Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
RUSSAMENTO E OSAS (SNORING AND OSAS)
")
2
Obstructive Sleep Apnea Syndrome
O. S. A. S Obstructive Sleep Apnea Syndrome

3
O.S.A.S Sindrome caratterizzata da: russamento
episodi apnoici durante il sonno

4
OSAS Base della patologia è l’apnea che si caratterizza per un interruzione dell’attività respiratoria nasale ed orale per almeno 10 secondi e persistenza dei movimenti toracici ed addominali per vincere l’ostruzione (apnea ostruttiva) Se vi è abolizione dei movimenti toracici si parla di apnea centrale Le apnee costituiscono il sintomo cardine, insieme alle ipopnee, della sindrome delle apnee ostruttive o sindrome OSAS
 Se vi è abolizione dei movimenti toracici si parla di apnea centrale. Le apnee costituiscono il sintomo cardine, insieme alle ipopnee, della sindrome delle apnee ostruttive o sindrome OSAS.")
5
eziopatogenesi Apnea centrale:
disfunzione dei centri del respiro a livello del SNC, con abolizione dei movimenti toraco-addominali e quindi del flusso aereo ( rara ) Apnea ostruttiva periferica: collasso delle vie aeree superiori di varia natura, con persistenza dei movimenti toraco-addominali Apnee di tipo misto periferico-centrale
 Apnea ostruttiva periferica: collasso delle vie aeree superiori di varia natura, con persistenza dei movimenti toraco-addominali. Apnee di tipo misto periferico-centrale.")
6
RUSSAMENTO Rumore che si produce durante il sonno a causa delle vibrazione di parti molli delle prime vie aeree Non si realizza un’ostruzione completa È un disturbo di tipo “sociale” (partner) Non ha effetti secondari immediati sull’apparato cardiocircolatorio È spia di un decadimento anatomico e funzionale delle prime vie aree che può esitare nell’OSAS
 Non ha effetti secondari immediati sull’apparato cardiocircolatorio. È spia di un decadimento anatomico e funzionale delle prime vie aree che può esitare nell’OSAS.")
7
Apnea – cessation of airflow >10 sec, ends in arousal
Definizione Apnea – cessation of airflow >10 sec, ends in arousal Hypopnea – reduction in airflow with desaturation, ends in arousal Apnea / Hypopnea Index (Respiratory Disturbance Index)
")
8
Definizione di OSAS RDI 10<20 = mild
RDI > 20 increases risk of mortality RDI =moderate RDI >40 =severe Upper Airway Resistance Syndrome (UARS) Shares pathophysiology with OSA No desaturation, continuous ventilatory effort Snoring
 Shares pathophysiology with OSA. No desaturation, continuous ventilatory effort. Snoring.")
9
Apnea ostruttiva periferica fattori predisponenti
obesità stenosi nasale: deviazione del setto polipi nasali ipertrofia dei turbinati ipertrofia adenoidea ostruzioni faringee: ipetrofia tonsillare mega-ugola

12
apnea ostruttiva periferica stadiazione
Stadio 0: forti russatori con sporadiche apnee notturne Stadio 1: forti russatori con apnee ma solo in posizione supina Stadio 2:forti russatori con frequentissime apnee anche dormendo sul fianco Stadio 3: pz. scompensati ipoventilati anche in veglia con gravi apnee notturne

13
apnea ostruttiva periferica conseguenze
ipersonnia diurna cefalea faringodinia mattutina insufficienza respiratoria cuore polmonare > patologie cardio-circolatorie > patologie vasculo-cerebrali > incidenti automobilistici !!!!!!!!!!!!!

14
Obstructive Sleep Apnea
1-4% of population Pickwick Papers (1837) Osler (1906) Guilleminault (1973) - OSAS
 Osler (1906) Guilleminault (1973) - OSAS.")
15
(da Guilleminault nel 1973)
O.S.A.S Studiata e descritta in modo scientifico solo di recente (da Guilleminault nel 1973)
")
16
Epidemiologia 85% dei pazienti adulti sono di sesso maschile
2% delle donne oltre i 40 anni 4% degli uomini oltre i 40 anni circa 2\3 dei pz è obeso l’incidenza dell’OSAS aumenta con l’età

17
Physiology of Sleep REM Sleep Latency, REM Latency Arousal
Woodson, Tucker “Obstructive Sleep Apnea Syndrome, Diagnosis and Treatment” SIPAC 1996 REM Sleep Latency, REM Latency Arousal

18
Pathophysiology of OSA
Airway size:

19
Pathophysiology of OSA
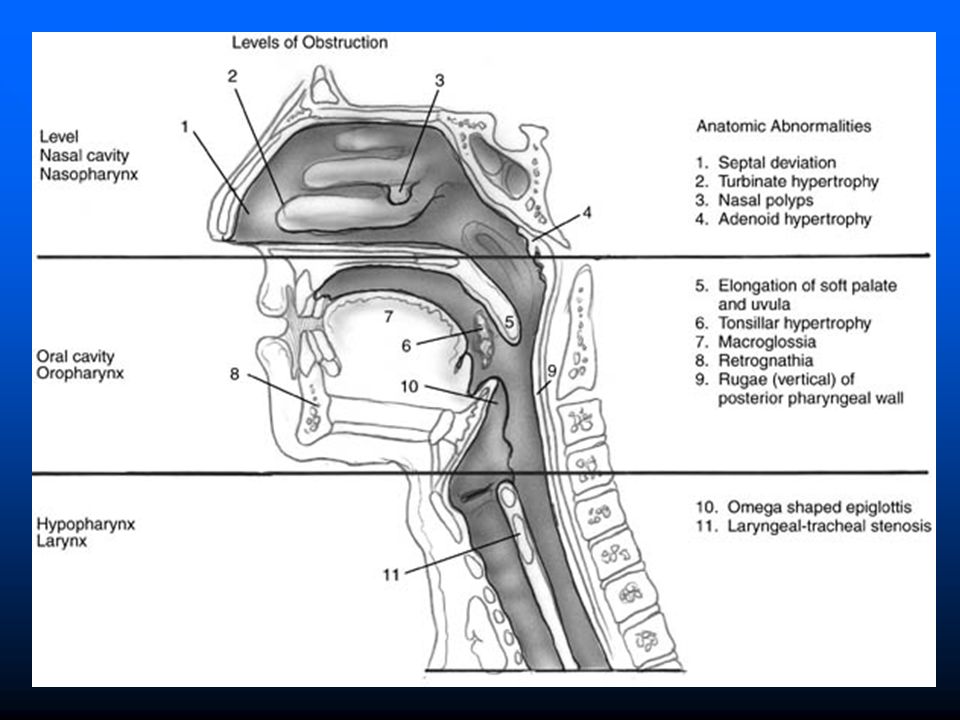
Sites of Obstruction: Obstruction tends to propagate

20
Pathophysiology of OSA
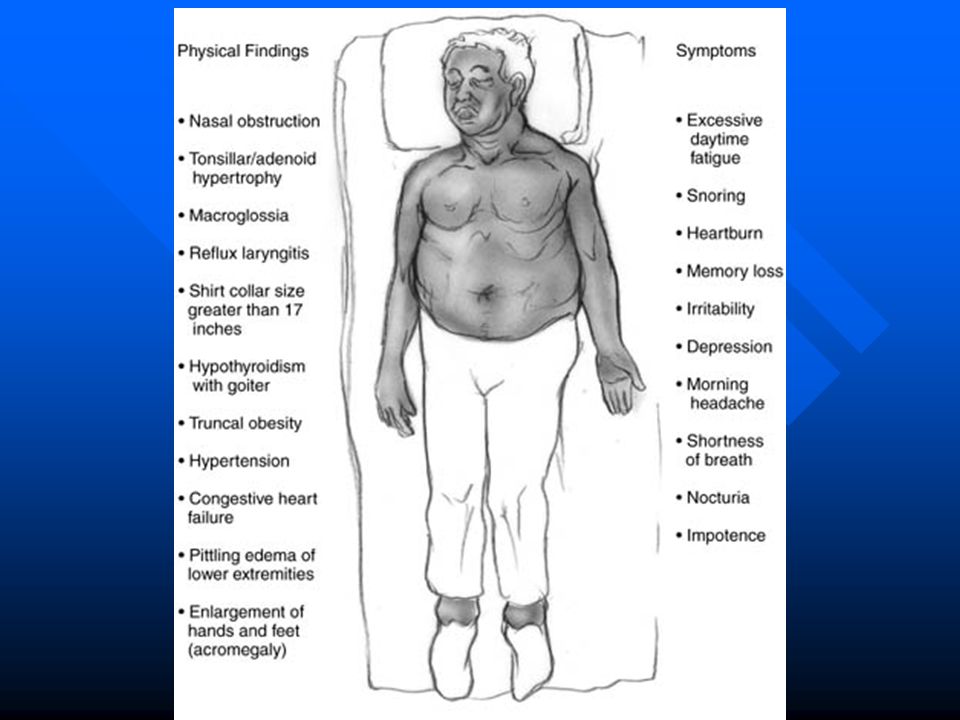
Findings in Obstruction: Nasal Obstruction Long, thick soft palate Retrodisplaced Mandible Narrowed oropharynx Redundant pharyngeal tissues Large lingual tonsil Large tongue Large or floppy Epiglottis Retro-displaced hyoid complex

21
Pathophysiology of OSA
Sites of Obstruction:

22
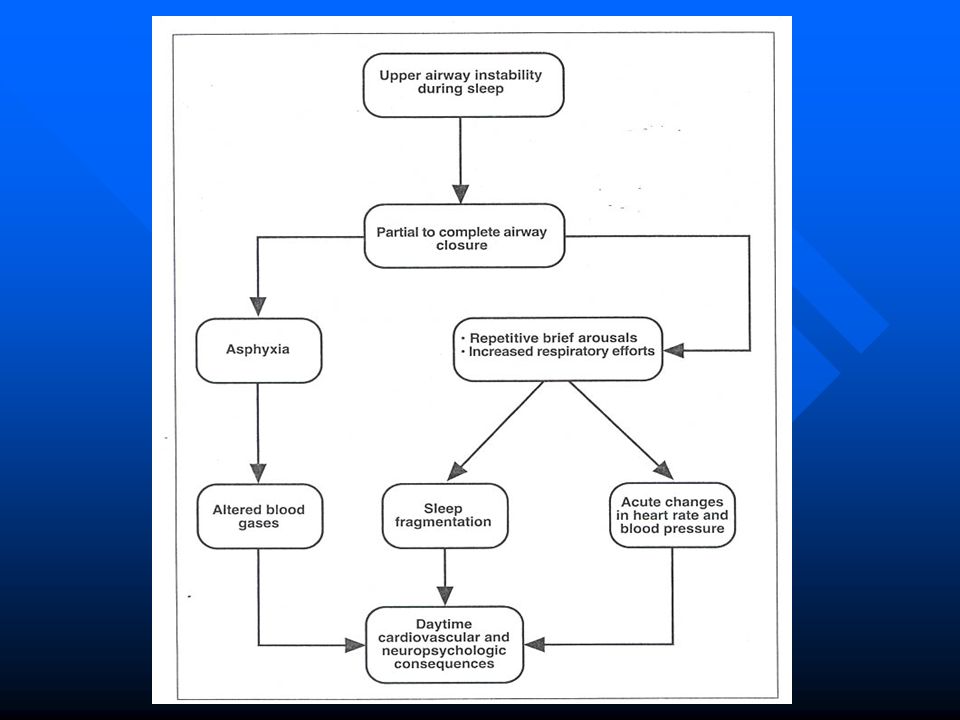
Pathophysiology Pharyngeal collapse Decreased airway patency
Increase in negative pressure Becomes a vicious cycle

23
Pathophysiology Anatomic narrowing Abnormal neuromuscular control
Requires increased inspiratory pressures Abnormal neuromuscular control Reflex activation of dilators in response to airway obstruction often fails

25
Risk factors Obesity (BMI > 30) Drunkenness Smoking ORN
Hormonic depletion (estrogeni)
")
26
Tests to determine site of obstruction:
Muller’s Maneuver Sleep endoscopy Fluoroscopy Manometry Cephalometrics Dynamic CT scanning and MRI scanning

27
Apnea ostruttiva periferica diagnosi
anamnesi e visita ORL tradizionale valutazione endoscopica delle VADS test di Muller ossimetria transcutanea polisonnografia rinomanometria posizionale tests allergici studio del reflusso gastro-esofageo valutazione neurologica e pneumologica

28
History Snoring* Excessive daytime sleepiness* Restless sleep
Personality changes Headaches Sexual dysfunction Job performance Sleep hygiene Bed partner’s input *

29
Physical Exam Vital signs Head & Neck exam Flexible endoscopy

30
Vital signs Height Weight Collar size Blood pressure Calculate BMI
Wt (kg) / Ht (meters) squared Men >27.8, Women >27.3
 / Ht (meters) squared. Men >27.8, Women >27.3.")
31
Examination Tongue Palate Uvula Tonsils Nasal cavity Hyoid Mandible
Maxilla

33
Classificazione di Mallampati

34
MALLAMPATI MODIFICATA
. Lo score viene calcolato osservando il piano del dorso linguale e il profilo del palato molle a bocca aperta e con la lingua adagiata sul pavimento orale e se ne identificano quattro gradi (vedi figura): o grado I: tonsille, pilastri e palato molle chiaramente visibili o grado II: ugola, pilastri e polo tonsillare superiore visibili o grado III: visibile solo parte del palato molle grado IV: palato molle non visibile, visibile solo il palato duro La classificazione di Mallampati permette una immediata quantificazione del volume linguale e può essere un utile indice di ostruzione faringea; è stata infatti dimostrata una stretta correlazione tra questo indice e la gravità della sindrome OSA. Anche il volume tonsillare è considerato un importante fattore predittivo sia della presenza dell’OSAS che della sua severità ed è stato individuato come fattore predittivo del successo chirurgico in diversi studi.L’ipertrofia tonsillare viene valutata tramite una classificazione che prevede cinque gradi
: o grado I: tonsille, pilastri e palato molle chiaramente visibili. o grado II: ugola, pilastri e polo tonsillare superiore visibili. o grado III: visibile solo parte del palato molle. grado IV: palato molle non visibile, visibile solo il palato duro. La classificazione di Mallampati permette una immediata quantificazione del volume linguale e può essere un utile indice di ostruzione faringea; è stata infatti dimostrata una stretta correlazione tra questo indice e la gravità della sindrome OSA. Anche il volume tonsillare è considerato un importante fattore predittivo sia della presenza dell’OSAS che della sua severità ed è stato individuato come fattore predittivo del successo chirurgico in diversi studi.L’ipertrofia tonsillare viene valutata tramite una classificazione che prevede cinque gradi.")
35
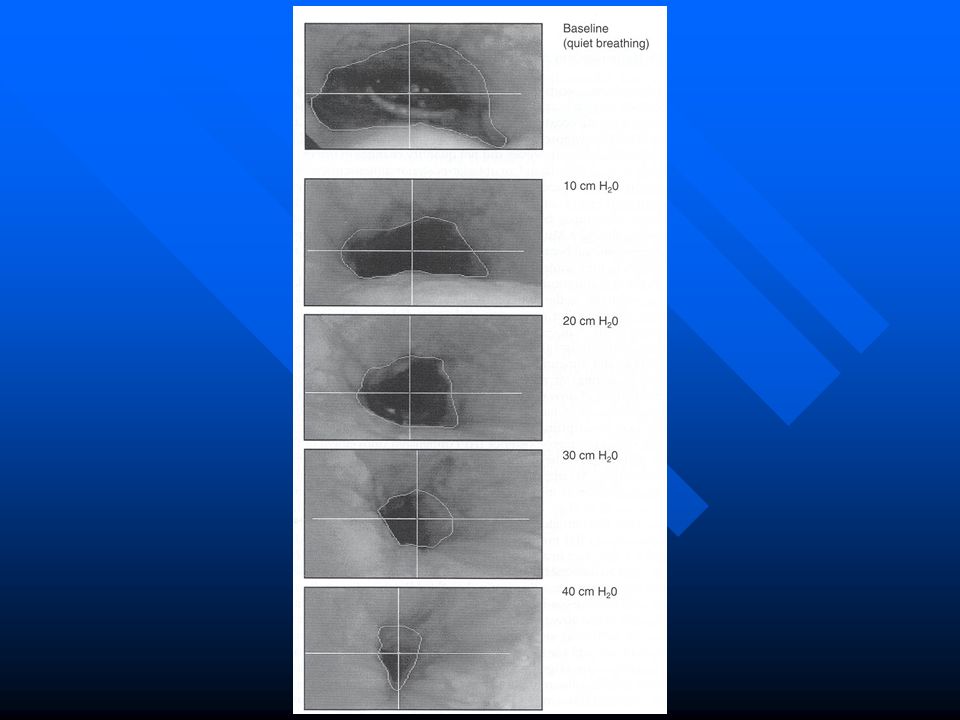
Test di Muller

36
Hypo-pharynx collapse
Test di Muller BOT collapse Hypo-pharynx collapse

38
Esame obiettivo

39
Tests Radiologici Cephalometrics Computed tomography
Magnetic resonance imaging

40
Cephalometrics Standardized lateral radiographs
Examines bony and soft-tissue structure Two-dimensional evaluation Lack of volumetric data Maxillomandibular surgery, oral appliances

41
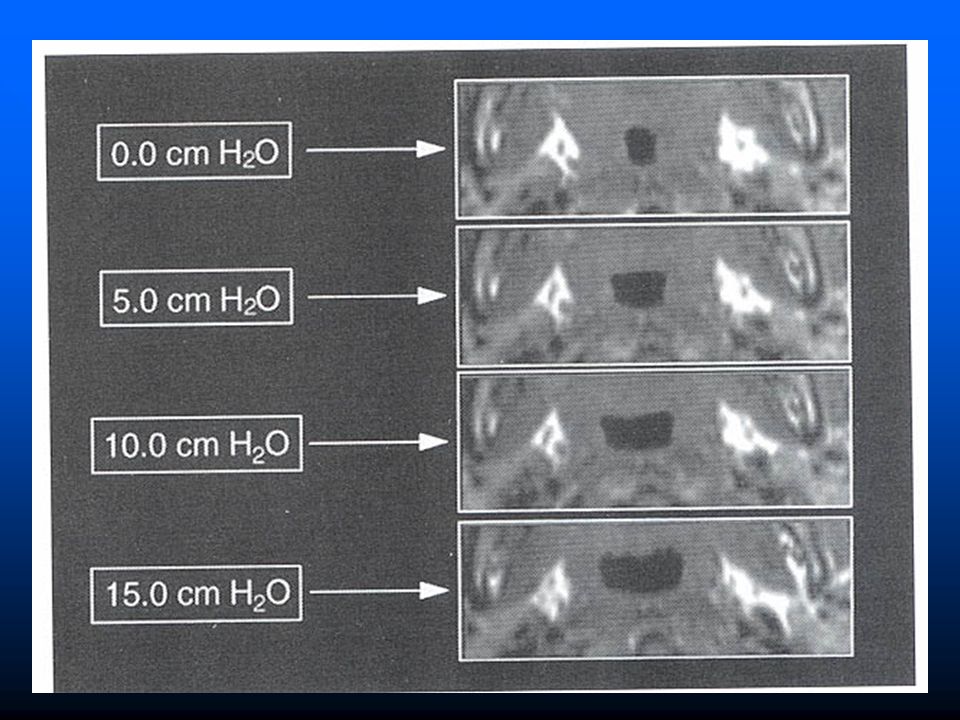
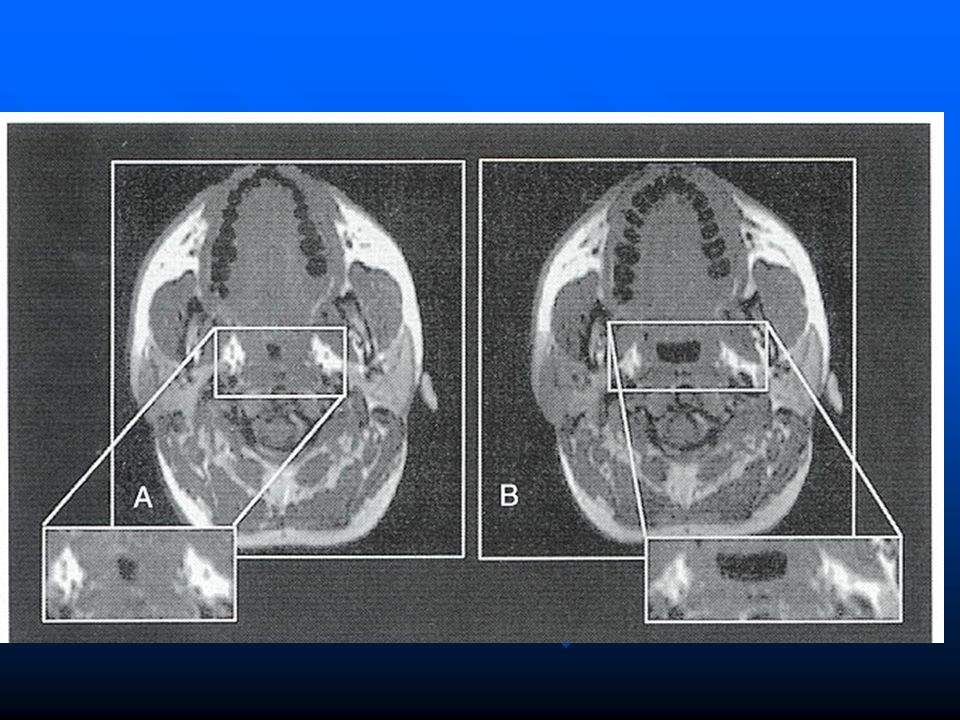
Computed tomography Supine Volumetric reconstruction Disadvantages
Cost Weight limitations Ionizing radiation

42
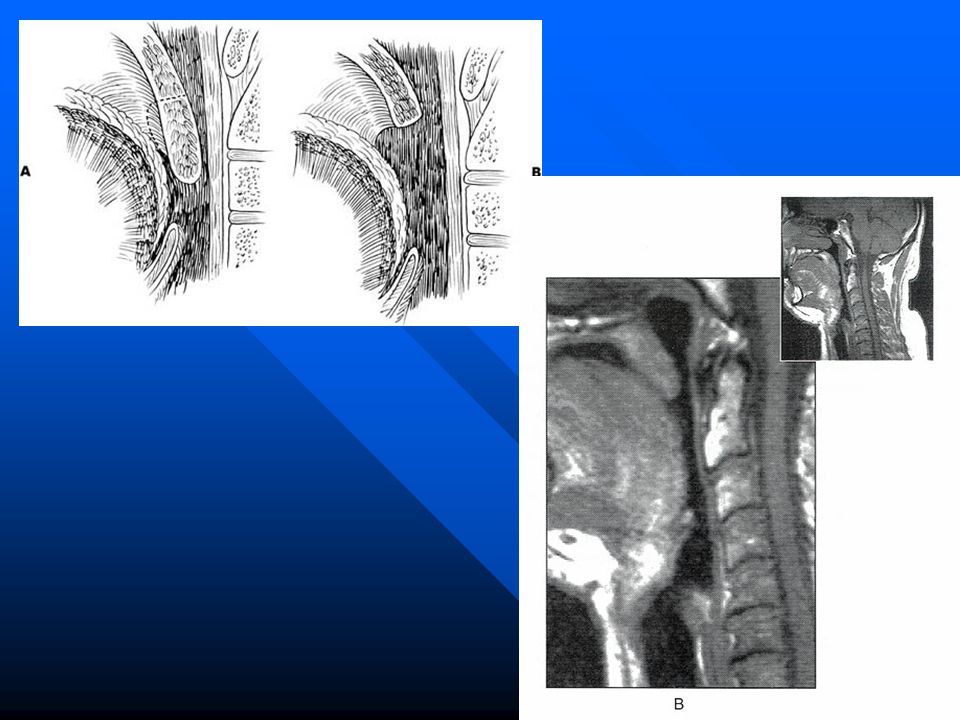
Magnetic Resonance Imaging
Excellent soft tissue anatomy Multiple planes No ionizing radiation Disadvantages Cost Weight limitations Noisy claustrophobia

45
Evaluation of Sleep Split-Night Polysomnography
Epworth Sleepiness Scale

46
Evaluation of Sleep Polysomnography EMG Airflow (nasal and oral)
EEG, EOG Oxygen Saturation Cardiac Rhythm -- Respiratory movement -- Sleeping position Leg Movements AI, HI, AHI, RDI

47
Evaluation of Sleep Polysomnography
Woodson, Tucker “Obstructive Sleep Apnea Syndrome, Diagnosis and Treatment” SIPAC 1996

48
Polisonnografia Apnea centrale:
disfunzione dei centri del respiro a livello del SNC, durata almeno 10 sec., con abolizione dei movimenti toraco-addominali e quindi del flusso aereo ( rara ) Apnea ostruttiva periferica: collasso delle vie aeree superiori di varia natura, almeno 10 sec. di durata, con persistenza dei movimenti toraco-addominali Apnee di tipo misto periferico-centrale: (caratteristiche di entrambi) Ipopnea: ipoventilazione secondaria ad ostruzione parziale
 Apnea ostruttiva periferica: collasso delle vie aeree superiori di varia natura, almeno 10 sec. di durata, con persistenza dei movimenti toraco-addominali. Apnee di tipo misto periferico-centrale: (caratteristiche di entrambi) Ipopnea: ipoventilazione secondaria ad ostruzione parziale.")
49
Polisonnografia Apnea index
Apnea-Hypopnea index = respiratory disturbance index Arousal index

50
Nonsurgical modalities Surgical modalities
TERAPIA Nonsurgical modalities Surgical modalities

51
Nonsurgical Treatment
Weight loss Sleep hygiene and sedative avoidance Pharmacotherapy Smoking cessation Nasal continuous positive airway pressure Oral appliances

52
Apnea ostruttiva periferica terapia
Terapia farmacologico-comportamentale: calo ponderale, terapia del GERD, stop fumo, alcool, tranquillanti, modifiche della postura a letto! antidepressivi?

53
Nonsurgical Treatment
Weight loss Get below “trigger weight” Diet, exercise, bariatric surgery, medications Sleep hygiene Avoidance of sedatives Positional changes

54
Terapia Farmacologica
Protriptyline – decreases REM sleep Xanthine based drugs Steroids Antibiotics Nasal medications

55
Medical Management CPAP since 1981 Very effective
Can be modified and used on a trial basis Pressure must be individually titrated Compliance is as low as 50% Air leakage, eustachian tube dysfunction, noise, mask discomfort, claustrophobia

56
CPAP Titrated to limit all respiratory events
50-90% acceptance – better if daytime symptoms improved Side effects in 40-50%

57
CPAP

58
CPAP

59
CPAP

60
Nonsurgical Management
Oral appliance Advances the mandible Retains the tongue anteriorly

61
Oral Appliances May be as effective as surgical options,
However low compliance rate of about 60% in study by Walker et al in 2002 rendered it a worse treatment modality than surgical procedures Walker-Engstrom ML. Tegelberg A. Wilhelmsson B. Ringqvist I. 4-year follow-up of treatment with dental appliance or uvulopalatopharyngoplasty in patients with obstructive sleep apnea: a randomized study. Chest. 121(3):739-46, 2002 Mar.
:739-46, 2002 Mar.")
62
Oral appliances Advances the mandible Retains the tongue anteriorly
Most effective in nonobese patients with retro or micrognathia Better for mild to moderate cases 51% achieve normal sleep, 61% improved RDI < 20 Consider TMJ dysfunction and occlusal changes

63
Surgical Management Therapy should be directed toward presumed site of obstruction This does not always guarantee results

64
Trattamento chirurgico
Algorithms Riley et al 1992 Studied 2 phase approach for multilevel site of obstruction (Stanford Protocol): Phase 1: Genioglossal advancement, hyoid myotomy and advancement, UP3 Phase 2: Maxillary-Mandibular advancement in 6 months if phase 1 failed Reported >90% success rate in patients who completed both phases Other studies have lowered this number Testing is done at 6 months
: Phase 1: Genioglossal advancement, hyoid myotomy and advancement, UP3. Phase 2: Maxillary-Mandibular advancement in 6 months if phase 1 failed. Reported >90% success rate in patients who completed both phases. Other studies have lowered this number. Testing is done at 6 months.")
65
Riley-Powell-Stanford Protocol

66
Riley-Powell-Stanford Protocol
Post operative PSG at 6 months Phase I = 61% success Phase II = % success

67
Trattamento chirurgico
Measures of success – No further need for medical or surgical therapy Response = 50% reduction in RDI Reduction of RDI to < 20 Reduction in arousals and daytime sleepiness

68
Trattamento chirurgico
Perioperative Issues High risk in patients with severe symptoms Nasal CPAP often required after surgery Nasal CPAP before surgery improves postoperative course Risk of pulmonary edema after relief of obstruction

69
Trattamento chirurgico
Tracheostomy Primary treatment modality Temporary treatment while other surgery is done Thatcher GW. et al: tracheostomy leads to quick reduction in sequelae of OSA, few complications (see table II) Once placed, uncommon to decannulate Thatcher GW. Maisel RH. The long-term evaluation of tracheostomy in the management of severe obstructive sleep apnea. [Journal Article] Laryngoscope. 113(2):201-4, 2003 Feb.
 Once placed, uncommon to decannulate. Thatcher GW. Maisel RH. The long-term evaluation of tracheostomy in the management of severe obstructive sleep apnea. [Journal Article] Laryngoscope. 113(2):201-4, 2003 Feb.")
70
Tracheotomia Bypasses all areas of obstruction
Virtually 100% effective Two indications Temporary procedure during airway reconstruction Severe OSA when CPAP refused, ineffective, or not tolerated or if other conditions exacerbated by the apneas Line the tract with skin flaps Lack of social acceptance

71
Trattamento chirurgico
Nasal Surgery Improved symptoms and CPAP Septoplasty Turbinate reduction Functional nasal reconstruction Limited efficacy when used alone Verse et al 2002 showed 15.8% success rate when used alone in patients with OSA and day-time nasal congestion with snoring (RDI<20 and 50% reduction) Adenoidectomy
 Adenoidectomy.")
72
Trattamento chirurgico
Retropalatal obstruction Retrolingual obstruction

73
ALTERAZIONI DI PALATO MOLLE ED UGOLA

74
NELL’AFFRONTARE IL PROBLEMA VELARE NELL’OSAS NON SI PUO’ PRESCINDERE DA UNA RISOLUZIONE DEL PROBLEMA TONSILLARE

75
SITUAZIONE TONSILLARE
Grado esiti di tonsillectomia Grado I tonsille atrofiche intraveliche Grado II tonsille appena visibili minimamente debordanti dal pilastro anteriore Grado III tonsille ipertrofiche occupanti uno spazio pari a 3/4 dell’istmo delle fauci Grado IV tonsille completamente ostruenti l’istmo delle fauci (kissing tonsils)
")
76
Grado 0 esiti di tonsillectomia
Grado I tonsille atrofiche intraveliche Grado II tonsille appena visibili minimamente debordanti dal pilastro anteriore Grado III tonsille ipertrofiche occupanti uno spazio pari a 3/4 dell’istmo delle fauci Grado IV tonsille completamente ostruenti l’istmo delle fauci (kissing tonsils)
")
77
Trattamento chirurgico
Uvulopalatopharyngoplasty (UPPP) The most commonly performed surgery for OSA Severity of disease is poor outcome predictor Levin and Becker (1994) up to 80% initial success decreased to 46% success rate at 12 months Friedman et al showed a success rate of 80% at 6 months in carefully selected patients Friedman M, Ibrahim H, Bass L. Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg 2002; 127: 13–21.
 The most commonly performed surgery for OSA. Severity of disease is poor outcome predictor. Levin and Becker (1994) up to 80% initial success decreased to 46% success rate at 12 months. Friedman et al showed a success rate of 80% at 6 months in carefully selected patients. Friedman M, Ibrahim H, Bass L. Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg 2002; 127: 13–21.")
78
UPPP Fujita (1981) Most common procedure
1st line tx for retropalatal collapse 10-50% success

79
UPPP

81
UPPP – Fujita / Ikematsu

82
Uppp PRE E POST

83
UPP

84
Trattamento chirurgico
UP3 Complications Minor Transient VPI Hemorrhage<1% Major NP stenosis VPI

85
Trattamento chirurgico
Cahali, 2003 proposed the Lateral Pharyngoplasty for patients with significant lateral narrowing: Cahali MB. Lateral pharyngoplasty: a new treatment for obstructive sleep apnea hypopnea syndrome. Laryngoscope. 113(11):1961-8, 2003 Nov.
:1961-8, 2003 Nov.")
86
Trattamento chirurgico
Lateral Pharyngoplasty

87
Trattamento chirurgico
Lateral Pharyngoplasty Median apnea-hypopnea index decreased from 41.2 to 9.5 (P = .009) No control group No evaluation at 12 months
 No control group. No evaluation at 12 months.")
88
LAUP Laser Assisted Uvulopalatoplasty
High initial success rate for snoring Rates decrease, as for UP3 at twelve months Performed awake

89
COMPLICANZE LAUP- STENOSI

90
Surgical Management Radiofrequency Ablation – Fischer et al 2003
Radiofrequency device is inserted into various parts of palate, tonsils and tongue base at various thermal energies Fischer et al 2003 At 6 months Showed significant reduction of: RDI (but not to below 20) Arousals
 Arousals.")
91
TERAPIA INTERSTIZIALE
RVFR palatale

92
TERAPIA INTERSTIZIALE:
Coblator - Cold Ablation (ablazione fredda). E’ un sistema bipolare che lavora ad una frequenza di 10 KHz. L’ablazione dei tessuti avviene per dissociazione molecolare, anziché per vaporizzazione od esplosione cellulare. I tessuti vengono quindi ridotti in molecole di idrocarburi ed ossidi, Lavora tra i 40 ed i 70°.
. E’ un sistema bipolare che lavora ad una frequenza di 10 KHz. L’ablazione dei tessuti avviene per dissociazione molecolare, anziché per vaporizzazione od esplosione cellulare. I tessuti vengono quindi ridotti in molecole di idrocarburi ed ossidi, Lavora tra i 40 ed i 70°.")
93
IMPIANTI PALATALI: procedura semplice ed efficace consiste nell’inserimento nello spessore del palato molledi tre barrette di materiale sintetico (poliestere) a lento riassorbimento; lo scopo della procedura è causare un irrigidimento velare e di conseguenza minori vibrazioni del palato, monoseduta
 a lento riassorbimento; lo scopo della procedura è causare un irrigidimento velare e di conseguenza minori vibrazioni del palato, monoseduta")
94
Tongue reduction Lingual tonsillectomy Laser midline glossectomy
Lingualplasty Radiofrequency volumetric tissue reduction

95
Trattamento chirurgico
Tongue Base Procedures Lingual Tonsillectomy may be useful in patients with hypertrophy, but usually in conjunction with other procedures

96
Trattamento chirurgico
Tongue Base Procedures Lingualplasty Chabolle, et al success rate of 77% (RDI<20, 50% reduction) in 22 patients in conjunction with UPPP Complication rate of 25% - bleeding, altered taste, odynophagia, edema Can be combined with epiglottectomy
 in 22 patients in conjunction with UPPP. Complication rate of 25% - bleeding, altered taste, odynophagia, edema. Can be combined with epiglottectomy.")
97
Trattamento chirurgico
Lingual Suspension:

98
Trattamento chirurgico
Lingual Suspension:

99
Trattamento chirurgico
Hyoid Myotomy and Suspension Advances (the tongue base ) hyoid bone anteriorly and inferiorly Advances epiglottis anteriorly Enlarges retrolingual airspace Performed in conjunction with other procedures Dysphagia may result
 hyoid bone anteriorly and inferiorly. Advances epiglottis anteriorly. Enlarges retrolingual airspace. Performed in conjunction with other procedures. Dysphagia may result.")
100
Trattamento chirurgico
Mandibular Procedures Genioglossus Advancement Rarely performed alone Increases rate of efficacy of other procedures Transient incisor paresthesia

101
Mandibular Osteotomy with Genioglossus Advancement
Enlarges the retrolingual airway without disturbing dentition Prevents retrolingual collapse

102
Maxillary-Mandibular Advancement
Trattamento chirurgico Maxillary-Mandibular Advancement

103
Maxillomandibular Osteotomy and Advancement
Severe disease Failure with more conservative measures Midface, palate, and mandible advanced anteriorly Limited by ability to stabilize the segments and aesthetic facial changes

104
Trattamento chirurgico
Maxillary-Mandibular Advancement Performed in conjunction with oral surgeons

105
Pediatric OSAS Many features are different 2% of children
Males = Females Peak at age 2-5

106
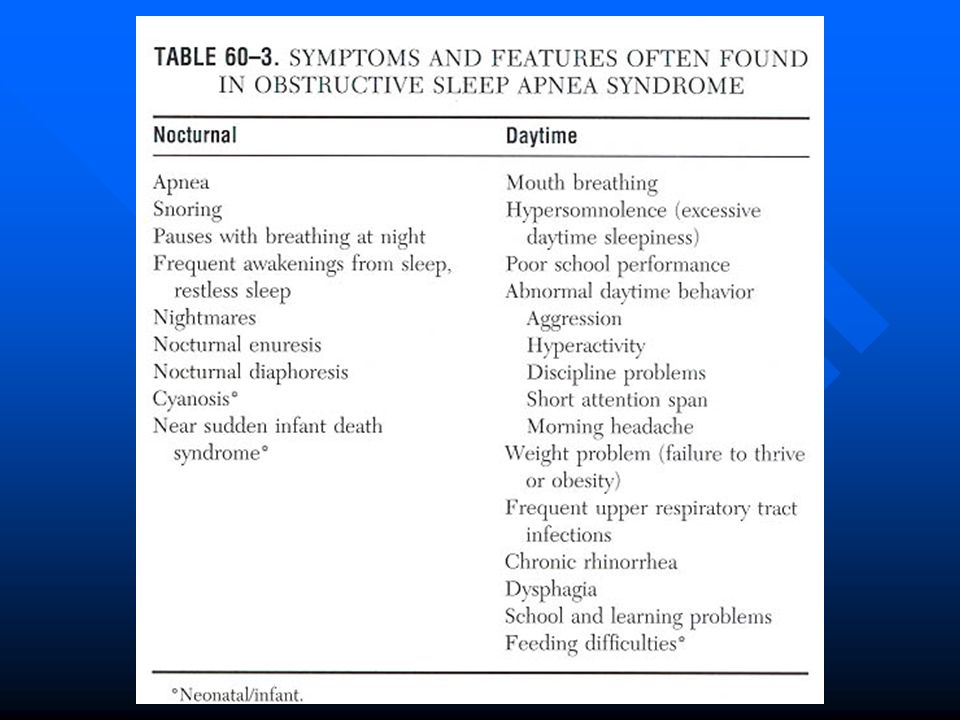
Pediatric OSAS Snoring – severity not predictive
Many are mouth breathers Adenoid facies (15% have OSAS) Excessive daytime sleepiness Obesity vs. FTT Increased respiratory effort
 Excessive daytime sleepiness. Obesity vs. FTT. Increased respiratory effort.")
107
Pediatric OSAS Parasomnias Restless sleep Aggressive behavior
Learning disabilities Enuresis

109
Pediatric OSAS Impaired growth Cor pulmonale Associated with GERD
Possible impairment of release or end-organ response to GH Increased caloric effort with respiration Difficulty with eating Cor pulmonale Associated with GERD

111
Diagnosis History * Physical exam *
The child who always snores, has restless sleep secondary to obstruction, & has apneic episodes per the parents virtually always has PSG confirmation (Brouillette)
")
112
Polisonnografia Not cost effective Considerations CNS disease
Age < 2 Increased surgical risks Family desires Discordant exam

113
Polysomnogram

114
Diagnosis Lateral neck radiographs Chest x-rays EKG

115
Terapia Tonsillectomy & adenoidectomy

116
Down Syndrome OSAS = 54-100% Physical factors
Small midface and cranium Narrow nasopharynx Large tongue Muscular hypotonia Obesity Small larynx Congenital heart disease / cor pulmonale UPPP

117
Trattamento chirurgico
Algorithms Friedman et al developed a staging system for type of operation:

118
Surgical Management Algorithms: Friedman et al:

119
Surgical Management Algorithms: Friedman et al:
Success = RDI<20 and RDI reduced 50% Friedman, Michael MD; Ibrahim, Hani MD; Joseph, Ninos J. BS Staging of Obstructive Sleep Apnea/Hypopnea Syndrome: A Guide to Appropriate Treatment. Laryngoscope. 114(3): , March 2004.
: , March")
121
Algorithm Weight loss CPAP Consider oral appliances for milder cases

122
Conclusions Physiology of Sleep Evaluation of Sleep
Definition of Obstructive Sleep Apnea (OSA) Prevalence of OSA Pathophysiology of OSA Medical Treatment of OSA Surgical Treatment of OSA
 Prevalence of OSA. Pathophysiology of OSA. Medical Treatment of OSA. Surgical Treatment of OSA.")
Presentazioni simili








 is a disease state characterized by airflow limitation that is not fully reversible. The.>")



>")









