Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Approcci Standard ed Innovativi alla Terapia del Tumore della Mammella
…conoscere il problema per affrontarlo con chiarezza e serenità

2
Le domande ■ Perché devo fare la chemioterapia dopo l’intervento?
■ Perché non basta la pillola che prende la mia amica? ■ Mia figlia è a rischio aumentato di tumore? ■ La chemioterapia danneggia le persone? ■ Avete trovato la cura per i tumori? ■ Potrò fare figli dopo? ■ Perché a me? ■ Guarirò? ■ …….. ■ ….. ■ … ■ .

3
Cos’è il Cancro? Cos’è il cancro? Cosa causa il cancro?
Come si diagnostica? Quale legame tra geni e cancro? Può essere prevenuto? Cancer is a renegade system of growth that originates within a patient’s biosystem, more commonly known as the human body. There are many different types of cancers, but all share one hallmark characteristic: unchecked growth that progresses toward limitless expansion. It is difficult to imagine anyone who has not heard of this illness. Most people have been affected because either they or their loved ones or friends are cancer survivors. Because cancer is so prevalent, people have many questions about its biology, detection, diagnosis, possible causes, and strategies for prevention.

4
Potenzialità replicative Refrattarietà a segnali
Caratteristiche di una Cellula Tumorale Indipendenza dai segnali di crescita Potenzialità replicative illimitate Invasività & metastasi Neo-angiogenesi Capacità di eludere l’apoptosi Refrattarietà a segnali inibenti la crescita

5
Crescita incontrollata
Perdita del Normale Controllo della Crescita Crescita cellulare neoplastica 1 mutazione Crescita incontrollata Morte Non riparazione Normale controllo della crescita 2 mutazione 3 mutazione x mutazione Cancer arises from a loss of normal growth control. In normal tissues, the rates of new cell growth and old cell death are kept in balance. In cancer, this balance is disrupted. This disruption can result from uncontrolled cell growth or loss of a cell’s ability to undergo cell suicide by a process called“apoptosis.” Apoptosis, or “cell suicide,” is the mechanism by which old or damaged cells normally self-destruct.

6
La progressione neoplastica
Progressione Tumorale Benign (not cancer) tumor cells grow only locally and cannot spread by invasion or metastasis Tempo Tumore in situ non invasivo Tumore invasivo Angiogenesi Invasione vascolare La progressione neoplastica richiede anni Depending on whether or not they can spread by invasion and metastasis, tumors are classified as being either benign or malignant. Benign tumors are tumors that cannot spread by invasion or metastasis; hence, they only grow locally. Malignant tumors are tumors that are capable of spreading by invasion and metastasis. By definition, the term “cancer” applies only to malignant tumors. Non origina mestastasi Può originare mestastasi
 tumor cells grow only locally and cannot spread by invasion or metastasis. Tempo. Tumore in situ. non invasivo. Tumore invasivo. Angiogenesi. Invasione vascolare. La progressione neoplastica. richiede anni. Depending on whether or not they can spread by invasion and metastasis, tumors are classified as being either benign or malignant. Benign tumors are tumors that cannot spread by invasion or metastasis; hence, they only grow locally. Malignant tumors are tumors that are capable of spreading by invasion and metastasis. By definition, the term cancer applies only to malignant tumors. Non origina mestastasi. Può originare mestastasi.")
7
Screening Mammografico
La mammografia di screening può diagnosticare la malattia in fase pre-invasiva Breast cancer can sometimes be detected in its early stages using a mammogram, an X-ray of the breast. Mammography is most beneficial for women as they age and undergo menopause. Mammography is a screening tool that can detect the possible presence of an abnormal tissue mass. By itself, it is not accurate enough to provide definitive proof of either the presence or the absence of breast cancer. If a mammogram indicates the presence of an abnormality, further tests must be done to determine whether breast cancer actually is present.

8
Terapia adiuvante una Malattia Sistemica
Il Tumore della Mammella è spesso una Malattia Sistemica Micrometastasi Metastasi cliniche Dopo l’intervento Terapia adiuvante

9
Tessuto Neoplastico I tumori sono spesso caratterizzati da peculiari aspetti istologici ► Caratteristiche biologiche

10
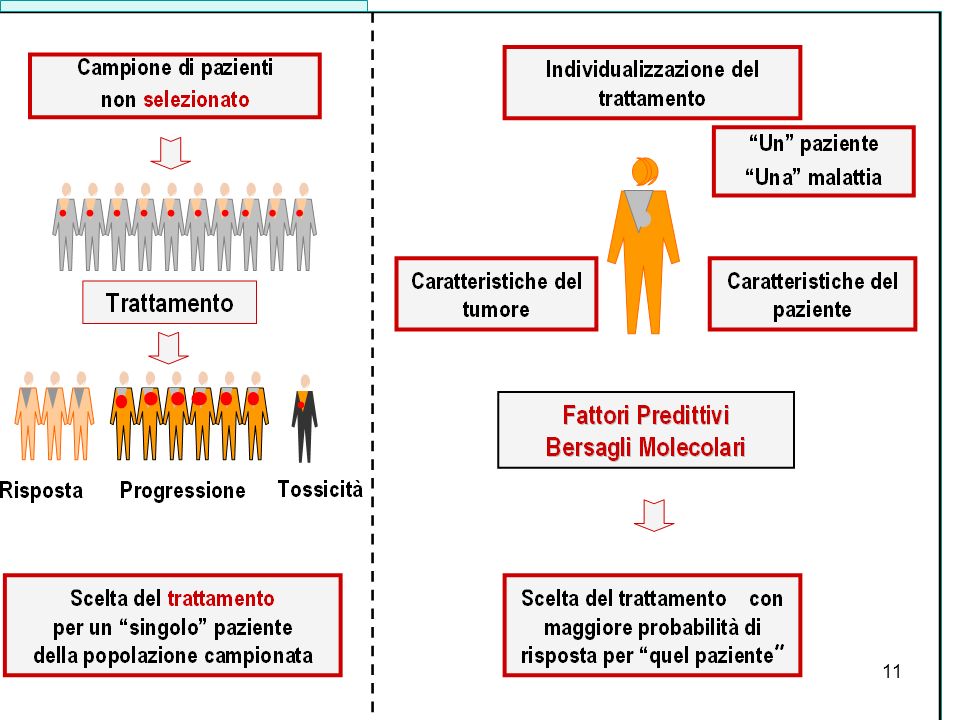
Scelta personalizzata della terapia
■ Chemioterapia ■ Ormonoterapia ■ Terapie biologiche Il carcinoma mammario è una malattia eterogenea ■ Efficacia ■ Effetti collaterali I trattamenti non sono ugualmente efficaci e tossici in tutte le pazienti Scelta personalizzata della terapia

12
HER-2/NEU Bersaglio Molecolare
Fattore di crescita Recettore HER2 IHC Carcinoma mammario Herceptin is a good example of a pharmacogenomics success story. In the 1980s, researchers discovered that some women who had particularly fast-growing breast cancers expressed extra copies of a gene called Her-2/neu. The genes were producing many copies of a protein that appeared to be driving the growth of the cancer cells. Proliferazione Gene Her-2/neu FISH

13
Un Anticorpo chiamato Herceptin
La crescita rallenta Herceptin blocca i recettori In the early 1990s, an antibody was developed that latches onto the her-2/neu proteins on the surface of a cancer cell. It stops the proteins from spurring on cancer-cell growth, and through this “stop signal” can also stop propagation of survival signals within the cancer cell. Some women who were given the experimental antibody saw their cancer growth slow or stop altogether when their Herceptin treatment was combined with cytotoxic chemotherapy. Herceptin was approved by the Food and Drug Administration in late 1998 as therapy for women who test positive for high levels of the her-2/neu protein (about 25 to 30 percent of all breast cancer patients).
.")
14
HER2+ HER2- RE+ RE- 20% ■ Sensibilità intermedia a CT
■ Sensibilità intermedia a OT ■ Sensibilità intermedia a HCT ■ Massima sensibilità a CT ■ Non sensibilità OT ■ Massima sensibilità a HCT ■ Non sensibilità a HCT ■ Massima sensibilità a OT ■ Moderata sensibilità CT “Triplo negativi” “Luminali A” “Luminali B” HER2+ RE+ 70% RE-

15
70% HER2+ HER2- RE+ RE- 20% ■ Sensibilità intermedia a CT
■ Sensibilità intermedia a OT ■ Sensibilità intermedia a HCT ■ Massima sensibilità a CT ■ Non sensibilità OT ■ Massima sensibilità a HCT ■ Non sensibilità a HCT ■ Massima sensibilità a OT ■ Moderata sensibilità CT “Triplo negativi” “Luminali A” “Luminali B” HER2+ RE+ 70% RE-

16
HER2+ HER2- RE+ RE- 20% ■ Sensibilità intermedia a CT
■ Sensibilità intermedia a OT ■ Sensibilità intermedia a HCT ■ Massima sensibilità a CT ■ Non sensibilità OT ■ Massima sensibilità a HCT ■ Non sensibilità a HCT ■ Massima sensibilità a OT ■ Modesta sensibilità CT “Triplo negativi” “Luminali A” “Luminali B” HER2+ RE+ 70% RE-

17
HER2+ HER2- RE+ RE- 20% ■ Sensibilità intermedia a CT
■ Sensibilità intermedia a OT ■ Sensibilità intermedia a HCT ■ Massima sensibilità a CT ■ Non sensibilità OT ■ Massima sensibilità a HCT ■ Non sensibilità a HCT ■ Massima sensibilità a OT ■ Moderata sensibilità CT “Triplo negativi” “Luminali A” “Luminali B” HER2+ RE+ 70% Prognosi sfavorevole, Recidive precoci e tardive Prognosi sfavorevole Recidive precoci Aggressiva, recidive precoci Agenti anti-HER2 aumentano OS Indolente, buona prognosi Recidive tardive RE-

18
La Trasduzione del Segnale
FTs PIK3 Ras AKT Raf mTOR MAPK HER2 NFB TKs cKit RE VEGF PDGF Sopravvivenza Proliferazione

19
Trattamento personalizzato
La Trasduzione del Segnale Tipifarnib Lonafarnib Everolimus Temsirolimus LI294002 Bortezomib Tamoxifen Inibitori Aromatasi GSK690693 Imatinib Sunitinib Herceptin Panerb Erlotinib Gefitinib Lapatinib Gefitinb Sunitinib Imatinib Genisteina Sorafenib PD AZD 6244 Bevacizumab RE HER2 PDGF VEGF NFB cKit FTs TKs Trattamento personalizzato PIK3 Ras AKT Raf mTOR MAPK Sopravvivenza Proliferazione Angiogenesi

20
Variabili che Influenzano la Possibilità di Guarigione
■ Stadio di malattia ■ Caratteristiche genetiche e biologiche ■ Adeguatezza del trattamento ■ Condizioni associate alla paziente

21
Lo stadio è la variabile prognostica
Stadio di Malattia Mammella Ghiandole linfatiche Altri organi Stadio 1 Stadio 2 Stadio 4 Guaribile Curabile Lo stadio è la variabile prognostica più importante

22
Terapie per il Carcinoma Mammario
Loco-regionali Sistemiche ■ Chirurgia ■ Radioterapia ■ Chemioterapia ■ Ormonoterapia ■ Terapie biologiche Quando indicata, la chirurgia conservativa + RT ottiene una sopravvivenza sovrapponibile alla chirurgia radicale La terapia medica precauzionale migliora la sopravvivenza

23
Fasi di applicazione del trattamento sistemico
FASE MALATTIA OBIETTIVO PREVENZIONE NO Prevenzione primaria ADIUVANTE LOCALIZZATA Prevenzione metastasi GUARIGIONE PRIMARIA LOCALMENTE Controllo locale AVANZATA Prevenzione metastasi GUARIGIONE TERAPEUTICA METASTATICA Qualità vita Regressione tumore Prolungamento sopravvivenza PALLIAZIONE

24
Milan Cancer Institute Across Studies Results
1.0 Anni ’90 Taxani .75 Anni ’80 Antracicline Probability Relapse-Free Anni’70 CMF .50 Chirurgia Popolazione non selezionata .25 1 2 3 4 5 years

25
adiuvante Resistenti Sensibili Recidive Guarite con chirurgia a 5 anni
40% 60% Recidive 20% 40% 40% a 5 anni

26
Selezione Convenzionale
Definizione del rischio ■ Stato dei linfonodi ■ Dimensioni del tumore ■ Età ■ Indici cinetici ■ Recettori Ormonali ■ Stato di HER2 Identificazione subottimale dei pazienti a rischio Potere predittivo limitato Selezione del trattamento

27
Selezione del Trattamento
Biopsia A B C

28
Fasi di Applicazione del Trattamento Sistemico
FASE MALATTIA OBIETTIVO PREVENZIONE NO Prevenzione primaria ADIUVANTE LOCALIZZATA Prevenzione metastasi GUARIGIONE PRIMARIA LOCALMENTE Controllo locale AVANZATA Prevenzione metastasi GUARIGIONE TERAPEUTICA METASTATICA Qualità vita Regressione tumore Prolungamento sopravvivenza PALLIAZIONE

29
Studio ECTO Chirurgia Conservativa vs T iniziale
Criteri stratificazione ■ T clinico ■ RE/PgR ■ Centro 1 Chirurgia Primaria Chemioterapia Primaria p < 0.001 7 5 5 2 5 <3 3.1-4 4.1-5 >5 Dimensioni tumorali (cm) Gianni, 2009
 Gianni,")
30
Risposta Patologica pCR NR PR anni 20-25% Bonadonna, 2002

31
alla diagnosi e (?) alla recidiva
Adiuvante CH → CT Anni Evento Molti pazienti Costi elevati Ricerca: complessa NeoAdiuvante CT → CH Sett Risposta patologica Pochi pazienti Mesi Costi contenuti Ricerca: obiettivo Tessuto pre-post terapia alla diagnosi e (?) alla recidiva
 alla recidiva.")
32
Pathological Response: ITT (%)
Malattia HER2+ 43% 23% 17% 38% 20% 16 % HER2+ + H HER2- pCR t pCR p=0.002 p=0.003 p=0.29 p=0.43 Gianni, 2008

33
Vantaggio di Sopravvivenza nella Popolazione con Incremento di pCR
■ CT + H ■ CT HER2+ 1.00 0.75 0.50 0.25 0.00 6 12 18 24 30 36 42 Probability EFS Months Events HR 0.56 p value 0.006 0.55 0.0062 Patients unadjusted adjusted Gianni, 2008 33

34
NeoSphere pCR Rates ITT Population Summary
50 40 30 pCR, % 95% CI 20 10 29.0 45.8 16.8 24.0 H, trastuzumab; P, pertuzumab; T, docetaxel TH THP HP TP 6 Gianni 2010

35
A B Memo per Paziente 1 Mammografia /Ecografia/ Biopsia …………………………………
Da consegnare alla segretaria Q1 per prenotazioni ■ Sig.ra………………………………. DATA………………………. 1 Mammografia /Ecografia/ Biopsia ………………………………… Radiologia senologica, Settore x, Piano x 2 Visita collegiale ……………………………….. Settore y, piano +1, ore 8.30 Accettazione Segreteria y 3 Stadiazione RX torace .………………………………… Scintigrafia ossea …………………………………. Ecografia addome …………………………………. Visita cardiologica …………………………………. Esami ematologici ...………………………………. Altro……… ………………………………… 4 Visita oncologia medica ...………………………………. Prericovero ………………………………… CALL CENTER………………… I, G, RE, PGR, HER2, Mib TNM, CP vs CH Data diagnosi Data terapia Maschera PC A B Copia per pz, cartella

36
Informazioni a paziente
Prima Visita Visita Collegiale ■ Segreteria Radiologia A. patologica 2-11 giorni 7 giorni Indicazioni di cura Chirurgia Chemioterapia Stadiazione Call center Informazioni a paziente

37
Probabilità di Sviluppare il Tumore della Mammella Entro i 65 Anni
BRCA1 alterato 1 2 3 4 5 6 7 8 10 20 30 40 50 60 70 80 90 100 BRCA1 normale I tests genetici identificano la mutazione, non la malattia La mutazione BRCA spiega solo il 5% dei tumori della mammella An accurate gene test can tell if a mutation is present, but that finding does not guarantee that disease will develop. For example, women with the BRCA1 breast cancer susceptibility gene have an 80 percent chance of developing breast cancer by the age of 65. The risk is high but not absolute. And family members who test negative for the BRCA1 mutation are not exempt from breast cancer risk; over time, they can acquire breast cancer-associated genetic changes at the same rate as the general population.

38
Counseling Genetico ■ Identificazione paziente Psicologo Clinico
Genetista ■ Consulenza/ Test Genetista, biologo molecolare ■ Consegna test (paziente, familiari) Genetista, oncologo, chirurgo, ginecologo, psicologo ■ Tempo sufficiente per valutare ■ Discussione preliminare con almeno due figure professionali ■ Separatamente
 Genetista, oncologo, chirurgo, ginecologo, psicologo. ■ Tempo sufficiente per valutare. ■ Discussione preliminare con almeno. due figure professionali. ■ Separatamente.")
39
Approccio multidisciplinare Strutture di alto profilo
Miglioramento delle conoscenze come presupposto per il miglioramento ■ Delle terapie ■ Della prognosi Ricerca come dovere per il beneficio del paziente ■ Data base clinici ■ Data base molecolari Studi clinici come strumento di miglioramento della prognosi ■ Accessibilità a trattamenti innovativi ■ Tutela del paziente Approccio multidisciplinare Strutture di alto profilo

40
Qualità e indipendenza della ricerca
Presidente Gianni Bonadonna Qualità e indipendenza della ricerca

42
Le caratteristiche molecolari influenzano la storia della malattia
e il suo trattamento

43
Negli esseri umani il genoma è omologo nell’99%
Il Codice Genetico “Il libro” Negli esseri umani il genoma è omologo nell’99% Il libro 23 cromosomi (geni) (= i capitoli) I capitoli x 106 nucleotidi (= le lettere) Contenuto nel nucleo della cellula In quasi tutte le cellule
 (= i capitoli) I capitoli x 106 nucleotidi (= le lettere) Contenuto nel nucleo della cellula. In quasi tutte le cellule.")
44
La maggior parte silente
Progetto Genoma Umano geni La maggior parte silente Identifying genes associated with disease--indeed, tracking down every chemical base in each of the estimated 25,000 genes as well as the spaces between them, a process called mapping the human genome--has been accomplished successfully by an international collaboration known as the Human Genome Project. Scientists have developed a consensus sequence, laying out the order in which all the human genes sit along the chromosomes. This information can be used to determine where gene mutations occur in specific diseases. For example, here is a chart of disease-linked genes located along the X chromosome. Cromosoma X

45
DNA Geni DNA Chromosomes Cell Nucleus ■ Membrana ■ Nucleo ■ Citoplasma
The story of gene testing begins with DNA. DNA is a vast chemical information database. It resides in the core, or nucleus, of each of the body’s trillions of cells, and it carries the complete set of instructions for making all the proteins a cell will ever need.

46
DNA->RNA->Proteine
Nucleus DNA mRNA Proteine Ribosoma Aminoacidi Building proteins lies at the heart of cell function. For a cell to make a protein, the information from a gene is copied, base by base, from a strand of DNA into a strand of messenger RNA. Messenger RNA travels out of the nucleus into the cytoplasm, to cell organelles called ribosomes. There, messenger RNA directs the assembly of amino acids that fold into a completed protein molecule.

47
DNA Alterato = Proteina Alterata
Nucleus Proteine Amino acidi Ribosoma DNA mRNA Gene When a gene contains a mutation, the protein encoded by that gene is likely to be abnormal. Sometimes the protein will be able to function, but imperfectly. In other cases, it will be totally disabled. The outcome depends not only on how it alters a protein’s function but also on how vital that particular protein is to survival.

Presentazioni simili













>")






