Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Valvulopatia Aortica Stenosi aortica Insufficienza aortica Steno-insufficienza aortica

2
Stenosi Aortica Ostruzione all’efflusso ventricolare sinistro. Localizzata a livello: Valvolare Sottovalvolare Sopravalvolare

3
Stenosi Aortica Eziologia
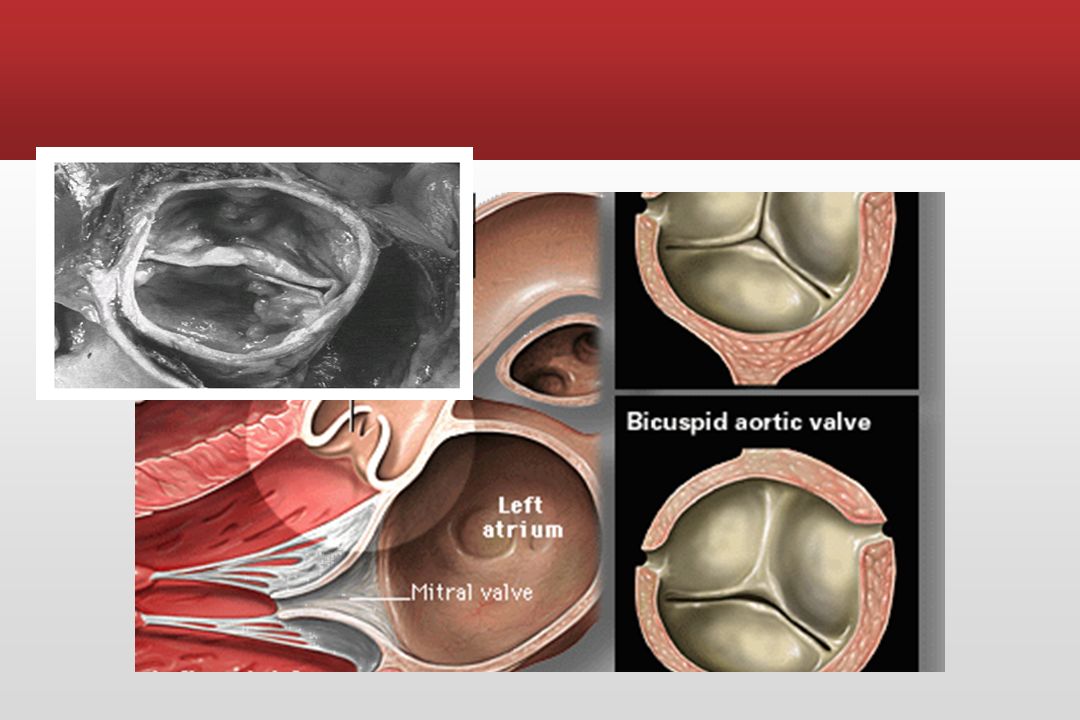
Congenita : Malformazioni a carico della valvola: Unicuspide Bicuspide Tricuspide Membrana sottovalvolare Stenosi sopravalvolare

4
Stenosi Aortica Eziologia
Acquisita: Reumatica Spesso si associa a valvulopatia mitralica Degenerativa (senile) Attualmente è la forma più frequente
 Attualmente è la forma più frequente.")
5
Eziologia della stenosi valvolare aortica
Euro Heart Survey sulle Valvulopatie Eziologia della stenosi valvolare aortica Iung B, EHJ (2003); 24: Iung B, et al. Eur Heart J 2003;24:1231
; 24: Iung B, et al. Eur Heart J 2003;24:1231.")
8
Stenosi Aortica Eziopatologia
Reumatica: Adesione e fusione delle cuspidi e delle commissure Retrazione e rigidità dei bordi delle cuspidi Calcificazione di entrambe le superfici L’orifizio è ridotto a una superficie spesso triangolare Spesso concomita insufficienza

9
Stenosi Aortica Eziopatologia
Degenerativa: Si pensava rappresentasse il risultato dello stress meccanico del flusso ematico su una valvola normale Attualmente si ritiene dovuta a: Cambiamenti infiammatori e proliferativi dovuti a: Accumulo lipidico Upregulation dell’attività ACE Infiltrazione di macrofagi e linfociti T Produzione di tessuto osseo

10
Stenosi Aortica Eziopatologia
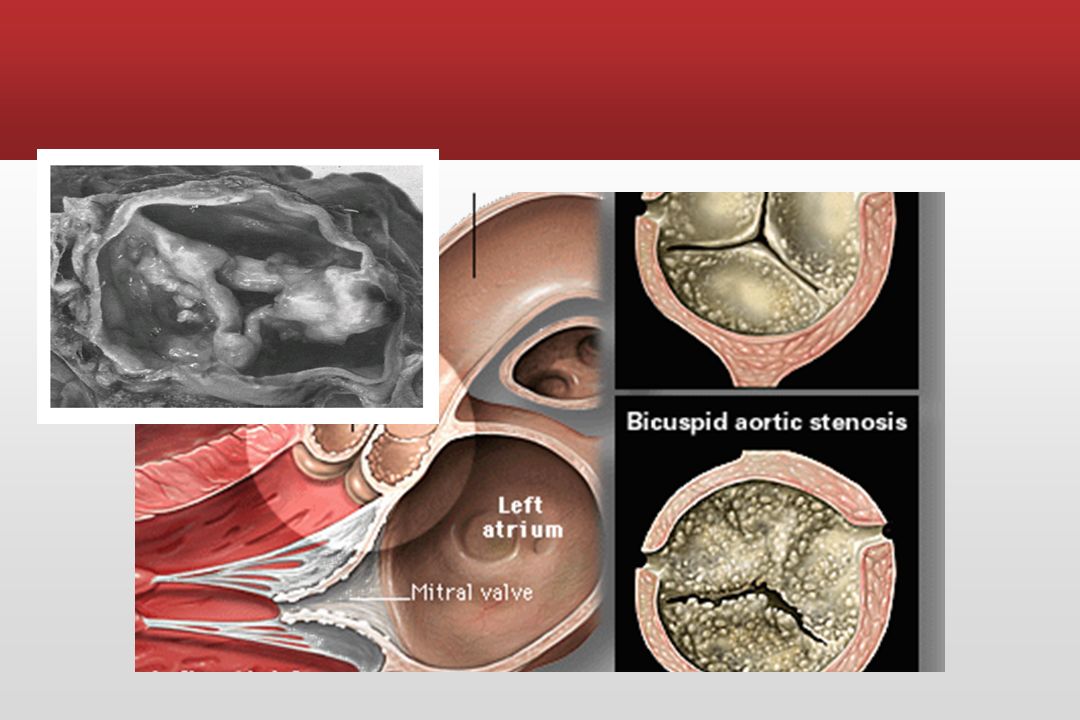
(Forma degenerativa) La calcificazione: Inizia dalla base delle cuspidi Ne determina immobilità Raramente la forma degenerativa determina insufficienza
 La calcificazione: Inizia dalla base delle cuspidi. Ne determina immobilità. Raramente la forma degenerativa determina insufficienza.")
11
Stenosi Aortica Fisiopatologia (1)
L’orifizio valvolare aortico è normalmente di 3-4 cm² Una stenosi aortica lieve ha una superficie di 1,5-2,0 cm² Una stenosi aortica moderata ha una superficie di 1-1,5 cm² Una stenosi aortica severa ha: Una superficie minore di 0,8 cm² Una superficie minore di 0,5cm²/m²

12
Stenosi Aortica Fisiopatologia (2)
La gittata sistolica è mantenuta dallo sviluppo di ipertrofia VS Questa determina una riduzione della compliance VS La contrazione atriale ha un ruolo importante nel riempimento VS In quanto aumenta la pressione telediastolica VS Necessaria per sviluppare una adeguata forza di contrazione Senza aumentare la pressione media atriale sinistra Effettuando, quindi, una protezione del circolo polmonare

13
Stenosi Aortica Fisiopatologia (3)
La perdita: Della contrazione atriale (fibrillazione atriale) Del sincronismo atrio-ventricolare (dissociazione AV) Può determinare un rapido deterioramento clinico nella SA
 Del sincronismo atrio-ventricolare (dissociazione AV) Può determinare un rapido deterioramento clinico nella SA.")
14
Storia Naturale della Stenosi Aortica
Può sussistere un lungo periodo (anche decadi) di asintomaticità (in questa fase il rischio di morte improvvisa è molto basso) La progressione della stenosi è pari a circa cm2/yr. (la media è 0.12 cm2/yr) Circa il 50% delle StAo non progredisce (attualmente non è possibile identificare precocemente le StAo che progrediranno) Sintomatici Solitamente presentano una StAo severa con un’AVA ≤0.9 cm2 Sintomatologia all’esordio: Angina Sincope Scompenso Cardiaco
 di asintomaticità (in questa fase il rischio di morte improvvisa è molto basso) La progressione della stenosi è pari a circa cm2/yr. (la media è 0.12 cm2/yr) Circa il 50% delle StAo non progredisce (attualmente non è possibile identificare precocemente le StAo che progrediranno) Sintomatici. Solitamente presentano una StAo severa con un’AVA ≤0.9 cm2. Sintomatologia all’esordio: Angina. Sincope. Scompenso Cardiaco.")
15
Storia Naturale della Stenosi Aortica
Ross J Jr, Braunwald E; Circulation 1968;37 (Suppl V):61
:61.")
16
Storia Naturale della Stenosi Aortica
I pazienti sintomatici non sottoposti a chirurgia presentano la seguente aspettativa media di vita: Angina = 5 anni Sincope = 3 anni HF = 2 anni La StAo è considerata un fattore di rischio indipendente di morbidità perioperatoria

17
Stenosi Aortica Fisiopatologia (4)
")
18
Fisiopatologia della Stenosi Aortica
Ostruzione all’efflusso VSx Gradiente di pressione transvalvolare Cronico Overload Pressorio VSx Ipertrofia Vsx

19
Funzione Miocardica nella StAo
Sviluppo dell’ipertrofia Vsx come sistema di adattamento (l’ipertrofia riduce lo stress di parete) L’ipertrofia VSx incrementa la stiffness diastolica
 L’ipertrofia VSx incrementa la stiffness diastolica.")
20
Ischemia nella StAo Massa VSx ipertrofica
Incremento della pressione sistolica Prolungamento dell’eiezione Riduzione della fase diastolica Riduzione relativa della densità capillare miocardica Alta incidenza di CAD concomitante

21
* Assumendo un normale cardiac output
Severità della StAo Assumendo una AVA normale pari a cm2 , la sintomatologia sopraggiunge quando l’AVA è ridotta di ~ 75% ( cm2) Area valvolare (cm2) Gradiente medio (mm Hg)* Lieve > 1.5 < 25 Moderata Severa < 0.9 > 50 * Assumendo un normale cardiac output
 Area valvolare (cm2) Gradiente medio (mm Hg)* Lieve > 1.5 < 25 Moderata Severa < 0.9 > 50 * Assumendo un normale cardiac output.")
22
Stenosi Aortica Sintomatologia
Angina pectoris Sincope Dispnea Scompenso cardiaco

23
Stenosi Aortica Sintomatologia
Angina pectoris Generalmente scatenata dallo sforzo e risolta con il riposo Presente in 2/3 dei pazienti Nel 50% in cui non è presente coronaropatia è dovuta All’aumentata richiesta di O2 dovuta all’ipertrofia Al ridotto apporto di O2 da compressione coronarica

24
Stenosi Aortica Sintomatologia
Sincope Generalmente da sforzo Ipoperfusione cerebrale vasodilatazione non bilanciata da aumento della portata Talora a riposo: Fibrillazione atriale o ventricolare (risoluzione spontanea) Blocco AV transitorio Perdita del contributo atriale
 Blocco AV transitorio. Perdita del contributo atriale.")
25
Stenosi Aortica Sintomatologia
Dispnea Da sforzo Ortopnea Parossistica notturna Edema polmonare acuto Riflettono vari gradi di ipertensione polmonare

26
Stenosi Aortica Sintomatologia
Angina Sopravvivenza media 5 anni se non operati Sincope Sopravvivenza media 3 anni se non operati Dispnea Sopravvivenza media 2 anni se non operati

27
Esame Obiettivo Aia cardiaca aumentata (generalmente a sinistra)
Soffio sistolico rude meglio udibile sui focolai della base T2 ridotto di intensità, talora assente (stenosi severa)
")
28
Diagnostica strumentale ECG

29
Ecocardiografia e Stenosi Aortica
Rilevare la valvulopatia e quantificarne la severità Definirne la sede (valvolare, sotto-sopravalvolare) Identificare eventuali patologie concomitanti (valvolari e non) Valutare la funzione sistolica ventricolare sinistra Valutare le ripercussioni sul circolo polmonare
 Identificare eventuali patologie concomitanti (valvolari e non) Valutare la funzione sistolica ventricolare sinistra. Valutare le ripercussioni sul circolo polmonare.")
30
Quantificazione della SA
Misurazione della velocità massima Calcolo dei gradienti transvalvolari massimo e medio Calcolo dell’area valvolare Rapporto tra velocità misurate nel TEVS ed all’orifizio aortico

36
Conclusioni Più frequente in vecchiaia
Ricercare segni all’esame obiettivo Ecocardiogramma per la valutazione della severità Asintomatici: Trattamento farmacologico e sorveglianza clinica Sintomatici: Valutazione per la chirurgia sostitutiva

37
INSUFFICIENZA AORTICA

38
Insufficienza Aortica
Malattia reumatica Endocardite Dissezione dell’arco aortico Trauma Patologie del tessuto connettivo Dexfenfluramina (anoressizzante serotoninergico)
")
39
Insufficienza Aortica

40
Storia naturale Lunghi periodi asintomatici in cui il VSx va incontro ad una progressiva ipertrofia eccentrica Scompenso cardiaco Angina

41
Fisiopatologia dell’IA
Flusso sanguigno retrogrado dall’aorta al VS (diastolico) Rapido calo della pressione aortica durante la diastole Aumento del volume e della pressione VS Aumento della pressione dell’AS Aumento della gittata sistolica (meccanismo di Frank-Starling) Aumento della pressione venosa polmonare Aumento della pressione sistolica di picco a causa dell’incremento della gittata nell’aorta Edema polmonare Aumento pressione polso L’aumento della tensione parietale diastolica produce ipertrofia eccentrica
 Rapido calo della pressione. aortica durante la diastole. Aumento del. volume e della. pressione VS. Aumento della. pressione dell’AS. Aumento della gittata sistolica. (meccanismo di Frank-Starling) Aumento della. pressione venosa. polmonare. Aumento della pressione. sistolica di picco a. causa dell’incremento. della gittata nell’aorta. Edema. polmonare. Aumento pressione polso. L’aumento della tensione. parietale diastolica produce. ipertrofia eccentrica.")
42
Ipertrofia eccentrica

43
Insufficienza aortica Principi di Fisiologia - Storia naturale
La fase latente, come per la StAo, può durare decadi Decompensazione quando La funzione sistolica VSx comincia a decadere Progressiva dilatazione del VSx Si sviluppa una geometria sferica Inizialmente questi processi sono reversibili La funzione sistolica del VSx ed il ESD sono i maggiori predittori di sopravvivenza postop e di recupero della funzione VSx

44
Rigurgito Aortico Fisiologia-Storia naturale
In pz asintomatici con normale EF la progressione è lenta 4.3%/anno sviluppa sintomi di disfunzione VSx 1.3%/anno progredisce a disfunzione VSX senza sintomi† † pool di dati da 7 serie di 490 pz con follow-up medio di 6.4 anni

46
Management della IA Generale: profilassi infettiva in caso di procedure odontoiatriche se presente protesi valvolare aortica o storia di endocardite. Medica: Vasodilatori (ACE-I), Nifedipina migliorano lo stroke volume e riducono l’insufficienza (solo nei pazienti sintomatici o ipertesi). Eco seriati: per monitorare la progressione Chirurgia: trattamento definitivo
, Nifedipina migliorano lo stroke volume e riducono l’insufficienza (solo nei pazienti sintomatici o ipertesi). Eco seriati: per monitorare la progressione. Chirurgia: trattamento definitivo.")
49
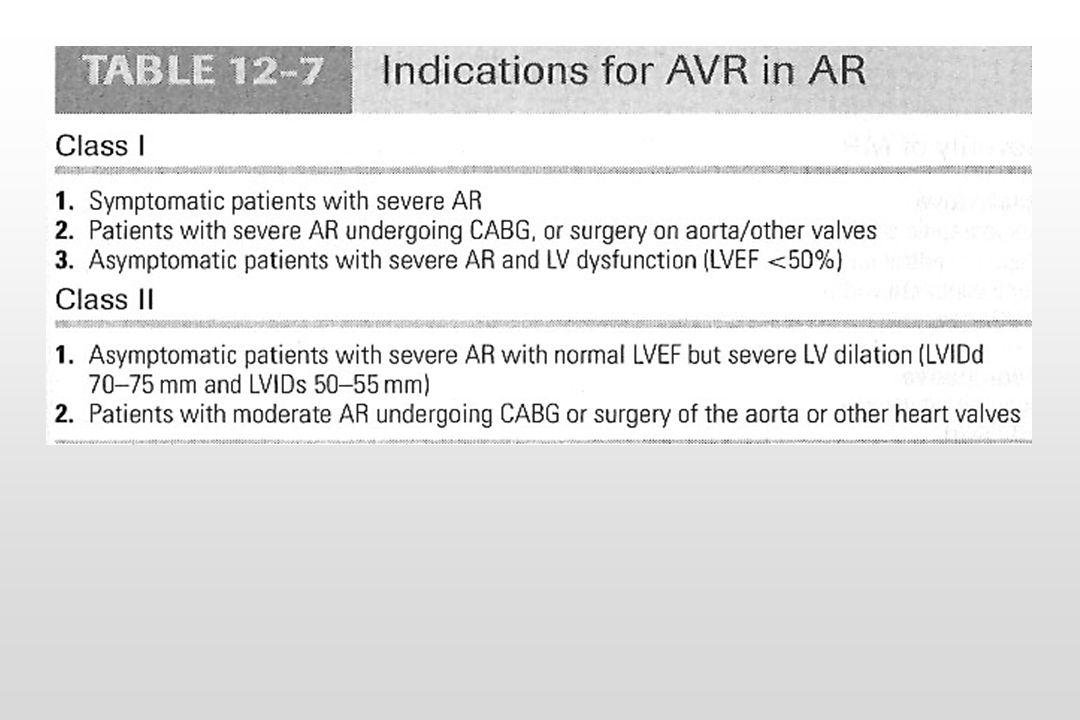
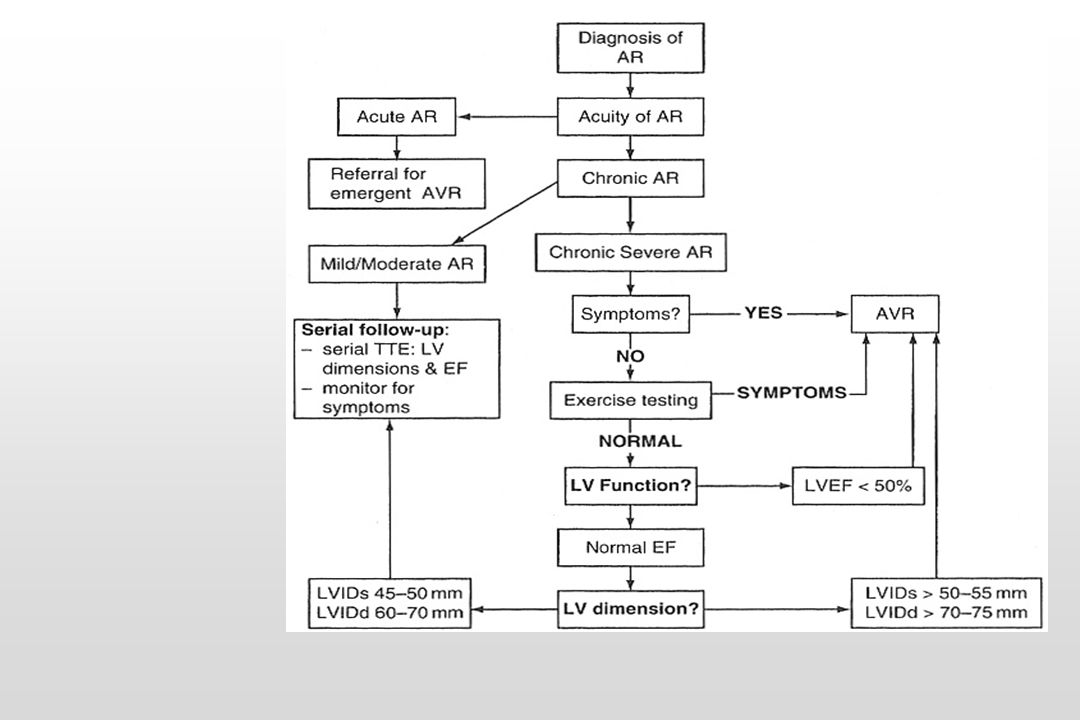
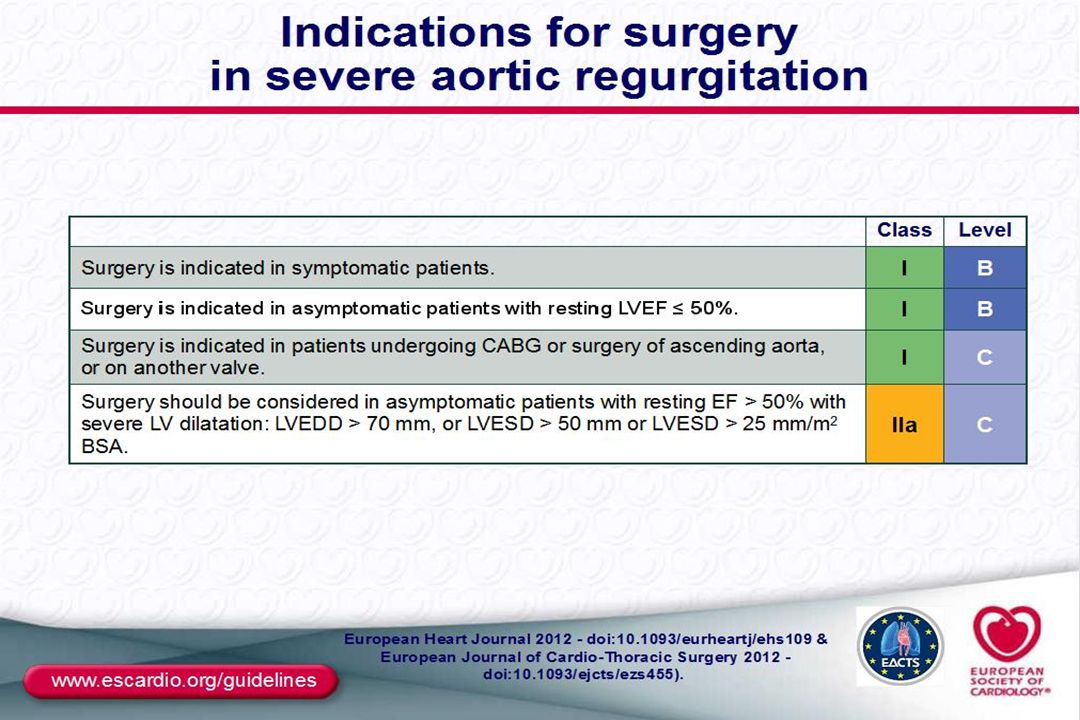
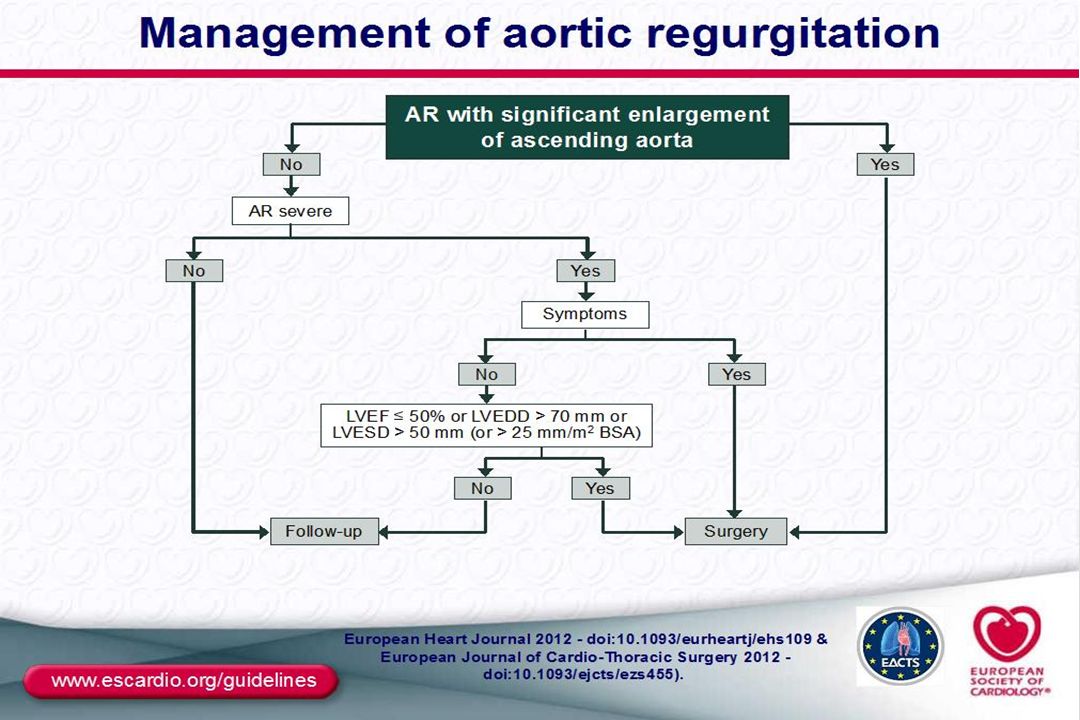
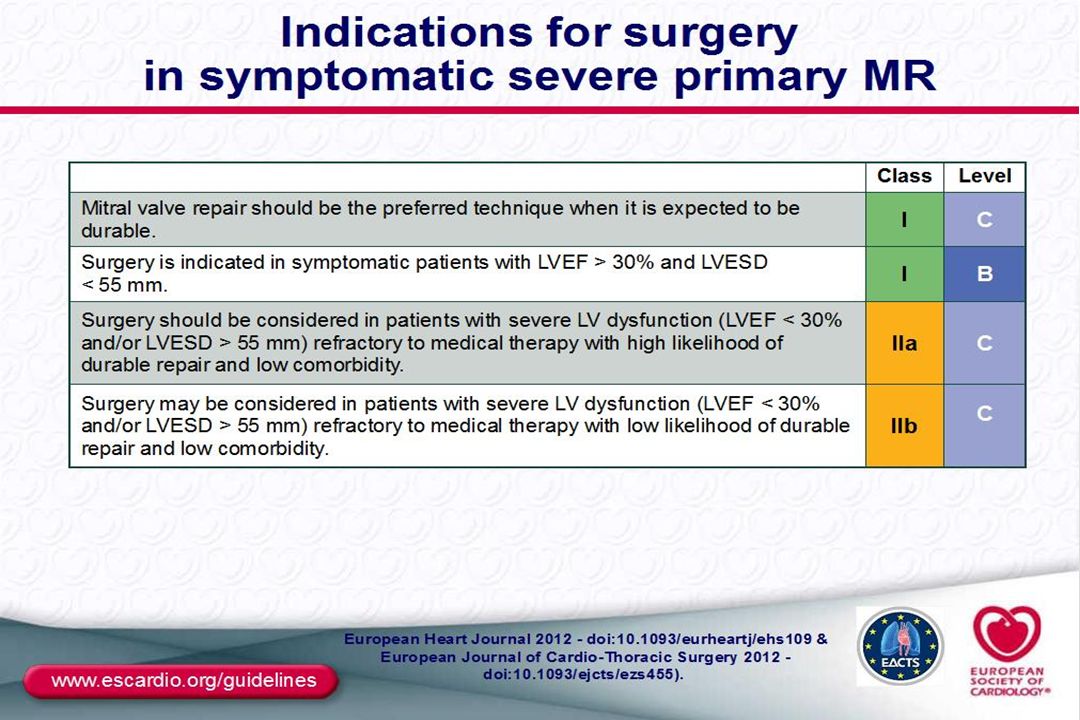
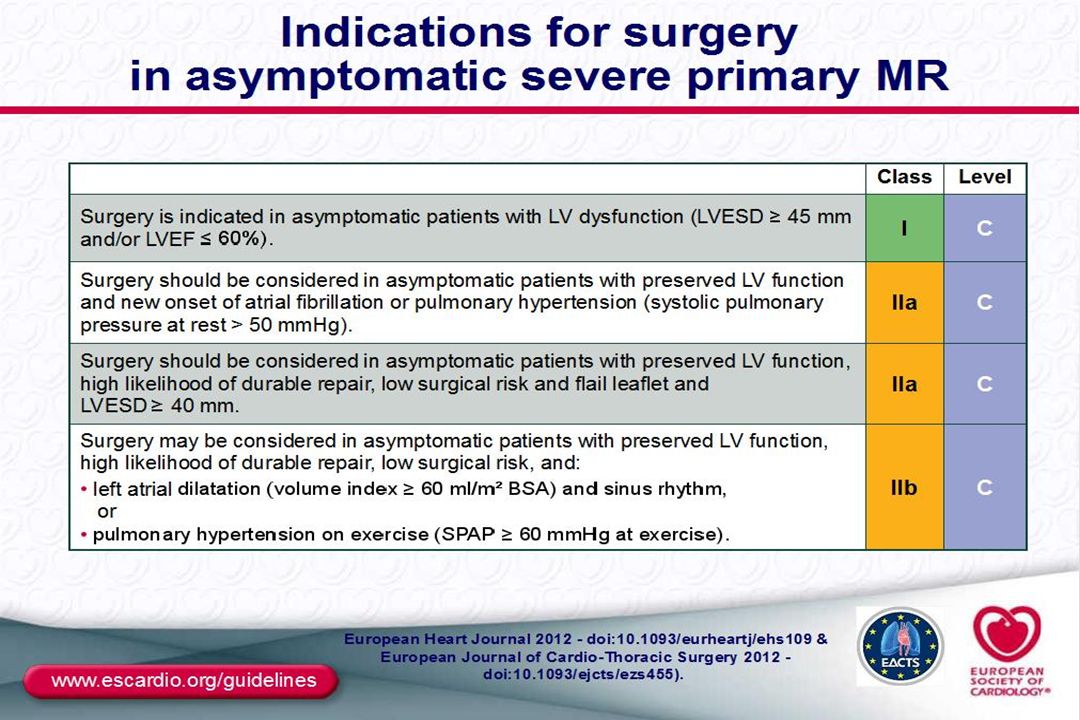
Indicazioni semplificate al trattamento chirurgico della IA
Qualsiasi sintomo a riposo o da sforzo Pazienti asintomatici se: FE scende a <50% o VSx dilatato

53
STENOSI MITRALICA

54
Stenosi mitralica Cause: Asintomatica per circa 20 anni
Reumatica Donne 4x > Uomini Congenita Artrite reumatoide LES Sindrome Carcinoide Asintomatica per circa 20 anni Sintomi di presentazione: Scompenso cardiaco (50%) Fibrillatione atriale
 Fibrillatione atriale.")
55
Stenosi mitralica

56
Fisiopatologia della stenosi mitralica
Ostruzione allo svuotamento dell’AS Diminuito riempimento del VS Aumento della pressione dell’AS Aumento delle dimensioni dell’AS Edema polmonare Aumento della pressione venosa polmonare Fibrillazione atriale Aumento della pressione arteriosa polmonare Sovraccarico del VD

57
Fisiopatologia: Vsx La funzione VSx è di solito nella norma
La FE è solitamente ridotta in 1/3 dei pts: Underloading cronico di volume CAD concomitante Ipertrofia del setto in pz con ipertensione polmonare

58
Stenosi mitralica Fisiologia/storia naturale
MVA Normale: 4 -5 cm2 I sintomi non compaiono sino ad un’area < 2.5 cm2 valve area (cm sq) mean gradient (mmHg)* Mild > < 5 Moderate Severe < > 10 * assumes normal cardiac output
 mean gradient (mmHg)* Mild > 1.5 < 5. Moderate Severe < 1.0 > 10. * assumes normal cardiac output.")
59
Stenosi mitralica Fisiologia/storia naturale
Fase latente (subclinica) anche per anni 10 anni di sintomi sino alla disabilità Con sintomi limitanti 10 aa: sopravvivenza 0-15% 10-20% embolia sistemica 30-40% sviluppano FA Con la comparsa di ipertensione polmonare severa : sopravvivenza media < 3 yrs Continually progressive lifelong disease These features become important when we later discuss management guidelines
 anche per anni. 10 anni di sintomi sino alla disabilità. Con sintomi limitanti. 10 aa: sopravvivenza 0-15% 10-20% embolia sistemica % sviluppano FA. Con la comparsa di ipertensione polmonare severa : sopravvivenza media < 3 yrs. Continually progressive lifelong disease. These features become important when we later discuss management guidelines.")
60
Esame obiettivo nella stenosi mitralica
Onda "a" prominente nelle pulsazioni venose giugulari: dovuta a ipertensione polmonare e ipertrofia ventricolare destra Segni di scompenso cardiaco destro: nella patologia in stadio avanzato Facies mitralica: quando la SM è grave e la gittata cardiaca risulta diminuita, si instaura vasocostrizione che conferisce agli zigomi un colorito violaceo

61
Stenosi mitralica Management
Trattamento Medico Profilassi febbre reumatica Profilassi endocardite infettiva Limitazione attività fisica Controllo FC (cronotropi negativi) Restrizione sodica, uso intermittente di diuretici Management della FA
 Restrizione sodica, uso intermittente di diuretici. Management della FA.")
62
Stenosi mitralica Management
Ecocardiogrammi: Lieve: 3-5 aa Moderata: 1-2 aa Severa: annualmente Farmaci: la SM come la StAo è un problema meccanico e la Tx farmacologica non previene la progressione -bloccanti, Ca-Ant, Digitale che controllona la FC e quindi prolungano la diastole per migliorare il riempimento diastolico Diuretici per l’overload di fluidi

64
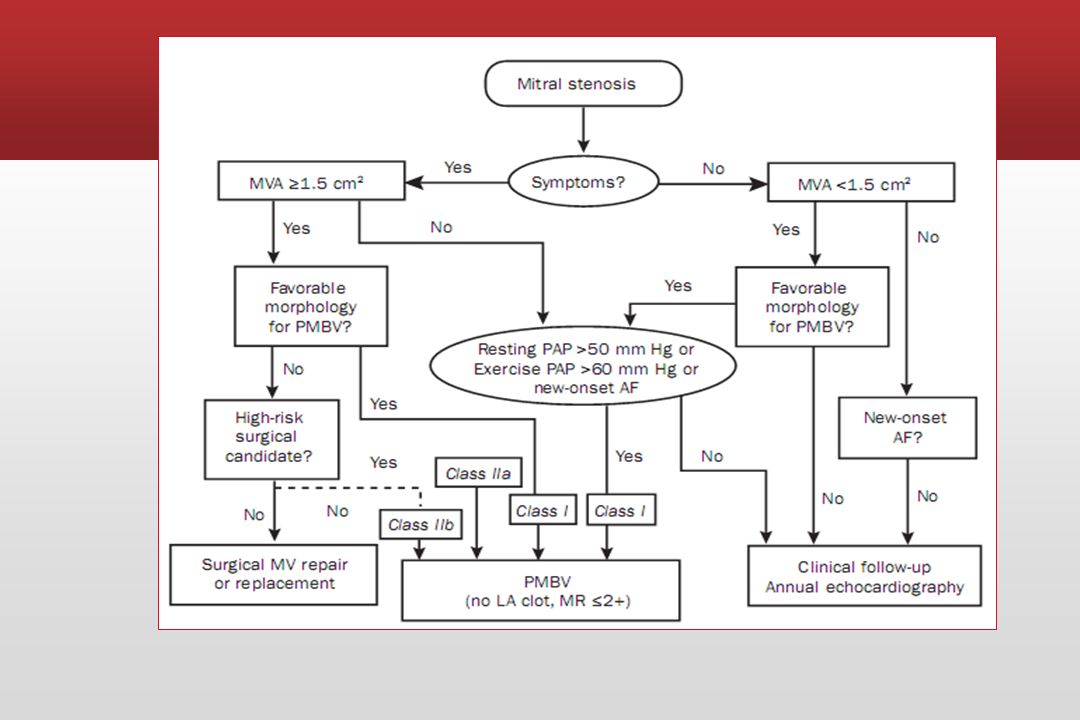
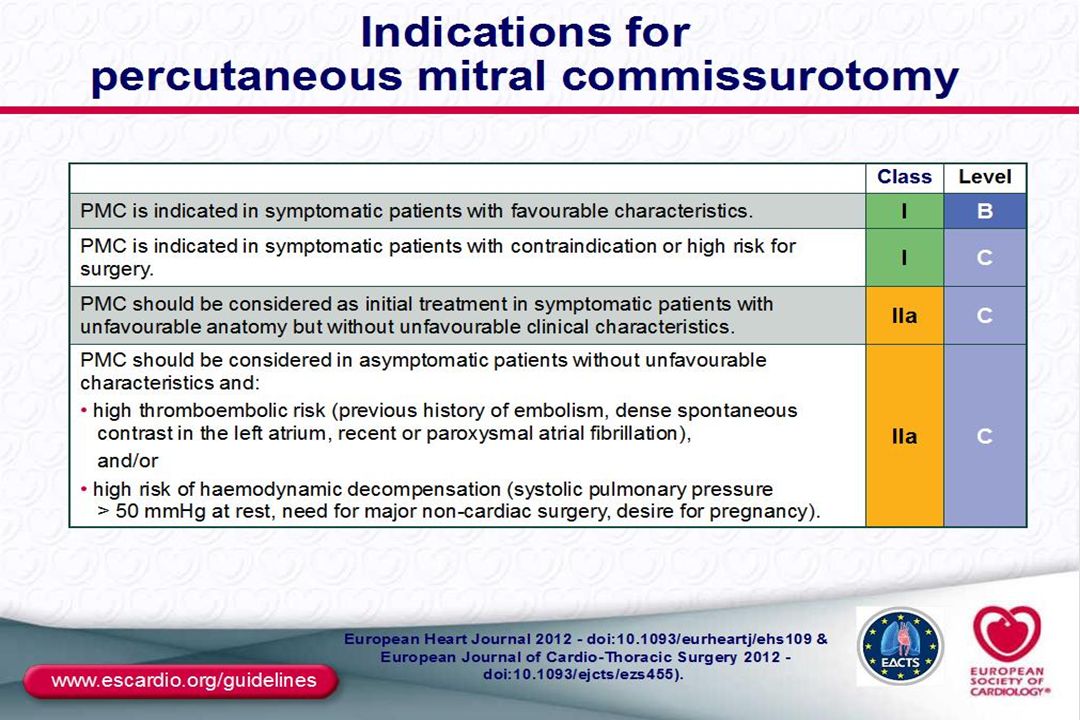
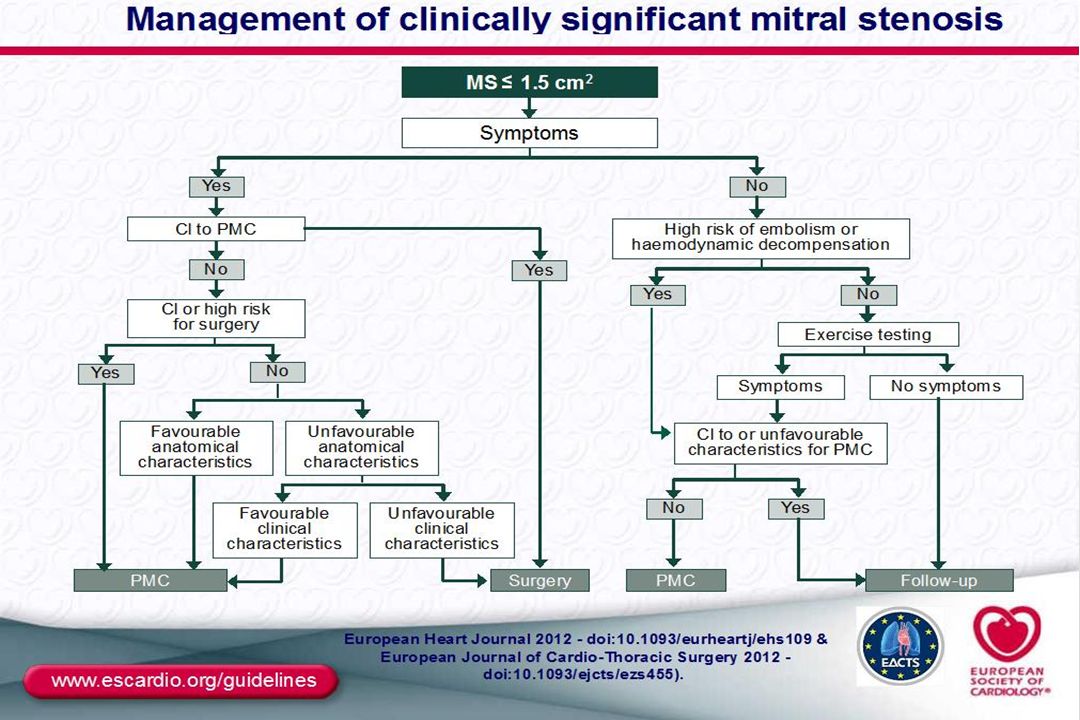
Indicazioni semplificate al trattamento chirurgico della stenosi mitralica
Stenosi moderato/severa nei casi in cui la valvuloplastica mitralica sia controindicata o non disponibile Pazienti sintomatici per stenosi mitralica moderato/severa con insufficienza mitralica concomitante

69
INSUFFICIENZA MITRALICA

70
Insufficienza mitralica
Leaflets valvolari Corde tendinee Muscoli papillari

71
Insufficienza mitralica
Malattia reumatica Endocardite Prolasso valvolare mitralico Allargamento anulus mitralico Ischemia Infarto miocardico Trauma

72
Fisiopatologia dell’IM
Flusso sanguigno retrogrado dal VS all’AS (sistolico) Ingrossamento dell’AS Aumento del volume e della pressione dell’AS Aumento della pressione venosa polmonare Aumentato riempimento del VS (aumento PTDVS) Edema polmonare Aumento gittata sistolica Sangue immesso nell’aorta
 Ingrossamento dell’AS. Aumento del. volume e della. pressione dell’AS. Aumento della. pressione venosa. polmonare. Aumentato riempimento. del VS (aumento PTDVS) Edema. polmonare. Aumento gittata. sistolica. Sangue immesso nell’aorta.")
73
Storia Naturale IM cronica (decorso variabile)
IM cronica può essere protetta dalla congestione polmonare per mezzo di un atrio sinistro ingrandito, altamente compliante IM acuta solitamente conduce ad edema polmonare fulminante

75
Management Farmaci Vasodilatori
Controllo della frequenza per la FA con -bloccanti, digitale Anticoagulazione in FA e Flutter Diuretici per l’overload di fluidi

76
Management Eco Seriati: Lieve: 2-3 aa Moderata: 1-2 aa
Severa: 6-12 mesi

77
Catheter Cardiovasc Interv (2003) 60:410-416
Effetti del dispositivo di anuloplastica sulla geometria dell’anulus mitralico A: nel rigurgito mitralico ischemico, i lembi mostrano una ridotta coaptazione. Il catetere guida è stato posizionato nel seno coronarico. B: il dispositivo di anuloplastica riduce la distanza tra l’anulus anteriore e posteriore, aumentando la coaptazione dei lembi. Catheter Cardiovasc Interv (2003) 60:
 60:")
82
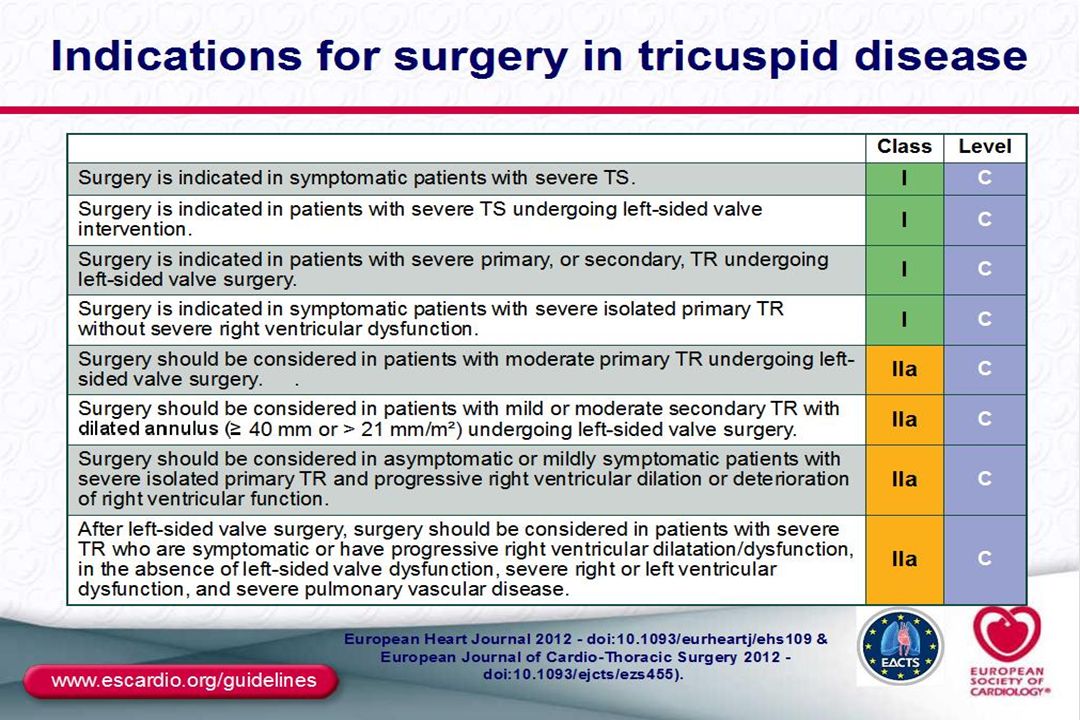
Stenosi tricuspidale Cause e fisiopatologia
Prevalentemente di origine reumatica Altre cause: atresia congenita, masse atriali destre, sindrome da carcinoide Nella maggior parte dei casi è associata a insufficienza tricuspidale e mitralica

83
Fisiopatologia Pesenza di un gradiente diastolico atrio-ventricolare. E’ sufficiente un gradiente di 5 mmHg per dare segni sistemici di congestione venosa, distensione delle giugulari, ascite e edema. Basta un gardiente diastolico medio di 2 mmHg per diagnosticare una stenosi della tricuspide.

84
Presentazione clinica
Astenia, epatomegalia, ascite

85
History • Progressive fatigue, edema, anorexia • Minimal orthopnea, paroxysmal nocturnal dyspnea • Rheumatic fever in two thirds of patients • Female preponderance • Pulmonary edema and hemoptysis rare Physical Findings • Signs of multivalvular involvement • Diastolic rumble at lower left sternal border, increasing in intensity with inspiration • Often confused with mitral stenosis • Peripheral cyanosis • Neck vein distention, with prominent a waves and slow y descent • Absent right ventricular lift • Associated murmurs of mitral and aortic valve disease • Hepatic pulsation • Ascites, peripheral edema Imaging Findings • ECG—tall right atrial P waves and no right ventricular hypertrophy • Chest roentgenogram—dilated right atrium without enlarged pulmonary artery segment • Echocardiogram—diastolic doming of tricuspid valve leaflet

86
Physical Examination . The lung fields are clear and, despite engorged neck veins and the presence of ascites and anasarca, the patient may be comfortable while lying flat. The auscultatory findings of the accompanying MS are usually prominent and often overshadow the more subtle signs of TS. A tricuspid OS may be audible but is often difficult to distinguish from a mitral OS. However, the tricuspid OS usually follows the mitral OS and is localized to the lower left sternal border, whereas the mitral OS is usually most prominent at the apex and radiates more widely. The diastolic murmur of TS is also commonly heard best along the lower left parasternal border in the fourth intercostal space and is usually softer, higher pitched, and shorter in duration than the murmur of MS. The presystolic component of the TS murmur has a scratchy quality and a crescendo- decrescendo configuration that diminishes before S1. The diastolic murmur and OS of TS are both augmented by maneuvers that increase transtricuspid valve flow, including inspiration, the Mueller maneuver (forced inspiration against a closed glottis), assumption of the right lateral decubitus position, leg raising, inhalation of amyl nitrite, squatting, and isotonic exercise. They are reduced during expiration or the strain of the Valsalva maneuver and return to control levels immediately (i.e., within two to three beats) after Valsalva release.
, assumption of the right lateral decubitus position, leg raising, inhalation of amyl nitrite, squatting, and isotonic exercise. They are reduced during expiration or the strain of the Valsalva maneuver and return to control levels immediately (i.e., within two to three beats) after Valsalva release.")
87
Echocardiography diastolic doming of the leaflets (especially the anterior tricuspid valve leaflet), thickening and restricted motion of the other leaflets, reduced separation of the tips of the leaflets, and a reduction in diameter of the tricuspid orifice. Doppler evaluation of TS has largely replaced the need for catheterization to assess severity. Electrocardiography The P wave amplitude in leads II and V1 exceeds 0.25 mV. Because most patients with TS have mitral valvular disease, the electrocardiographic signs of biatrial enlargement are commonly found. Radiography conspicuous enlargement of the right atrium (i.e., prominence of the right heart border), The vascular changes in the lungs characteristic of mitral valvular disease may be masked, with little or no interstitial edema or vascular redistribution, but left atrial enlargement may be present.
, thickening and restricted motion of the other leaflets, reduced separation of the tips of the leaflets, and a reduction in diameter of the tricuspid orifice. Doppler evaluation of TS has largely replaced the need for catheterization to assess severity. Electrocardiography. The P wave amplitude in leads II and V1 exceeds 0.25 mV. Because most patients with TS have mitral valvular disease, the electrocardiographic signs of biatrial enlargement are commonly found. Radiography. conspicuous enlargement of the right atrium (i.e., prominence of the right heart border), The vascular changes in the lungs characteristic of mitral valvular disease may be masked, with little or no interstitial edema or vascular redistribution, but left atrial enlargement may be present.")
88
Tricuspid Regurgitation
The most common cause of TR is not intrinsic involvement of the valve itself (i.e., primary TR) but rather dilation of the right ventricle and of the tricuspid annulus causing secondary (functional) TR] This may be a complication of RV failure of any cause. It is observed in patients with RV hypertension secondary to any form of cardiac or pulmonary vascular disease, most commonly mitral valve disease. TR can also occur secondary to RV infarction, congenital heart disease (e.g., pulmonic stenosis and pulmonary hypertension secondary to Eisenmenger syndrome,primary pulmonary hypertension and, rarely, cor pulmonale. Causes • Anatomically abnormal valve • Rheumatic • Nonrheumatic Infective endocarditis Ebstein anomaly Floppy (prolapse) Congenital (non- Ebstein) Carcinoid Papillary muscle dysfunction Trauma Connective tissue disorders (Marfan) Rheumatoid arthritis Radiation injury • Anatomically normal valve (functional) • Elevated right ventricular systolic pressure (dilated annulus)
 but rather dilation of the right ventricle and of the tricuspid annulus causing secondary (functional) TR] This may be a complication of RV failure of any cause. It is observed in patients with RV hypertension secondary to any form of cardiac or pulmonary vascular disease, most commonly mitral valve disease. TR can also occur secondary to RV infarction, congenital heart disease (e.g., pulmonic stenosis and pulmonary hypertension secondary to Eisenmenger syndrome,primary pulmonary hypertension and, rarely, cor pulmonale. Causes. • Anatomically abnormal valve. • Rheumatic • Nonrheumatic. Infective endocarditis Ebstein anomaly Floppy (prolapse) Congenital (non- Ebstein) Carcinoid Papillary muscle dysfunction Trauma Connective tissue disorders (Marfan) Rheumatoid arthritis Radiation injury • Anatomically normal valve (functional) • Elevated right ventricular systolic pressure (dilated annulus)")
89
Thus, organic TR may occur on a congenital basis as part of Ebstein anomaly, defects involving the atrioventricular canal, when the tricuspid valve is involved in the formation of an aneurysm of the ventricular septum, or in corrected transposition of the great arteries, or it may occur as an isolated congenital lesion. Rheumatic fever may involve the tricuspid valve directly. When this occurs, it usually causes scarring of the valve leaflets and/or chordae tendineae, leading to limited leaflet mobility and either isolated TR or a combination of TR and TS. Rheumatic involvement of the mitral, and often aortic, valves coexist. TR or the combination of TR and TS is an important feature of the carcinoid syndrome, which leads to focal or diffuse deposits of fibrous tissue on the endocardium of the valvular cusps and cardiac chambers and on the intima of the great veins and coronary sinus .The white, fibrous carcinoid plaques are most extensive on the right side of the heart, where they are usually deposited on the ventricular surfaces of the tricuspid valve and cause the cusps to adhere to the underlying RV wall, thereby producing TR. TR may result from prolapse of the tricuspid valve caused by myxomatous changes in the valve and chordae tendineae; prolapse of the mitral valve is usually present in these patients as well. Prolapse of the tricuspid valve occurs in about 20% of all patients with MVP Less common causes of TR include cardiac tumors (particularly right atrial myxoma), transvenous pacemaker leads, repeated endomyocardial biopsy in a transplanted heart, endomyocardial fibrosis, methysergide-induced valvular disease, exposure to fenfluramine-phentermine, and systemic lupus erythematosus involving the tricuspid valve.
, transvenous pacemaker leads, repeated endomyocardial biopsy in a transplanted heart, endomyocardial fibrosis, methysergide-induced valvular disease, exposure to fenfluramine-phentermine, and systemic lupus erythematosus involving the tricuspid valve.")
90
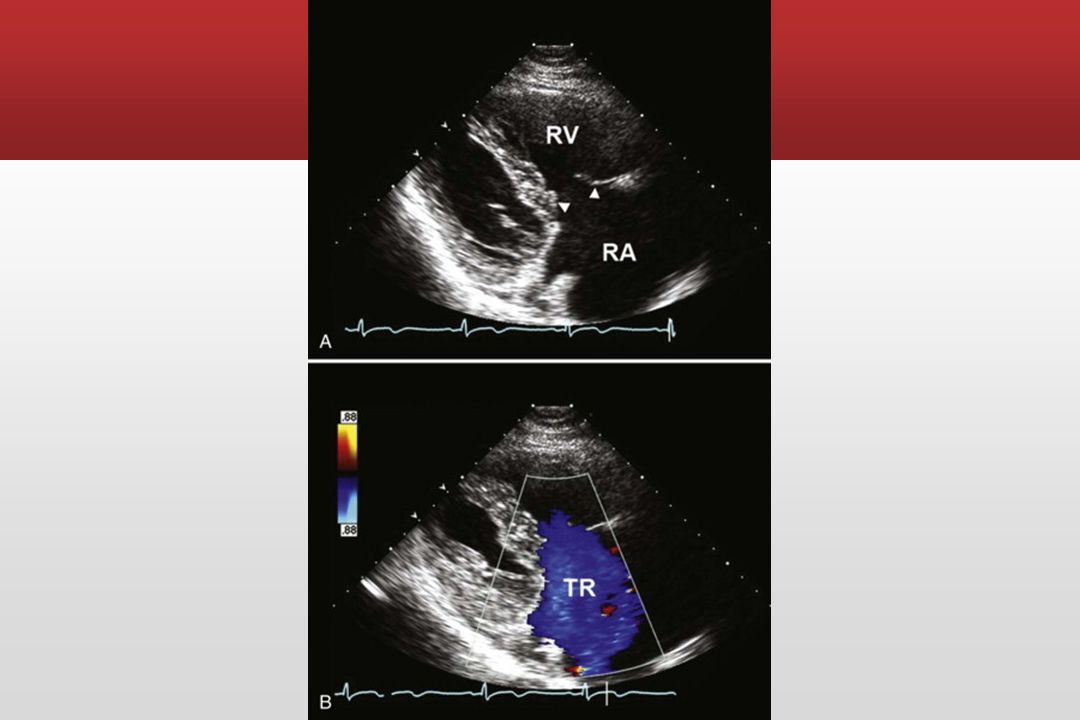
TR caused by carcinoid involvement of the tricuspid valve
TR caused by carcinoid involvement of the tricuspid valve. Serial two-dimensional echocardiograms (A and C) and color Doppler studies (B and D), separated by 3 years are shown. C, After 3 years, there is severe thickening and fixation of the tricuspid leaflets, leading to severe TR and associated right ventricular (RV) and right atrial (RA) enlargement.(From M?ller JE, Connolly HM, Rubin J, et al: Factors associated with progression of carcinoid heart disease. N Engl J Med 348:1005, 2003.)
 and color Doppler studies (B and D), separated by 3 years are shown. C, After 3 years, there is severe thickening and fixation of the tricuspid leaflets, leading to severe TR and associated right ventricular (RV) and right atrial (RA) enlargement.(From M ller JE, Connolly HM, Rubin J, et al: Factors associated with progression of carcinoid heart disease. N Engl J Med 348:1005, 2003.)")
91
Tricuspid valve prolapse, viewed from the right atrium (RA)
Tricuspid valve prolapse, viewed from the right atrium (RA). AL = anterior leaflet; PL = posterior leaflet; SL = septal leaflet.(From Virmani R, Burke AP, Farb A: Pathology of valvular heart disease. In Rahimtoola SH [ed]: Valvular Heart Disease. In Braunwald E [series ed]: Atlas of Heart Diseases. Vol 11. Philadelphia, Current Medicine, 1997, p 1.17.)
. AL = anterior leaflet; PL = posterior leaflet; SL = septal leaflet.(From Virmani R, Burke AP, Farb A: Pathology of valvular heart disease. In Rahimtoola SH [ed]: Valvular Heart Disease. In Braunwald E [series ed]: Atlas of Heart Diseases. Vol 11. Philadelphia, Current Medicine, 1997, p 1.17.)")
92
Clinical Presentation
In patients with TR secondary to dilation of the tricuspid annulus, the right atrium, right ventricle, and tricuspid annulus are all usually greatly dilated on echocardiography. There is evidence of RV diastolic overload with paradoxical motion of the ventricular septum similar to that observed in atrial septal defect. Exaggerated motion and delayed closure of the tricuspid valve are evident in patients with Ebstein anomaly. Prolapse of the tricuspid valve caused by myxomatous degeneration may be evident on echocardiography. Echocardiographic indications of tricuspid valve abnormalities, especially TR by Doppler examination, can be detected in most patients with carcinoid heart disease. In patients with TR caused by endocarditis, echocardiography may reveal vegetations on the valve or a flail valve. TEE enhances detection of TR. Doppler echocardiography is a sensitive technique for visualizing the TR jet. The magnitude of TR can be quantified using techniques similar to those used to evaluation MR.

94
Other Diagnostic Evaluation Modalities
Electrocardiography The ECG is usually nonspecific and characteristic of the lesion causing TR. Incomplete right bundle branch block, Q waves in lead V1, and AF are commonly found. Radiography In patients with functional TR, marked cardiomegaly is usually evident, and the right atrium is prominent. Evidence of elevated right atrial pressure may include distention of the azygos vein and the presence of a pleural effusion. Ascites with upward displacement of the diaphragm may be present.

96
Valvola polmonare The congenital form is the most common cause of pulmonic stenosis (PS). Rheumatic inflammation of the pulmonic valve is very uncommon, is usually associated with involvement of other valves, and rarely leads to serious deformity. Carcinoid plaques, similar to those involving the tricuspid valve, are often present in the outflow tract of the right ventricle of patients with malignant carcinoid. The plaques result in constriction of the pulmonic valve ring, retraction and fusion of the valve cusps, and either PS or the combination of PS and pulmonic regurgitation. Obstruction in the region of the pulmonic valve may be extrinsic to the valve apparatus and may be produced by cardiac tumors or by aneurysm of the sinus of Valsalva. Pulmonic Regurgitation Pulmonic regurgitation (PR) can result from dilation of the valve ring secondary to pulmonary hypertension (of any cause) or from dilation of the pulmonary artery. Infective endocarditis can involve the pulmonic valve, resulting in valve regurgitation. As more patients with congenital heart disease survive to adulthood, there is an increasing population of young adults with residual pulmonic regurgitation after surgical treatment of congenital PS or tetralogy of Fallot. PR may also result from various lesions that directly affect the pulmonic valve. These include congenital malformations, such as absent, malformed, fenestrated, or supernumerary leaflets. These anomalies may occur as isolated lesions but more often are associated with other congenital anomalies, particularly tetralogy of Fallot, ventricular septal defect, and pulmonic valvular stenosis. Less common causes include trauma, carcinoid syndrome, rheumatic involvement, injury produced by a pulmonary artery flow-directed catheter, syphilis, and chest trauma.
. Rheumatic inflammation of the pulmonic valve is very uncommon, is usually associated with involvement of other valves, and rarely leads to serious deformity. Carcinoid plaques, similar to those involving the tricuspid valve, are often present in the outflow tract of the right ventricle of patients with malignant carcinoid. The plaques result in constriction of the pulmonic valve ring, retraction and fusion of the valve cusps, and either PS or the combination of PS and pulmonic regurgitation. Obstruction in the region of the pulmonic valve may be extrinsic to the valve apparatus and may be produced by cardiac tumors or by aneurysm of the sinus of Valsalva. Pulmonic Regurgitation. Pulmonic regurgitation (PR) can result from dilation of the valve ring secondary to pulmonary hypertension (of any cause) or from dilation of the pulmonary artery. Infective endocarditis can involve the pulmonic valve, resulting in valve regurgitation. As more patients with congenital heart disease survive to adulthood, there is an increasing population of young adults with residual pulmonic regurgitation after surgical treatment of congenital PS or tetralogy of Fallot. PR may also result from various lesions that directly affect the pulmonic valve. These include congenital malformations, such as absent, malformed, fenestrated, or supernumerary leaflets. These anomalies may occur as isolated lesions but more often are associated with other congenital anomalies, particularly tetralogy of Fallot, ventricular septal defect, and pulmonic valvular stenosis. Less common causes include trauma, carcinoid syndrome, rheumatic involvement, injury produced by a pulmonary artery flow-directed catheter, syphilis, and chest trauma.")
97
Clinical Presentation
Physical Examination The right ventricle is hyperdynamic and produces palpable systolic pulsations in the left parasternal area, and an enlarged pulmonary artery often produces systolic pulsations in the second left intercostal space. Sometimes systolic and diastolic thrills are felt in the same area. A tap reflecting pulmonic valve closure is usually easily palpable in the second intercostal space in patients with pulmonary hypertension and secondary PR. Auscultation P2 is not audible in patients with congenital absence of the pulmonic valve; however, this sound is accentuated in patients with PR secondary to pulmonary hypertension. There may be wide splitting of S2 caused by prolongation of RV ejection accompanying the augmented RV stroke volume. A nonvalvular systolic ejection click due to the sudden expansion of the pulmonary artery by the augmented RV stroke volume frequently initiates a midsystolic ejection murmur, most prominent in the second left intercostal space. An S3 and S4 originating from the right ventricle are often audible, most readily in the fourth intercostal space at the left parasternal area, and are augmented by inspiration. In the absence of pulmonary hypertension, the diastolic murmur of PR is low-pitched and usually heard best at the third and fourth left intercostal spaces adjacent to the sternum. The murmur commences when pressures in the pulmonary artery and right ventricle diverge, approximately 0.04 second after P2. It is diamond- shaped in configuration and brief, reaching a peak intensity when the gradient between these pressures is maximal, and ending with equilibration of the pressures. The murmur becomes louder during inspiration. When systolic pulmonary arterial pressure exceeds approximately 55 mm Hg, dilation of the pulmonic annulus results in a high-velocity regurgitant jet resulting in the audible murmur of PR, or Graham Steell murmur. (Doppler ultrasonography reveals pulmonary regurgitation at much lower pulmonary arterial pressures.) This murmur is high-pitched, blowing, and decrescendo, beginning immediately after P2 and is most prominent in the left parasternal region in the second to fourth intercostal spaces. Thus, although it resembles the murmur of AR, it is usually accompanied by severe pulmonary hypertension—that is, an accentuated P2 or fused S2, an ejection sound, and a systolic murmur of TR, and not by a widened arterial pulse pressure. Sometimes, a low-frequency presystolic murmur is present, originating from increased diastolic flow across the tricuspid valve. The murmur of PR secondary to pulmonary hypertension usually increases in intensity with inspiration, is diminished during the Valsalva strain, and returns to baseline intensity almost immediately after release of the Valsalva strain. This PR murmur resembles and may be confused with the diastolic blowing murmur of AR. However, a diastolic blowing murmur along the left sternal border in patients with rheumatic heart disease and pulmonary hypertension (even in the absence of peripheral signs of AR) is usually caused by AR rather than PR.
 This murmur is high-pitched, blowing, and decrescendo, beginning immediately after P2 and is most prominent in the left parasternal region in the second to fourth intercostal spaces. Thus, although it resembles the murmur of AR, it is usually accompanied by severe pulmonary hypertension—that is, an accentuated P2 or fused S2, an ejection sound, and a systolic murmur of TR, and not by a widened arterial pulse pressure. Sometimes, a low-frequency presystolic murmur is present, originating from increased diastolic flow across the tricuspid valve. The murmur of PR secondary to pulmonary hypertension usually increases in intensity with inspiration, is diminished during the Valsalva strain, and returns to baseline intensity almost immediately after release of the Valsalva strain. This PR murmur resembles and may be confused with the diastolic blowing murmur of AR. However, a diastolic blowing murmur along the left sternal border in patients with rheumatic heart disease and pulmonary hypertension (even in the absence of peripheral signs of AR) is usually caused by AR rather than PR.")
98
Echocardiography Two-dimensional echocardiography shows RV dilation and, in patients with pulmonary hypertension, RV hypertrophy as well. RV function can be evaluated. Abnormal motion of the septum characteristic of volume overload of the right ventricle in diastole and/or septal flutter may be evident. The motion of the pulmonic valve may point to the cause of the PR. Absence of a waves and systolic notching of the posterior leaflet suggest pulmonary hypertension; large a waves indicate pulmonic stenosis. Doppler echocardiography is extremely accurate in detecting PR and in helping estimate its severity (see Fig and Fig ). Abnormal Doppler signals in the RV outflow tract with velocity sustained throughout diastole are generally observed in patients in whom PR is caused by dilation of the valve ring secondary to pulmonary hypertension. When the velocity falls during diastole, the pulmonary artery pressure is usually normal, and the regurgitation is caused by an abnormality of the valve itself. Electrocardiography In the absence of pulmonary hypertension, PR often results in an ECG that reflects RV diastolic overload—an rSr (or rsR) configuration in the right precordial leads. PR secondary to pulmonary hypertension is usually associated with ECG evidence of RV hypertrophy. Radiography Both the pulmonary artery and right ventricle are usually enlarged, but these signs are nonspecific. Fluoroscopy may demonstrate pronounced pulsation of the main pulmonary artery. PR can be diagnosed by observing opacification of the right ventricle following injection of contrast material into the main pulmonary artery, but this diagnosis is made in almost all patients with echocardiography or cardiac magnetic resonance.
. Abnormal Doppler signals in the RV outflow tract with velocity sustained throughout diastole are generally observed in patients in whom PR is caused by dilation of the valve ring secondary to pulmonary hypertension. When the velocity falls during diastole, the pulmonary artery pressure is usually normal, and the regurgitation is caused by an abnormality of the valve itself. Electrocardiography. In the absence of pulmonary hypertension, PR often results in an ECG that reflects RV diastolic overload—an rSr (or rsR) configuration in the right precordial leads. PR secondary to pulmonary hypertension is usually associated with ECG evidence of RV hypertrophy. Radiography. Both the pulmonary artery and right ventricle are usually enlarged, but these signs are nonspecific. Fluoroscopy may demonstrate pronounced pulsation of the main pulmonary artery. PR can be diagnosed by observing opacification of the right ventricle following injection of contrast material into the main pulmonary artery, but this diagnosis is made in almost all patients with echocardiography or cardiac magnetic resonance.")
Presentazioni simili