Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
U.O. Neurologia Vascolare A.O. Spedali Civili di Brescia
ICTUS CEREBRI, STENOSI CEREBROVASCOLARI E ULTRASUONI: DIAGNOSI E TERAPIA CON IL DOPPLER TRANSCRANICO Dr A. Costa U.O. Neurologia Vascolare A.O. Spedali Civili di Brescia

4
Indicazioni Visualizzare le occlusioni e le stenosi intracraniche nelle principali arterie Valutare gli effetti emodinamici intracranici in presenza di stenosi o occlusioni extracraniche Monitorare la ricanalizzazione dei vasi intracranici nella fase acuta dell’ictus Monitorare l’emodinamica cerebrale intracranica Dopo emorragia subaracnoidea InIn pazienti con aumentata ICP Durante/dopo procedure di rivascolarizzazione extracranica Endarterectomia carotidea Angioplastica Durante/dopo interventi neuroradiologici Balloon occlusion Coiling of AVM Durante interventi cardiochirurgici Visualizzazione e quantificazione dello shunt destro-sinistro Patent foramen ovale

5
Indicazioni (2) Test funzionali
Stimulazione delle arteriole intra craniche con CO2 o altri farmaci vasoattivi Lateralizzazione del linguaggio prima della neurochirurgia NEW Brain perfusion imaging Trombolisi con ultrasuoni Stratificazione del richio

6
Diagnostic Criteria – Stenosis
Increased flow velocity – generally focal Disturbed flow Turbulence; spectral broadening Covibration phenomena Vibration of the vessel wall & surrounding soft tissue Drop in post-stenotic velocity Changes in post-stenotic waveform morphology Prolonged systolic upstroke Decreased pulsatility

7
Diagnostic Criteria – Occlusion
Absence of arterial signal at expected depth Presence of signals in vessels which communicate with the occluded artery Altered flow in communicating vessels, indicating collateralization

9
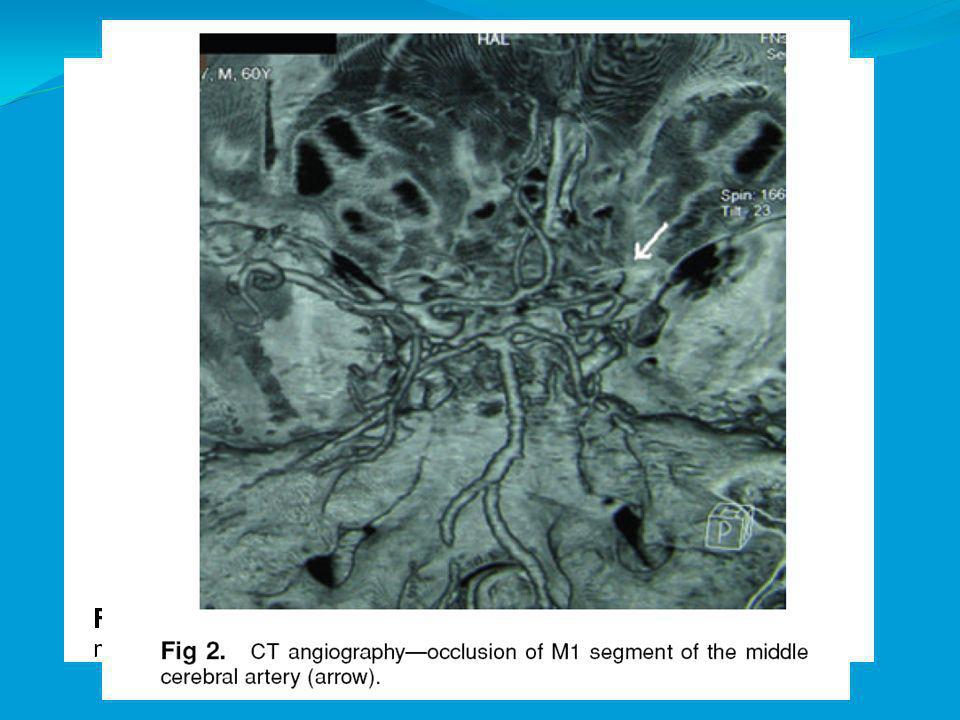
Occlusione Arteria Cerebrale Media M1 - Criteri diagnostici
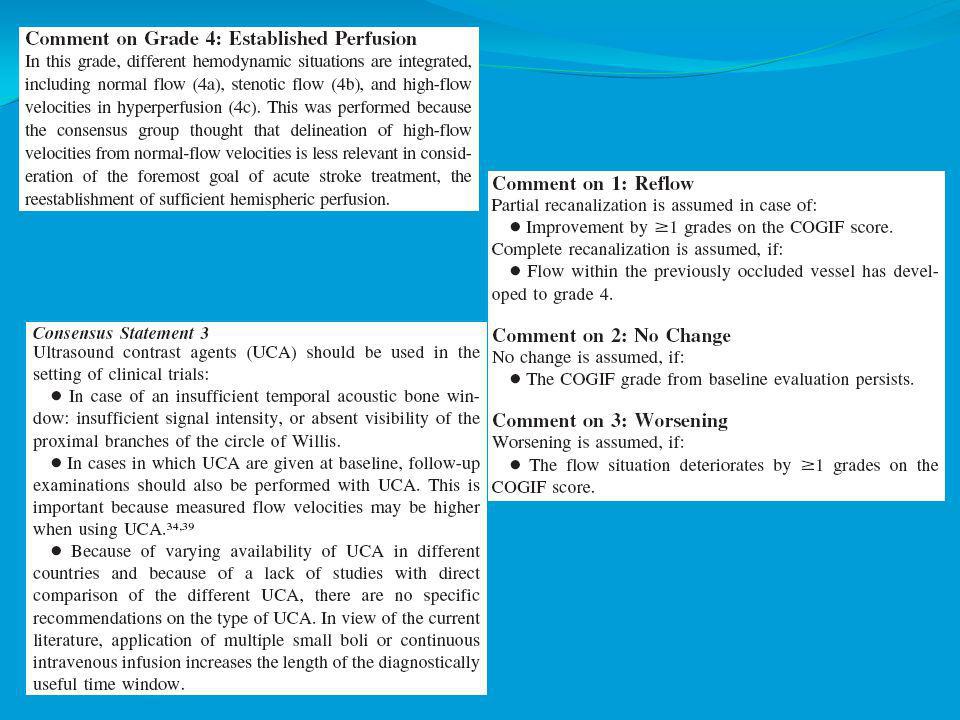
NAIS TCCS Consensus Il segnale di flusso dell’MCA è assente in contemporanea alla visualizzazione delle restanti arterie del circolo anteriore o delle vene profonde cerebrali o del circolo controlaterale Sensibilità % Specificità 90-98%

11
Occlusione ICA a T - Criteri diagnostici
NAIS TCCS Consensus Il segnale di flusso dell’MCA, ICA distale e A1 è assente in contemporanea alla visualizzazione dalla finestra omolaterale di A1 del circolo controlaterale o omolaterale La visualizzazione delle vene profonde cerebrali, di A2 o del circolo controlaterale aumenta la credibilità della diagnosi. Meglio se confermata dalla riduzione della velocità di flusso diastolico sull’ICA cervicale o sulla CCA o dalla presenza di flusso oscillante Sensibilità 70-90% Specificità 90-95%

12
Occlusione segmento distale M1 o di multipli rami di M2- Criteri diagnostici
NAIS TCCS Consensus Differenze del 30% nella velocità di picco sistolico nel segmento prossimale di M1 Velocità di fine diastole inferiore a 26 cm/s e indice di fine diastole inferiore a 2.5 (se >2.5 indice di occlusione M1)(?). Calcolare l’indice di asimmetria se non vi sono alterazioni del flusso lungo l’ICA o M1 bilateralmente. Basse velocità di flusso vanno comunque tenute in considerazione in relazione al beneficio derivante dalla trombolisi Sensibilità 70-90% Specificità 90-95%
( ). Calcolare l’indice di asimmetria se non vi sono alterazioni del flusso lungo l’ICA o M1 bilateralmente. Basse velocità di flusso vanno comunque tenute in considerazione in relazione al beneficio derivante dalla trombolisi. Sensibilità 70-90% Specificità 90-95%")
13
Stenosi M1 (o del segmento distale dell’ICA) – Criteri diagnostici
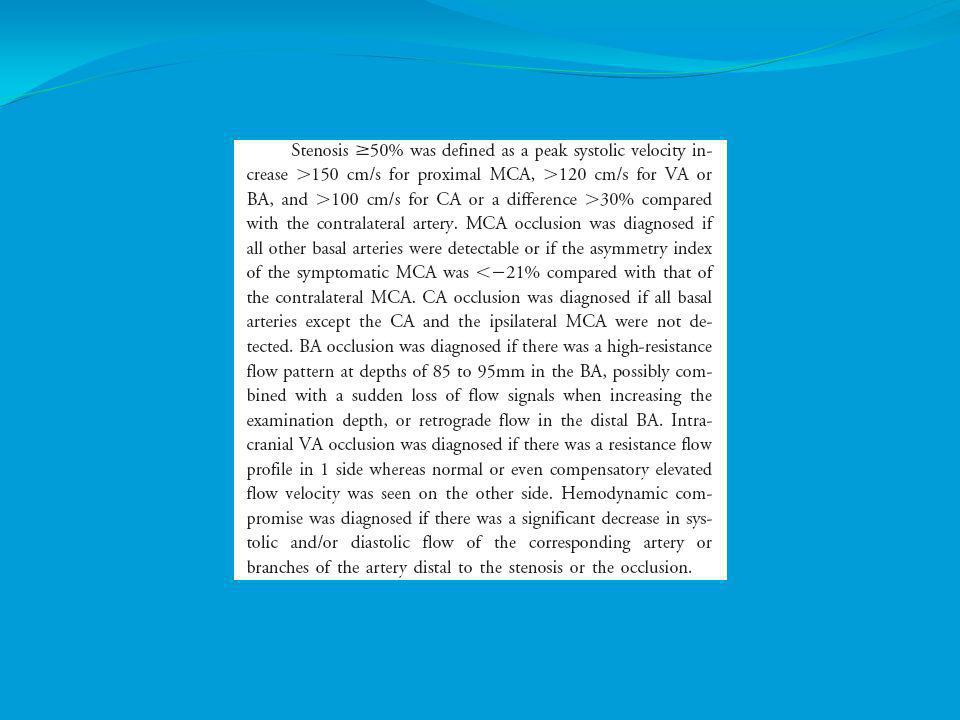
NAIS TCCS Consensus Significativa (cioè superiore al 50%) se la velocità di picco sistolico dell’MCA o ICA distale è superiore a 220 cm/s. Non vi sono dati validati per definire una diagnosi. Sensibilità 70-90%? Specificità 90-95%?
 se la velocità di picco sistolico dell’MCA o ICA distale è superiore a 220 cm/s. Non vi sono dati validati per definire una diagnosi. Sensibilità 70-90% Specificità 90-95%")
14
MCA Stenosis

15
Pitfalls & Diagnostic Accuracy
Lack of flow signal due to an inadequate temporal window Misinterpretation of hyperdynamic collateral channels or AVM feeders as stenosis Displacement of arteries because of a space-occupying lesion Misinterpretation of physiologic variables in the circle of Willis Misdiagnosis of vasospasm as stenosis Misinterpretation of reactive hyperemia following spontaneous recanalization as stenosis

16
Pitfalls & Diagnostic Accuracy Vertebral-Basilar System
Normal flow and size of vessels are highly variable Location and course of the arteries are unpredictable Difficulty in reliably identifying the junction of the vertebral arteries Absence of the vertebral artery flow signal on one side may not represent disease Lack of flow in one vertebral artery distally, above the origin of the PICA due to vertebral artery hypoplasia Occlusion of one vertebral artery or a “top of the basilar” occlusion does not necessarily lead to relevant flow abnormalities

18
Summary of findings Intracranial Steno-Occlusive Disease
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Intracranial Steno-Occlusive Disease: Conventional angiography Anterior Circulation 70-90 90-95 Posterior Circulation Occlusion 50-80 80-96 Copyright 2004 American Academy of Neurology
 SPECIFICITY (%) REFERENCE STANDARD. Intracranial Steno-Occlusive Disease: Conventional angiography. Anterior Circulation Posterior Circulation. Occlusion Copyright 2004 American Academy of Neurology.")
19
Summary of findings Intracranial Steno-Occlusive Disease (Continued )
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD MCA 85-95 90-98 ICA, VA, BA 55-81 96 Recommendation: Data are insufficient to establish TCD criteria for greater than 50% stenosis or for progression of stenosis in intracranial arteries (Type U). Copyright 2004 American Academy of Neurology
 SPECIFICITY (%) REFERENCE STANDARD. MCA ICA, VA, BA Recommendation: Data are insufficient to establish TCD criteria for greater than 50% stenosis or for progression of stenosis in intracranial arteries (Type U). Copyright 2004 American Academy of Neurology.")
20
Summary of findings Acute cerebral infarction
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Acute cerebral infarction 85-95 90-98 Recommendation: TCD is probably useful for the evaluation of patients with suspected intracranial steno-occlusive disease, particularly in the ICA siphon and MCA (Type B, Class II evidence). The relative value of TCD compared with MRA or CTA remains to be determined (Type U). Data are insufficient to give a recommendation regarding replacing conventional angiography with TCD (Type U).
 SPECIFICITY (%) REFERENCE STANDARD. Acute cerebral infarction Recommendation: TCD is probably useful for the evaluation of patients with suspected intracranial steno-occlusive disease, particularly in the ICA siphon and MCA (Type B, Class II evidence). The relative value of TCD compared with MRA or CTA remains to be determined (Type U). Data are insufficient to give a recommendation regarding replacing conventional angiography with TCD (Type U).")
21
Summary of findings Extracranial ICA Stenosis
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Extracranial ICA Stenosis: Conventional angiography Single TCD variable 3-78 60-100 TCD Battery 49-95 42-100 TCD Battery & Carotid Duplex 89 100 Recommendation:TCD is possibly useful for the evaluation of severe extracranial ICA stenosis or occlusion (Type C, Class II-III evidence).
 SPECIFICITY (%) REFERENCE STANDARD. Extracranial ICA Stenosis: Conventional angiography. Single TCD variable TCD Battery TCD Battery & Carotid Duplex Recommendation:TCD is possibly useful for the evaluation of severe extracranial ICA stenosis or occlusion (Type C, Class II-III evidence).")
22
Transcranial Color-Coded Sonography (TCCS) or Imaging TCD
 or Imaging TCD")
23
Summary of findings Ischemic Cerebrovascular Disease
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD ACoA Collateral Flow 100 PCoA Collateral Flow 85 98
 SPECIFICITY (%) REFERENCE STANDARD. ACoA Collateral Flow PCoA Collateral Flow")
24
Summary of findings Ischemic Cerebrovascular Disease (Continued)
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Intracranial Steno-Occlusive Lesions Any Up to 100 Up to 83
 SPECIFICITY (%) REFERENCE STANDARD. Intracranial Steno-Occlusive Lesions. Any. Up to 100. Up to 83.")
25
Summary of findings Ischemic Cerebrovascular Disease (Continued)
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD /= 50% Stenosis MCA 100 ACA VA BA PCA
 SPECIFICITY (%) REFERENCE STANDARD. /= 50% Stenosis. MCA ACA. VA. BA. PCA.")
26
Summary of findings Ischemic Cerebrovascular Disease (Continued)
Recommendation: (CE)-TCCS is probably useful in the evaluation and monitoring of patients with ischemic cerebrovascular disease (Type B, Class II-IV evidence).
-TCCS is probably useful in the evaluation and monitoring of patients with ischemic cerebrovascular disease (Type B, Class II-IV evidence).")
27
Summary of findings Hemorrhagic Cerebrovascular Disease
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Parenchymal Hypoechogenicity in MCA Distribution 69 83 Computed tomographic scan Recommendation: (CE-) TCCS is probably useful in the evaluation and monitoring of patients with aneurysmal SAH or intracranial ICA/MCA VSP following SAH (Type B, Class II-III evidence). Data are insufficient regarding the use of TCCS to replace CT for diagnosis of ICH (Type U).
 SPECIFICITY (%) REFERENCE STANDARD. Parenchymal Hypoechogenicity in MCA Distribution Computed tomographic scan. Recommendation: (CE-) TCCS is probably useful in the evaluation and monitoring of patients with aneurysmal SAH or intracranial ICA/MCA VSP following SAH (Type B, Class II-III evidence). Data are insufficient regarding the use of TCCS to replace CT for diagnosis of ICH (Type U).")
35
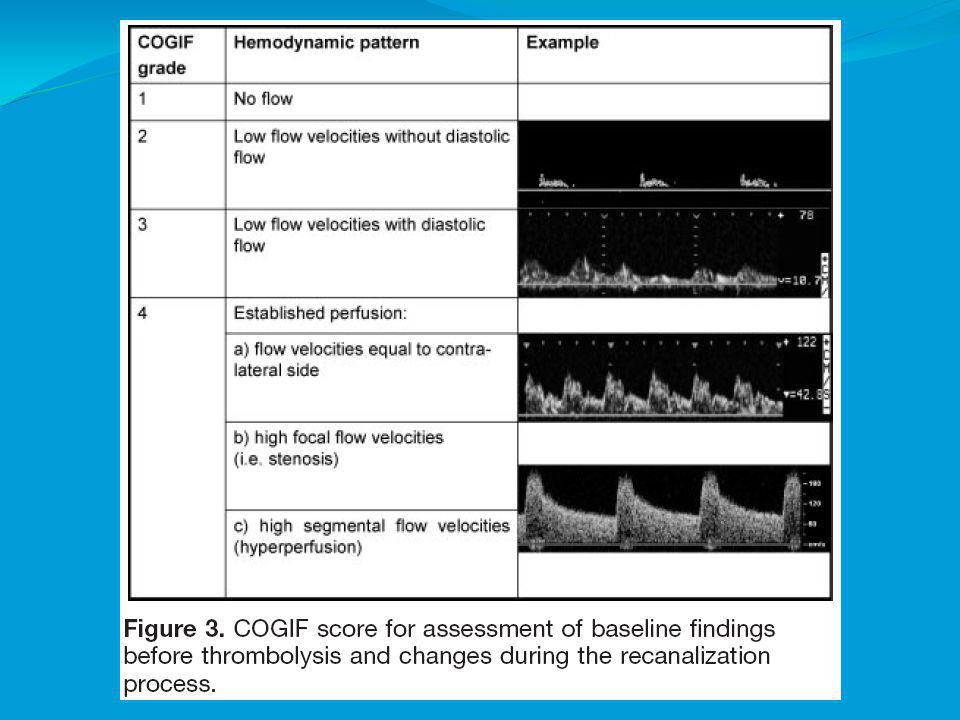
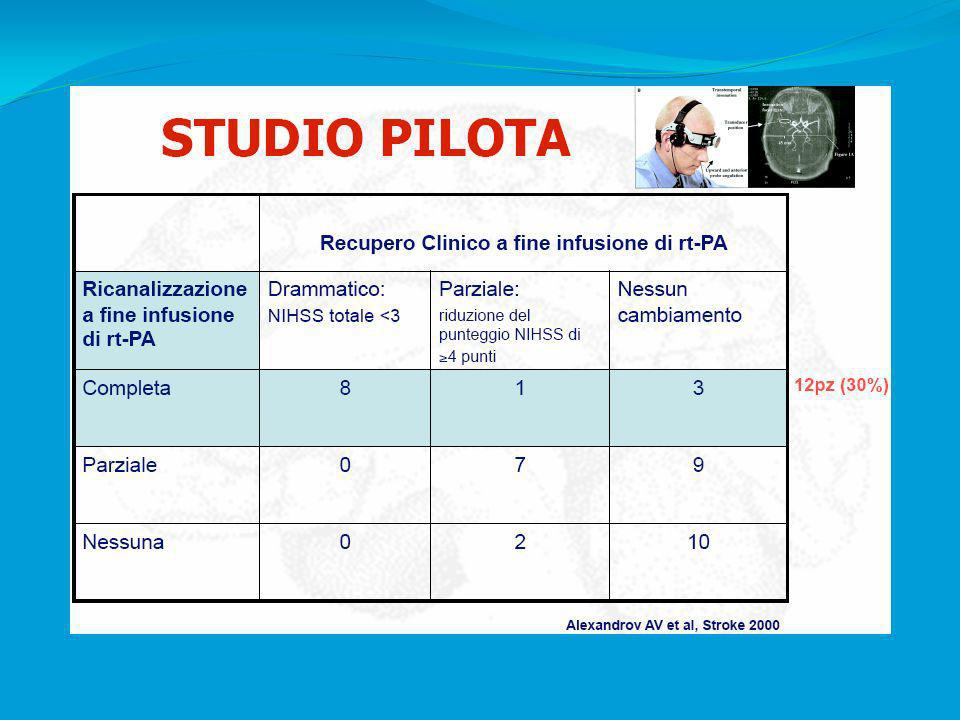
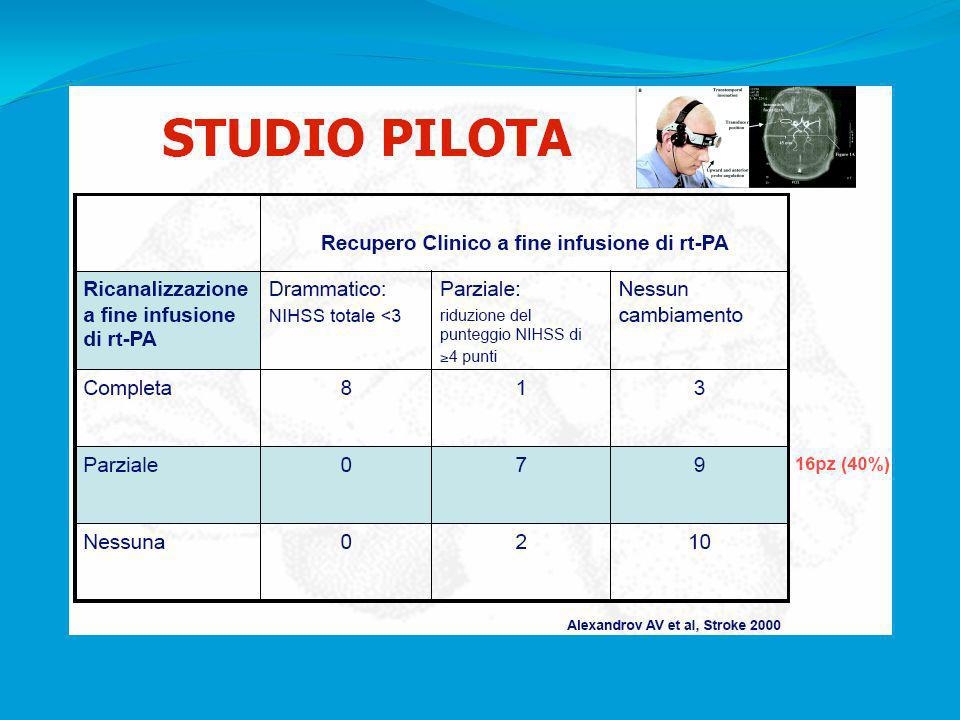
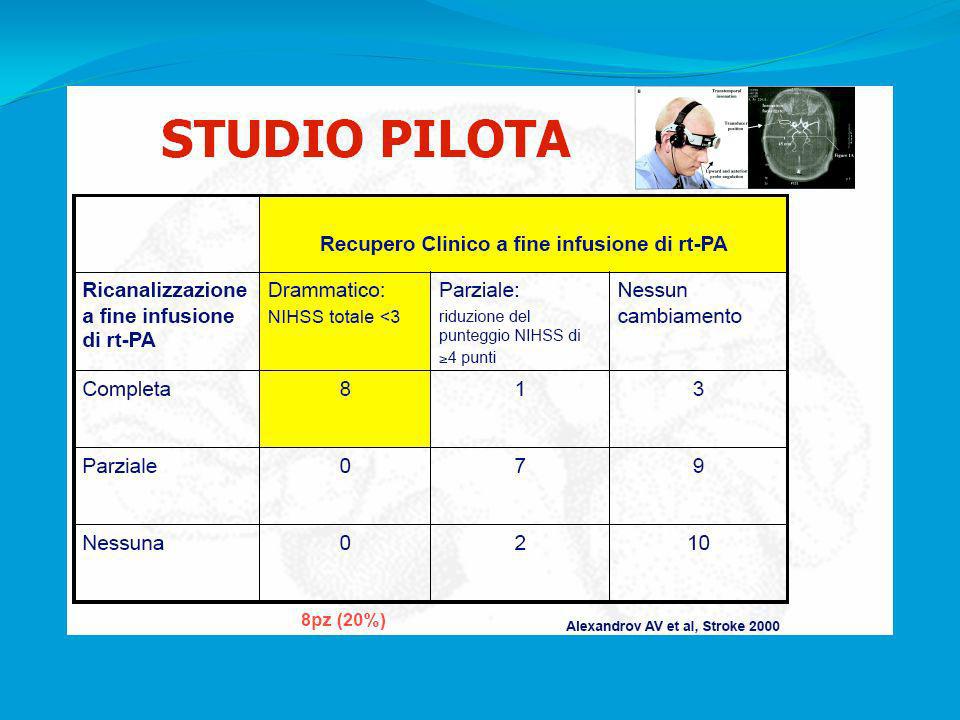
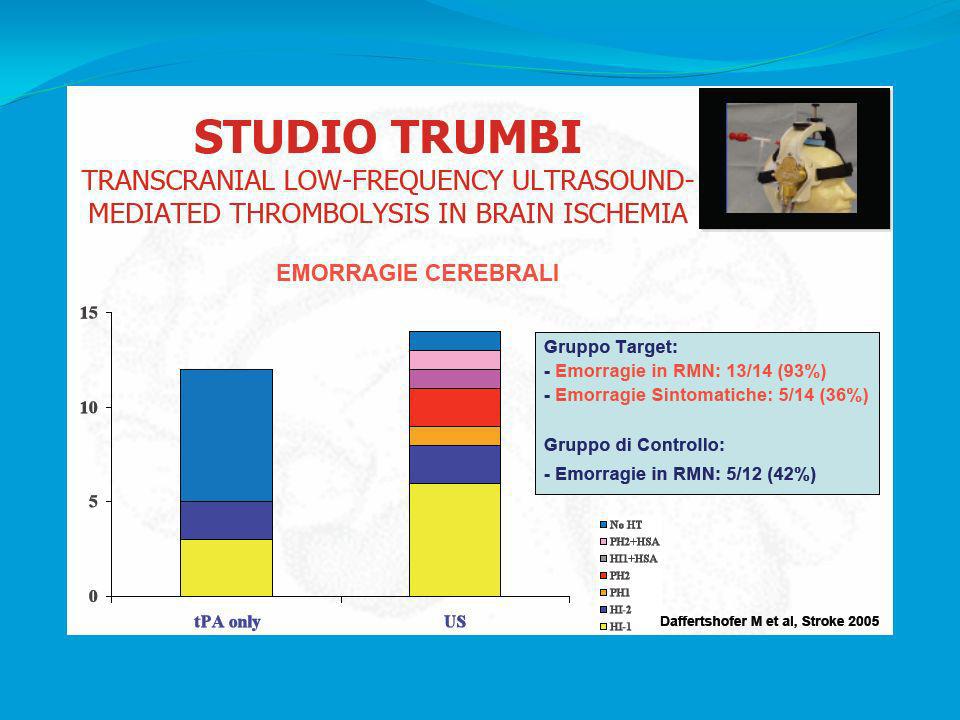
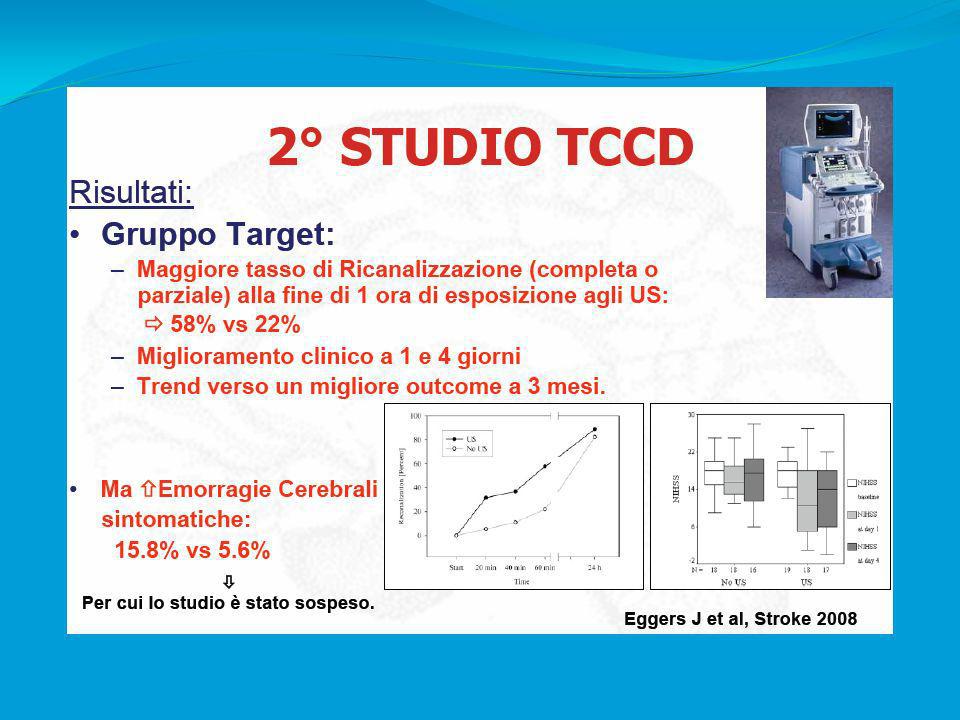
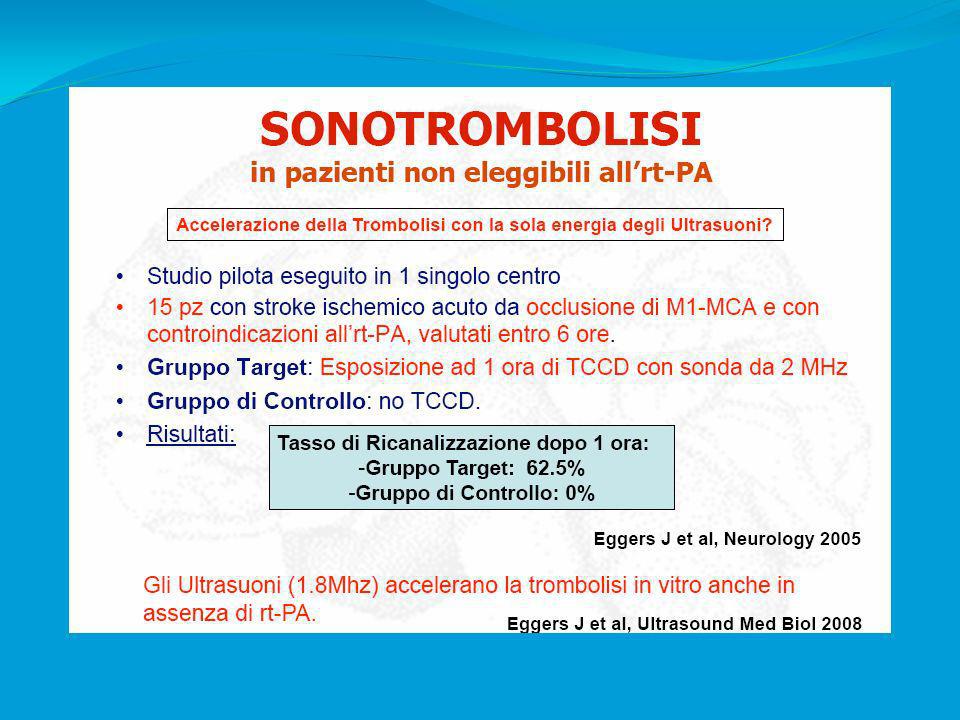
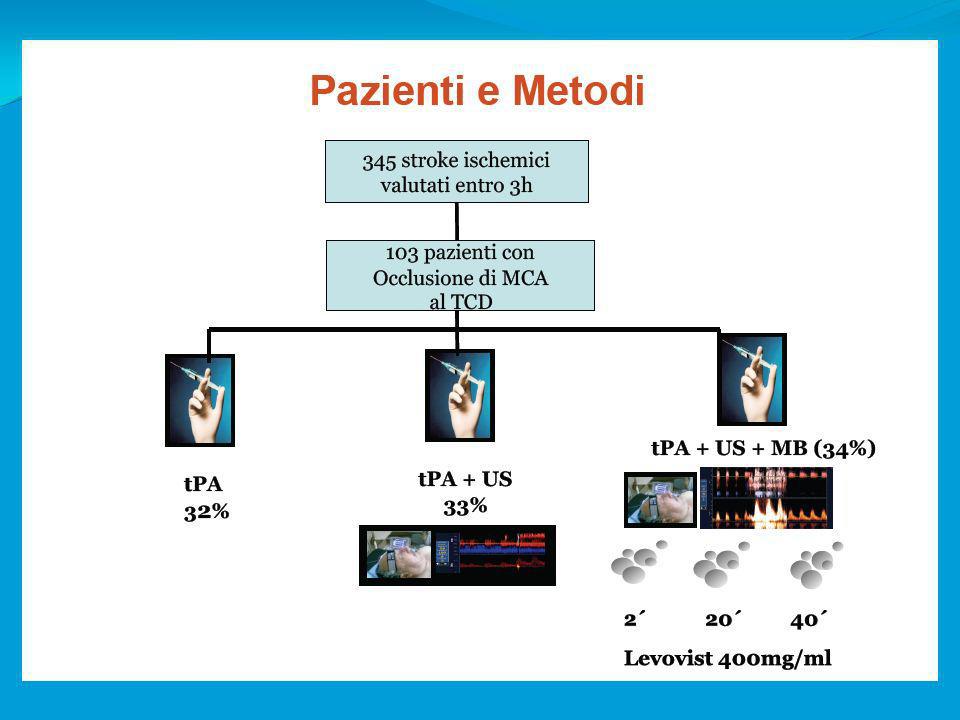
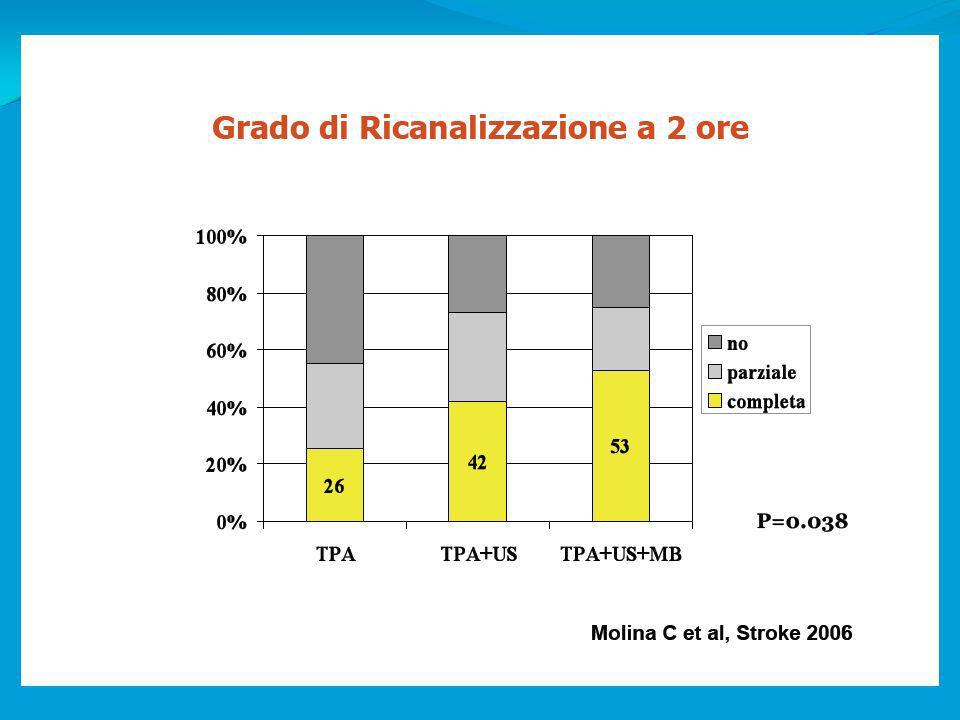
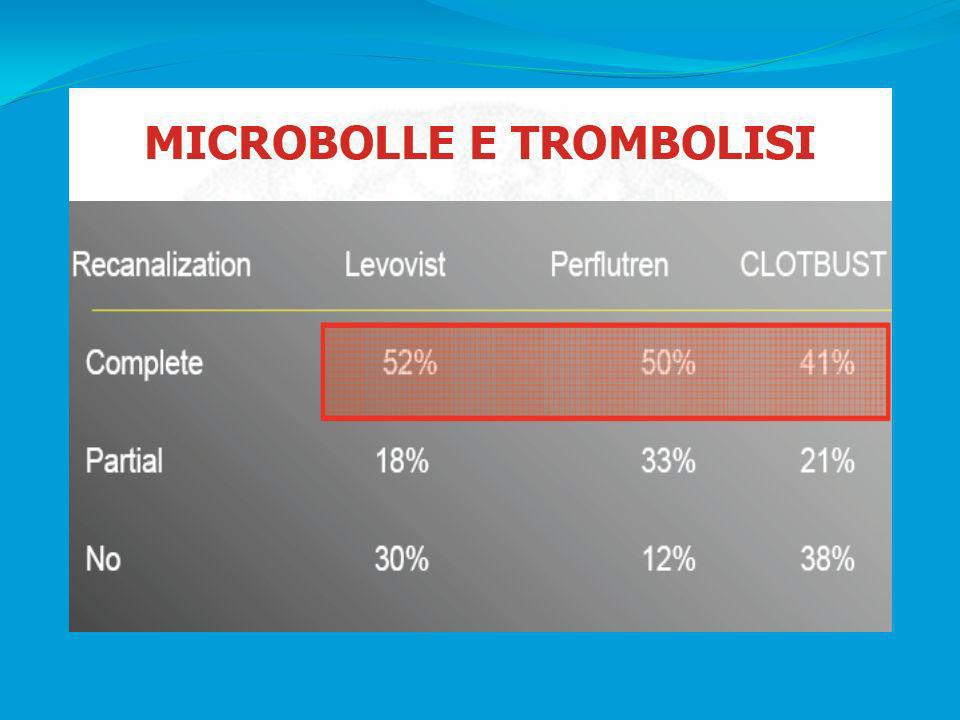
Summary of findings Cerebral Thrombolysis
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Cerebral Thrombolysis Conventional angiography, magnetic resonance angiography, clinical outcome Complete Occlusion 50 100 Partial Occlusion 76 Recanalization 91 93
 SPECIFICITY (%) REFERENCE STANDARD. Cerebral Thrombolysis. Conventional angiography, magnetic resonance angiography, clinical outcome. Complete Occlusion Partial Occlusion. 76. Recanalization")
36
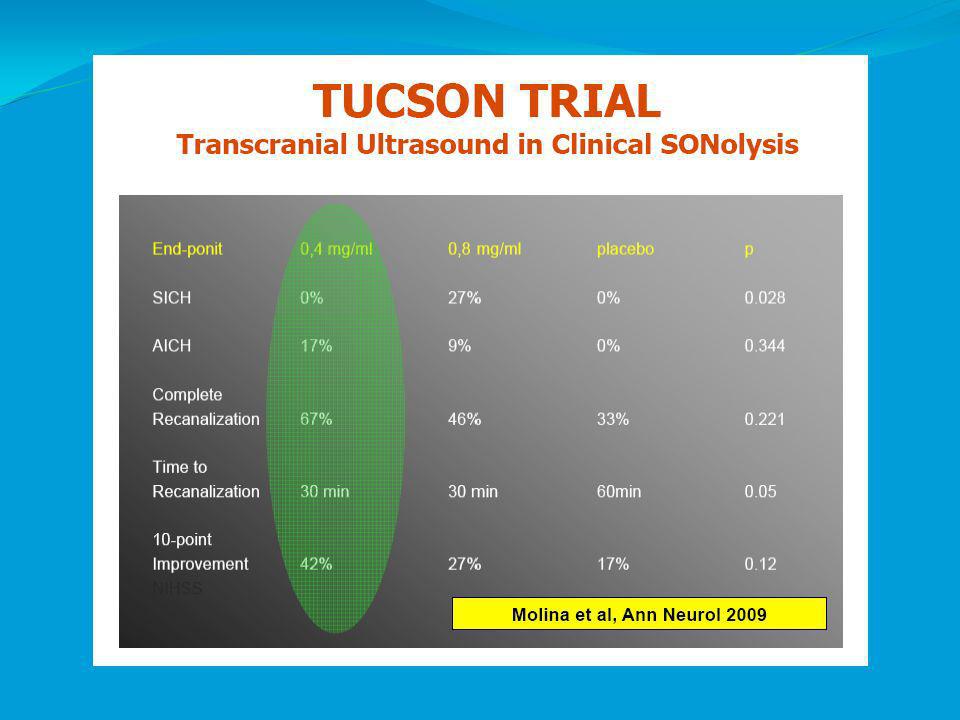
Summary of findings Cerebral Thrombolysis (continued)
Recommendation: TCD is probably useful for monitoring thrombolysis of acute MCA occlusions (Type B, Class II-III evidence). Present data are insufficient to either define the optimal frequency of TCD monitoring for clot dissolution and enhanced recanalization or to influence therapy (Type U).
. Present data are insufficient to either define the optimal frequency of TCD monitoring for clot dissolution and enhanced recanalization or to influence therapy (Type U).")
79
Summary of findings Carotid Endarterectomy (CEA)
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Carotid Endarterectomy (CEA): EEG, magnetic resonance imaging, clinical outcomes Recommendation: CEA monitoring with TCD can provide important feedback pertaining to hemodynamic and embolic events during and after surgery that may help the surgeon take appropriate measures at all stages of the operation to reduce the risk of perioperative stroke. TCD monitoring is probably useful during and after CEA in circumstances where monitoring is felt to be necessary (Type B, Class II-III evidence).
 SPECIFICITY (%) REFERENCE STANDARD. Carotid Endarterectomy (CEA): EEG, magnetic resonance imaging, clinical outcomes. Recommendation: CEA monitoring with TCD can provide important feedback pertaining to hemodynamic and embolic events during and after surgery that may help the surgeon take appropriate measures at all stages of the operation to reduce the risk of perioperative stroke. TCD monitoring is probably useful during and after CEA in circumstances where monitoring is felt to be necessary (Type B, Class II-III evidence).")
80
Summary of findings Vasomotor Reactivity (VMR) Testing
Recommendation: TCD vasomotor reactivity testing is considered probably useful for the detection of impaired cerebral hemodynamics in patients with asymptomatic severe (>70%) stenosis of the extracranial ICA patients with symptomatic or asymptomatic extracranial ICA occlusion and patients with cerebral small artery disease (Type B, Class II-III evidence). How the results from these techniques should be used to influence therapy and affect patient outcomes remains to be determined (Type U).
 stenosis of the extracranial ICA. patients with symptomatic or asymptomatic extracranial ICA occlusion and patients with cerebral small artery disease (Type B, Class II-III evidence). How the results from these techniques should be used to influence therapy and affect patient outcomes remains to be determined (Type U).")
81
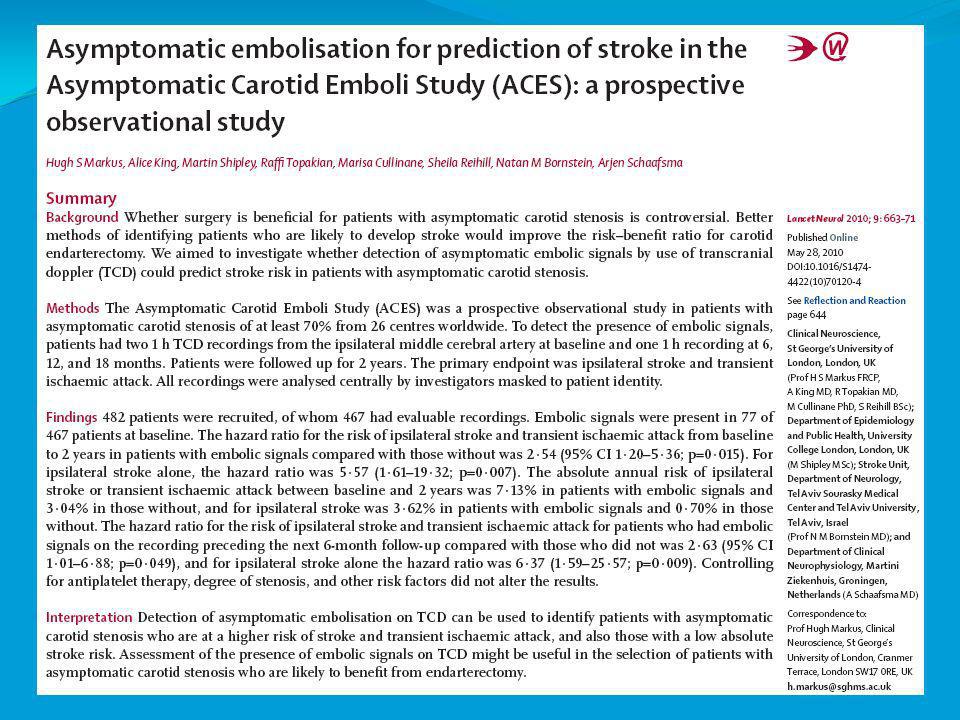
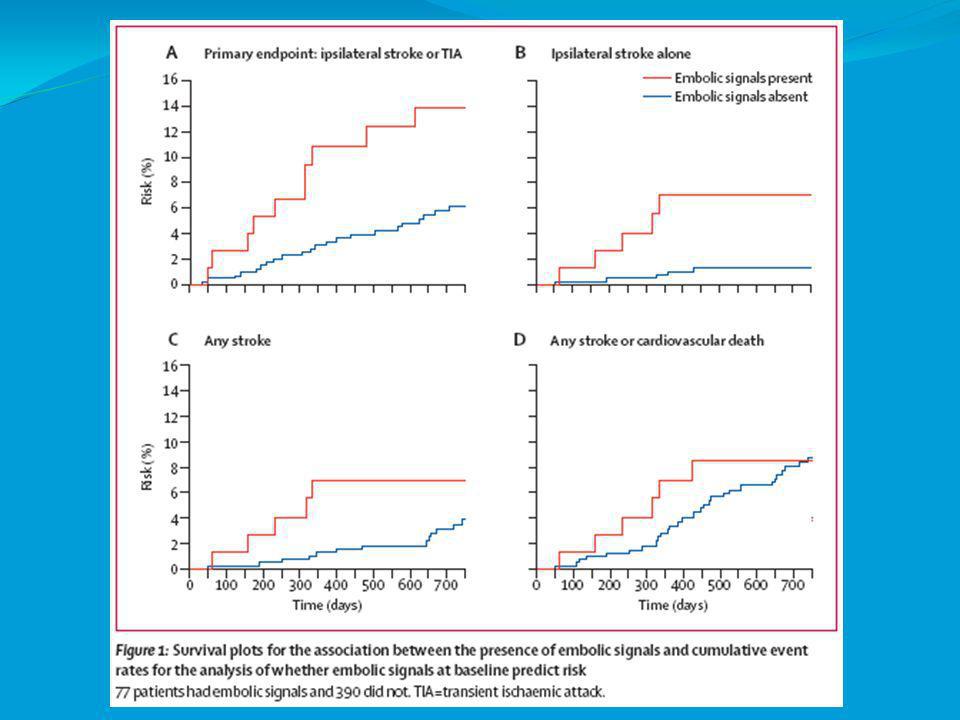
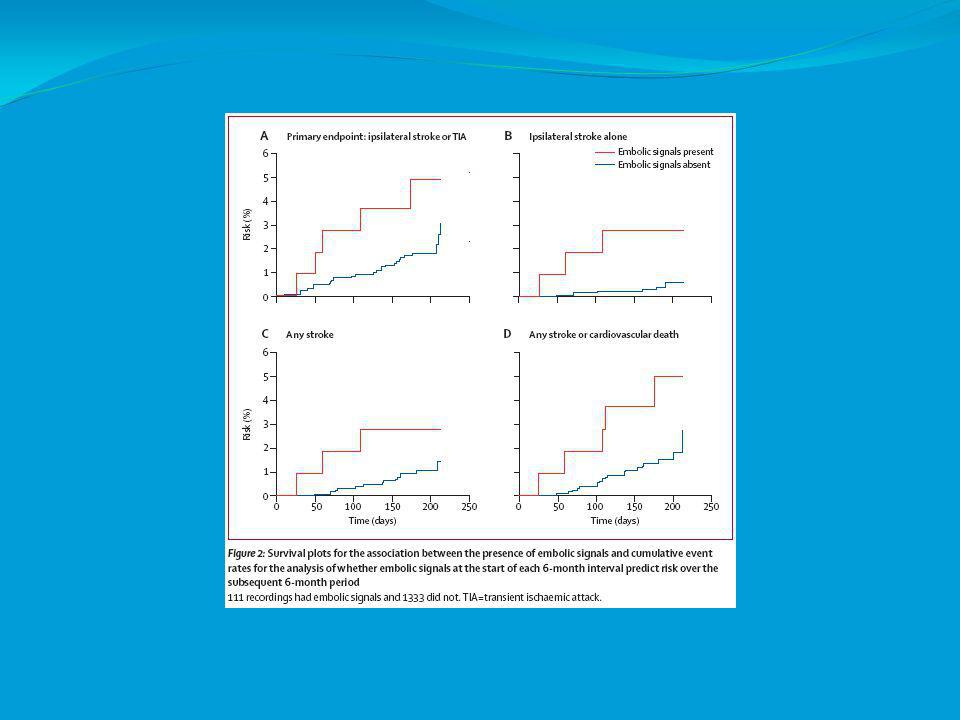
Summary of findings Detection of Cerebral Microemboli
INDICATION SENSITIVITY (%) SPECIFICITY (%) REFERENCE STANDARD Cerebral Microembolization Experimental model, pathology, magnetic resonance imaging, neuropsychological tests Recommendation: TCD is probably useful to detect cerebral microembolic signals in a wide variety of cardiovascular/ cerebrovascular disorders/procedures (Type B, Class II-IV evidence). However, data at present do not support the use of TCD for diagnosis or for monitoring response to antithrombotic therapy in ischemic cerebrovascular disease in these settings(Type U).
 SPECIFICITY (%) REFERENCE STANDARD. Cerebral Microembolization. Experimental model, pathology, magnetic resonance imaging, neuropsychological tests. Recommendation: TCD is probably useful to detect cerebral microembolic signals in a wide variety of cardiovascular/ cerebrovascular disorders/procedures (Type B, Class II-IV evidence). However, data at present do not support the use of TCD for diagnosis or for monitoring response to antithrombotic therapy in ischemic cerebrovascular disease in these settings(Type U).")
94
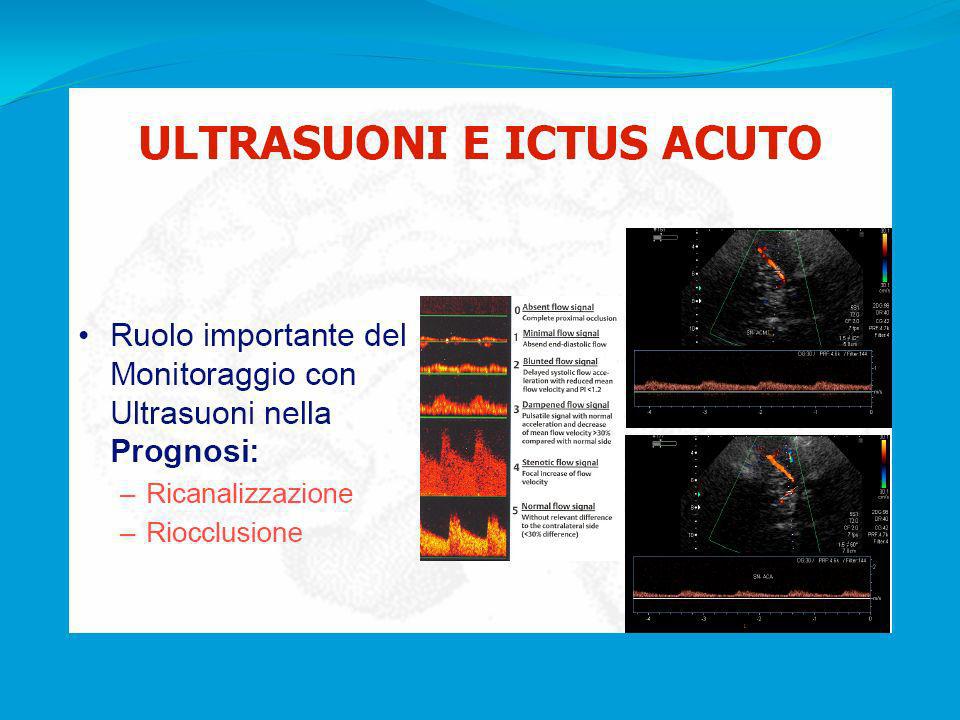
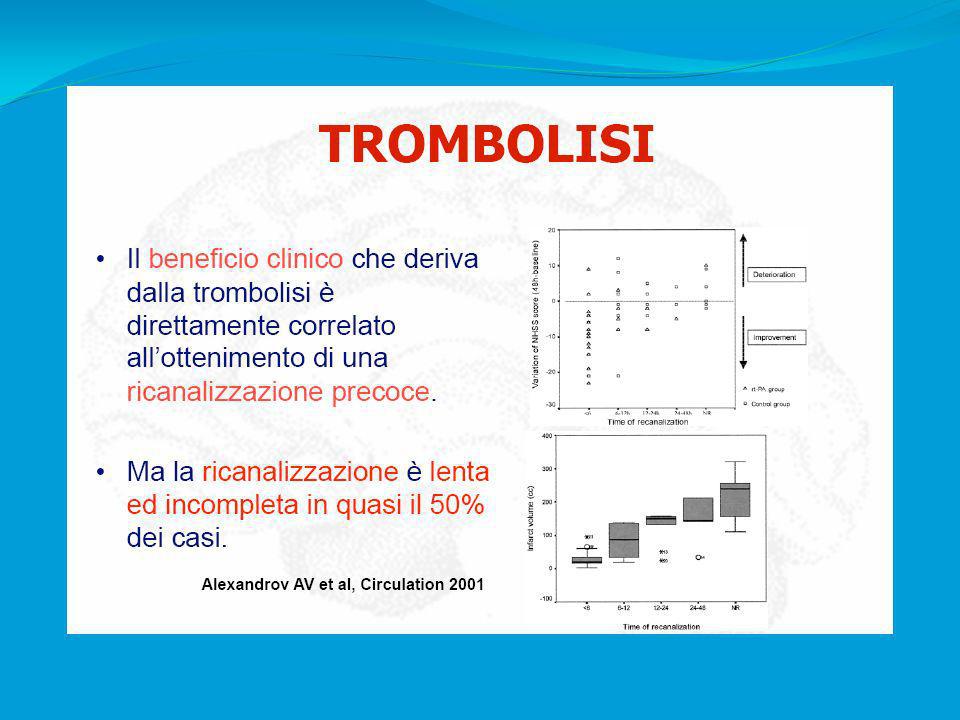
TCD in fase acuta Conclusioni
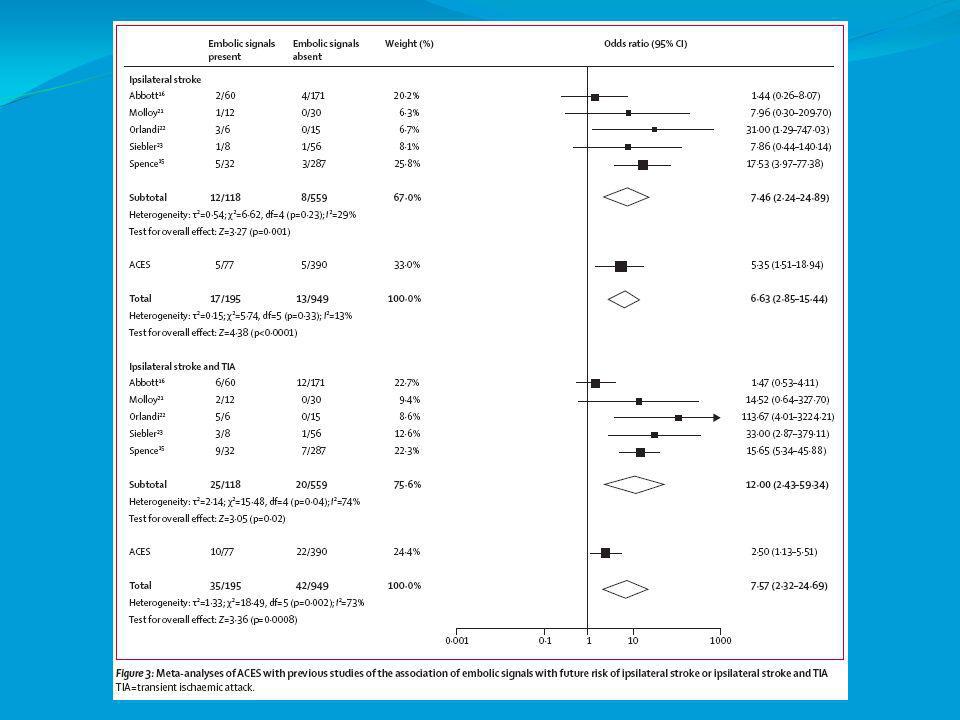
Utile nell’approccio diagnostico in fase acuta Consente il monitoraggio dei vasi intracranici sia in fase acuta che a lungo termine Migliora la trombolisi sia farmacologica che spontanea Consente il monitoraggio dell’interventistica cardio-cerebrovascolare Ha valore prognostico in fase acuta del TIA (stenosi e microemboli) e dell’ictus acuto (stenosi)
 e dell’ictus acuto (stenosi)")
Presentazioni simili


























 is a disease state characterized by airflow limitation that is not fully reversible. The.>")




>")





