Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
AGGIORNAMENTO STUDI CLINICI IN CORSO
RIUNIONE MITO MESAGNE 19/01/2017 AGGIORNAMENTO STUDI CLINICI IN CORSO Domenica Lorusso

2
OVAIO PRIMA LINEA DI TRATTAMENTO
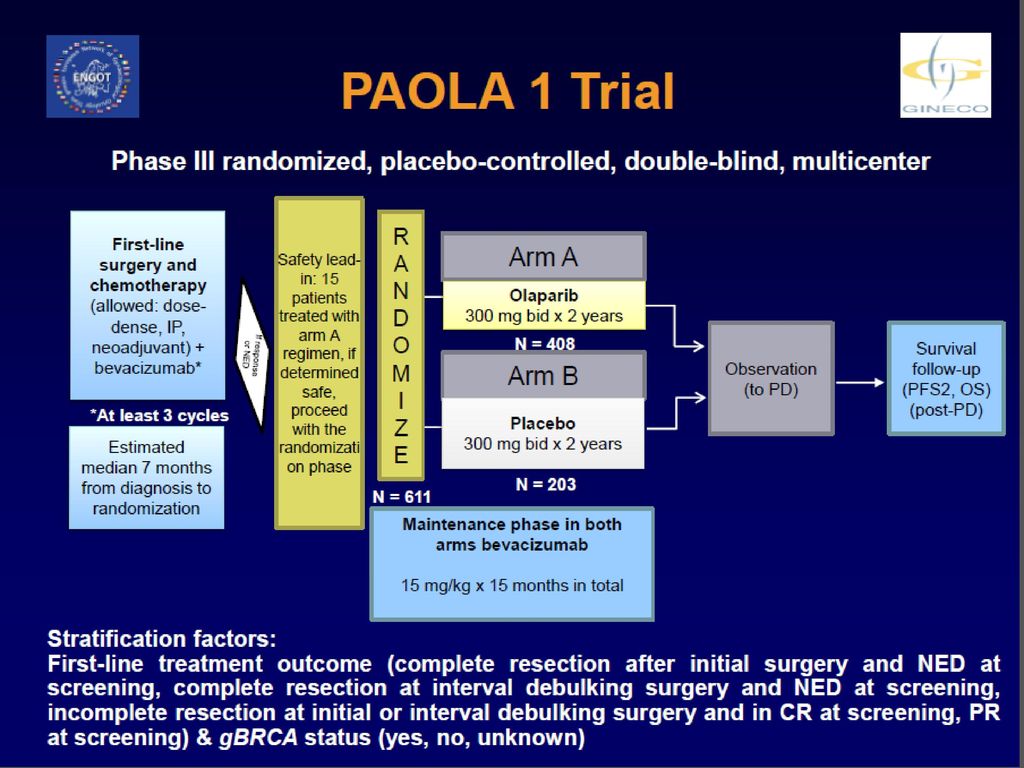
Mito 16 Chiuso PAOLA 1 Chiuso EWOC TRIAL (Coordinato da INT Milano) MITO 24 PDL 1, MITO 25 RUCAPARIB, PRIMA TRIAL : Coming soon
 MITO 24 PDL 1, MITO 25 RUCAPARIB, PRIMA TRIAL : Coming soon.")
4
Enrollment: 519 pts randomized
Date ARCAGY - GINECO 2015

5
Enrollment by group Date ARCAGY - GINECO 2015

6
Date ARCAGY - GINECO 2015

8
Elderly Women Ovarian Cancer
EWOC Elderly Women Ovarian Cancer Multicenter, randomized trial of carboplatin +/- paclitaxel in vulnerable elderly patients with stage III-IV advanced ovarian cancer Participating Groups GINECO, AGO, MITO, ANZGOG, Canada, JGOG, GOTIC, NSGO

9
Arm A : carboplatin AUC 5 + paclitaxel 175mg/m² q21 X 6 cycles
Arm B : carboplatin AUC 5-6 q21 X 6 cycles Arm C : carboplatin AUC 2 + paclitaxel 60 mg/m² weekly q28 (d1, d8, d15) x 6 cycles Patient >70 years old GVS* > 3 Rando EWOC DESIGN of Chemotherapy in Advanced OC (stage III-IV - Elderly Vulnerable Pts in an adjuvant or neoadjuvant setting ) *GVS = Geriatric Vunerability Score : - score ADL < 6 - score IADL < 25 - score HADS > 14 - albuminemia < 35g/L - Lymphopenia < 1G/L GVS = factors with vulnerable score
 x 6 cycles. Patient >70 years old. GVS* > 3. Rando. EWOC DESIGN of Chemotherapy in Advanced OC (stage III-IV - Elderly Vulnerable Pts in an adjuvant or neoadjuvant setting ) *GVS = Geriatric Vunerability Score : - score ADL < 6. - score IADL < score HADS > albuminemia < 35g/L. - Lymphopenia < 1G/L. GVS = factors with vulnerable score.")
10
Procedures of registration and randomization

11
+/- Interval debulking (stratified)
PRIMARY ENDPOINT To compare the rate of success to deliver 6 courses of chemotherapy without progression at 6 months or unacceptable toxicity* of 3 different regimens in vulnerable elderly patients Screening Chemotherapy 6 cycles 6 month visit Follow-up every 3 mo. (up to 2 years) GVS>3 Imagery QOL Imagery QOL +/- Interval debulking (stratified) * Unacceptable Toxicity = is defined as a major adverse event related to chemotherapy or treatment procedures leading either to early treatment stopping, to an unplanned hospital admission or to death.
 GVS>3. Imagery. QOL. Imagery. QOL. +/- Interval debulking (stratified) * Unacceptable Toxicity = is defined as a major adverse event related to chemotherapy or treatment procedures leading either to early treatment stopping, to an unplanned hospital admission or to death.")
12
STATISTICAL CONSIDERATION
Etude ENDOPIK STATISTICAL CONSIDERATION The first step will include 22 patients in each arm (total = 66 patients for the 3 arms); An interim analysis will be conducted when 22 patients in each arm will have completed their 6 courses of chemotherapy: - if a chemotherapy regimen is associated with more than 8/22 treatment failure , the regimen will be considered as having insufficient activity (expected number of failure n= 3) and the regimen will be dropped for the second step of the study; - if a chemotherapy regimen is associated with more than 6/22 major adverse event leading either to early treatment stopping, or to hospitalization for toxicity or to death, the regimen will be considered as having too high toxicity (expected number of major adverse event n= 3) and the regimen will be The second step of the study will be run with the chemotherapy regimens considered as active enough and tolerable at the interim analysis. This step will include an additional 58 patients per arm with the following assumptions: - a risk of accepting a regimen having insufficient activity α1 = 0,05, - a risk of accepting a regimen with too high toxicity α2 = 0,05, - a risk of rejecting regimen active enough (1-β) = 0,1 - with an unacceptable rate of disease progression at 6 month of > 0,4 - and an unacceptable toxicity rate > 0,3. The total number of patients per arm will be of 80 for a maximum total number of patients of 240 if all 3 regimens are selected for step 2. After completion of the 6 chemotherapy cycles, conditions to reject the experimental arms are the following: number of patients with insufficient efficacy n> 26/80 and/or number of patients with unacceptable toxicity n> 18/80 (expected tumour progression or treatment failure: 9, major adverse events: 9).
; An interim analysis will be conducted when 22 patients in each arm will have completed their 6 courses. of chemotherapy: - if a chemotherapy regimen is associated with more than 8/22 treatment failure , the regimen will be. considered as having insufficient activity (expected number of failure n= 3) and the regimen will be. dropped for the second step of the study; - if a chemotherapy regimen is associated with more than 6/22 major adverse event leading either to. early treatment stopping, or to hospitalization for toxicity or to death, the regimen will be considered. as having too high toxicity (expected number of major adverse event n= 3) and the regimen will be. The second step of the study will be run with the chemotherapy regimens considered as active enough. and tolerable at the interim analysis. This step will include an additional 58 patients per arm with the. following assumptions: - a risk of accepting a regimen having insufficient activity α1 = 0,05, - a risk of accepting a regimen with too high toxicity α2 = 0,05, - a risk of rejecting regimen active enough (1-β) = 0,1. - with an unacceptable rate of disease progression at 6 month of > 0,4. - and an unacceptable toxicity rate > 0,3. The total number of patients per arm will be of 80 for a maximum total number of patients of 240 if all. 3 regimens are selected for step 2. After completion of the 6 chemotherapy cycles, conditions to reject the experimental arms are the. following: number of patients with insufficient efficacy n> 26/80 and/or number of patients with. unacceptable toxicity n> 18/80 (expected tumour progression or treatment failure: 9, major adverse. events: 9).")
13
December 2016 – UPDATE

14
December 2016– UPDATE Groups Countries Planned sites Open sites
Active sites Inclusions Randomised Patients MITO Italy 14 5 2 12 6 NSGO Sweden 1 Denmark 4 Finland CHUM- Montréal Canada GINECO France 51 49 39 296 98 TOTAL 73 62 44 312 106

15
ITALIAN SITES Upadate Site Principal Investigator
IRCCS Istituto Nazionale Tumori – Milano Francesco Raspagliesi/ Domenica Lorusso Activated, 11 patients Istituto Nazionale Tumori Pascale - Napoli Sandro Pignata Waiting for contract Policlinico Universitario A. Gemelli - Roma Giovanni Scambia Suspended for institute denomination IRCCS Arcispedale Santa Maria Nuova – Reggio Emilia Alessandra Bologna Refusal by the ethics committee CRO IRCCS - Aviano Roberto Sorio Activated, 0 patients AOU Federico II Sabino De Placido IRE-Istituto Nazionale Tumori REGINA ELENA - Roma Patrizia Vici Fondazione del Piemonte per l'Oncologia - Istituto di Candiolo Giorgio Valabrega Activated. 0 patients U.O.Oncologia Medica - Ospedale Vito Fazzi - Lecce Graziana Ronzino ULLS 13, Mirano - Venezia Grazia Artioli Activated, 5 patients Casa Sollievo della Sofferenza - S.Giovanni Rotondo Francesco Petruzzelli Fondazione IRCCS Policlinico S.Matteo di Pavia Stefano Bogliolo Waiting for emendment Ospedale SS.Trinità - Sora Teresa Gamucci Sumitted AULSS 21 LEGNAGO Filippo Greco Activated, 1 patient Ospedale di Sassuolo Giovanni Partesotti

16
OVAIO RECIDIVA PLATINO RESISTENTE
PLD-Avelumab vs PLD nella recidiva platino resistente di ca ovaio: Definitivamente bocciato da AIFA In arrivo: Pembro nelle resistenti Decitabina nelle resistenti

17
OVAIO RECIDIVA PLATINO SENSIBILE
SOLO 2: chiuso, SGO 2017 ENGOT –OV 27 Farletuzumab in platinum sensitive ovarian cancer with low CA125 MITO 18 Coming soon: ICON 9, OREO

18
BGOG-ov18 Randomized Phase II of chemo +/- Farletuzumab
Carbo PLD x6 + Farletuzumab : Concomittant + maintenance till PD loading dose for the first 2 weeks of 10 mg/kg farletuzumab (double blind), followed by 5 mg/kg weekly First recurrent platin sensitive high grade serous ovarian carcinoma CA125 < 3UNL Evaluable or measurable according to RECIST N = 210 Carbo PLD 2:1 Carbo PLD x6 + Placebo : Concomittant + maintenance Investigator Choice 1:1 Carbo Pacli + Farletuzumab : Concomittant + maintenance till PD loading dose for the first 2 weeks of 10 mg/kg farletuzumab (double blind), followed by 5 mg/kg weekly Carbo Pacli 2:1 Carbo Pacli x6 + Placebo : Concomittant + maintenance FPI: Mar 2015 (US); Aug 2015 (EU) ENGOT Model: C Primary endpoint: PFS * (Assumed HR = 0.667, investigator read) Secondary endpoints: OS, Pt free interval, OR, TTR, DR, safety, PK and exposure-response
, followed by 5 mg/kg weekly. First recurrent platin sensitive high grade serous ovarian carcinoma. CA125 < 3UNL. Evaluable or measurable according to RECIST. N = 210. Carbo PLD. 2:1. Carbo PLD x6 + Placebo : Concomittant + maintenance. Investigator Choice. 1:1. Carbo Pacli + Farletuzumab : Concomittant + maintenance till PD. loading dose for the first 2 weeks of 10 mg/kg farletuzumab (double blind), followed by 5 mg/kg weekly. Carbo Pacli. 2:1. Carbo Pacli x6 + Placebo : Concomittant + maintenance. FPI: Mar 2015 (US); Aug 2015 (EU) ENGOT Model: C. Primary endpoint: PFS * (Assumed HR = 0.667, investigator read) Secondary endpoints: OS, Pt free interval, OR, TTR, DR, safety, PK and exposure-response.")
19
ENGOT ov-27/MORAb-003-011 Site Activation & Enrollment
REGION COUNTRY DATA SITE SELECTION SITES ACTIVATED SUBJECT ENROLLMENT # of countries Name Planned for SIV Opened for Recruiting Screened Randomized NA 1 US 41 80 52 Europe 5 Spain 9 23 18 Belgium 7 15 8 Germany 8* 4 2 Italy 11 24 13 UK 3 Asia-Pacific Japan 16 Total 88 87 166 107 *one site dropped after being selected

20
ENGOT ov-27/MORAb-003-011 Enrollment Summary

21
MITO sites Country Site Name Activated First Screened First Randomized
Status Total Screen Total Scrn Fail Total Rand. Italy 070010 Pignata, Sandro 27-Oct-2015 27-Apr-2016 Active 1 070020 Zamagni, Claudio 21-Dec-2015 22-Dec-2015 30-Dec-2015 4 070030 Scambia, Giovanni 29-Oct-2015 10-Feb-2016 24-Feb-2016 6 2 070040 Savarese, Antonella 11-Mar-2016 22-Apr-2016 30-Jun-2016 070050 Lorusso, Domenica 23-Oct-2015 28-Oct-2016 24-Nov-2016 3 070060 Cicinelli, Ettore 23-Jun-2016 070070 Mosconi, Anna Maria 17-Nov-2015 070080 De Placido, Sabino 26-Feb-2016 1-Jun-2016 2-Jan-2017 070090 Mangili, Giorgia 4-Jan-2016 070100 Gridelli, Cesare 3-Feb-2016 17-Feb-2016 070110 Benedetti Panici, Pierluigi 25-Jan-2016 5-Feb-2016 23-Feb-2016 5 Totals 24 11 13

22
Surgery plus Hyperthermic Intra-PEritoneal Chemotherapy (HIPEC) versus surgery alone in patients with platinum-sensitive first recurrence of ovarian cancer: a prospective randomized multicenter trial. PROTOCOL ID: HORSE Hyperthermic intra-peritoneal chemotherapy (HIPEC) in platinum-sensitive Ovarian cancer recurrence: Randomized trial on Survival Evaluation.
 in platinum-sensitive Ovarian cancer recurrence: Randomized trial on Survival Evaluation.")
23
Patients included (inclusion/exclusion criteria)
LPT: Maximal Surgical Effort Patients eligible (CC-0; CC-1) Patients not eligible (CC>1) Randomization CDDP 75 mg/m2 in 2L/m2 SF temperature 41.5C for 60 min 79 HIPEC NO 79 HIPEC YES Pl based CHT Pl based CHT Drop-out FU FU Drop-out
 Patients not eligible. (CC>1) Randomization. CDDP 75 mg/m2 in 2L/m2 SF. temperature 41.5C for 60 min. 79 HIPEC. NO. 79 HIPEC. YES. Pl based CHT. Pl based CHT. Drop-out. FU. FU. Drop-out.")
24
Status: On going Enrollement 112/158 patients 55 ARM A 57 ARM B

25
Arruolamento per centro
CODICE CENTRO ISTITUTO Principal Investigator Pazienti Arruolate Braccio A Braccio B 001 Policlinico Gemelli-UCSC UO di Ginecologia Oncologica Giovanni Scambia 85 43 42 003 Casa di cura Fondazione Giovanni Paolo II Campobasso Vito Chiantera 4 2 005 A.O. per l'emergenza Cannizzaro SC di Ginecologia ed Ostetricia Paolo Scollo / 006 IEO di Milano Angelo Maggioni 007 IRCCS Arcispedale S. Maria Nuova, Oncologia Medica, Martino Abrate 6 3 029 Centro di Chirurgia Oncologica avanzata c/o Clinica Chirurgica Enricomaria Pasqual 030 Istituto Nazionale Tumori Napoli Stefano Greggi 1 032 Ospedale Sant'Orsola Malpighi -Bologna- Pierandrea De Iaco 12 7 5 038 IRCCS Centro di Riferimento Oncologico CRO Aviano (PN) Giorgio Giorda 046 AUSLL 11 di Empoli Ospedale San Giuseppe Empoli (FI) PI Marco Filippeschi - SOMMA 112 57 55
 Giorgio Giorda AUSLL 11 di Empoli Ospedale San Giuseppe Empoli (FI) PI Marco Filippeschi - SOMMA")
26
OVAIO TUMORI RARI Mito 9 Raccolta retrospettiva su tumori germinali e stromali ovarici MITO 14: chiuso, elaborazione dati in corso Mito 15: sottostudio BACO MITO 21 piccole cellule MITO 22: Studio retrospettivo sui tumori sierosi di basso grado MILO Low grade serous (ENGOT, INT Napoli, chiuso all’interim analisi per futilita’) - Studio Alienor (ENGOT, chiuso)
 - Studio Alienor (ENGOT, chiuso)")
27
Dott.ssa Giorgia Mangili- Alice Bergamini
MITO 9-AGGIORNAMENTO 2017 Dott.ssa Giorgia Mangili- Alice Bergamini

28
MITO9 STROMALI – RETROSPETTIVO
TIPO TUMORE TOT Tumori a cellule della granulosa - Adulto 213 Tumori a cellule della granulosa- Giovanile 19 Tumore Sertoli Leydig 33 Tumori dei cordoni sessuali – tubuli anulari 9 Esclusi 14 Totale complessivo 288

29
MITO 9 – GERMINALI TIPO TUMORE Totale Totale complessivo 250
DISGERMINOMA 90 TERATOMI IMMATURI 77 TUMORI SENO ENDODERMICO 44 MISTI 24 CARCINOMA EMBRIONARIO 1 CARCINOIDE 7 ESCLUSI Totale complessivo 250

30
MITO 9-TUMORI del TROFOBLASTO

31
MITO 14 AGGIORNAMENTO Dott. Enrico Breda

32
Ospedale N° Fatebenefratelli Tiberina (RM) 45
Dipartimento Oncologia Ospedale Mirano (VE) 15 Università Bari Policlinico II (BA) 62 Santa Maria della Misericordia (PG) 8 San Raffaele (MI) 68 Centro Riferimento Oncologico Aviano (UD) 35 Istituto Tumori (MI) 47 Policlinico Gemelli (RM) 201 Azienda Ospedaliera Univ Integrata (VR) 51 Istituto Nazionale Tumori (NA) 67 Campus Biomedico (RM) 18 Mater Salutis ULSS21 Legnago (VR) 20 II Università Napoli (NA) IRCCS Casa sollievo della sofferenza (FG) 13 Ospedale Guastalla (RE) 5 Ospedale Santa Maria Goretti (LT) 27 Ospedali Riuniti (BG) 92 Ospedale di Trento (TN) 39 Ospedale Canizzaro (CT) 40 Ospedale Civile (CZ) 19 Policlinico S. Orsola (BO) 152 INT Regina Elena (RM) Cattedra Oncologica Medica Federico II (NA) 24 III Clinica di Ginecologia e Ostretricia (BA) 1 Arcispedale Santa Maria Nuova (RE) Ospedale S. Giuseppe USL 11 Toscana Ospedale Faenza 6 Vici INT Regina Elena B (RM) Ospedale Civile Boldrini Thiene (VI) 34 SCDU Ginecologia e Ostetricia Ospedale Mauriziano (TO) 81 Università La Sapienza (RM) 44 1359
 15. Università Bari Policlinico II (BA) 62. Santa Maria della Misericordia (PG) 8. San Raffaele (MI) 68. Centro Riferimento Oncologico Aviano (UD) 35. Istituto Tumori (MI) 47. Policlinico Gemelli (RM) 201. Azienda Ospedaliera Univ Integrata (VR) 51. Istituto Nazionale Tumori (NA) 67. Campus Biomedico (RM) 18. Mater Salutis ULSS21 Legnago (VR) 20. II Università Napoli (NA) IRCCS Casa sollievo della sofferenza (FG) 13. Ospedale Guastalla (RE) 5. Ospedale Santa Maria Goretti (LT) 27. Ospedali Riuniti (BG) 92. Ospedale di Trento (TN) 39. Ospedale Canizzaro (CT) 40. Ospedale Civile (CZ) 19. Policlinico S. Orsola (BO) 152. INT Regina Elena (RM) Cattedra Oncologica Medica Federico II (NA) 24. III Clinica di Ginecologia e Ostretricia (BA) 1. Arcispedale Santa Maria Nuova (RE) Ospedale S. Giuseppe USL 11 Toscana. Ospedale Faenza. 6. Vici INT Regina Elena B (RM) Ospedale Civile Boldrini Thiene (VI) 34. SCDU Ginecologia e Ostetricia Ospedale Mauriziano (TO) 81. Università La Sapienza (RM)")
33
Age 51 (14-103) Microinvasion 79/1259 (6.2%) Micropapillary type 17/1259 (1.3%) Implants 33/1259 (2.6%) Invasive implants 4/1259 (0.3%)
")
35
BRCA mutations IN OVARIAN CANCER TUMOUR TISSUE
‘BACO’ study BRCA mutations IN OVARIAN CANCER TUMOUR TISSUE A MITO-15 retrospective evaluation Primary objective To assess BRCA somatic mutations as independent predictors of treatment response to trabectidin in Advanced Ovarian Cancer (AOC) Secondary objectives To assess BRCA mutations as independent predictor of survival Prevalence of BRCA somatic mutations in BRCA germline negative and patients with unknown BRCA status
 Secondary objectives. To assess BRCA mutations as independent predictor of survival. Prevalence of BRCA somatic mutations in BRCA germline negative and patients with unknown BRCA status.")
36
In MITO 15 study: planned to study BRCA 1 and 2 gene in formalin-fixed paraffin embedded tumor tissues obtained from OC patients. A specific informed consent for translational studies has been collected at time of enrollment Due to financial and operational constraints, this sub-study were not carried on as planned. Given the availability of Tumor BRACAnalysis CDx, a full somatic BRCA 1 and 2 sequencing by Myriad Genetics GmBH using Next Generation Sequencing (NGS), MITO 15 study committee agreed to ask Myriad Genetics to support analysis of sporadic BRCA1 or BRCA2 mutations in archived tumor tissues. This study is aimed to retrospectively estimate to what extent BRCA mutations found in paraffin embedded tumor samples are associated with trabectidin response in patients enrolled into MITO 15 study
, MITO 15 study committee agreed to ask Myriad Genetics to support analysis of sporadic BRCA1 or BRCA2 mutations in archived tumor tissues. This study is aimed to retrospectively estimate to what extent BRCA mutations found in paraffin embedded tumor samples are associated with trabectidin response in patients enrolled into MITO 15 study.")
37
CENTRO 002 RASPAGLESI - MILANO
CENTRI Blocchetti tissutali disponibili status CENTRO 001 SCAMBIA - ROMA 12 pronti CENTRO 002 RASPAGLESI - MILANO 17 Attesa CE CENTRO 011 MOSCONI - PERUGIA 7 CENTRO 013 SABBATINI - MODENA 5 CENTRO 021 ARTIOLI - MIRANO 3 CENTRO 030 PIGNATA - NAPOLI 16 CENTRO 039 SORIO - AVIANO 8

38
MITO 21: STUDIO OSSERVAZIONALE SUL TRATTAMENTO DEI TUMORI A PICCOLE CELLULE DELL’APPARATO GENITALE

39
Criteri di inclusione sesso femminile, senza limiti di età
diagnosi di tumore a piccole cellule del tratto genitale femminile (carcinoma a piccole cellule della cervice, dell’utero, dell’ovaio, della vagina e della vulva, tumori dell’utero PNET, tumore desmoplastico a piccole cellule dell’utero) disponibilità (ove applicabile) a fornire il consenso informato al trattamento dei dati personali disponibilità (ove applicabile) a fornire i preparati allestiti dell’esame istologico per la revisione centralizzata
 disponibilità (ove applicabile) a fornire il consenso informato al trattamento dei dati personali. disponibilità (ove applicabile) a fornire i preparati allestiti dell’esame istologico per la revisione centralizzata.")
40
Procedure di raccolta dati
Compilato Database Richiesta per alcuni centri invio vetrini per revisione centralizzata. Arruolamento per centro (Dicembre 2017) Centro Principal Investigator Codice centro Pazienti inserite Policlinico A. Gemelli Roma Giovanni Scambia 1 25 INT MILANO Raspagliesi 2 San Raffaele Milano Giorgia Mangili 14 10 Dipartimento di Oncologia Medica B, Istituto Nazionale Tumori Regina Elena Roma Patrizia Vici 49 4 Di. Ginecologia, Ostetricia, Neonatologia Policlinico Bari Gennaro Cormio 20 8 III U.O. Ginecologia e Ostetricia, Policlinico di Bari Marco Marinaccio 27 Istituto Nazionale Tumori Napoli Sandro Pignata 30 7 Dip. Di Ostetricia e Ginecologia IRCCS Policlinico San Matteo Pavia Stefano Bogliolo 50 IRST- Istituto Scientifico Romagnolo per lo studio e la cura dei tumori -ONCOLOGIA MEDICA Ugo De Giorgi 19 totale 82/100
 Centro. Principal Investigator. Codice centro. Pazienti inserite. Policlinico A. Gemelli Roma. Giovanni Scambia INT MILANO. Raspagliesi. 2. San Raffaele Milano. Giorgia Mangili Dipartimento di Oncologia Medica B, Istituto Nazionale Tumori Regina Elena Roma. Patrizia Vici Di. Ginecologia, Ostetricia, Neonatologia Policlinico Bari. Gennaro Cormio III U.O. Ginecologia e Ostetricia, Policlinico di Bari. Marco Marinaccio. 27. Istituto Nazionale Tumori Napoli. Sandro Pignata Dip. Di Ostetricia e Ginecologia IRCCS Policlinico San Matteo Pavia. Stefano Bogliolo. 50. IRST- Istituto Scientifico Romagnolo per lo studio e la cura dei tumori -ONCOLOGIA MEDICA. Ugo De Giorgi. 19. totale. 82/100.")
41
Mito 22: LOW GRADE SEROUS criteri di inclusione
LGSOC/Recidiva Invasiva di SBLT operato Diagnosi posta tra e il Preparato istologico per revisione centralizzata Età > 18 aa EMENDARE?? …SI POTREBBE SPOSTARE IL TERMINE DELLA DATA DIAGNOSI ALL’ INT Napoli Ist Regina Elena CRO Aviano Pol Univ A. Gemelli Roma

42
Mito 22: obiettivi endpoint primari endpoint secondari
Rischio di recidiva in pazienti operate RR a CHT, OT e terapia combinata in I linea e in linee successive endpoint secondari PFS, OS Profilo di tossicità KRAS, BRAF, p53 correlazione tra mutazione di BRAF e outcome favorevole??? Grisham, BRAF mutation is associated with early stage disease and improved outcome in patients with low-grade serous ovarian cancer, Cancer 2013; 1;119(3): Wong, BRAF mutation is rare in advanced-stage low-grade ovarian serous carcinomas, Am J Pathol, 2010; 177(4):1611-7
: Wong, BRAF mutation is rare in advanced-stage low-grade ovarian serous carcinomas, Am J Pathol, 2010; 177(4):")
43
Informazioni operative (1)
")
44
Informazioni operative (2)
")
45
Avastin and weekly pacLItaxel use in sEx cord-stromal ovariaN tumORs
ALIENOR ENGOT- OV7 Avastin and weekly pacLItaxel use in sEx cord-stromal ovariaN tumORs A randomized, open label, phase II trial of bevacizumab plus weekly paclitaxel followed by maintenance with bevacizumab monotherapy versus weekly paclitaxel followed by observation in patients with relapsed ovarian sex-cord stromal tumors

46
Standard surveillance
STUDY DESIGN Bevacizumab 15mg/Kg every 3 weeks Paclitaxel alone 80mg/m², IV, at D1, D8 and D15 every 4 weeks Paclitaxel 80mg/m², IV, D1, D8 and D15 every 4 weeks + 10mg/kg, IV, D1 and D15 RANDOMISATION Maximum of 6 cycles Up to 1 year or until PD / intolerance Arm A Arm B Standard surveillance Standard of care PD or Toxicity At the investigator discretion Population : Patients with an histologically confirmed diagnosis of ovarian sex-cord stromal tumor in relapse after a platinum-based chemotherapy. Stratification Anterior chemotherapy lines : 1 or 2 vs 3 and more Platinum Free Interval Interval (PFI) <12 months vs >12 months Primary objective : Clinical benefit rate (non-progression rate after 6 months of treatment) GCIG Meeting-Melbourne 2014
 <12 months vs >12 months. Primary objective : Clinical benefit rate. (non-progression rate after 6 months of treatment) GCIG Meeting-Melbourne")
47
GCIG Meeting-Melbourne 2014
PRIMARY OBJECTIVE To evaluate the clinical benefit of combining bevacizumab long-term treatment to weekly paclitaxel measured by the non progression rate after 6 months of treatment SECONDARY OBJECTIVES To evaluate in the 2 study arms: The Progression-Free survival The Overall Survival The duration of response The Quality of Life (FACTO); To describe the safety profile of the association Paclitaxel plus Bevacizumab using the NCI- CTC AE scale version 4.0; To evaluate the benefit of Bevacizumab alone after re progression in the arm A GCIG Meeting-Melbourne 2014
; To describe the safety profile of the association Paclitaxel plus Bevacizumab using the NCI- CTC AE scale version 4.0; To evaluate the benefit of Bevacizumab alone after re progression in the arm A. GCIG Meeting-Melbourne")
48
ALIENOR STUDY – UPDATE December 2016
Enrollment period : 36 months First Patient In : February 2013 Treatment + maintenance : 18 months Last Patient Out of Maintenance : August 2017 Follow-up : 36 months Last Patient Out : August 2020

49
UPDATE - December 2016 TOTAL 48 41 28 88 60 GROUPS Countries
Planned sites Open sites Active sites Planned Recruitment Randomised Patients AGO Germany 8 7 4 20 10 BGOG Belgium 2 9 GINECO France 23 18 40 38 GOTIC Japon 5 1 MITO Italy 3 TOTAL 48 41 28 88 60

50
ITALIAN SITES SITE Principal Investigator Status N patients
Istituto Nazionale Tumori – Milano – Coordinating center Francesco Raspagliesi/ Domenica Lorusso Active 4 Policlinico Agostino Gemelli - Roma Giovanni Scambia Not active Istituto Tumori Pascale - Napoli Sandro Pignata 3 Ospedale San Raffaele - Milano Giorgia Mangili Avtive 1 IRST di Meldola Ugo De Giorgi IRE-Istituto Nazionale Tumori REGINA ELENA - Roma Patrizia Vici Ospedale Vito Fazzi - Lecce Graziana Ronzino Fondazione del Piemonte per l'Oncologia - Istituto di Candiolo Giorgio Valabrega Ospedale SS. Trinità - Sora Teresa Gamucci Arcispedale sant’Anna - Cona, Ferrara Antonio Frassoldati

51
CARCINOMA DELL’ENDOMETRIO
Trattamento conservativo : ECCO study (S. Greggi) ENGOT EN2-EORTC (Coordinamento italiano: Dr Greggi) A phase III trial of postoperative chemotherapy or no further treatment for patients with node negative stage I-II intermediate or high risk endometrial cancer. PALEO study: A randomized phase II trial of Palbociclib in combination with letrozole versus letrozole for patients with oestrogen receptor positive recurrent endometrial cancer.
 ENGOT EN2-EORTC (Coordinamento italiano: Dr Greggi) A phase III trial of postoperative chemotherapy or no further treatment for patients with node negative stage I-II intermediate or high risk endometrial cancer. PALEO study: A randomized phase II trial of Palbociclib in combination with letrozole versus letrozole for patients with oestrogen receptor positive recurrent endometrial cancer.")
52
Seconda relazione di avanzamento Gennaio 2017

53
Project Project Type / Design & Time Perspective
E.C.Co. Endometrial Cancer Conservative treatment A multicentre archive Project Project Type / Design & Time Perspective Observational / Patient archive, Prospective (a first phase of three years is planned, eventually followed by further three years) Inclusion Criteria - Conservatively treated endometrial cancer - Informed consent to personal data processing - Existence of an IRB-approved local protocol that allows conservative treatment to be performed (or statement that such treatment is considered as a standard) Interventions & Outcome Measures Data collection - Primary Outcome Measures: proportion of complete regression, duration of response, frequency and pattern of relapse, frequency of metachronous ovarian cancer, tumor-related deaths; Secondary Outcome Measures: treatment related morbidity, frequency of spontaneous pregnancies, frequency of pregnancies after ART, pattern of residual disease on definitive surgical specimens Treatment Since this is a archive, treatment is not dictated by a protocol, however, treatment has to be administered according to a IRB-approved local protocol (except for the countries where conservative treatment can be given outside a IRB-approved study because considered as a standard procedure)
 Inclusion Criteria. - Conservatively treated endometrial cancer. - Informed consent to personal data processing. - Existence of an IRB-approved local protocol that allows conservative treatment to be performed (or statement that such treatment is considered as a standard) Interventions & Outcome Measures. Data collection - Primary Outcome Measures: proportion of complete regression, duration of response, frequency and pattern of relapse, frequency of metachronous ovarian cancer, tumor-related deaths; Secondary Outcome Measures: treatment related morbidity, frequency of spontaneous pregnancies, frequency of pregnancies after ART, pattern of residual disease on definitive surgical specimens. Treatment. Since this is a archive, treatment is not dictated by a protocol, however, treatment has to be administered according to a IRB-approved local protocol (except for the countries where conservative treatment can be given outside a IRB-approved study because considered as a standard procedure)")
54
s.greggi@istitutotumori.na.it – ginecologia@istitutotumori.na.it
E.C.Co. Endometrial Cancer Conservative treatment A multicentre archive Participation (10/06/2016) 6 Data collection is made by appropriate eCRFs via the Clinical Trials Unit of National Cancer Institute of Naples (Study Data Center) website –
 6. Data collection is made by appropriate eCRFs via the Clinical Trials Unit of National Cancer Institute of Naples (Study Data Center) website. –")
55
138/678

56
ENGOT-EN2-DGCG EORTC55102

57
ENGOT-EN2-DGCG EORTC55102

58
MITO Centers – Italy In corso emendamento per diventare phase II EORTC chiede per il momento di non allargare le adesioni prima che i siti già individuati siano aperti e attivi Avvenuto ciò, sarà fatto un emendamento ad hoc per i nuovi siti richiedenti

59
ENGOT-ENxx - NSGO / PALEO Study Design
Randomization: 1:1 N=80 (0) Endometrial Cancer Primary stage 4 or relapsed incurable disease ER positive endometrioid adenocarcinoma ARM A Letrozole, 2.5mg d 1-28 every 28 days Until progression Randomize ARM B Letrozole, 2.5mg d 1-28 every 28 days Palbociclib 125mg d 1-21 every 28 days Until progression Stratification: Number of prior lines of therapy (0 vs. 1 vs. more than one) Disease status RECIST 1.1 (measurable disease vs. evaluable disease only) Prior MPA/Megace
 Endometrial Cancer. Primary stage 4 or relapsed incurable disease. ER positive endometrioid adenocarcinoma. ARM A. Letrozole, 2.5mg d 1-28 every 28 days. Until progression. Randomize. ARM B. Letrozole, 2.5mg d 1-28 every 28 days. Palbociclib 125mg d 1-21 every 28 days. Until progression. Stratification: Number of prior lines of therapy (0 vs. 1 vs. more than one) Disease status RECIST 1.1 (measurable disease vs. evaluable disease only) Prior MPA/Megace.")
60
ENGOT-ENxx - NSGO / PALEO
Study Population Histological confirmed endometrial cancer of endometrioid type. Mixed tumor histology is allowed if the non-endometrioid component is less than 5%. Tumour must be oestrogen receptor positive. Prior therapy Patients may have received chemotherapy for primary advanced (stage 3-4) or relapsed disease, though maximum one-line of therapy. Patients may have received adjuvant chemotherapy for stage 1 or 2. Patients may have received external beam radiotherapy, brachytherapy, surgery. Max one line of prior endocrine therapy with MPA/Megace is permitted. Disease status 7. Patients must have measureable disease or non measurable disease on CT scan according to RECIST 1.1 outside irradiated field. ENGOT-ENxx - NSGO / PALEO
 or relapsed disease, though maximum one-line of therapy. Patients may have received adjuvant chemotherapy for stage 1 or 2. Patients may have received external beam radiotherapy, brachytherapy, surgery. Max one line of prior endocrine therapy with MPA/Megace is permitted. Disease status 7. Patients must have measureable disease or non measurable disease on CT scan according to RECIST 1.1 outside irradiated field. ENGOT-ENxx - NSGO / PALEO.")
61
ENGOT-ENxx - NSGO / PALEO
Study Endpoints Primary: Investigator-assessed progression-free survival (PFS) Secondary: Investigator-assessed PFS in the sub-populations as in stratification factors. Overall Survival (OS) Objective response rate according to RECIST (ORR) Disease Control Rate (CR+PR+SD) Progression-Free Survival 2 (PFS2): Time to second subsequent therapy (TSST) Patient Reported Outcomes (PROs) (e.g. QoL) Safety and tolerability in the two treatment arms Compliance in the two treatment arms. Time to subsequent therapy ENGOT-ENxx - NSGO / PALEO
 Secondary: Investigator-assessed PFS in the sub-populations as in stratification factors. Overall Survival (OS) Objective response rate according to RECIST (ORR) Disease Control Rate (CR+PR+SD) Progression-Free Survival 2 (PFS2): Time to second subsequent therapy (TSST) Patient Reported Outcomes (PROs) (e.g. QoL) Safety and tolerability in the two treatment arms. Compliance in the two treatment arms. Time to subsequent therapy. ENGOT-ENxx - NSGO / PALEO.")
62
Statistical Assumptions ENGOT-ENxx - NSGO / PALEO
Design Parameters: Type 1 error (1-sided) % Statistical power 80% Randomization 1:1 Interim analysis none Hazard Ratio No. of PFS events required 64 Accrual 80 ENGOT-ENxx - NSGO / PALEO
 12.5% Statistical power 80% Randomization 1:1. Interim analysis none. Hazard Ratio No. of PFS events required 64. Accrual 80. ENGOT-ENxx - NSGO / PALEO.")
63
A randomized phase II trial of Palbociclib in combination with letrozole versus letrozole for patients with oestrogen receptor positive recurrent endometrial cancer. ENGOT-EN3-NSGO/PALEO Study Status MITO coordinator centre Policlinico Gemelli (sottomissione etica Marzo 2017) Adjuvant Endometrial Cancer Trial - Mirza
 Adjuvant Endometrial Cancer Trial - Mirza.")
64
CARCINOMA DELLA CERVICE UTERINA
BGOG-CX1 Nintedanib in cervical cancer: Coordinato da INT-Napoli

65
BGOG-cx1: Basic Trial Design
Patients (# 120) with histologically or cytologically confirmed squamous, adenosquamous or adenocarcinoma of the cervix Advanced stage (FIGO stage IVB) OR Recurrent/persistent disease 1:1 Randomization IXRS Nintedanib 200 mg p.o. BID PLUS Paclitaxel 175 mg/m2 + carboplatin AUC5 Every 21 days for 6 cycles Nintedanib monotherapy up to 120 weeks Placebo p.o. BID Placebo monotherapy up to 120 weeks
 with histologically or cytologically confirmed squamous, adenosquamous or adenocarcinoma of the cervix. Advanced stage (FIGO stage IVB) OR Recurrent/persistent disease. 1:1 Randomization IXRS. Nintedanib 200 mg p.o. BID. PLUS. Paclitaxel 175 mg/m2 + carboplatin AUC5. Every 21 days for 6 cycles. Nintedanib monotherapy up to 120 weeks. Placebo p.o. BID. Placebo monotherapy up to 120 weeks.")
66
BGOG-cx1: Rationale and objectives
Dominant role of angiogenesis related to HPV inhibition of p53 and stabilization of HIF-1 alfa → increase of VEGF. Previous studies confirmed activity of anti-angiogenesis agents in advanced and recurrent cervical cancer. Objectives Primary: Progression free survival (RECIST 1.1) Secondary: Toxicity and safety Response rate and overall survival Patient reported health status (QOL-CX24 and QOQ-C30)
 Secondary: Toxicity and safety. Response rate and overall survival. Patient reported health status (QOL-CX24 and QOQ-C30)")
67
BGOG-cx1: Cumulative enrollment graph
1st site to open Italy

68
Protocol amendment Protocol v5.0 :
Approved in Belgium/EC approval in Germany – pending CA approval/to be submitted in Spain (Jan 2017) – to be submitted in Italy April 2017 Allow prior treatment with angiogenesis inhibitors Allow one prior line of chemotherapy for metastatic cervical cancer Allow inclusion for patients with recurrence within 6 months after last therapy.
 – to be submitted in Italy April Allow prior treatment with angiogenesis inhibitors. Allow one prior line of chemotherapy for metastatic cervical cancer. Allow inclusion for patients with recurrence within 6 months after last therapy.")
Presentazioni simili
>")









 vs clinician’s choice chemotherapy in recurrent ovarian, primary peritoneal or fallopian tube cancers.>")

 5 I Clinica Ostetrica Ginecologica Bari (ex Bari II) – Cormio.>")






 in ognuna delle prime 2 liste verranno eletti i 3 candidati che avranno ottenuto il maggior numero di voti.>")