Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
8 milioni 2 milioni 2 miliardi NEL MONDO di individui sviluppano
la malattia ogni anno di morti ogni anno 2 miliardi di individui infettati dal M. tuberculosis

2
200 milioni 50.000 NELL’UNIONE EUROPEA nuovi casi di malattia
ogni anno di individui infettati dal M. tuberculosis

3
Figure 1 Reported rates of incidence of tuberculosis in the 10 new member states of the European Union and Germany (2002). Kaufmann, S H E Ann Rheum Dis 2004;63:ii50-56ii Copyright ©2004 BMJ Publishing Group Ltd.

4
LA TB PUÒ PRESENTARSI IN DUE FORME:
Forma “attiva”, caratterizzata dall’osservazione microscopica di batteri vitali nell’espettorato Forma “latente”, definita, in assenza di sintomi clinici, da una reazione di ipersensibilità di tipo ritardato quando il paziente viene stimolato per via s.c. con derivato proteico purificato PPD (test della tubercolina o di Mantoux)
")
5
TEST DELLA TUBERCOLINA (o test di Mantoux)
")
6
The pathology of the granuloma
Infection with Mycobacterium tuberculosis follows a relatively well-defined sequence of events. The infectious bacilli are inhaled as droplets from the atmosphere. Exhaled droplets or nuclei are known to remain in the atmosphere for several hours, and the infectious dose is estimated at a single bacterium. In the lung the bacteria are phagocytosed by alveolar macrophages and induce a localized proinflammatory response that leads to the recruitment of mononuclear cells from neighbouring blood vessels (see figure). These cells are the building blocks for the granuloma, or tubercle, which is the signature of tuberculosis. The granuloma consists of a kernel of infected macrophages surrounded by foamy macrophages and other mononuclear phagocytes, with a mantle of lymphocytes in association with a fibrous cuff of collagen and other extracellular matrix components that delineates the periphery of the structure (see figure). This tissue response typifies the 'containment' phase of the infection in which there are no overt signs of disease and the host does not transmit the infection to others. In the later stages, the granuloma develops a marked fibrous sheath and the number of blood vessels penetrating the structure diminishes markedly. Histological studies with nitroimidazole indicate that at least the boundary to the central region of these granulomas is hypoxic30. Containment usually fails when the immune status of the host changes, which is usually a consequence of old age, malnutrition or co-infection with HIV— basically any condition that reduces the number, or impairs the function, of CD4+ T cells. Following such a change in immune status the granuloma caseates (decays into a structureless mass of cellular debris), ruptures and spills thousands of viable, infectious bacilli into the airways. This results in the development of a productive cough that facilitates aerosol spread of infectious bacilli.
. These cells are the building blocks for the granuloma, or tubercle, which is the signature of tuberculosis. The granuloma consists of a kernel of infected macrophages surrounded by foamy macrophages and other mononuclear phagocytes, with a mantle of lymphocytes in association with a fibrous cuff of collagen and other extracellular matrix components that delineates the periphery of the structure (see figure). This tissue response typifies the containment phase of the infection in which there are no overt signs of disease and the host does not transmit the infection to others. In the later stages, the granuloma develops a marked fibrous sheath and the number of blood vessels penetrating the structure diminishes markedly. Histological studies with nitroimidazole indicate that at least the boundary to the central region of these granulomas is hypoxic30. Containment usually fails when the immune status of the host changes, which is usually a consequence of old age, malnutrition or co-infection with HIV— basically any condition that reduces the number, or impairs the function, of CD4+ T cells. Following such a change in immune status the granuloma caseates (decays into a structureless mass of cellular debris), ruptures and spills thousands of viable, infectious bacilli into the airways. This results in the development of a productive cough that facilitates aerosol spread of infectious bacilli.")
7
FIGURE 1 | Trafficking of Mycobacterium tuberculosis bacilli in cells
Following phagocytosis, phagosomes containing IgG-coated beads acidify rapidly to pH 5 (a) and lower, and the inert particles are subsequently delivered to the lysosome (b). By contrast, phagosomes containing M. tuberculosis only acidify to pH 6.4 (a) and fail to fuse with lysosomes. The vacuoles containing M. tuberculosis retain many of the characteristic of the early endosomal system (b). They are accessible to recycling endosomes, as evidenced by their acquisition of labelled transferrin when it is added to the external medium. Components of the peripheral cell wall of the bacteria that are shed into the bacteria-containing vacuoles traffic out of the vacuoles and coalesce in dense, lysosomal compartments. Finally, the bacteria-containing vacuoles, in common with most endosomal/lysosomal stages, fuse with delivery vesicles trafficking from the trans-Golgi network of the host cell. The data imply that the vacuoles in which M. tuberculosis reside are not particularly hostile with respect to both pH and hydrolytic activity35. Russell Nature Reviews Microbiology 5, 39–47 (January 2007) | doi: / nrmicro1538
 and lower, and the inert particles are subsequently delivered to the lysosome (b). By contrast, phagosomes containing M. tuberculosis only acidify to pH 6.4 (a) and fail to fuse with lysosomes. The vacuoles containing M. tuberculosis retain many of the characteristic of the early endosomal system (b). They are accessible to recycling endosomes, as evidenced by their acquisition of labelled transferrin when it is added to the external medium. Components of the peripheral cell wall of the bacteria that are shed into the bacteria-containing vacuoles traffic out of the vacuoles and coalesce in dense, lysosomal compartments. Finally, the bacteria-containing vacuoles, in common with most endosomal/lysosomal stages, fuse with delivery vesicles trafficking from the trans-Golgi network of the host cell. The data imply that the vacuoles in which M. tuberculosis reside are not particularly hostile with respect to both pH and hydrolytic activity35. Russell Nature Reviews Microbiology 5, 39–47 (January 2007) | doi: / nrmicro1538.")
8
FIGURE 2 | Release and trafficking of bacterial lipids
Mycobacterium tuberculosis sheds its peripheral cell-wall components into its vacuole. These lipids accumulate in multilamellar bodies (a) in mixed micellar structures that contain both host- and pathogen-derived components. The multilamellar bodies coalesce in the multivesicular lysosome, known as the major histocompatibility complex class II-enriched compartment in antigen-presenting cells (b). The vesicles gain egress from the infected macrophage by exocytosis and are released as exosomes into the external milieu (c). The exosomes, carrying pathogen-derived lipids and proteins, are internalized by neighbouring cells (d)
 in mixed micellar structures that contain both host- and pathogen-derived components. The multilamellar bodies coalesce in the multivesicular lysosome, known as the major histocompatibility complex class II-enriched compartment in antigen-presenting cells (b). The vesicles gain egress from the infected macrophage by exocytosis and are released as exosomes into the external milieu (c). The exosomes, carrying pathogen-derived lipids and proteins, are internalized by neighbouring cells (d)")
9
DATI SALIENTI SULLA TB Due miliardi di individui portatori dell’infezione 8,4 milioni di nuovi casi/anno Tre milioni di morti/anno Ogni individuo malato può infettarne fino ad altri 20 La TB si può prevenire e curare Un trattamento inadeguato favorisce l’insorgenza di resistenza Lo sviluppo della TB è favorito dall’infezione da virus HIV e viceversa

10
FATTORI CHE HANNO FAVORITO LA RIPRESA DELLA TB NEI PAESI INDUSTRIALIZZATI
Immigrazione da Paesi con elevata prevalenza di TB Diffusione dell’infezione da HIV Emergenza di MDR Problemi sociali

11
FATTORI CHE PREDISPONGONO ALL’INFEZIONE DA M.tuberculosis
Stretto contatto con assembramenti di persone (p.e. in scuole, ospedali, dormitori, carceri etc.) scarsa alimentazione uso di farmaci iv alcoolismo infezione da HIV (il 10%di tutti gli individui HIV-positivi è portatore di M.TB, pari a circa 400x l’incidenza nella popolazione generale)
 scarsa alimentazione. uso di farmaci iv. alcoolismo. infezione da HIV (il 10%di tutti gli individui HIV-positivi è portatore di M.TB, pari a circa 400x l’incidenza nella popolazione generale)")
12
FATTORI CHE FAVORISCONO LA PROGRESSIONE DELLA MALATTIA
ceppo di M.TB precedente esposizione vaccinazione dose infettiva status immunitario dell’ospite

13
Caratteristiche del Mycobacterium tuberculosis
Elevato contenuto di acidi micolici e altri lipidi nella parete cellulare.

14
Caratteristiche del Mycobacterium tuberculosis
Elevato contenuto di acidi micolici e altri lipidi nella parete cellulare. diminuita permeabilità della parete cellulare ai coloranti resistenza a molti antibiotici resistenza all’uccisione da parte di composti acidi e alcalini resistenza alla lisi osmotica mediata da deposizione di complemento resistenza a ossidazioni letali sopravvivenza all’interno dei macrofagi (grazie alla presenza di lipoarabinomannano)
")
15
FARMACI ANTITUBERCOLARI
FARMACI DI I LINEA:

16
FARMACI ANTITUBERCOLARI
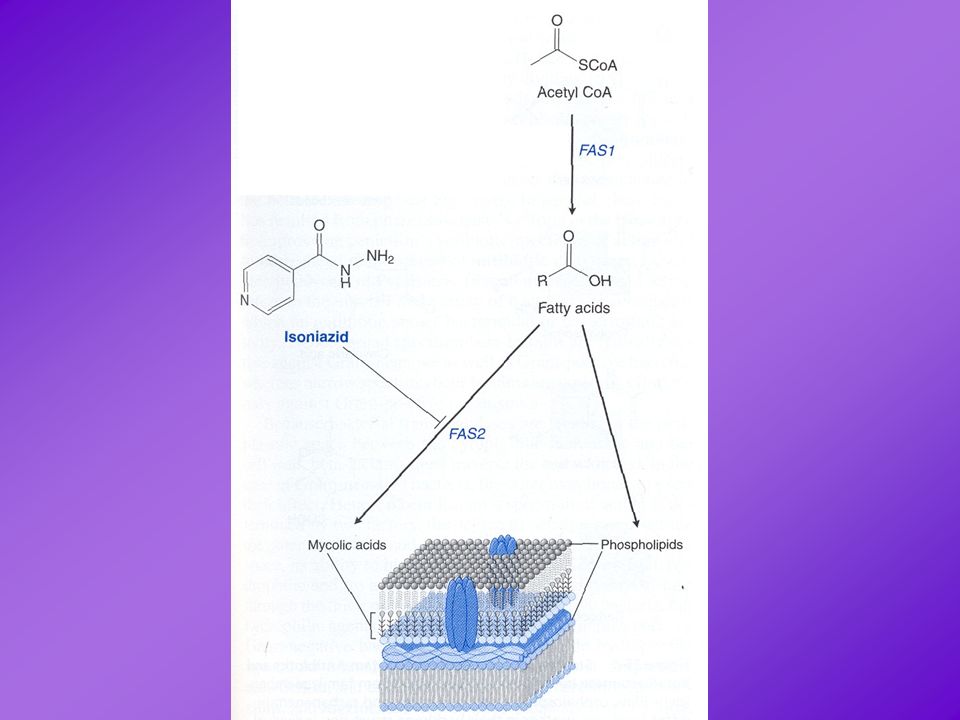
Isoniazide Meccanismo d’azione: blocco della sintesi degli acidi micolici per inibizione del sistema di sintesi degli acidi grassi FAS-II. È un profarmaco, attivato dalla catalasi batterica.

18
Fig. 2. The bacterial fatty acid biosynthesis (FAB) elongation cycle, with antibacterial sites of action indicated. The FAB pathway is highly conserved in bacteria and involves at least nine enzymes in the elongation cycle. (a) The first step is condensation, catalyzed by -ketoacyl-ACP synthase, which condenses the malonyl-ACP with either acetyl-CoA (FabH synthase) or acyl-ACP (FabB and FabF synthases). The malonyl-ACP used in the condensing step is formed by malonyl-CoA:ACP transacylase (FabD). (b) The second step is a reduction, in which the ketoester is catalyzed by the NADPH-dependent -ketoester-dependent reductase, FabG. (c) The third step is dehydration, catalyzed by -hydroxylacyl-ACP dehydrase (FabZ or FabA in proteobacteria), capable of forming trans-2-enoyl-ACP. (d) The final step in each cycle is catalyzed by the NADPH-dependent enoyl-ACP reductase (FabI), which converts the trans-2-enoyl-ACP to acyl-ACP to be used at the new cycle of FAB. There is good homology among the FAB genes of bacteria, although some FAB genes are a bit more species specific. For example, the enoyl ACP-reductase in most of the gram-positive bacteria is FabI, whereas in S. pneumoniae it is FabK and in B. subtilis it is FabL. Note that each step through the cycle adds two carbons (coming from acetyl-CoA) to a growing chain.
 elongation cycle, with antibacterial sites of action indicated. The FAB pathway is highly conserved in bacteria and involves at least nine enzymes in the elongation cycle. (a) The first step is condensation, catalyzed by -ketoacyl-ACP synthase, which condenses the malonyl-ACP with either acetyl-CoA (FabH synthase) or acyl-ACP (FabB and FabF synthases). The malonyl-ACP used in the condensing step is formed by malonyl-CoA:ACP transacylase (FabD). (b) The second step is a reduction, in which the ketoester is catalyzed by the NADPH-dependent -ketoester-dependent reductase, FabG. (c) The third step is dehydration, catalyzed by -hydroxylacyl-ACP dehydrase (FabZ or FabA in proteobacteria), capable of forming trans-2-enoyl-ACP. (d) The final step in each cycle is catalyzed by the NADPH-dependent enoyl-ACP reductase (FabI), which converts the trans-2-enoyl-ACP to acyl-ACP to be used at the new cycle of FAB. There is good homology among the FAB genes of bacteria, although some FAB genes are a bit more species specific. For example, the enoyl ACP-reductase in most of the gram-positive bacteria is FabI, whereas in S. pneumoniae it is FabK and in B. subtilis it is FabL. Note that each step through the cycle adds two carbons (coming from acetyl-CoA) to a growing chain..")
19
FARMACI ANTITUBERCOLARI
Isoniazide Meccanismo d’azione: blocco della sintesi degli acidi micolici per inibizione del sistema di sintesi degli acidi grassi FAS-II. È un profarmaco, attivato dalla catalasi batterica. Meccanismi di resistenza: mutazione del gene che codifica per catalasi-perossidasi mutazione di geni implicati nella sintesi di acidi micolici Effetti collaterali: Reazioni di ipersensibilità (orticaria, febbre, epatite) Ittero; epatotossicità Effetti legati al deficit di vitamina B6
 Ittero; epatotossicità. Effetti legati al deficit di vitamina B6.")
21
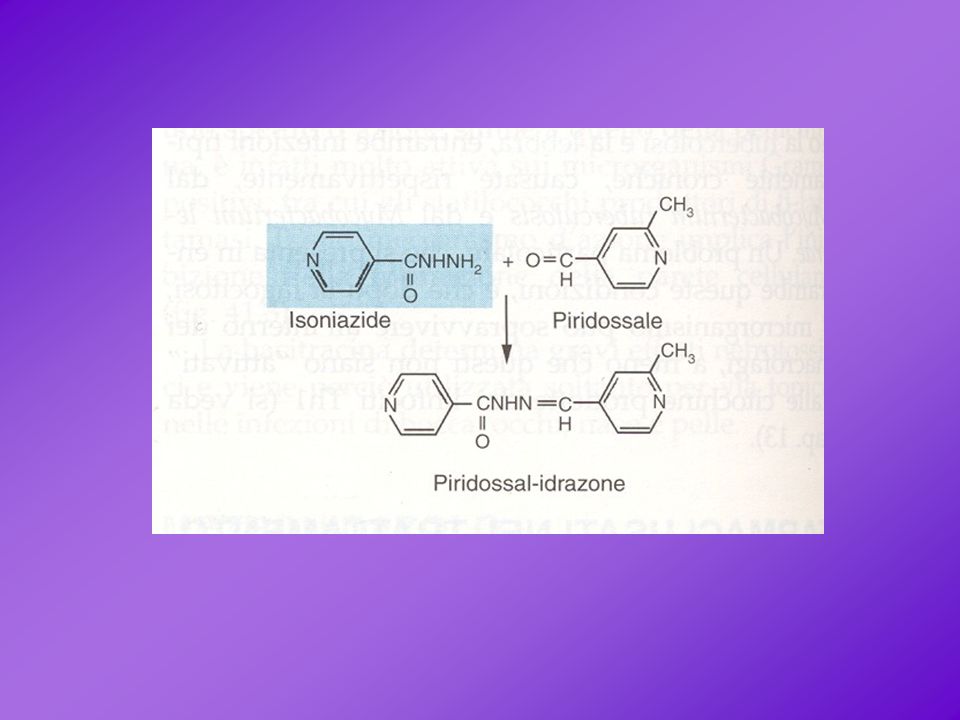
Effetti della isoniazide legati al deficit di vitamina B6
Reazioni cutanee Tossicità neurologica: neurite periferica convulsioni anomalie mentali Tossicità ematologica: anemia

22
DIFFERENZE FARMACOGENETICHE NELL’INATTIVAZIONE DELL’ISONIAZIDE

24
FARMACI ANTITUBERCOLARI:
FARMACI DI I LINEA: rifamicine

25
FARMACI ANTITUBERCOLARI
Rifamicine Meccanismo d’azione: inibizione della RNA-polimerasi DNA dipendente blocco dell’inizio della sintesi proteica

26
STRUTTURA DELLA RNA POLIMERASI BATTERICA
Fig. 5. Assembly and function of the RNA polymerase subunits. During assembly of the RNA polymerase holoenzyme the subunit initiates assembly, which proceeds as shown –– the order of assembly of the polymerase is shown at the top of the figure. The subunit also has a function in transcriptional activation at some promoters, interacting with an upstream element (UP) or with transcription factors (TF). The subunit has a role in nucleotide binding, while ' is involved in DNA template binding. The subunit is responsible for promoter recognition and initiation.
 or with transcription factors (TF). The subunit has a role in nucleotide binding, while is involved in DNA template binding. The subunit is responsible for promoter recognition and initiation.")
27
DIFFERENZE TRA RNA POLIMERASI BATTERICA
E RNA POLIMERASI DEGLI EUCARIOTI I batteri esprimono una sola forma di RNA “polivalente” Gli eucarioti esprimono tre diverse RNA polimerasi La RNA polimerasi batterica è costituita da 5 subunità Ognuna delle RNA polimerasi eucariotiche ha una struttura quaternaria assai più complessa (p.e. la RNA polimerasi II è costituita da 8-12 subunità) Fig. 5. Assembly and function of the RNA polymerase subunits. During assembly of the RNA polymerase holoenzyme the subunit initiates assembly, which proceeds as shown –– the order of assembly of the polymerase is shown at the top of the figure. The subunit also has a function in transcriptional activation at some promoters, interacting with an upstream element (UP) or with transcription factors (TF). The subunit has a role in nucleotide binding, while ' is involved in DNA template binding. The subunit is responsible for promoter recognition and initiation.
 Fig. 5. Assembly and function of the RNA polymerase subunits. During assembly of the RNA polymerase holoenzyme the subunit initiates assembly, which proceeds as shown –– the order of assembly of the polymerase is shown at the top of the figure. The subunit also has a function in transcriptional activation at some promoters, interacting with an upstream element (UP) or with transcription factors (TF). The subunit has a role in nucleotide binding, while is involved in DNA template binding. The subunit is responsible for promoter recognition and initiation.")
28
FARMACI ANTITUBERCOLARI
Rifamicine IMPORTANTE: la RIFAMPICINA è in grado di indurre l’attività degli enzimi microsomiali epatici E QUINDI …… … può dare luogo a interazioni con altri farmaci

29
FARMACI ANTITUBERCOLARI
FARMACI DI I LINEA

30
FARMACI ANTITUBERCOLARI
Etambutolo Meccanismo d’azione: blocco delle arabinosiltransferasi implicate nella sintesi della parete cellulare

31
FARMACI ANTITUBERCOLARI
FARMACI DI I LINEA

33
FARMACI ANTITUBERCOLARI
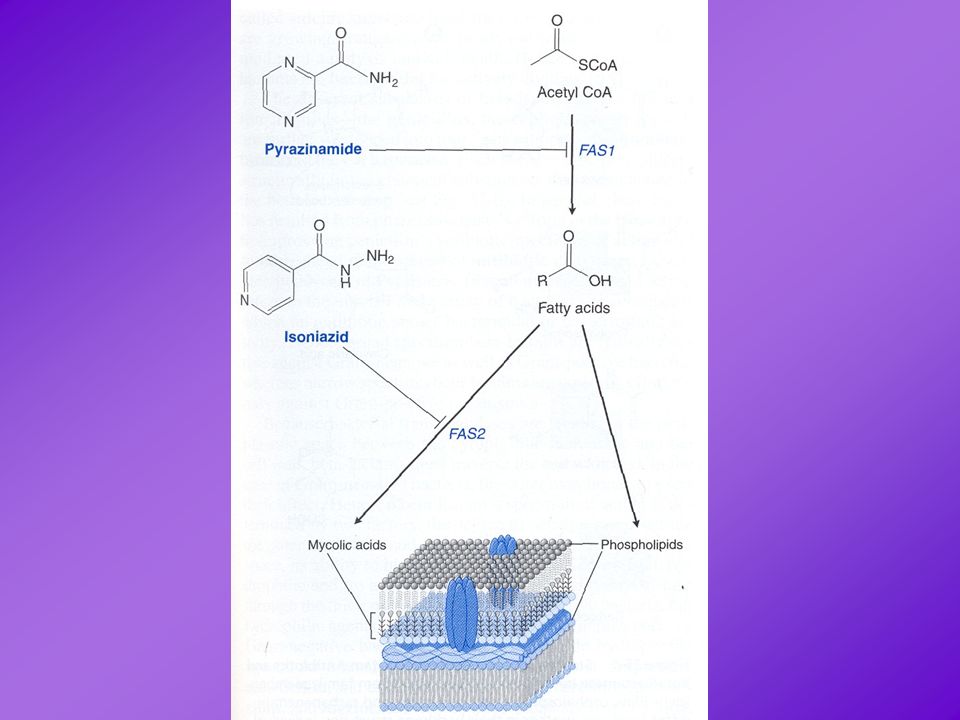
Pirazinamide Meccanismo d’azione: blocco della acido grasso sintetasi I (FAS I), implicata nella sintesi dei precursori degli acidi micolici; è un profarmaco che viene attivato a pH acido Effetti collaterali: epatotossicità escrezione di acido urico
, implicata nella sintesi dei precursori degli acidi micolici; è un profarmaco che viene attivato a pH acido. Effetti collaterali: epatotossicità. escrezione di acido urico.")
34
FARMACI ANTITUBERCOLARI
FARMACI DI I LINEA: Isoniazide Rifampicina Etambutolo Pirazinamide Streptomicina

35
FARMACI ANTITUBERCOLARI
DOTS: directly observed treatment, short-course I FASE: isoniazide/rifampicina/etambutolo/pirazinamide per 2 mesi II FASE: isoniazide/rifampicina per 4 mesi

36
FARMACI ANTITUBERCOLARI
FARMACI DI II LINEA: fluorochinoloni etionamide cicloserina acido aminosalicilico (PAS) amikacina, kanamicina (aminoglicosidi) capreomicina
 amikacina, kanamicina (aminoglicosidi) capreomicina.")
37
TERAPIA PROFILATTICA CON AGENTI ANTITUBERCOLARI
Per chi è indicata? Individui esposti al M. tuberculosis che non presentano segni di infezione Individui che pur essendo stati infettati non presentano segni di malattia Individui con una storia di TB, in cui la malattia è in un dato momento inattiva Individui immunocompromessi

Presentazioni simili