Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
LE DISLIPIDEMIE

2
RISULTATI DELLO STUDIO BOTNIA
NGT IFG/IGT T2DM Pazienti HbA1C, % HOMAIR Trigliceridi, mmol/l Colesterolo, mmol/l LDL-col, mmol/l HDL-col, mmol/l 1988 5.30.6 1.801.13 1.290.80 5.71.1 3.81.0 1.380.36 798 5.40.6 2.831.69 1.580.86 5.81.1 3.91.0 1.270.32 1697 7.51.8 6.585.87 2.081.60 5.81.1 3.81.0 1.150.3 Isomaa B et al. Diabetes Care 2001

3
LIPIDS AND LIPOPROTEINS OF DIABETIC PATIENTS WITH AND WITHOUT THE METABOLIC SYNDROME
MSDR+ 85 (53/32) 7.51.4 1.20.3 5.20.9 3.40.8 1.280.28 8920 26.41.1 MSDR- N (male/female) HbA1C, % Triglycerides, mmol/l Cholesterol, mmol/l LDL-chol, mmol/l HDL-chol, mmol/l Apo B, mg/dl LDL-size, nm 85 (53/32) 7.91.6 1.90.9 *** 5.30.9 3.30.9 1.100.26 *** 9818** 25.61.3 *** Isomaa B et al. Diabetologia, 2001
 7.5 1.1. MSDR- N (male/female) HbA1C, % Triglycerides, mmol/l. Cholesterol, mmol/l. LDL-chol, mmol/l. HDL-chol, mmol/l. Apo B, mg/dl. LDL-size, nm. 85 (53/32) 7.9 0.9 *** 5.3 0.26 *** 9818** 25.61.3 *** Isomaa B et al. Diabetologia,")
4
Elevati livelli plasmatici di colesterolo LDL e di trigliceridi e bassi livelli di colesterolo HDL sono predittori indipendenti di rischio cardiovascolare nel diabete. La riduzione dei livelli plasmatici di LDL, e di trigliceridi e l’incremento di HDL riduce la mortalità nei diabetici. UKPDS 23: BMJ 1998

5
Mortalità Cardiovascolare nei Diabetici
UOMINI DONNE 60 50 Diabetici hanno un rischio cardiovascolare equivalente ai non diabetici con CHD ospedalizzati Non ospedalizzati 40 % mortalità (Crude Rate) 30 20 Cardiovascular Mortality in People with Diabetes The Finnish contribution to the World Health Organization Multinational Monitoring of Trends and Determinants of Cardiovascular Disease, FINMONICA, was different from most cardiologic studies in that it monitored prognosis from the beginning of symptoms, including out-of-hospital deaths, which occurred before admission to a hospital. In this study, mortality rates were again higher in diabetic men, who had a little more than a 50% 1-year case fatality rate, than in nondiabetic men, who had about a 35% 1-year case fatality rate. Mortality rates were also higher in diabetic women, who had a 45% case fatality rate, than in nondiabetic women, who had a 24% case fatality rate. However, the case fatality rate is higher in diabetic men than in diabetic women, which is somewhat unusual but can be understood by looking at when the deaths occurred. Time of death was divided into three periods: out-of-hospital deaths, deaths occurring within 28 days of hospitalization, and deaths occurring 28 days to 1 year after hospitalization. In diabetic men, out-of-hospital mortality was much higher than in diabetic women, suggesting that diabetic women may survive long enough to reach the hospital but then have much higher 28-day mortality. In fact, if out-of-hospital mortality is excluded, mortality rates from hospitalization to 1 year are higher in diabetic women than diabetic men, as was shown in the Minnesota Heart Study in the previous slide. Another interesting feature about the FINMONICA study is that it examined the prognosis of people having a first myocardial infarction. Given that diabetics have an increased rate of CHD and an increased case fatality rate, any diabetic who dies before reaching the hospital with a first myocardial infarction cannot possibly benefit from the secondary prevention program. This study was an important influence for the ADA's recommendation that perhaps all diabetics should be treated as if they have preexisting atherosclerosis. Reference: Miettinen H, Lehto S, Salomaa V, Mahonen M, Niemela M, Haffner SM, Pyorala K, Tuomilehto J, for the FINMONICA Myocardial Infarction Register Study Group. Impact of diabetes on mortality after the first myocardial infarction. Diabetes Care 1998;21:69-75. 10 Diabetici Non Diabetici Diabetici Non Diabetici Adapted from Miettinen H et al. Diabetes Care. 1998;21:69-75.
 Cardiovascular Mortality in People with Diabetes. The Finnish contribution to the World Health Organization Multinational Monitoring of Trends and Determinants of Cardiovascular Disease, FINMONICA, was different from most cardiologic studies in that it monitored prognosis from the beginning of symptoms, including out-of-hospital deaths, which occurred before admission to a hospital. In this study, mortality rates were again higher in diabetic men, who had a little more than a 50% 1-year case fatality rate, than in nondiabetic men, who had about a 35% 1-year case fatality rate. Mortality rates were also higher in diabetic women, who had a 45% case fatality rate, than in nondiabetic women, who had a 24% case fatality rate. However, the case fatality rate is higher in diabetic men than in diabetic women, which is somewhat unusual but can be understood by looking at when the deaths occurred. Time of death was divided into three periods: out-of-hospital deaths, deaths occurring within 28 days of hospitalization, and deaths occurring 28 days to 1 year after hospitalization. In diabetic men, out-of-hospital mortality was much higher than in diabetic women, suggesting that diabetic women may survive long enough to reach the hospital but then have much higher 28-day mortality. In fact, if out-of-hospital mortality is excluded, mortality rates from hospitalization to 1 year are higher in diabetic women than diabetic men, as was shown in the Minnesota Heart Study in the previous slide. Another interesting feature about the FINMONICA study is that it examined the prognosis of people having a first myocardial infarction. Given that diabetics have an increased rate of CHD and an increased case fatality rate, any diabetic who dies before reaching the hospital with a first myocardial infarction cannot possibly benefit from the secondary prevention program. This study was an important influence for the ADA s recommendation that perhaps all diabetics should be treated as if they have preexisting atherosclerosis. Reference: Miettinen H, Lehto S, Salomaa V, Mahonen M, Niemela M, Haffner SM, Pyorala K, Tuomilehto J, for the FINMONICA Myocardial Infarction Register Study Group. Impact of diabetes on mortality after the first myocardial infarction. Diabetes Care 1998;21: Diabetici. Non Diabetici. Diabetici. Non Diabetici. Adapted from Miettinen H et al. Diabetes Care. 1998;21:")
6
ADA (American Diabetes Association)
NCEP (National Cholesterol Education Program) JEG (Joint European Guidelines) SISA (Società Italiana per lo studio dell’aterosclerosi) Parametri lipidici Obiettivi lipidici Terapia
 JEG (Joint European Guidelines) SISA (Società Italiana per lo studio dell’aterosclerosi) Parametri lipidici. Obiettivi lipidici. Terapia.")
7
PARAMETRI LIPIDICI Colesterolo totale Colesterolo LDL
Colesterolo HDL Trigliceridi Colesterolo LDL: Colesterolo tot.- HDL- 1/5Triglicerdi Colesterolo non-HDL: Colesterolo totale –Colest. HDL (NCEP/SISA)
")
8
quali obiettivi lipidici nel diabete
? quale terapia ipolipemizzante ?

9
OBIETTIVI LIPIDICI Colesterolo LDL : < 100 mg/dl
Colesterolo HDL: > 40 mg/dl maschi > 50 mg/dl femmine Trigliceridi: < 150 mg/dl ADA / NCEP/SiSA/JEG

10
OBIETTIVI LIPIDICI SECONDARI
COLESTEROLO TOTALE: <175 mg/dl JEG <160 mg/dl SISA/NECP COLESTEROLO non HDL <130 mg/dl NCEP/SISA

11
Ordine di priorità per il trattamento della dislipidemia
Ridurre il colesterolo LDL Incrementare il colesterolo HDL Ridurre i trigliceridi Ridurre LDL < 100 mg è il primo goal nella terapia delle dislipidemie ADA / NCEP/SiSA

12
Heart Protection Study (5-Year Trial)
Log CHD Risk 100 LDL-C (mg/dL) Simvastatin 40 mg 60 26% Reduction in CVD 22% Reduction in CVD Heart Protection Study (5-year trial) Since the ATP III guidelines were published, evidence from HPS was not supportive of the threshold model and has suggested that the relationship between LDL-C level and CHD risk is curvilinear (or possibly linear) across the full range of baseline LDL-C levels included in the study. In HPS, similar benefit on cardiovascular event reduction was provided with simvastatin therapy in patients whose baseline LDL-C was above or below the ATP III goal of 100 mg/dL. Reference: Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:7-22. Heart Protection Study Collaborative Group. Lancet 2002;360:7–22
 Simvastatin 40 mg % Reduction in CVD. 22% Reduction in CVD. Heart Protection Study (5-year trial) Since the ATP III guidelines were published, evidence from HPS was not supportive of the threshold model and has suggested that the relationship between LDL-C level and CHD risk is curvilinear (or possibly linear) across the full range of baseline LDL-C levels included in the study. In HPS, similar benefit on cardiovascular event reduction was provided with simvastatin therapy in patients whose baseline LDL-C was above or below the ATP III goal of 100 mg/dL. Reference: Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:7-22. Heart Protection Study Collaborative Group. Lancet 2002;360:7–22.")
13
Proposte modifiche NCEP
Colesterolemia LDL <70 mg/dl HPS -PROVE-IT

14
QUALE TERAPIA?

15
Livello di evidenza A: Modifica dello stile di vita Terapia farmacologica ADA / NCEP/SiSA/ JEG

16
Stile di vita Terapia nutrizionale Riduzione del peso corporeo
Attività fisica Astensione dal fumo Migliora il profilo lipidico

17
Come deve essere la dieta?
Numerosi studi, non sempre randomizzati e controllati, spesso a breve termine 1. Dieta varia e con tutti i componenti nutrizionali 2. Mantenere un peso ideale SOGGETTI OBESI (diabetici e non): Dieta ipocalorica! SOGGETTI NORMOPESO (diabetici e non): Dieta isocalorica
: Dieta ipocalorica! SOGGETTI NORMOPESO (diabetici e non): Dieta isocalorica.")
18
GRASSI + proteine < 30%
Grassi monoinsaturi + carboidrati 70% I grassi saturi non devono superare il 10% delle calorie totali (<7% se LDL > 100 mg/dl). Colesterolo < 300 mg/die (<200 mg/die se LDL > 100 mg/dl). Diabetes 12,1963 Diabetes Care 12, 1989
. Colesterolo < 300 mg/die (<200 mg/die se LDL > 100 mg/dl). Diabetes 12,1963. Diabetes Care 12,")
19
EFFETTO DELLA RIDUZIONE DEGLI ACIDI GRASSI SATURI
Meta-analisi di 37 studi DIETA LIBERA TG 20 40 60 80 100 120 -8% LDL -12% -16% Col tot -10% -13% HDL -7% GRASSI SATURI 10% GRASSI SATURI 7% % DECREMENTO Am. J. Clin. Nutr., Diabetes Care, 2002

20
Quando iniziare la terapia farmacologica?
Quali farmaci?

21
Indicazioni alla terapia farmacologica nell’ipercolesterolemia
Pazienti che non raggiungono il goal con le modifiche dello stile di vita (Evidenza A- ADA 2004) Diabetici senza CVD con LDL>130 mg/dl (Evidenza A- ADA 2004) Diabetici con LDL mg/dl Diabetici con CVD con LDL> 100 mg/dl Diabetici di età >40 anni e con colesterolo totale >135 mg/dl può essere considerata (Evidenza A- ADA 2004)
 Diabetici senza CVD con LDL>130 mg/dl (Evidenza A- ADA 2004) Diabetici con LDL mg/dl. Diabetici con CVD con LDL> 100 mg/dl. Diabetici di età >40 anni e con colesterolo totale >135 mg/dl può essere considerata (Evidenza A- ADA 2004)")
22
Indicazioni alla terapia farmacologica nell’ipercolesterolemia
Diabetici con LDL mg/dl Molteplici scelte terapeutiche: A) intensificare le modifiche dello stile di vita e/o terapia farmacologica con statine B) ritardare l’adozione di terapie che abbassino le LDL e trattare gli altri fattori di rischio C) se HDL < 40 mg/dl aggiungere fenofibrato
 intensificare le modifiche dello stile di vita e/o terapia farmacologica con statine. B) ritardare l’adozione di terapie che abbassino le LDL e trattare gli altri fattori di rischio. C) se HDL < 40 mg/dl aggiungere fenofibrato.")
23
Farmaci che riducono LDL
Prima scelta: Statine Statine/ezetemibe Seconda scelta: Resine o fenofibrato Quando si usano le statine bisogna controllare: Transaminasi e CPK

24
STATINE Mevalonato Colesterolo B-idrossi-B metil glutaril Coa.
HmgCoA R STATINE Mevalonato Colesterolo 24

25
Profilo farmacocinetico di una selezione delle principali statine
Rosuvastatina Atorvastatina Simvastatina Pravastatina Metabolismo Cyp450 3A4 no sì Metaboliti clinicamente significativi Eliminazione plasmatica duplice: renale / epatica principalmente epatica Idrofilica Epatoselettiva Biodisponibilità 20% 14% <5% 17% Emivita* (ore) 19 14 1,9 2,0 Alcuni punti sul profilo farmacocinetico di rosuvastatina: l’eliminazione di rosuvastatina non dipende dal metabolismo del citocromo P450 in maniera clinicamente significativa. Per questo motivo la probabilità di interazione con altri farmaci smaltiti attraverso questa strada è ridotta. Dovrebbe essere osservato che circa il 50% dei farmaci, comprese atorvastatina e simvastatina, metabolizzati dal sistema del CYP 450, sono metabolizzati attraverso la via del 3A4. C’è una duplice escrezione, renale ed epatica. La rosuvastatina è relativamente idrofila in natura. Una molecola idrofila è potenzialmente molto più selettiva per le cellule epatiche che non una molecola lipofila. Coerentemente con la sua natura di molecola idrofila, la rosuvastatina si è mostrata altamente selettiva per i suoi effetti nelle cellule epatiche rispetto alle cellule non epatiche (fibroblasti). McTaggart F et al. Am J Cardiol 2001;87(suppl):28B-32B Horsmans Y. Eur Heart J Suppl 1999;1(suppl):T7-T12 Buckett L et al. Atherosclerosis 2000;151:41 abs MoP29:W6 25
 ,9. 2,0. Alcuni punti sul profilo farmacocinetico di rosuvastatina: l’eliminazione di rosuvastatina non dipende dal metabolismo del citocromo P450 in maniera clinicamente significativa. Per questo motivo la probabilità di interazione con altri farmaci smaltiti attraverso questa strada è ridotta. Dovrebbe essere osservato che circa il 50% dei farmaci, comprese atorvastatina e simvastatina, metabolizzati dal sistema del CYP 450, sono metabolizzati attraverso la via del 3A4. C’è una duplice escrezione, renale ed epatica. La rosuvastatina è relativamente idrofila in natura. Una molecola idrofila è potenzialmente molto più selettiva per le cellule epatiche che non una molecola lipofila. Coerentemente con la sua natura di molecola idrofila, la rosuvastatina si è mostrata altamente selettiva per i suoi effetti nelle cellule epatiche rispetto alle cellule non epatiche (fibroblasti). McTaggart F et al. Am J Cardiol 2001;87(suppl):28B-32B Horsmans Y. Eur Heart J Suppl 1999;1(suppl):T7-T12 Buckett L et al. Atherosclerosis 2000;151:41 abs MoP29:W")
26
Baseline LDL-C, mg/dl (mmol/L)
CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses Study Drug No. Baseline LDL-C, mg/dl (mmol/L) LDL-C Lowering Primary Prevention AFCAPS/TexCAPS Lovastatin 155 150 (3.9) 25% HPS Simvastatin 3985 127 (3.3) 30% STELLAR Rosuvastatin 46% Secondary Prevention CARE Pravastatin 586 136 (3.6) 28% CHD prevention trials with statins in diabetic subjects: subgroup analyses I Most clinical trials of statin therapy with clinical events as the primary endpoint have included patients with diabetes. Note that the HPS data are still unpublished and thus should be regarded as preliminary. The following slide shows the CHD risk reduction in the overall groups and the diabetic subgroups. References: Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr, for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998;279: Collins R. Randomised trial of cholesterol-lowering therapy and of antioxidant vitamins in 20,536 people at increased risk of coronary heart disease death. Presented at American Heart Association Scientific Sessions, Anaheim, California, 13 November 2001. Goldberg RB, Mellies MJ, Sacks FM, Moye LA, Howard BV, Howard WJ, Davis BR, Cole TG, Pfeffer MA, Braunwald E. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events (CARE) trial. Circulation 1998;98: Pyorala K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G, Scandinavian Simvastatin Survival Study (4S) Group. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 1997;20: Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339: Haffner SM, Alexander CM, Cook TJ, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: subgroup analyses in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159: 4S Simvastatin 202 186 (4.8) 36% LIPID* Pravastatin 782 150 (3.9) 25% HPS Simvastatin 1978 127 (3.3) 30% *LDL-C values for overall group Downs JR et al. JAMA 1998;279: | HPS Investigators. Presented at AHA, | Goldberg RB et al. Circulation 1998;98: | Pyorala K et al. Diabetes Care 1997;20: | Haffner SM et al. Arch Intern Med 1999;159: | LIPID Study Group. N Engl J Med 1998;339:
 LDL-C Lowering. Primary Prevention. AFCAPS/TexCAPS. Lovastatin (3.9) 25% HPS. Simvastatin (3.3) 30% STELLAR. Rosuvastatin. 46% Secondary Prevention. CARE. Pravastatin (3.6) 28% CHD prevention trials with statins in diabetic subjects: subgroup analyses I. Most clinical trials of statin therapy with clinical events as the primary endpoint have included patients with diabetes. Note that the HPS data are still unpublished and thus should be regarded as preliminary. The following slide shows the CHD risk reduction in the overall groups and the diabetic subgroups. References: Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr, for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998;279: Collins R. Randomised trial of cholesterol-lowering therapy and of antioxidant vitamins in 20,536 people at increased risk of coronary heart disease death. Presented at American Heart Association Scientific Sessions, Anaheim, California, 13 November Goldberg RB, Mellies MJ, Sacks FM, Moye LA, Howard BV, Howard WJ, Davis BR, Cole TG, Pfeffer MA, Braunwald E. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events (CARE) trial. Circulation 1998;98: Pyorala K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G, Scandinavian Simvastatin Survival Study (4S) Group. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 1997;20: Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339: Haffner SM, Alexander CM, Cook TJ, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: subgroup analyses in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159: S. Simvastatin (4.8) 36% LIPID* Pravastatin (3.9) 25% HPS. Simvastatin (3.3) 30% *LDL-C values for overall group. Downs JR et al. JAMA 1998;279: | HPS Investigators. Presented at AHA, | Goldberg RB et al. Circulation 1998;98: | Pyorala K et al. Diabetes Care 1997;20: | Haffner SM et al. Arch Intern Med 1999;159: | LIPID Study Group. N Engl J Med 1998;339:")
27
Sequestranti degli acidi biliari
Questi farmaci legano in maniera covalente gli acidi biliari, bloccandone il riassorbimento intestinale, aumentando l’espressione di recettori LDL epatici e stimolando il catabolismo delle LDL •Gli acidi biliari (> 95%) sono riassorbiti a livello dell’ileo distale •Il blocco del riassorbimento porta a conversione del colesterolo in acidi biliari nel fegato •La riduzione del colesterolo intracellulare porta ad aumentata sintesi endogena e captazione mediante aumento dell’espressione dei recettori LDL Resine a scambio ionico ad elevato peso molecolare, insolubili in acqua e fortemente igroscopiche.
 sono riassorbiti a livello dell’ileo distale. •Il blocco del riassorbimento porta a conversione del colesterolo. in acidi biliari nel fegato. •La riduzione del colesterolo intracellulare porta ad aumentata. sintesi endogena e captazione mediante aumento dell’espressione. dei recettori LDL. Resine a scambio ionico ad elevato peso molecolare, insolubili in. acqua e fortemente igroscopiche.")
28
Sequestranti degli acidi biliari
Indicazioni cliniche: •Tutte le forme di ipercolesterolemia tranne l’ipercolesterolemiafamiliare omozigote •Trattamento di elezione nei bambini con ipercolesterolemia eterozigote Dosaggio e precauzioni: •12-24 g/die in 2-3 volte lontano dai pasti o dalla somministrazione di altri farmaci per os •Non hanno effetti sistemici ma possono causare sint. gastrointestinali: nausea, vomito, stipsi, dolori addominali •Riducono l’assorbimento intestinale di warfarina, tiazidi, glucosidi digitalici, tetracicline, propranololo, furosemide, vitamine liposolubili •Il trattamento con questi farmaci riduce il colesterolo totale fino ad un massimo del 30% e le LDL-C fino al 40% •In molti pazienti le HDL-C aumentano del 5-10%

29
Ezetimibe – meccanismo di azione
Chilomicroni Formazione della placca Sangue Remnant Dieta Micelle Colesterolo libero Colesterolo Acidi biliari Sottile strato mucoso Sintesi Biosintesi CL ACAT Colesterolo Esterificato (CE) CL ENTEROCITA Orletto a spazzola CE Sequestranti degli acidi biliari Steroli / Stanoli Statine Inibitori dell’assorbimento del colesterolo (Ezetimibe) L’ezetimibe riduce i livelli di colesterolo inibendone l’assorbimento a livello dell’orletto a spazzola dell’intestino tenue. Mahley et al. Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 10th ed. New York McGraw-Hill, 2001;971–1001 Van Heek M et al. Br J Pharmacol 2001;134:409–417 Miettinen TA Int J Clin Pract 2001;55: 29
 CL. ENTEROCITA. Orletto a. spazzola. CE. Sequestranti. degli acidi biliari. Steroli / Stanoli. Statine. Inibitori dell’assorbimento del colesterolo (Ezetimibe) L’ezetimibe riduce i livelli di colesterolo inibendone l’assorbimento a livello dell’orletto a spazzola dell’intestino tenue. Mahley et al. Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 10th ed. New York McGraw-Hill, 2001;971–1001. Van Heek M et al. Br J Pharmacol 2001;134:409–417. Miettinen TA Int J Clin Pract 2001;55:")
30
Terapia per basso HDL Interventi sullo stile di vita (dieta, attività fisica, astensione fumo) Interventi farmacologici difficili
 Interventi farmacologici difficili.")
31
Colesterolo HDL Numerosi studi epidemiologici hanno evidenziato una relazione inversa tra i valori di colesterolo HDL e l’incidenza delle patologie cardiovascolari. L’aumento di 1 mg/dl di colesterolo HDL ridurrebbe il rischio cardiovascolare del 3%. Gordon D, Circulation 1989

32
Farmaci ed HDL Derivati acido nicotinico: aumento dal 15 al 35%
Fibrati: aumento dal 10 al 25% Statine: aumento dal 4 al 10% Colestiramina: aumento del 2% Ezetimibe: aumento dal 6 all’8% Tiazolidinedioni Muraglitazar

33
Farmaci utilizzati per aumentare i livelli di colesterolo HDL:
Acido nicotinico •Inibizione lipasi ormono-sensibile–Recettore HM74A adipociti •↓liberazione FFA •Inibizione sintesi acidi grassi e TG–↓diacilgliceroloacetiltransferasi2 ↓sintesi VLDL →LDL•↑LPL–↓TG in VLDL e chilomicroni •↑HDL

34
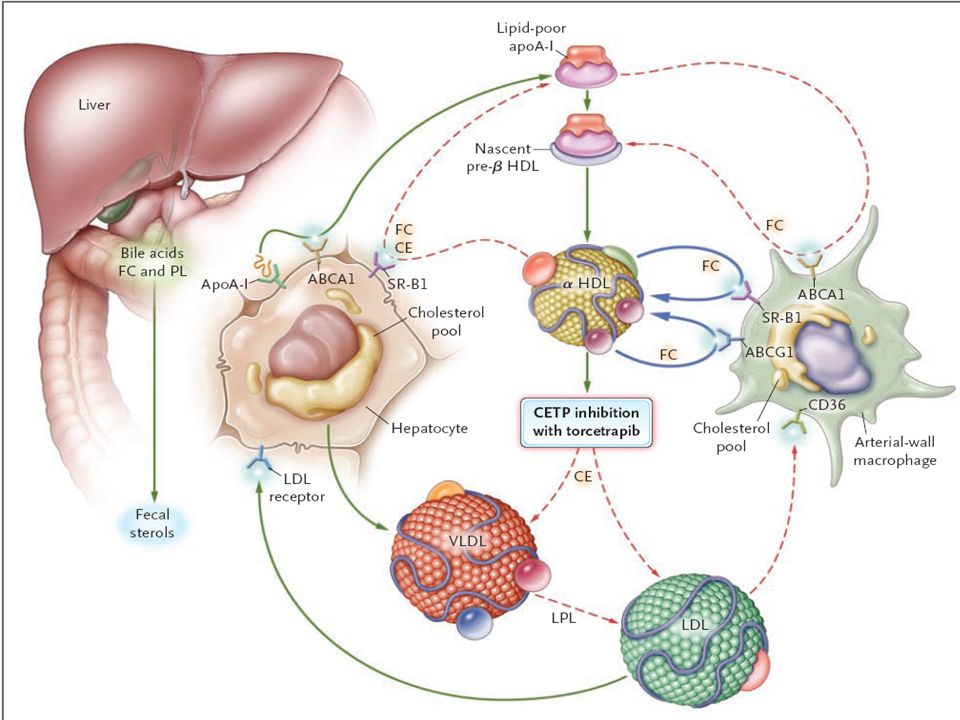
Cholesteryl ester transfer protein (CETP)
La CETP facilita il passaggio di esteri del colesterolo dalle HDL alle LDL e VLDL Sulla base del riscontro di aumentati valori di HDL in soggetti con deficit genetico di CETP, è stata sviluppata una nuova classe di farmaci che inibisce la CETP La somministrazione di un inibitore della CETP, torcetrapib, aumenta i livelli di HDL del 50% Brousseau ME, NEJM 2004

36
TRIALS CLINICI ILLUMINATE
(Investigation of Lipid Level Management to Understand Its Impact in Atherosclerotic Events) ILLUSTRATE (Investigation of Lipid Level Management Using Coronary Ultrasound to Assess Reduction of Atherosclerosis by CETP Inhibition and HDL Elevation
 ILLUSTRATE. (Investigation of Lipid Level Management Using Coronary Ultrasound to Assess Reduction of Atherosclerosis by CETP Inhibition and HDL Elevation.")
37
ILLUMINATE Studio su pazienti ad alto rischio di patologie cardiovascolari Atorvastatina (dosi mg) versus atorvastatina (10-80 mg)+torcetrapib (60 mg) End-point: effetto su eventi cardiovascolari
 versus atorvastatina (10-80 mg)+torcetrapib (60 mg) End-point: effetto su eventi cardiovascolari.")
38
FDA Statement Il 2 dicembre 2006 la PFIZER ha sospeso i trials clinici che utilizzavano il torcetrapib L’ILLUMINATE è stato sospeso dopo un anno dall’inizio dello studio in quanto si sono verificati 82 decessi per IMA ed ictus nel braccio A+T versus 51 decessi nel braccio con sola A; anche gli eventi CV non fatali erano significativamente aumentati nel gruppo in trattamento con torcetrapib

39
EFFETTI DEL TORCETRAPIB

40
ILLUSTRATE Studio parallelo, indipendente, su 1188 pazienti
Effetto di torcetrapib+atorvastatina versus atorvastatina sul processo aterosclerotico a livello coronarico, utilizzando l’ecografia intravascolare per evidenziare le placche End point: azione sulla placca aterosclerotica

41
Terapia dell’ipertrigliceridemia
Prima scelta Controllo glicemico Seconda scelta Terapia con fibrati

42
Indicazioni alla terapia farmacologica con fibrati nell’ipertrigliceridemia
Pazienti con TG > 500 mg/dl Pazienti con TG mg/dl dopo aver raggiunto l’obiettivo per il colesterolo LDL ADA 2004

43
VA-HIT: Incidence of Death from CHD and Nonfatal MI
25 20 Placebo 15 Cumulative Incidence (%) Gemfibrozil 10 5 VA-HIT: Incidence of Death from CHD and Nonfatal MI In the overall study population of VA-HIT, CHD death and nonfatal myocardial infarction were significantly reduced with gemfibrozil. Separation of the Kaplan-Meier curve occurred sometime between the first and second year of the study. Reference: Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J, for the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341: 1 2 3 4 5 6 Year Adapted from Rubins HB et al. N Engl J Med 1999;341:
 Gemfibrozil VA-HIT: Incidence of Death from CHD and Nonfatal MI. In the overall study population of VA-HIT, CHD death and nonfatal myocardial infarction were significantly reduced with gemfibrozil. Separation of the Kaplan-Meier curve occurred sometime between the first and second year of the study. Reference: Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J, for the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341: Year. Adapted from Rubins HB et al. N Engl J Med 1999;341:")
44
Indicazioni alla terapia nella dislipidemia combinata
Prima scelta Controllo glicemico ed alte dosi di statine Seconda scelta Controllo glicemico e statine più fibrati Terza scelta Controllo glicemico e resine più fibrati

45
NCEP: Management of Diabetic Dyslipidemia
Target primario della terapia: LDL-C Diabete: rischio equivalente a quello di soggetti con cardiopatia ischemica Goal per i diabetici: <100 mg/dL Opzioni terapeutiche : – LDL-C 100–129 mg/dL: Aumento di intensità di TLC; Farmaci per modificare dislipidemia aterogenica (fibrate or nicotinic acid); intensificare la terapia con statine – LDL-C 130 mg/dL: simultaneamente iniziare TLC e statine ATP III: Management of diabetic dyslipidemia The primary target of lipid therapy in diabetic subjects in the NCEP ATP III is the reduction of LDL-C. NCEP considers diabetes to be a CHD risk equivalent, therefore the LDL-C goal for persons with diabetes is <100 mg/dL. Note that if a diabetic patient has an LDL-C level of greater than or equal to 130 mg/dL, NCEP suggests simultaneously initiating therapeutic lifestyle changes (TLC) and LDL-lowering drugs. For patients who have an LDL-C between 100 and 129 mg/dL, NCEP suggests a variety of therapeutic options including intensifying TLC or statins or adding a drug to modify atherogenic dyslipidemia (fibrate or nicotinic acid). After the LDL-C goal is met, if the triglyceride level is 200 mg/dL or greater, non–high-density lipoprotein cholesterol (non-HDL-C) should be calculated. The non-HDL-C goal in diabetic subjects is <130 mg/dL. The non-HDL-C goal can be reached by intensifying TLC or statin use or by adding a fibrate or nicotinic acid. Note that the use of a fibrate and a statin together has a small but definable risk of myositis, and nicotinic acid in diabetic subjects has been associated with higher glucose levels in some but not all studies. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Keywords: diabetes, guidelines, LDL cholesterol, non-HDL cholesterol, treatment Slide type: text Se TG 200 mg/dL dopo aver raggiunto il target di LDL-C, il non–HDL-C (<130 mg/dl) diventa target secondario (+statine o ac. nicotinico/fibrati) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:
; intensificare la terapia con statine. – LDL-C 130 mg/dL: simultaneamente iniziare TLC e statine. ATP III: Management of diabetic dyslipidemia. The primary target of lipid therapy in diabetic subjects in the NCEP ATP III is the reduction of LDL-C. NCEP considers diabetes to be a CHD risk equivalent, therefore the LDL-C goal for persons with diabetes is <100 mg/dL. Note that if a diabetic patient has an LDL-C level of greater than or equal to 130 mg/dL, NCEP suggests simultaneously initiating therapeutic lifestyle changes (TLC) and LDL-lowering drugs. For patients who have an LDL-C between 100 and 129 mg/dL, NCEP suggests a variety of therapeutic options including intensifying TLC or statins or adding a drug to modify atherogenic dyslipidemia (fibrate or nicotinic acid). After the LDL-C goal is met, if the triglyceride level is 200 mg/dL or greater, non–high-density lipoprotein cholesterol (non-HDL-C) should be calculated. The non-HDL-C goal in diabetic subjects is <130 mg/dL. The non-HDL-C goal can be reached by intensifying TLC or statin use or by adding a fibrate or nicotinic acid. Note that the use of a fibrate and a statin together has a small but definable risk of myositis, and nicotinic acid in diabetic subjects has been associated with higher glucose levels in some but not all studies. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: cmd=Retrieve&db=PubMed&list_uids= &dopt=Abstract. Keywords: diabetes, guidelines, LDL cholesterol, non-HDL cholesterol, treatment. Slide type: text. Se TG 200 mg/dL dopo aver raggiunto il target di LDL-C, il non–HDL-C (<130 mg/dl) diventa target secondario (+statine o ac. nicotinico/fibrati) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:")
46
JEG: Management of Diabetic Dyslipidemia
Target primario della terapia: LDL-C Diabete: rischio equivalente a quello di soggetti con cardiopatia ischemica Goal per i diabetici: LDL<100 mg/dL Colest. Tot. <175 mg/dl Terapia con statine : – LDL-C 115 mg/dL e Colest-T 190 mg/dl Le concentrazioni di HDL-C e TG non sono utilizzati come obiettivo di terapia, ma sono indicatori di aumentato rischio coronarico ATP III: Management of diabetic dyslipidemia The primary target of lipid therapy in diabetic subjects in the NCEP ATP III is the reduction of LDL-C. NCEP considers diabetes to be a CHD risk equivalent, therefore the LDL-C goal for persons with diabetes is <100 mg/dL. Note that if a diabetic patient has an LDL-C level of greater than or equal to 130 mg/dL, NCEP suggests simultaneously initiating therapeutic lifestyle changes (TLC) and LDL-lowering drugs. For patients who have an LDL-C between 100 and 129 mg/dL, NCEP suggests a variety of therapeutic options including intensifying TLC or statins or adding a drug to modify atherogenic dyslipidemia (fibrate or nicotinic acid). After the LDL-C goal is met, if the triglyceride level is 200 mg/dL or greater, non–high-density lipoprotein cholesterol (non-HDL-C) should be calculated. The non-HDL-C goal in diabetic subjects is <130 mg/dL. The non-HDL-C goal can be reached by intensifying TLC or statin use or by adding a fibrate or nicotinic acid. Note that the use of a fibrate and a statin together has a small but definable risk of myositis, and nicotinic acid in diabetic subjects has been associated with higher glucose levels in some but not all studies. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Keywords: diabetes, guidelines, LDL cholesterol, non-HDL cholesterol, treatment Slide type: text
 and LDL-lowering drugs. For patients who have an LDL-C between 100 and 129 mg/dL, NCEP suggests a variety of therapeutic options including intensifying TLC or statins or adding a drug to modify atherogenic dyslipidemia (fibrate or nicotinic acid). After the LDL-C goal is met, if the triglyceride level is 200 mg/dL or greater, non–high-density lipoprotein cholesterol (non-HDL-C) should be calculated. The non-HDL-C goal in diabetic subjects is <130 mg/dL. The non-HDL-C goal can be reached by intensifying TLC or statin use or by adding a fibrate or nicotinic acid. Note that the use of a fibrate and a statin together has a small but definable risk of myositis, and nicotinic acid in diabetic subjects has been associated with higher glucose levels in some but not all studies. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: cmd=Retrieve&db=PubMed&list_uids= &dopt=Abstract. Keywords: diabetes, guidelines, LDL cholesterol, non-HDL cholesterol, treatment. Slide type: text.")
47
Patients Achieving Goal (%)
Inadequate Achievement of NCEP ATP III Treatment Goals, Especially among Patients at Highest Risk Patients Achieving Goal (%) 100% 70% 80% 60% 40% 39% 40% 18% 20% Inadequate achievement of NCEP ATP III treatment goals, especially among patients at highest risk Over the years, various surveys have documented that the very patients who are at highest CHD risk appear to be the least likely to achieve lipid treatment goals. One such survey was the Lipid Treatment Assessment Project (L-TAP). This analysis evaluated 4,888 patients (4,137 treated with drug therapy and 751 treated with diet and exercise) from 5 regions of the United States who were being treated for hypercholesterolemia in a primary care setting from August 1996 to February Of these patients, 30% had established CHD, 47% had 2 risk factors without evidence of CHD (high-risk group), and 23% had <2 risk factors (low-risk group). Although current achievement of lipid treatment goals may be improved over what may have been achieved in 1996–1997 (based upon this L-TAP analysis), it continues to be true that many of those patients at highest CHD risk often do not achieve lipid treatment goals. Reference: Pearson TA, Laurora I, Chu H, Kafonek S. The Lipid Treatment Assessment Project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving low-density lipoprotein cholesterol goals. Arch Intern Med 2000;160: 0% Low Risk High Risk CHD Patients n = 861 1,924 1,352 4,137 Drug therapy included statins (fluvastatin, lovastatin, pravastatin, simvastatin), gemfibrozil, bile acid sequestrants, niacin, psyllium fiber, and combination drug therapy. Adapted from Pearson TA et al. Arch Intern Med 2000;160;
 100% 70% 80% 60% 40% 39% 40% 18% 20% Inadequate achievement of NCEP ATP III treatment goals, especially among patients at highest risk. Over the years, various surveys have documented that the very patients who are at highest CHD risk appear to be the least likely to achieve lipid treatment goals. One such survey was the Lipid Treatment Assessment Project (L-TAP). This analysis evaluated 4,888 patients (4,137 treated with drug therapy and 751 treated with diet and exercise) from 5 regions of the United States who were being treated for hypercholesterolemia in a primary care setting from August 1996 to February Of these patients, 30% had established CHD, 47% had 2 risk factors without evidence of CHD (high-risk group), and 23% had <2 risk factors (low-risk group). Although current achievement of lipid treatment goals may be improved over what may have been achieved in 1996–1997 (based upon this L-TAP analysis), it continues to be true that many of those patients at highest CHD risk often do not achieve lipid treatment goals. Reference: Pearson TA, Laurora I, Chu H, Kafonek S. The Lipid Treatment Assessment Project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving low-density lipoprotein cholesterol goals. Arch Intern Med 2000;160: % Low Risk. High Risk. CHD. Patients. n = ,924. 1,352. 4,137. Drug therapy included statins (fluvastatin, lovastatin, pravastatin, simvastatin), gemfibrozil, bile acid sequestrants, niacin, psyllium fiber, and combination drug therapy. Adapted from Pearson TA et al. Arch Intern Med 2000;160;")
48
DiSLIPIDEMIA nel DIABETE TIPO 2
Alterazioni qualitative dei trigliceridi Incremento della lipemia postprandiale Alterazioni qualitative delle LDL Alterazioni qualitative delle HDL

49
Size and apolipoprotein composition are the main factors determining atherogenicity of TRL particles
Figure 46 Apoprotein content determines metabolism and atherogenicity of lipoproteins. Apo C-III is associated with high atherogenicity which is attributed to the following mechanisms: decrease in LPL-activated lipolysis; decrease in the capture of small VLDL by the normal receptor; increase in the circulatory residence time of VLDL; increased duration of exposure to atherogenic particles.

50
Metabolismo Postprandiale nel T2DM
Insulina Soppressione di produzione VLDL1 VLDL LPL TRLs Remnants Chilomicroni lipolisi Aterosclerosi

51
PERCHE’ I REMNANTS DELLE TRLs POST-PRANDIALI SONO ATEROGENICHE?
Small remnants sono capaci di penetrare la parete arteriosa con accumulo di CE TRLs sono associati con modificazioni aterogeniche di sottogruppi di LDL e HDL Accumulo di remnants è associato a disfunzione endoteliale e generazione di stress ossidativo

52
Perchè è importante la lipemia postprandiale?
24 1 2 3 4 6 9 12 24 TEMPO, ore TRIGLiCERIDi, mmol/l Type 2 DM Controls 18 6 12 TRLs permangono elevati nel corso delle 24 hrs

53
Nuove Farmaci nella dislipidemia
Farmaci capaci di modulare il metabolismo dei lipidi e delle apoproteine glitazoni agonisti PPAR g Metabolismo dei lipidi PPAR a Fegato muscolo Tessuto adiposo sensibilità insulina captazione glucosio lipolisi

Presentazioni simili








 N. Pazienti in Dialisi (2002: 308.910)>")







 Area Prevenzione ANMCO>")

 sottoposto a CABG.>")
