Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
UO Diagnostica ed Interventistica
Come gestire la terapia antiaggregante e anticoagulante nei pazienti in attesa di chirurgia non cardiaca? Marco Comeglio UO Diagnostica ed Interventistica del Cuore e dei Vasi USL 3 Pistoia I POTENZIALI GRAVI EVENTI AVVERSI HANNO RESO LA GESTIONE DEL TRATTAMENTO ANTICOAGULANTE ED ANTIAGGREGANTE UNO DEGLI ASPETTI Più CONTROVERSI DELLA MEDICINA PERIOPERATORIA. ANCHE IN RELAZIONE ALLA SCARSITà DI TRIALS CLINICI RANDOMIZZATI E LA sostanziale MANCANZA DI LINEE GUIDA DEFINITIVE.

2
Risk Stratification for Perioperative TE in patients on OAT
Nella gestione perioperatoria dei pazienti in OAT il primo step è la caratterizzazione del rischio TE a cui sono soggetti i pazienti. L’american college of Chest phys suddivide i pazienti che maggiormente necessitano di una OAT cronica (protesi valvolari, AF e VTE) in tre categorie di rischio : basso moderato ed alto Mod from Douketis et al. Chest 2008
 in tre categorie di rischio : basso moderato ed alto. Mod from Douketis et al. Chest")
3
HEMORRHAGIC RISK IN NON CARDIAC SURGERY
BLOOD TRANSFUSION TYPE OF SURGERY RISK Skin, and general surgery Minor orthopedic, ORL Endoscopy Cataract, anterior eye Dental extr & surgery Usually not required LOW Visceral surgery CV surgery Major orthop, ORL, urologic Frequently required INTERMEDIATE Intracranial neurosurgery Spinal canal surgery Eye post chamber surgery Possible bleeding in a closed space HIGH Adapted Abualsaud et al, JACC Int 2010

4
Perioperative Management of OAT
in Low- and High-Risk patients/procedures Low thromboembolic risk/low bleeding risk Continue anticoagulant therapy with INR in therapeutic range Low thromboembolic risk/high bleeding risk Discontinue anticoagulant therapy 5 days before the procedure Start LMWH prophylaxis once daily or UFH i.v. 1 day after acenocoumarol interruption, and 2 days after warfarin interruption. Administer the last dose of LMWH at least 12 h before the procedure or give UFH i.v. up to 4 h prior to surgery Resume LMWH or UFH at the pre-procedural dose 1-2 days (at least 12 h) after the procedure according to the haemostatic status. Resume anticoagulant therapy 1 to 2 days after surgery at the pre-procedural dose + 50% boost dose for 2 consecutive days according to the haemostatic status. LMWH/UFH until therapeutic INR is reached BRIDGING
 after the procedure according to the haemostatic status. Resume anticoagulant therapy 1 to 2 days after surgery at the pre-procedural dose + 50% boost dose for 2 consecutive days according to the haemostatic status. LMWH/UFH until therapeutic INR is reached. BRIDGING.")
5
Perioperative Management of OAT
in Low- and High-Risk patients/procedures (2) High thromboembolic risk Discontinue anticoagulant therapy 5 days before the procedure Start therapeutic LMWH twice daily or UFH i.v. 1 day after acenocoumarol interruption, and 2 days after warfarin interruption. Administer the last dose of LMWH at least 12 h before the procedure or give UFH i.v. up to 4 h prior to surgery Resume LMWH or UFH at the pre-procedural dose 1-2 days (at least 12 h) after the procedure according to the haemostatic status. Resume anticoagulant therapy 1 to 2 days after surgery at the pre-procedural dose + 50% boost dose for 2 consecutive days according to the haemostatic status. LMWH or UHF is continued until the INR has returned to therapeutic levels BRIDGING
 High thromboembolic risk. Discontinue anticoagulant therapy 5 days before the procedure. Start therapeutic LMWH twice daily or UFH i.v. 1 day after acenocoumarol interruption, and 2 days after warfarin interruption. Administer the last dose of LMWH at least 12 h before the procedure or give UFH i.v. up to 4 h prior to surgery. Resume LMWH or UFH at the pre-procedural dose 1-2 days (at least 12 h) after the procedure according to the haemostatic status. Resume anticoagulant therapy 1 to 2 days after surgery at the pre-procedural dose + 50% boost dose for 2 consecutive days according to the haemostatic status. LMWH or UHF is continued until the INR has returned to therapeutic levels. BRIDGING.")
6
Indication for OAT (n = 1,262)
Circulation 2009; 119: 2920

7
Anticoagulation Protocols According to Patient Thromboembolic Risk
HIGH TE-RISK CRITERIA Mechanical mitral valve prostheses Monoleaflet aortic prostheses or bileaflet with AF or previous TE AF associated with previous TE or mitral valve disease Previous cardiogenic or unesplained systemic embolism Venous TE < 3 m Pengo et al, Circulation 2009

8
According to the Bleeding Risk
Types of Procedures According to the Bleeding Risk LOW BLEEDING RISK (893) GI Endoscopy Cutaneous Surgery Cistoscopy Biopsies Hand surgery Angiography Ocular anterior ENT procedures Gyno procedures PM/ICD Hepatic procedures Arthroscopy Miscellaneous HIGH BLEEDING RISK (369) Abdominal Orthopedic Maxillofacial Urologic Vascular Gynecologic Ocular Mammary Neurosurgery Pengo et al, Circulation 2009
 GI Endoscopy. Cutaneous Surgery. Cistoscopy. Biopsies. Hand surgery. Angiography. Ocular anterior. ENT procedures. Gyno procedures. PM/ICD. Hepatic procedures. Arthroscopy. Miscellaneous. HIGH BLEEDING RISK (369) Abdominal. Orthopedic. Maxillofacial. Urologic. Vascular. Gynecologic. Ocular. Mammary. Neurosurgery. Pengo et al, Circulation")
9
Thromboembolic Events
5 TE events: 3 venous and 2 arterial 1 fatal event All 5 events in HIGH TE-risk patients 3 events : LMWH not administered according to protocol 2 events : not “bridget” at all Hemorrhagic Events 15 major bleedings : none fatal 11 / 15 : surgical site bleeding 8 / 15 : protocol A ; 7 / 15 : protocol B 53 minor bleedings 27 /53 : at the procedure site Related to protocol (A > B) and procedure bleeding risk Pengo et al, Circulation 2009
 and procedure bleeding risk. Pengo et al, Circulation")
10
Come gestire la terapia antiaggregante nei pazienti in attesa di chirurgia non cardiaca?
EVENTI ISCHEMICI EMORRAGICI Prevenzione Primaria Prevenzione Secondaria Post-Stenting BMS/DES

11
Thrombosis and Haemostasis 2011;105
Prevenzione Primaria As the peri-operative use of aspirin is associated with increased blood loss and blood product use and as patients undergoing primary prophylaxis show no manifestation of any cardiovascular disease, this expert group suggests that aspirin given for primary prevention should be stopped 5–7 days before any type of surgery (46, 47). Further trials are required in order to confirm or refute this recommendation in the future. Thrombosis and Haemostasis 2011;105
. Further trials are required in order to confirm or refute this recommendation in the future. Thrombosis and Haemostasis 2011;105.")
12
A large meta-analysis, including 41 studies in patients, which compared perioprocedural withdrawal vs. bleeding risks of aspirin, concluded that the risk of bleeding complications was increased by 1.5 but that aspirin did not lead to higher severity levels of bleeding complications.121

13
Thrombosis and Haemostasis 2011;105
Prevenzione Secondaria In summary, there is likely a favourable peri-operative benefit-to risk profile for antiplatelet monotherapy (aspirin or clopidogrel) in secondary prevention with the exception of specific types of surgery and situations where the additional bleeding implies an important risk to the patient. This expert group therefore recommends the continuation of aspirin (or clopidogrel) monotherapy for secondary prevention during most types of surgery. Only in patients undergoing surgical procedures in areas of closed space (e.g. intracranial neurosurgery, posterior chamber of the eye, medullary canal etc.) or when major bleeding complications are to be expected, stopping monotherapy with aspirin or clopidogrel 5–7 days pre operatively should be evaluated on a case by case basis. Further clinical trials are warranted. Thrombosis and Haemostasis 2011;105
 in secondary prevention with the exception of specific types of surgery and situations where the additional bleeding implies an important risk to the patient. This expert group therefore recommends the continuation of aspirin (or clopidogrel) monotherapy for secondary prevention during most types of surgery. Only in patients undergoing surgical procedures in areas of closed space (e.g. intracranial neurosurgery, posterior chamber of the eye, medullary canal etc.) or when major bleeding complications are to be expected, stopping monotherapy with aspirin or clopidogrel 5–7 days pre operatively should be evaluated on a case by case basis. Further clinical trials are warranted. Thrombosis and Haemostasis 2011;105.")
14
Antiaggreganti Piastrinici dopo Angioplastica Coronarica

15
Shomig et al NEJM, 1996

16
The main complication of BMS is In-stent-restenosis

17
Late Loss measured by quantitative angiographic analysis at 6 months
A “KEYSTONE” of Interventional Cardiology will be….. …a stent with optimal deliverability and scaffolding which is also impervious to intimal hyperplasia N = 238 patients de novo, native coronary artery Randomized Sirolimus-coated Bx VelocityTM Stent n = 120 Uncoated n = 118 Primary Endpoint Late Loss measured by quantitative angiographic analysis at 6 months RAVEL trial NEJM ; 23

18
RAVEL – Event-Free Survival (Death, MI, CABG, Re-PTCA)
100 94.0% 95 Sirolimus 90 85 P (FE) < P (LR) = Patients Without Event(%) 80 75 70.7% 70 Control 65 60 60 120 180 240 300 360 Time (Days) N Engl J M ; 23
 < P (LR) = Patients Without Event(%) % 70. Control Time (Days) N Engl J M ; 23.")
19
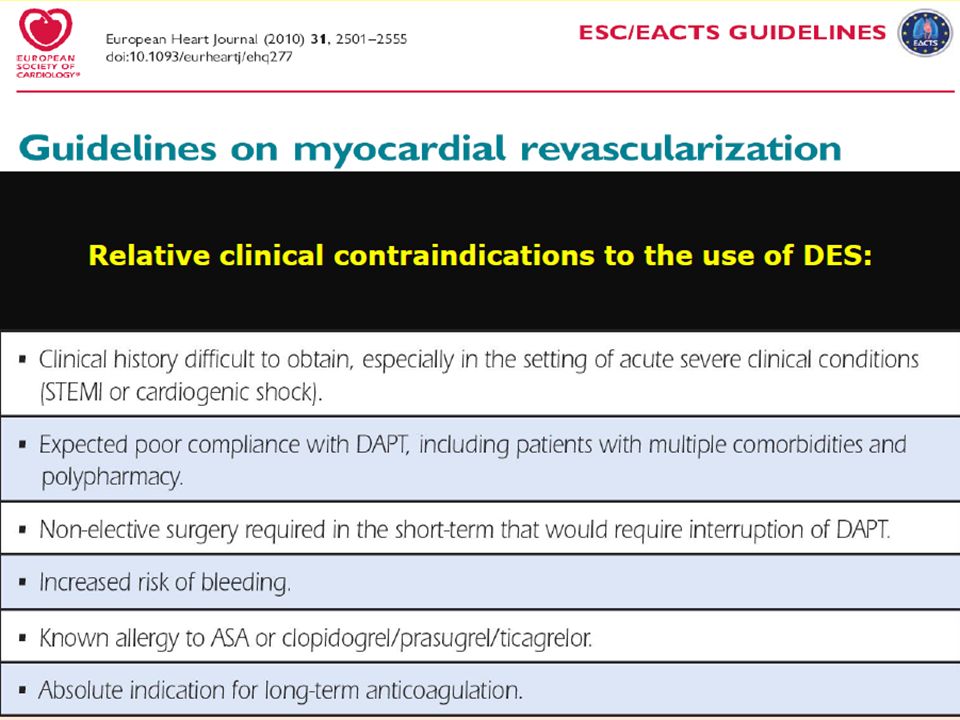
DES use must be cautious in patients with
Lancet 2004 DES use must be cautious in patients with ASA/Clopidogrel intolerance or allergy Surgery candidates Haemorrhagic diseases

21
VLST in DES

25
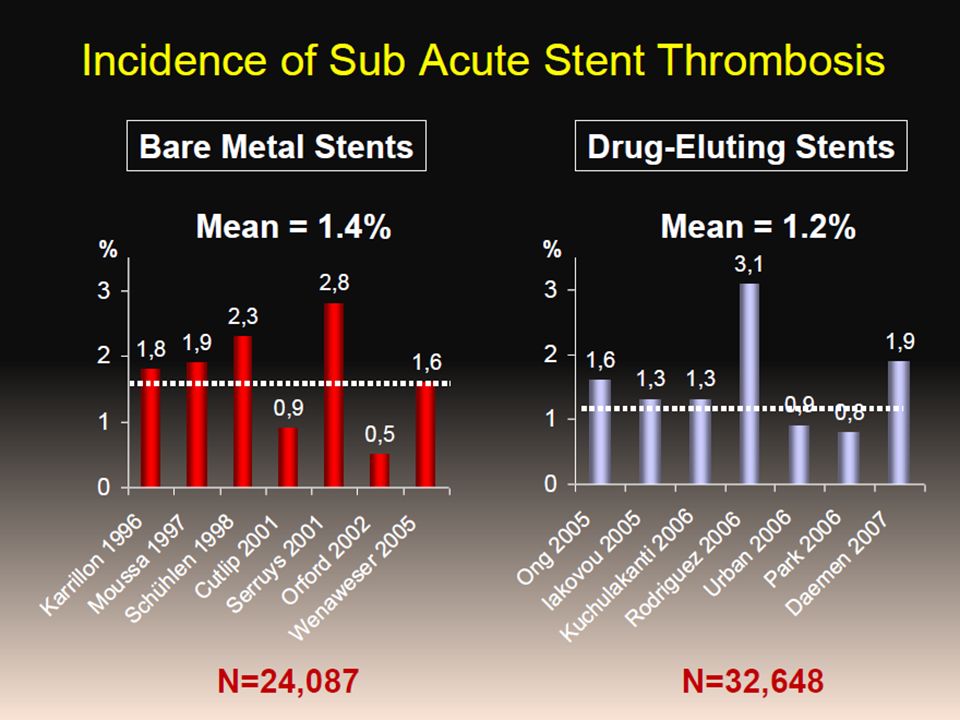
Occurrence and Frequency of
First Generation DES Occurrence and Frequency of ST over time VLST Daemen et al, Lancet 2007

26
DES and VLST Bern-Rotterdam Cohort Study @ 4 Years
8,146 consecutive patients treated with 1st gen DES Risk of VLST 0.4 – 0.5 % per year Wenaveser et al, JACC 2008

27
Mortality in Patients with Stent Thrombosis
(38/2974 – 1.27%) Lack of CLOPI Rx was the strongest ST predictor p = 40 % Acute 5 Sub-acute ± 8.5 d Late (>30d) ± 100 d 30 31% 20 19% 10 12% 1 M 6 M F-UP Kuchulakanti et al, Circ 2006
 Lack of CLOPI Rx was the strongest ST predictor p = % Acute 5. Sub-acute ± 8.5 d. Late (>30d) ± 100 d % % % 1 M. 6 M. F-UP. Kuchulakanti et al, Circ")
29
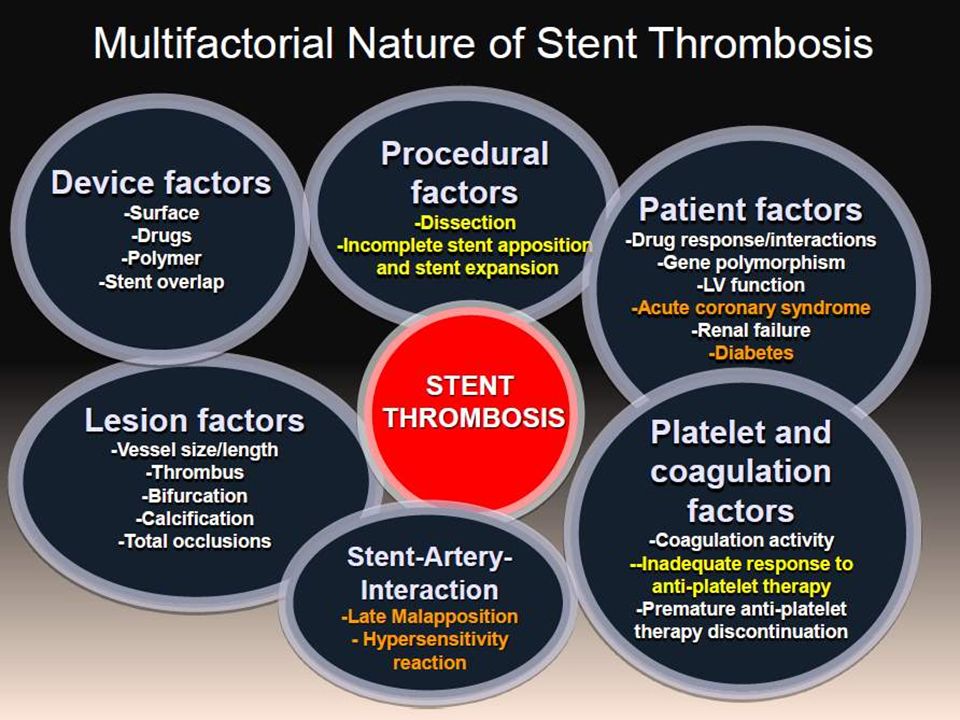
PREDICTORS OF THROMBOSIS AFTER SUCCESSFUL IMPLANTATION OF DES
Iakovou et al, JAMA, 2005

31
Major Non-Cardiac Surgery After DES
Factors identified with premature discontinuation of APT Not receiving discharge instructions for medication use Not being referred for a cardiac rehabilitation program Older age Low cultural level Not being married Economical issues Pre-existing anemia Invasive procedures Surgery Berger et al JACC Int 2010 Days after hospital discharge Freedom from Major Surgery 0.5% per month after the first 2 months 5% EVENT Registry Major Non-Cardiac Surgery After DES 206/4,367

34
RESTENOSIS STENT THROMBOSIS 42,773 12,153 6,425 Sarno G, ESC 2011

35
Bern-Rotterdam Cohort Study PES N = 4308 SES N = 3819 EES N = 4212
Raber et al, ESC 2011

36
Bern-Rotterdam Cohort Study Raber et al, ESC 2011

37
Valgimigli, ESC, 2011

38
Valgimigli, ESC, 2011

39
Valgimigli, ESC, 2011

40
Valgimigli, ESC, 2011

41
Kastrati, ESC, 2011

42
PRASUGREL Novel Antiplatelets Oral Thienopyridine
Pro-drug metabolized via cit P450 Selective and irreversible binding More rapid, potent and consistent platelet inhibition More effective than Clopidogrel in ACS but with more bleedings Peri-operative use maight be limited because of increased risk of bleeding Potentially useful soon after surgery

43
TICAGRELOR Novel Antiplatelets Oral ADP P2Y12 receptor antagonist
Non thienopyridine ADP analog Binds directly and reversibly to the P2Y12 without metabolic activation Achieves greater platelet aggregation inhibition than Clopidogrel Short half-life (6-12 h) Rapid onset of action (2-4 h) Reversibility Patients with stents would discontinue TICAGRELOR only 1 day before surgery and resume it soon after surgery, reducing the risk of both ST and Hemorrhage
 Rapid onset of action (2-4 h) Reversibility. Patients with stents would discontinue TICAGRELOR only 1 day before surgery and resume it soon after surgery, reducing the risk of both ST and Hemorrhage.")
44
The BRIDGE trial ongoing CANGRELOR Novel Antiplatelets
Intravenous ADP P2Y12 receptor antagonist Non thienopyridine ADP analog Binds directly and reversibly to the P2Y12 without metabolic activation Very short half-life (3 min) Rapid onset of action Reversibility Could be used as a “Bridging Therapy” in the perioperative setting: stopped minutes before surgery and resumed sooner than other APT post-operatively The BRIDGE trial ongoing
 Rapid onset of action. Reversibility. Could be used as a Bridging Therapy in the perioperative setting: stopped minutes before surgery and resumed sooner than other APT post-operatively. The BRIDGE trial. ongoing.")
45
Preoperative evaluation of patients with stents
CHECKLIST Preoperative evaluation of patients with stents Determine type of stent: BMS or DES ? In case of DES: 1st or 2° generation DES ? Determine how long ago each stent was implanted Determine location of each stent & tecnique (eg, crush) How complicated was the revascularisation? Were there any complications (eg, underexpansion, malapposition)? Is there any prior history of stent thrombosis? What APT regimen is being used? Determine patient’s comorbidities to further ascertain risk level (EF, diabetes, renal insufficiency) What is the recommended duration of DAPT? What is the surgery bleeding risk? Jaffer AK. Clev Clin J 2009
 How complicated was the revascularisation Were there any complications (eg, underexpansion, malapposition) Is there any prior history of stent thrombosis What APT regimen is being used Determine patient’s comorbidities to further ascertain risk level (EF, diabetes, renal insufficiency) What is the recommended duration of DAPT What is the surgery bleeding risk Jaffer AK. Clev Clin J")
47
Recommendations Experts Korte et al, Thromb Haemost, 2011

48
Perioperative Antiplatelet Management in Patients with Recently Implanted Coronary Stents
“BRIDGING” May et al, Thromb Haemost 2008

49
Protocollo Peri-Operatorio
ASA o TPD Pregresso IMA, CAD, Ictus, PAOD, Stent NO SI Prevenzione Primaria Prevenzione Secondaria Stop APT ASA : 7 gg prima int elett TPD : 15 gg prima int elett Valutazione del Rischio Emorragico Intermedio Elevato Basso * Valutazione Collegiale del Rapporto R/B ASA : 75 mg/die + PPI Da 7 gg prima dell’int elettivo nei pazienti trattati con ASA Da 15 gg prima dell’int elettivo nei pazienti trattati con TPD * Riprendere ASA asap Profilassi TE “dopo” intervento

50
Valutazione Collegiale del Rapporto R/B
Protocollo Peri-Operatorio ASA + TPD Valutazione Collegiale del Rapporto R/B Basso Rischio TR Elevato Rischio TR Chirurgia Differibile? SI Continua ASA Stop TPD 5 gg prima Differire NO Rischio di sanguinamento non controllabile chirurgicamente? * SI “Bridge Therapy” NO Operare in DAPT * Riprendere DAPT asap Profilassi TE “dopo” intervento

51
STENT/APT e Chirurgia non Cardiaca
Take Home Message STENT/APT e Chirurgia non Cardiaca DAPT in PCI = Obiettivo da perseguire Almeno 1 mese BMS; 6 mesi DES. In considerazione della gravità della ST e della incidenza di sanguinamenti relativamente bassa Valutazione collegiale : Chirurgo – Cardiologo – Anestesista Controindicazioni ai DES: in alcune situazioni cliniche prevenire la necessità di DAPT prolungata è preferibile rispetto a curare le complicanze emorragiche o trombotiche Rischio emorragico elevato : il trattamento con sola ASA è gravato da una incidenza di ST relativamente bassa Completa sospensione dell’ APT : raramente necessaria, in tal caso è opportuno adottare terapie “bridging” DES di nuova generazione : migliore profilo di sicurezza Nuovi farmaci antipiastrinici : posso facilitare la gestione peri-operatoria

54
Predictors of ARC Definite or Probable
2-Year Stent Thrombosis : EES Stent Discontinuation Hazard Ratio P of Thienopyridine (95% CI) VALUE Before 6 months YES vs. NEVER After 6 months 8.06 (1.79 , 36.22) 0.007 1.06 (0.24 , 4.73) 0.94 SPIRIT IV
 VALUE. Before 6 months. YES vs. NEVER. After 6 months (1.79 , 36.22) (0.24 , 4.73) SPIRIT IV.")
55
HEMORRHAGIC RISK IN NON CARDIAC SURGERY
BLOOD TRANSFUSION TYPE OF SURGERY RISK Skin, and general surgery Biopsies Minor orthopedic, ORL Endoscopy Cataract, anterior eye Dental extr & surgery Usually not required LOW Visceral surgery CV surgery Major orthop, ORL, urologic Frequently required INTERMEDIATE Intracranial neurosurgery Spinal canal surgery Eye post chamber surgery Possible bleeding in a closed space HIGH Adapted Abualsaud et al, JACC Int 2010

56
SURGICAL RISK ESTIMATE
Risk of MI and Cardiac Death within 30 days after Surgery

Presentazioni simili















>")




 17 Ottobre 2009 DOPPIA ANTIAGGREGAZIONE PIASTRINICA.>")

