Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
TERAPIA ELETTRICA DELLE ARITMIE
Pistoia, 12 ottobre 2013 Dr Alberto Mandorll U.O.CARDIOLOGIA, Osp.S.Jacopo Pistoia

2
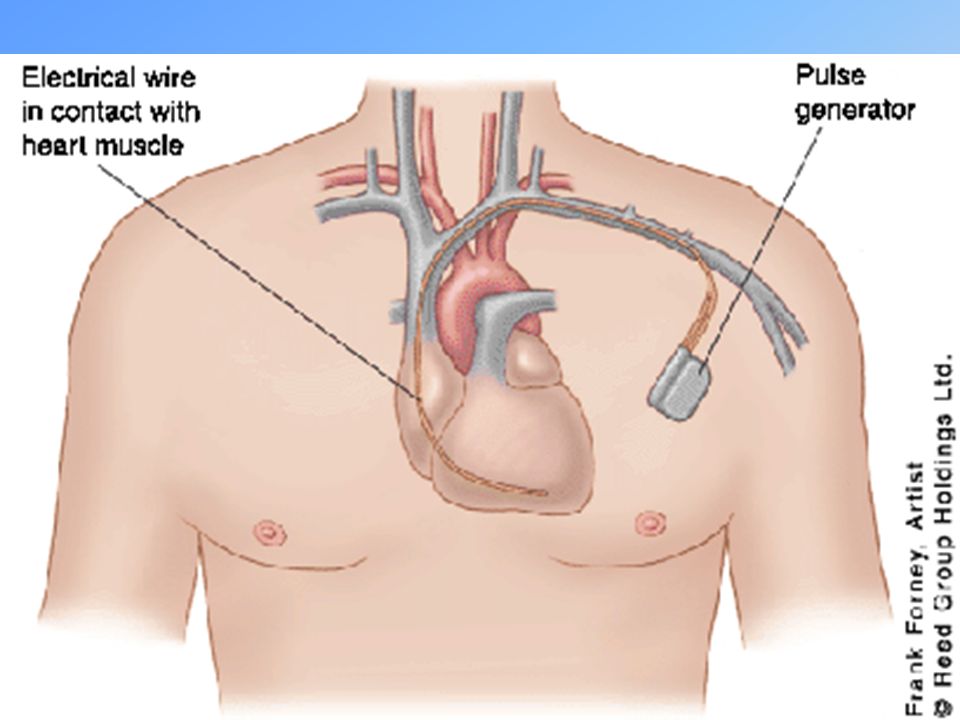
Componenti di un Sistema di Cardiostimolazione
Elettrocatetere Dispositivo Programmatore

3
L’elettrocatetere Meccanismo di Fissaggio Corpo dell’elettrocatetere
Connettore Elettrodo Corpo dell’elettrocatetere Meccanismo di Fissaggio

4
Stimolazione Ventricolare
Sistema Monocamerale A seconda del problema da trattare, può essere necessario impiantare un solo elettrocatetere… Stimolazione atriale Stimolazione Ventricolare ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

5
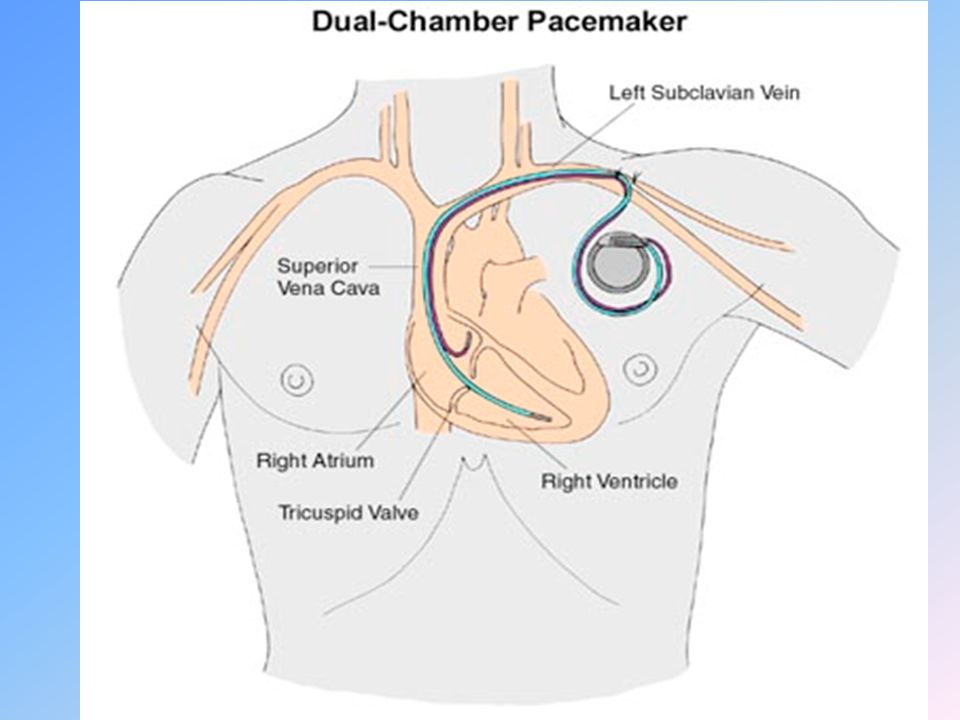
Sistema bicamerale doppio catetere
…Oppure può essere necessario impiantare due elettrocateteri Vantaggio sincronia AV

6
Sistema Bicamerale Monocatetere
VDD Viene utilizzato un unico catetere (Monocatetere), fissato in ventricolo, che presenta un dipolo atriale flottante in grado di rilevare i segnali atriali endocavitari.
, fissato in ventricolo, che presenta un dipolo atriale flottante in grado di rilevare i segnali atriali endocavitari.")
8
IMPIANTO (Tecnica di Accesso Venoso)
")
9
Pace-maker

10
Implantable-cardioverter defibrillator (ICD)
")
11
Cardiac Resynchronization Therapy (CRT)
")
12
Lo SPIKE di stimolazione
Caratteristiche: Ampiezza Durata Volts ms

13
Malattia del nodo seno-atriale

14
Malattia del nodo seno-atriale

15
Stimolazione Ventricolare
Sistema Monocamerale A seconda del problema da trattare, può essere necessario impiantare un solo elettrocatetere… Stimolazione atriale Stimolazione Ventricolare ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

16
Malattia del nodo seno-atriale

17
Blocco Atrio-Ventricolare

18
Sistema bicamerale doppio catetere
Vantaggio sincronia AV

19
Blocco atrio.ventricolare

20
Pacing nel Blocco AV

21
Pacing nel Blocco AV

22
Fibrillazione Atriale

23
Fibrillazione atriale bradicardica

24
Stimolazione Ventricolare
Sistema Monocamerale A seconda del problema da trattare, può essere necessario impiantare un solo elettrocatetere… Stimolazione atriale Stimolazione Ventricolare ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

25
Pacemker monocamerale in VVI

27
Cos’è un AICD? Defibrillazione + Automaticità AICD Pacemaker + =

28
Algoritmi di discriminazione
Come ragiona un ICD ATP Shock Frequenza AGC Durata Riconferma Riconoscimento Trattamento Diagnostica Selezione Algoritmi di discriminazione

29
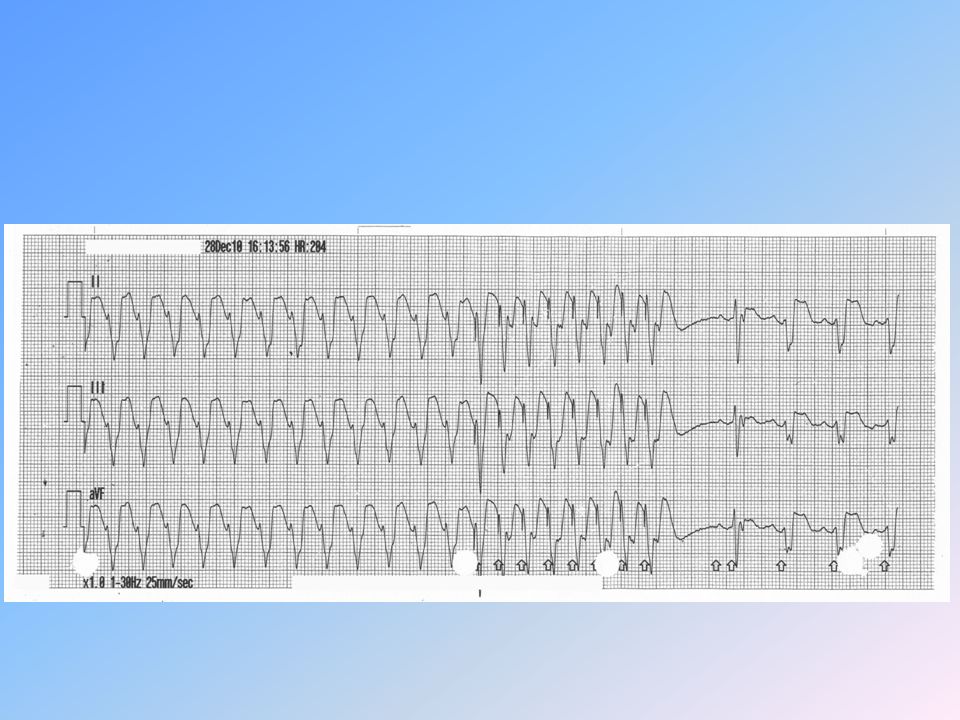
TV risolta con ATP TV Onset Evento Frequenza A media 79 min¯¹
Frequenza V media 175 min¯¹ Rilevazione Rhythm ID Rilevazione Frequenza A media 86 min¯¹ Frequenza V media 170 min¯¹ zona di frequenza; TV Stabilità 2 ms Frequenza V>A Vero AFib Falso RhythmID correlato Falso SRD soddisfatto Falso Timeout ATP Falso Tentat. 1, Rampa V ATP Tempo trascorso 00:00:06 Informazioni ATP Numero raffiche 1 Event term.: 00:00:19

30
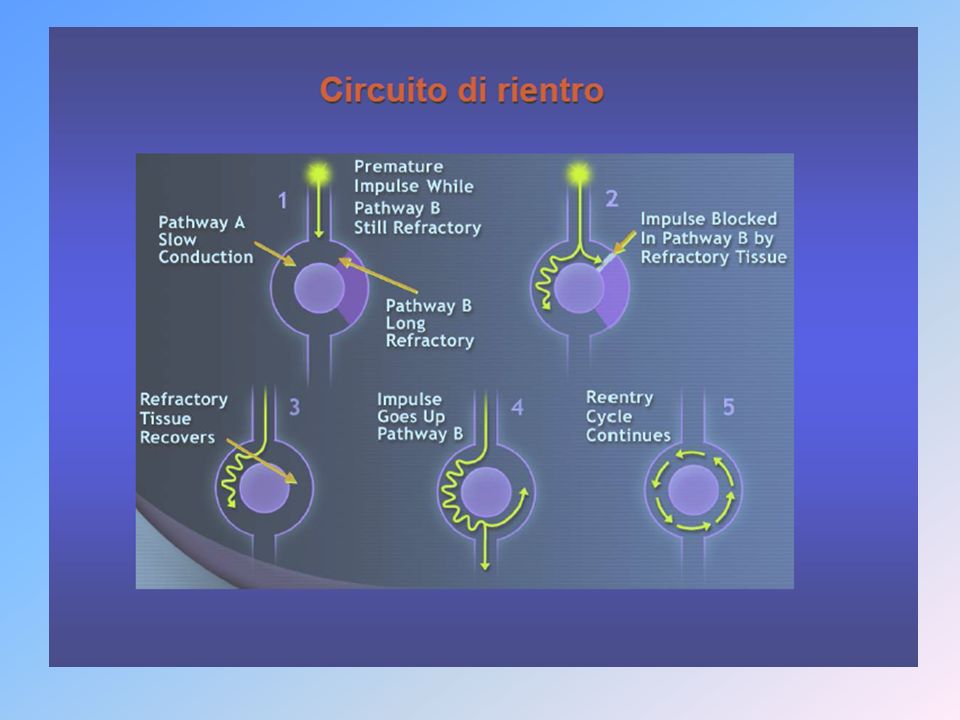
Circuito di Rientro

32
Terapia antitachicardica erogata con successo su
di un episodio di tachicardia ventricolare Tracciato EGM in memoria Pacing

35
Catetere quadripolare pacing, sensing e due coil di defibrillazione
Lo shock Catetere bipolare atriale pacing e sensing Catetere quadripolare ventricolare pacing, sensing e due coil di defibrillazione SHOCK TRIPOLARE

36
Tracciato ECG di superficie
Tracciato EGM endocavitario “Marche di riferimento” fibrillazione ventricolare ritmo sinusale shock (30J)
")
37
Implantable-cardioverter defibrillator (ICD)
")
38
Principali problemi nel paziente portatore di ICD

39
Problematiche nei pazienti impiantati con ICD
Errori di detection (Undersensing and Non detection / Re-detection) Terapie inefficaci o pro-aritmiche Shock inappropriati/non necessari Malfunzionamenti dei device o degli elettrocateteri Cluster shock e tempeste aritmiche What’s trobleshooting? It’s anything that can go wrong with a cardiac defibrillator, from its implant to its elective replacement. It includes…..Shoul we add a couple of things to the list, infections and any shock……we could also refer to this list of problems as the MORBIDITY of ICDs
 Terapie inefficaci o pro-aritmiche. Shock inappropriati/non necessari. Malfunzionamenti dei device o degli elettrocateteri. Cluster shock e tempeste aritmiche. What’s trobleshooting It’s anything that can go wrong with a cardiac defibrillator, from its implant to its elective replacement. It includes…..Shoul we add a couple of things to the list, infections and any shock……we could also refer to this list of problems as the MORBIDITY of ICDs.")
40
1. Undersensing di TV ICD: Prizm DR Esempio di undersensing di tachicardia ventricolare dovuto ad programmazione della frequenza di cut-off

41
Esempi di undersensing dovuto ad alternanza di picchi alto-basso-alto
1. Errori detection Esempi di undersensing dovuto ad alternanza di picchi alto-basso-alto 41

42
2. Terapie inefficaci ICD: Prizm VR In questa diapositiva e nelle successive viene riportato l’EGM dell’episodio numero3. Qui si vede l’onset, la durata e la carica dei condensatori relativi al primo shock erogato (quello per cui il device ha segnalato una corto circuito). La detection e la durata sono soddisfatte e l’eipsodio in corso è una TV molto veloce che per il cut off di frequenza programmato viene classificata come FV EGM dell’episodio. Onset dell’episodio, durata e carica dei condensatori: riconoscimento e durata FV soddisfatte
. La detection e la durata sono soddisfatte e l’eipsodio in corso è una TV molto veloce che per il cut off di frequenza programmato viene classificata come FV. EGM dell’episodio. Onset dell’episodio, durata e carica dei condensatori: riconoscimento e durata FV soddisfatte.")
43
3. Shock inappropriati/non necessari

44
Quando un defibrillatore NON deve intervenire
Non trattare questi tipi di ritmo

45
Quando un defibrillatore NON deve intervenire
Non trattare questi tipi di ritmo 45

46
Noise TENS (Transcutaneous Elettrical Nerve Stimulation)
")
47
5. Tempeste aritmiche Tempesta elettrica
intervento ICD su TV-FV = > 3 nelle 24 h

48
Ablazione fibrillazione atriale
Fibrillazione atriale parossistica Isolamento elettrico vene polmonari (trigger a partenza vene polmonari) Fibrillazione atriale persistente (dilatazione e fibrosi) Isolamento elettrico vene polmonari, ablazione potenziali elettrici frammentati, lesioni lineari istmo mitralico e parete posteriore atrio sx
 Fibrillazione atriale persistente (dilatazione e fibrosi) Isolamento elettrico vene polmonari, ablazione potenziali elettrici frammentati, lesioni lineari istmo mitralico e parete posteriore atrio sx.")
49
Fibrillazione atriale Ablazione

50
Fibrillazione Atriale

51
Atrial Fibrillation Initiation Mechanism – PV Triggers
Image taken from Mike’s AF brochure…

52
Fibrillazione atriale

53
Ablazione FA

54
How Arctic Front® Balloon Catheter and AchieveTM Work
2. Inflate and position 1. Access targeted vein Arctic Front demonstrates a simple, straightforward approach to PVI which can be obtained in 4 steps. Step 1: Lead your guide wire/Achieve mapping catheter into the targeted vein Step 2: Inflate the Arctic Front balloon in the left atrium. Once inflated, position the balloon at the PV atrum. Step 3: To assure occlusion, inject dye into the targeted pulmonary vein to make sure the vein is completely occluded. Once assured, ablate the PV for 240 seconds (the dosage used in the STOP AF trial). Step 4: Assess pulmonary vein isolation with the Achieve mapping catheter 4. Assess PVI 3. Occlude and ablate 54 54
. Step 4: Assess pulmonary vein isolation with the Achieve mapping catheter. 4. Assess PVI. 3. Occlude and ablate")
55
Gestione fibrillazione atriale tachiardica nel paz. scompensato

56
Catheter Position for AV Node Ablation
To perform ablation of the AV node, the ablation catheter is positioned at the AV node near the tricuspid annulus, and illustrated above. The right sided approach is most commonly used and generally successful. The left-sided approach is used when the right-sided attempt is unsuccessful. A catheter (not shown) is placed in the right ventricle for pacing and recording. Permanent cardiac pacing may be necessary following AV junction ablation. Singer: Interventional Electrophysiology. Williams & Wilkins 1997; 328.
 is placed in the right ventricle for pacing and recording. Permanent cardiac pacing may be necessary following AV junction ablation. Singer: Interventional Electrophysiology. Williams & Wilkins 1997; 328.")
57
Anatomy of the Human Atrioventricular Node
This slide reviews the anatomy of the AV node. The AV node is divided into two regions, the compact AV node and AV nodal tracts. The compact AV node is a button-like portion of the AV node from which the His bundle originates. AV nodal tracts are bands of conductive tissue that gather electrical impulses from the internodal pathways and deliver them to the compact AV node. The AV nodal tracts that converge to form the compact AV node are poorly defined—that is, it is not entirely clear where the internodal pathways end and the AV nodal tracts begin. Thus far, two distinct tracts have been identified: Anterior tract (also called the fast AV nodal pathway) Posterior tract (also called the slow AV nodal pathway) This picture also illustrates the triangle of Koch, and anatomical landmark used to visualize the location of the AV nodal tracts. The three sides of the Koch’s triangle are defined by the tricuspid valve annulus, the tendon of Todaro, and the ostium of the coronary sinus. The fast AV nodal pathway lies near the compact AV node along the tendon of Todaro. The slow AV nodal pathway is located along the tricuspid valve annulus near the ostium of the coronary sinus.
 Posterior tract (also called the slow AV nodal pathway) This picture also illustrates the triangle of Koch, and anatomical landmark used to visualize the location of the AV nodal tracts. The three sides of the Koch’s triangle are defined by the tricuspid valve annulus, the tendon of Todaro, and the ostium of the coronary sinus. The fast AV nodal pathway lies near the compact AV node along the tendon of Todaro. The slow AV nodal pathway is located along the tricuspid valve annulus near the ostium of the coronary sinus.")
58
Stimolazione Ventricolare
Sistema Monocamerale A seconda del problema da trattare, può essere necessario impiantare un solo elettrocatetere… Stimolazione atriale Stimolazione Ventricolare ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

59
Resincronizzazione cardiaca

60
Oblique View of Right Atrium
Superior Vena Cava Crista Terminalis Fossa Ovalis Pectinate Muscle This demonstrates an oblique view of the right atrium and shows some of the crucial structures. The isthmus of tissue responsible for atrial flutter is seen anterior to the orifice of the coronary sinus. The Eustachian ridge is part of the Crista Terminalis that separates the roughened part of the right atrium from the smooth septal part of the right atrium. Eustachian Ridge Orifice of Coronary Sinus Inferior Vena Cava Netter F. Atlas of Human Anatomy. 1989;Plate 208.

61
Seno Coronarico

62
Resincronizzazione cardiaca

63
Resincronizzazione Cardiaca

64
Resincronizzazione cardiaca

65
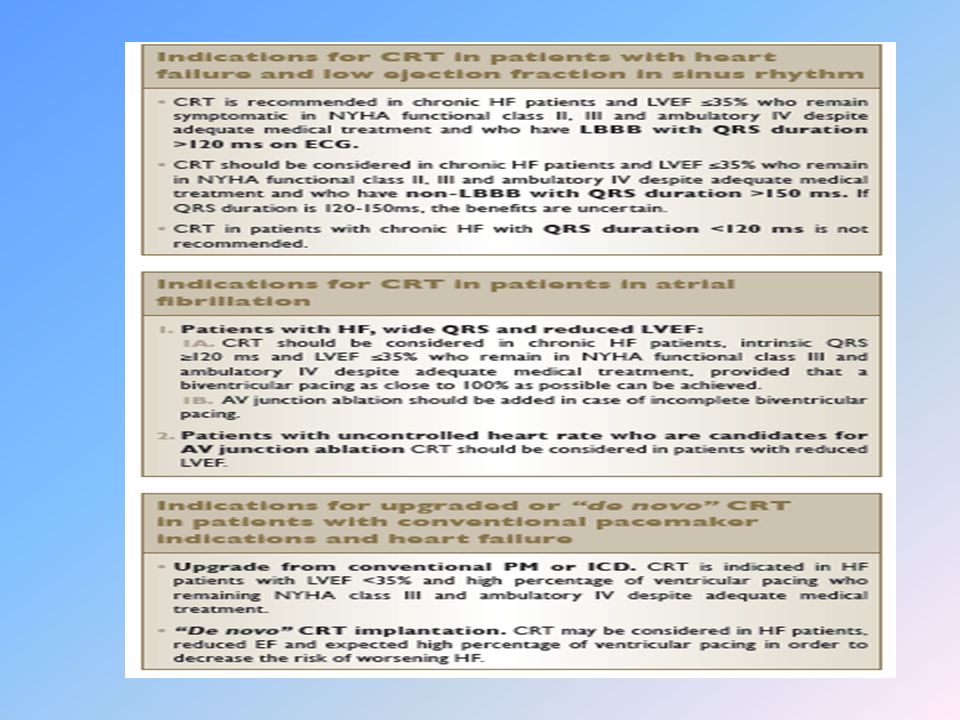
Linee guida europee 2013

Presentazioni simili



 e ATTIVAZIONE ELETTRICA DEL CUORE>")






e mostra un ritmo irregolare che varia continuamente nella forma. La frequenza ventricolare media.>")









