and the patient’s physical characteristics, biopsies can be performed with either ultrasound or CT guidance, with a similar diagnostic yield (47,50) (LE: 2b).")
37
BIOPSIA vs FINE-NEEDLE ASPIRATION (FNA)
FNA < BIOPSIA Materiale insufficiente per diagnosi Esperienza intraosservatore Percutaneous fine-needle aspiration (FNA) has also been used for cytologic diagnosis of renal masses. There is evidence that the accuracy of FNA for the diagnosis of malignancy is inferior to that of core biopsies and thatdiagnosis of tumour histotype and grade is possible in fewer cases on cytologic specimens [13,15,16,22,23]. However, some authors suggest that the two techniques can provide complementary results and eventually increase diagnostic rates and accuracy [24–27]. When FNA is performed before biopsy, an intraoperative check of the quality of the specimen by a dedicated cytologist may confirm the correct position of the guiding cannula within the tumour, thereby possibly increasing the likelihood of a diagnostic biopsy.
 has also been. used for cytologic diagnosis of renal masses. There is. evidence that the accuracy of FNA for the diagnosis of. malignancy is inferior to that of core biopsies and thatdiagnosis of tumour histotype and grade is possible in fewer. cases on cytologic specimens [13,15,16,22,23]. However, some authors suggest that the two techniques can provide. complementary results and eventually increase diagnostic. rates and accuracy [24–27]. When FNA is performed before. biopsy, an intraoperative check of the quality of the. specimen by a dedicated cytologist may confirm the correct. position of the guiding cannula within the tumour, thereby. possibly increasing the likelihood of a diagnostic biopsy.")
38
TECNICA BIOPTICA Biopsia Rx guidata (ago di Silverman)
Biopsia Eco guidata Biopsia TC guidata Biopsia RM guidata

39
Vantaggi - Limiti Ecografia Tac Semplice e rapida
Più gradita al paziente perché il decubito è più favorevole Può essere eseguita in ambienti diversi Non richiede norme di radioprotezione Mal eseguibile in lesioni molto piccole (<2 cm) Meno gradita al paziente per il decubito prono Maggiore durata Problemi di radioprotezione Possibilità di bioptizzare lesioni anche molto piccole (<2 cm)
 Meno gradita al paziente per il decubito prono. Maggiore durata. Problemi di radioprotezione. Possibilità di bioptizzare lesioni anche molto piccole (<2 cm)")
40
TECNICA COASSIALE

41
CONTROLLO QUALITA’ DEL CAMPIONE

42
Risk of non diagnostic specimen Specimen torn or less than 10 mm long
Immediate rebiopsy

43
ETEROGENEITA’ INTRATUMORALE
I vetrini di 43 ccRCC rimossi chirurgicamente e <3 cm sono stati riesaminati da un singolo anatomopatologo È stata valutata la presenza di eterogeneità di Fuhrman grading (I-II vs. III-IV) in aree differenti dello stesso tumore 7/43 tumori (16%) hanno mostrato eterogeneità intratumorale
 in aree differenti dello stesso tumore. 7/43 tumori (16%) hanno mostrato eterogeneità intratumorale.")
44
VARIABILITA’ INTEROSSERVATORE
È stata valutata la concordanza nella valutazione di adeguatezza del prelievo, istotipo e grado tumorale con indice kappa di Cohen Biopsie su banco sono state eseguite su 45 RCC rimossi chirurgicamente ed esaminate in cieco da due anatomopatologi ADEGUATEZZA BIOPSIE CENTRALI BIOPSIE PERIFERICHE Indice K= 0,82 Indice K= 0,91 ISTOTIPO Indice K= 0.94 GRADO DI FUHRMAN BIOPSIE CENTRALI BIOPSIE PERIFERICHE Indice K = 0,52 Indice K =0,63

45
BIOPSIA DELLA MASSE RENALI PERCHE’ RICONSIDERARNE IL RUOLO?
SEER DATABASE ( )
")
46
RCC – MIGRAZIONE DI STADIO NATIONAL CANCER DATABASE
STAGE I SIZE 4.1 cm 3.6 cm NATIONAL CANCER DATABASE ( ) Kane et al., Cancer 2007
 Kane et al., Cancer")
47
Small renal masses INCREASED NUMBER OF SURGICAL TREATMENTS
Hollingsworth et al., JNCI 2006

48
Competing risk analysis 26,000 pts
LA MORTE PER TUMORE RENALE LOCALIZZATO E’ EVENTO RARO PAZIENTI CON ETA’ > 70 ANNI HANNO UNA PROBABILITA’ DEL 30-40% DI MORIRE PER ALTRA CAUSA NEI 5 ANNI CHE SEGUONO L’ASPORTAZIONE CHIRURGICA DI UN TUMORE RENALE Competing risk analysis 26,000 pts < 4 cm – 5% cancer risk death within 5 years > 4 cm - 18% cancer risk death within 5 yrs, despite surgery > 70 years, 28% competing-cause mortality, regardless of tumor size Hollingsworth et al, Cancer 2007

49
A 5y Comprehensive Nomogram of Competing Risks of Death
Uomo di 78 anni con ccRCC diametro 2.5 cm: - 18% rischio a 5 anni di mortalittà per causa non neoplastica - 16% rischio a 5 anni di mortalità per altra neoplasia - 3% rischio a 5 anni di mortalità per RCC

50
In 2010 more and more incidental cases of SRM were found in elderly patients

51
SRM in 2011, looking at histological and functional characterization
The questions are: Benign or malignant? If malignant what grade of malignancy? If malignant how fast will it grow? If malignant how great is the risk of metastasis?

52
PICCOLE MASSE RENALI IMAGING ACCURATO, MA…
scarso potere discriminatorio Autore No. Diametro medio (cm) Istologia benigna Gill, 2007 771 2.7 215 (28%) Moinzadeh, 2007 100 3.1 32 (32%) Link, 2005 217 2.6 73 (34%) Venkatesh, 2006 123 37 (31%) Bollens, 2007 39 2.3 17 (44%) Beverley, 2008 174 2.9 44 (25%)
 Istologia benigna. Gill, (28%) Moinzadeh, (32%) Link, (34%) Venkatesh, (31%) Bollens, (44%) Beverley, (25%)")
54
Ogni cm in più nelle dimensioni del tumore determina
una percentuale del 17% in più di malignità

55
Tumor Size Low Grade (%) High Grade (%) Totals < 4 cm 7729 (86) 1250 (14) 8979 4-7 cm 5015 (79) 1361 (21) 6376 > 7 cm 2439 (70) 1024 (30) 3463 15183 (81) 3635 (19) 18818
 > 7 cm (70) 1024 (30) (81) 3635 (19)")
56
in rapporto alle dimensioni della neoplasia
Confronto tra alto e basso grado di malignità dei tumori renali a cellule chiare in rapporto alle dimensioni della neoplasia Ogni incremento di 1 cm nelle dimensioni dei tumore determina un aumento del 32% del rischio di una neoplasia di alto grado rispetto al basso grado

57
Median follow-up approx. 3 years

58
9 studies renal masses

59
Combined Mean growth cm / year Chawla et al, J Urol, 2006

61
IN PAZIENTI NON IDONEI ALLA CHIRURGIA
C’E’ UNA ALTERNATIVA ALLA BIOPSIA?

62
Size Growth rate

63
Può il «growth rate» rappresentare un
Fattore predittivo di «malignità? Esiste un cutoff di «size» correlato al growth rate?

64
Ogni cm in più nelle dimensioni del tumore determina una percentuale del 17%
in più di malignità J Urol Dec;170(6 Pt 1):
:")
65
Per ogni incremento di 1 cm nelle dimensioni del tumore si osserva:
+ 17% di tumori a cellule chiare rispetto ai tumori papillari - 9% dei tumori a cellule chiare rispetto ai tumori cromofobi - 19% dei tumori papillari rispetto ai tumori cromofobi J Urol Dec;170(6 Pt 1):
:")
66
Istologia delle SRM Medina SA.et al. Adv Urol, 2008

67
J Urol Dec;170(6 Pt 1):
:")
68
32% del rischio di una neoplasia di alto grado rispetto al basso grado
Confronto tra alto e basso grado di malignità dei tumori renali a cellule chiare in rapporto alle dimensioni della neoplasia Ogni incremento di 1 cm nelle dimensioni del tumore determina un aumento del 32% del rischio di una neoplasia di alto grado rispetto al basso grado

69
Medina SA.et al. Adv Urol, 2008

70
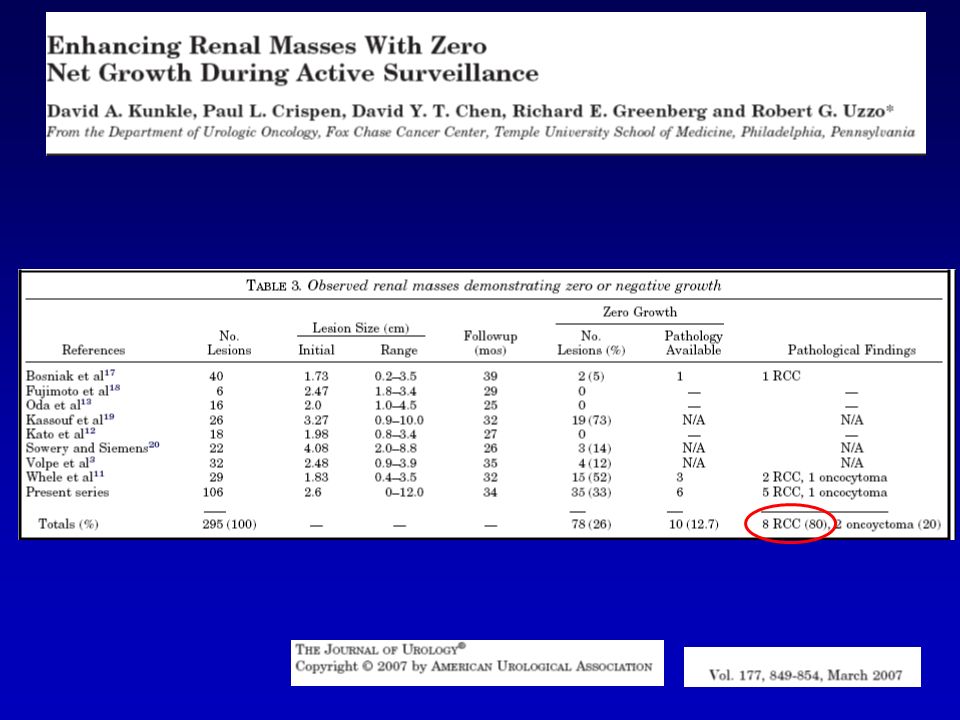
26-33% no growth

71
Prospective study of 82 patients with 84 renal masses
Average annual growth rate of 0.25 cm/yr (over a median follow-up of 3 yr.) Masses that are 2.45 cm in largest diameter at diagnosis grow more quickly than smaller masses.
 Masses that are 2.45 cm in largest diameter at. diagnosis grow more quickly than smaller masses.")
72
32% del rischio di una neoplasia di alto grado rispetto al basso grado
CONCLUSIONI Size e Growth rate GROWTH RATE SIZE growth rate/year SRM 0,25-0,28 cm/y Size > 2,45 cm faster Cut-off Ogni incremento di 1 cm nelle dimensioni dei tumore determina un aumento del 32% del rischio di una neoplasia di alto grado rispetto al basso grado

73
La sola velocità di crescita non può predire con accuratezza la malignità di una piccola massa renale in sorveglianza

74
The disease is often resistant to chemotherapy, but
targeted treatments, including tyrosine kinase inhibitors (TKIs; sunitinib (Motzer et al, 2007), sorafenib (Escudier et al, 2007a, 2009), pazopanib (Sternberg et al, 2010)), the vascular endothelial growth factor (VEGF) monoclonal antibody bevacizumab (Escudier et al, 2007b) and temsirolimus and everolimus (inhibitors of the mammalian target of rapamycin pathway) (Hudes et al, 2007; Motzer et al, 2008, 2010), have demonstrated clinical benefit in these patients. Axitinib is a potent and selective second-generation inhibitor of VEGF receptors (VEGFR)-1, 2, and 3 (Hu-Lowe et al, 2008)
, sorafenib (Escudier et al, 2007a, 2009), pazopanib (Sternberg et al, 2010)), the vascular endothelial. growth factor (VEGF) monoclonal antibody bevacizumab. (Escudier et al, 2007b) and temsirolimus and everolimus. (inhibitors of the mammalian target of rapamycin pathway) (Hudes et al, 2007; Motzer et al, 2008, 2010), have demonstrated. clinical benefit in these patients. Axitinib is a potent and selective second-generation inhibitor of. VEGF receptors (VEGFR)-1, 2, and 3 (Hu-Lowe et al, 2008)")
76
PICCOLE MASSE RENALI E’ necessaria una migliore definizione istologica mediante biopsia percutanea Malignità Istotipo Grado tumorale

77
SITUAZIONI CLINICHE PARTICOLARI

78
per le piccole mase renali
Perché farla per le piccole mase renali Se può cambiare l’approccio terapeutico -Neoplasia benigna evitare l’intervento -RCC di basso grado in pazienti anziani -Diagnosi istologica prima e dopo di un trattamento miniinvasivo

79
NECESSITA’ DELLA BIOPSIA NEI TUMORI SINCRONI MULTIPLI
La benignità di una lesione non esclude la malignità delle altre (Remzi M, Eur Urol 2009;55:359-67) Finally, in the presence of multiple and/or bilateral renal masses, we have to consider that the histology of a renal tumour does not predict the histologies of the other lesions. Therefore, if biopsy is considered in the case of synchronous renal tumours, all lesions should be biopsied [48]. [48] Remzi M, Marberger M. Renal tumor biopsies for evaluation of small renal tumors: why, in whom, and how? Eur Urol 2009;55: 359–67. TUTTE LE MASSE VANNO BIOPSIZZATE!
 Finally, in the presence of multiple and/or bilateral renal. masses, we have to consider that the histology of a renal. tumour does not predict the histologies of the other lesions. Therefore, if biopsy is considered in the case of synchronous. renal tumours, all lesions should be biopsied [48]. [48] Remzi M, Marberger M. Renal tumor biopsies for evaluation of. small renal tumors: why, in whom, and how Eur Urol 2009;55: 359–67. TUTTE LE MASSE VANNO BIOPSIZZATE!")
80
Tumor size e mortalità cancro specifica
SRMs Tumor size e mortalità cancro specifica -Tumor growth & T. size (pts >70aa.) NON CORRELANO - Più alto Charlson Comorbidity Index score (CCIs) >2 CORRELA SIGNIFICATIVAMENTE DOPO CHIRURGIA (Arrontes DS, J Urol 2008;179:857-61) Recent studies have shown that non-RCC– related mortality after surgical treatment for SRMs is significant and correlates with age and comorbidity [52,53]. A population-based analysis of patients who were surgically treated for locoregional kidney cancer between 1983 and 2002 showed that competing-cause mortality increases with increasing patient age, irrespective of tumour size (reaching 28.2% for patients >70 yr of age) [52]. In a retrospective review of 192 patients with clear cell RCC (ccRCC), Arrontes et al. observed that a higher Charlson Comorbidity Index (CCI) score (>2) is significantly associated with a worse overall survival (OS) after surgical treatment ( p < 0.001) [53]. [53] Arrontes DS, Acenero MJ, Gonzales JI, Munoz MM, Andres PP. Survival analysis of clear cell renal carcinoma according to the Charlson Comorbidity Index. J Urol 2008;179:857–61.
 NON CORRELANO. - Più alto Charlson Comorbidity Index score (CCIs) >2. CORRELA SIGNIFICATIVAMENTE DOPO CHIRURGIA. (Arrontes DS, J Urol 2008;179:857-61) Recent studies have shown that non-RCC– related mortality after surgical treatment for SRMs is. significant and correlates with age and comorbidity. [52,53]. A population-based analysis of patients. who were surgically treated for locoregional kidney cancer. between 1983 and 2002 showed that competing-cause. mortality increases with increasing patient age, irrespective. of tumour size (reaching 28.2% for patients >70 yr of age) [52]. In a retrospective review of 192 patients with clear cell. RCC (ccRCC), Arrontes et al. observed that a higher Charlson. Comorbidity Index (CCI) score (>2) is significantly associated. with a worse overall survival (OS) after surgical treatment. ( p < 0.001) [53]. [53] Arrontes DS, Acenero MJ, Gonzales JI, Munoz MM, Andres PP. Survival analysis of clear cell renal carcinoma according to the. Charlson Comorbidity Index. J Urol 2008;179:857–61.")
81
IMPORTANZA DELLA BIOPSIA NEL PROGRAMMI DI ACTIVE SURVEILLANCE
-Fattore basilare: «Rateo di crescita nel tempo» all’imaging Trattamento Rapida crescita Progressione The concept of active surveillance is based on the assessment of the tumour growth rate by serial abdominal imaging over time, with delayed intervention reserved for those masses that show rapid growth or signs of clinical progression during follow-up [56] Renal tumour biopsy can provide useful information for patients with a SRM who are not ideal surgical candidates because of their age and/or comorbidities

82
IMPORTANZA DELLA BIOPSIA NEL PROGRAMMI DI ACTIVE SURVEILLANCE
RCC alto grado RCC basso grado CCIs >2 Trattamento (Ch vs RFA) Active surveillance
 Active surveillance.")
83
BIOPSIA PRIMA DELLA TARGETED THERAPY
-Scarsa efficacia di Sunitinib e Sorafenib nelle forme «papillary» dei TKI (Choueiri TK, JCO 2008;26:127-31) -Maggiore efficacia dell’mTORi temsirolimus nelle forme “papillary” e nelle non clear cell (Dutcher JP, Med Oncol 2009;26:202-9) In some health care systems, biopsy may be formally required to start therapy because drug approval may be limited to patients with specific RCC subtypes At present, biopsy of the primary renal tumour is needed before starting systemic therapy formetastatic RCC to select the best-suited targeted therapy [3] recommended in all cases when a cytoreductive nephrectomy is not indicated orwhen neoadjuvant systemic therapy is planned [81] Choueiri TK, Plantade A, Elson P, et al. Efficacy of sunitinib and sorafenib in metastatic papillary and chromophobe renal cell carcinoma. J Clin Oncol 2008;26:127–31 In contrast, data from an exploratory subgroup analysis from the phase 3 global Advanced Renal Cell Carcinoma trial show that the efficacy of the mammalian target of rapamycin (mTOR) inhibitor temsirolimus (compared with interferon) appears more pronounced among patients with non-clear primary cell type and among patients with a papillary subtype than among those with clear cell histology or those without the papillary subtype [82] [82] Dutcher JP, de Souza P, McDermott D, et al. Effect of temsirolimus versus interferon-alpha on outcome of patients with advanced renal cell carcinoma of different tumor histologies. Med Oncol 2009;26:202–9.
 -Maggiore efficacia dell’mTORi temsirolimus nelle forme papillary e nelle non. clear cell. (Dutcher JP, Med Oncol 2009;26:202-9) In some health care systems, biopsy may be. formally required to start therapy because drug approval. may be limited to patients with specific RCC subtypes. At present, biopsy of the primary renal tumour is needed. before starting systemic therapy formetastatic RCC to select. the best-suited targeted therapy [3] recommended in all cases when a cytoreductive nephrectomy. is not indicated orwhen neoadjuvant systemic therapy. is planned. [81] Choueiri TK, Plantade A, Elson P, et al. Efficacy of sunitinib and. sorafenib in metastatic papillary and chromophobe renal cell. carcinoma. J Clin Oncol 2008;26:127–31. In contrast, data from an. exploratory subgroup analysis from the phase 3 global. Advanced Renal Cell Carcinoma trial show that the efficacy. of the mammalian target of rapamycin (mTOR) inhibitor. temsirolimus (compared with interferon) appears more. pronounced among patients with non-clear primary cell. type and among patients with a papillary subtype than. among those with clear cell histology or those without the. papillary subtype [82] [82] Dutcher JP, de Souza P, McDermott D, et al. Effect of temsirolimus. versus interferon-alpha on outcome of patients with advanced. renal cell carcinoma of different tumor histologies. Med Oncol. 2009;26:202–9.")
84
-Biopsia prima e dopo il trattamento ablativo (Crio o RFA)
Percutaneous biopsy can support the assessment of treatment outcomes after thermal ablation of small renal tumours -Biopsia prima e dopo il trattamento ablativo (Crio o RFA) -AUA ne stabilisce la indicazione se c’è «sospetto» di recidiva (Campbell SC, J Urol 2009;182:1271-9) [4] Campbell SC, Novick AC, Belldegrun A, et al. Guideline for management of the clinical T1 renal mass. J Urol 2009;182:1271–9.
 -AUA ne stabilisce la indicazione se c’è «sospetto» di recidiva. (Campbell SC, J Urol 2009;182:1271-9) [4] Campbell SC, Novick AC, Belldegrun A, et al. Guideline for management. of the clinical T1 renal mass. J Urol 2009;182:1271–9.")
86
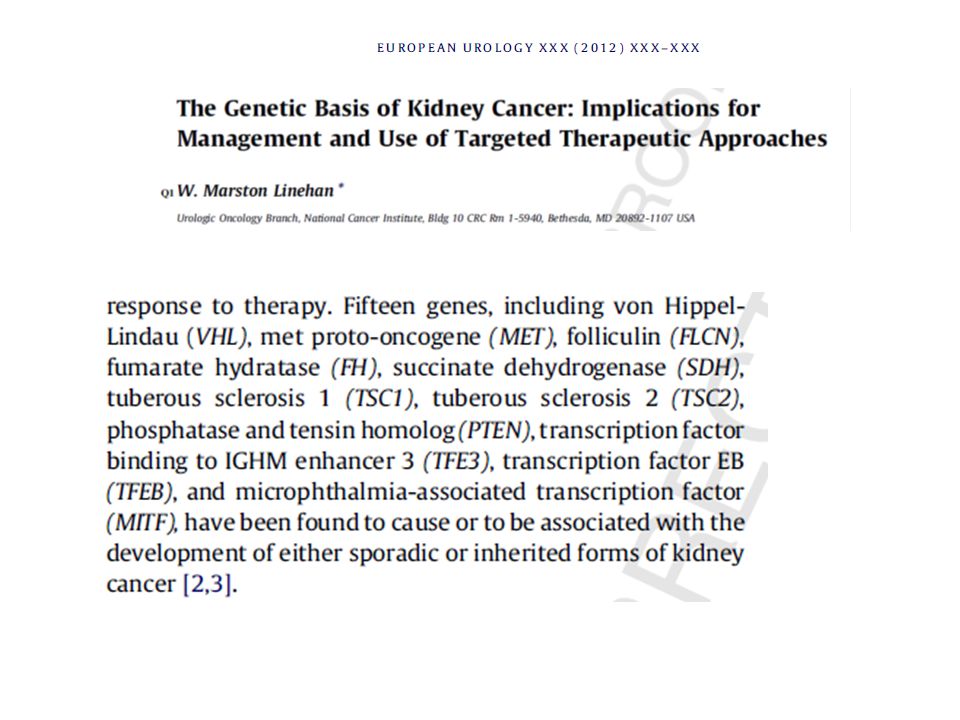
Rationale for molecular and genetic characterisation of
renal tumours on percutaneous biopsies [96] Gobbo S, Eble JN, Maclennan GT, et al. Renal cell carcinomas with papillary architecture and clear cell components: the utility of immunohistochemical and cytogenetical analyses in differential diagnosis. Am J Surg Pathol 2008;32:1780–6 Gobbo S, Am J Surg Pathol 2008; 32:1780-6

87
% Bx % Indeter. %FN %FP Accuracy
Failure Pathology Pre Post

88
CLINICAL IMPACT Author No. Mean size (cm) Wood, 1999 79 3.3 44%
Change of therapy (%) Wood, 1999 79 3.3 44% Neuzillet, 2004 88 2.8 48% Rybilowski, 2008 66 <4 6% Thullier, 2008 53 2.5 25% Volpe, 2008 100 2.4 43% Shannon, 2008 222 2.9 34%
 Wood, % Neuzillet, % Rybilowski, <4. 6% Thullier, % Volpe, % Shannon, %")
89
BIOPSIA PICCOLE MASSE RENALI
IMPATTO CLINICO Riduzione del numero di chirurgie non necessarie per patologia benigna Supporto nella scelta terapeutica sulla base delle caratteristiche istologiche in pazienti che sono candidati a trattamento conservativo

90
PICCOLE MASSE RENALI < 4 cm
Più ampio ventaglio di opzioni terapeutiche in pazienti selezionati Sorveglianza attiva con eventuale trattamento dilazionato Tecniche ablative miniinvasive - crioablazione - RFA - HIFU

92
Il ruolo della Biopsia percutanea

94
-Fistola a-v, pseudoaneurisma -Pneumotorace -Perforazione intestinale
Complicanze della biopsia renale percutanea Sanguinamento , in genere subclinico, in 1/3 dei casi Complicanze rare -Ematuria -Fistola a-v, pseudoaneurisma -Pneumotorace -Perforazione intestinale -Disseminazione neoplastica

95
BIOPSIA DELLA MASSE RENALI
INCERTEZZE SICUREZZA Rischio di sanguinamento Rischio di seeding TECNICA Rischio di prelievo non diagnostico Errori di campionamento (eterogeneità intratumorale) EFFICACIA Accuratezza diagnostica Impatto sulle decisioni cliniche x x x x
 EFFICACIA. Accuratezza diagnostica. Impatto sulle decisioni cliniche. x. x. x. x.")
96
Problemi principali di campionamento
Materiale non diagnostico Fattori predittivi che influiscono sulla appropriatezza diagnostica Diametro della massa (<3cm vs >3 cm) Numero e dimensione dei prelievi Presenza di un’altra neoplasia Esperienza del patologo Presenza di una componente cistica
 Numero e dimensione dei prelievi. Presenza di un’altra neoplasia. Esperienza del patologo. Presenza di una componente cistica.")
97
BIOPSIA DELLA MASSE RENALI
INCERTEZZE Definizione del miglior schema bioptico Accuratezza del grading tumorale su biopsia Diagnosi differenziale tra oncocitoma e carcinoma cromofobo

98
Small renal masses Certezze
Per questi tumori oggi il gold standard terapeutico è rappresentato dalla chirurgia conservativa Alternativa in casi selezionati : procedure ablative mini-invasive sorveglianza attiva con eventuale trattamento dilazionato Problematiche Elevata percentuale di neoplasie benigne( >20%) non sempre differenziabili dal carcinoma renale con le indagini strumentali (solo il 17% correttamente diagnosticate ;Remzi M.Eur.Urol. 2007). Small renal mass non è d’altra parte sinonimo obbligatorio di tumore benigno o di tumore maligno “non aggressivo “
 non sempre differenziabili dal carcinoma renale con le indagini strumentali (solo il 17% correttamente diagnosticate ;Remzi M.Eur.Urol. 2007). Small renal mass non è d’altra parte sinonimo obbligatorio di tumore benigno o di tumore maligno non aggressivo")
99
Razionale per tumori di piccole dimensioni
Biopsie Razionale per tumori di piccole dimensioni Quindi non sempre un piccolo tumore corrisponde ad un tumore innocuo Gli esami strumentali non ci consentono una valutazione del potenziale biologico di queste neoplasie Non disponiamo di markers sierologici utilizzabili per monitorare l’evoluzione di questi tumori Da un punto di vista decisionale può sorgere il dilemma : asportare?,osservare?

100
Può il risultato della biopsia modificare la strategia terapeutica ?
Sì: in caso di sorveglianza attiva la dimostrazione di un tumore high grade può sconsigliarne l’attuazione Sì: in presenza di lesione non ben tipizzata avviata verso un trattamento chirurgico:riscontro di patologia benigna ; o RCC low risk in un paziente high risk Sì: in caso di procedure ablative sia prima (lesioni benigne) che dopo (conferma o meno del risultato)
 che dopo (conferma o meno del risultato)")
101
Sì: in caso di procedure ablative sia prima (lesioni benigne) che dopo (conferma o meno del risultato) La valutazione del risultato dopo crioablazione o RFA si basa sulla dimostrazione di mancanza /presenza di enhancement della massa residua . Tuttavia la presenza di foci microscopici di tumore vitale può accompagnarsi alla mancanza di enhancement. Questo spiega la recidiva della lesione documentata strumentalmente solo a distanza di tempo

102
Tipizzazione della lesione
Possiamo migliorare questi risultati? Possiamo inoltre distinguere le forme aggressive dalle forme indolenti?

103
Future applicazioni della biopsia (analisi molecolare)
Definizione di fattori prognostici (studio del gene expression profile) Distinzione tra forme aggressive e forme indolenti Predire la risposta ad una terapia profilo completo dell’espressione genica
 Distinzione tra forme aggressive. e forme indolenti. Predire la risposta ad una terapia. profilo completo dell’espressione genica.")
105
ESISTONO «BIOMARCATORI» IN GRADO, OGGI, DI STABILIRE
IL RUOLO DI KILLER DELLE PICCOLE MASSE RENALI?

107
Pathology – molecular markers
None are routinely used However proliferation markers (Ki-67, PCNA) and somatic mutations in VHL gene are being explored
 and somatic mutations in VHL gene are being explored.")
108
Pathogenesis Role of VHL locus (3p)
VHL is mutated in 57% of sporadic cases In 98% of cases in which VHL is mutated there is LOH VHL expressed at high levels in kidney and brain Codes for elongin B and C facilitate rate of transcriptional elongation May also serve to suppress TGF- and TGF- Transfection of normal VHL into RCC cell lines leads to decrease tumor in mice but no decrease in growth in vitro

109
Grazie per l’attenzione

120
CONCLUSIONI Le piccole masse renali vanno «sempre» attentamente valutate Per masse al di sotto dI 1 cm , anche se maligne, non è riportato che abbiano date metastasi Per masse fino a 2.45 cm, il growth rate si attesta intorno a 0,25-0,28 cm/y Masse al di sopra di 2,45 cm crescono più rapidamente Ogni incremento di 1 cm determina un aumento del 32% di rischio di una neoplasia ad alto grado di malignità Non dimenticare che molte piccole masse, soprattutto se della midollare possono regredire dopo trattamento antibatterico quando siano reperto occasionale in comorbidità come pancreatiti o colecistiti in diabetici

121
GRAZIE PER L’ATTENZIONE
CONCLUSIONI In futuro la biologia molecolare con la introduzione di biomarcatori di malignità, affidabili e disponibili nella pratica clinica, saranno di grande aiuto nella definizione diagnostica e, soprattutto, nella scelta del tipo e della qualità del trattamento delle PICCOLE MASSE RENALI GRAZIE PER L’ATTENZIONE

Presentazioni simili



















 devices receive FDA approval annually 3500 medium-risk (class II) products are approved for marketing.>")



>")

