Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Terapia con insuline: “l’evoluzione della specie”
Limiti e rischi

2
Terapia insulinica: limiti

3
Insulin treatment and special populations
Insulin analogues are currently used for treating diabetic patients PK/PD profiles for specific insulin analogues may be altered in special patients populations such as elderly patients or children but also in special conditions such as pregnancy Specific efficacy and safety data about the use of insulin analogues across the spectrum of special populations, although limited, should be considered when designing treatment regimens for special patient group

4
Cura del diabete in popolazioni specifiche
Standard Italiani per la cura del diabete mellito SID/AMD 2010.

5
Steatment sugli analoghi rapidi SID, AMD, SIEDP Giugno 2012
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Steatment sugli analoghi rapidi SID, AMD, SIEDP Giugno 2012

6
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Aspart Glulisine Lispro Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) (>6 anni) Anziani (>65 anni) (studi di PK) (dati limitati) Insufficienza renale Insufficienza epatica Somministrazione dopo il pasto Uso in microinfusori Somministrazione per via endovenosa ( con limitazioni) Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro
 (dati retrospettivi) Pediatria. (>2 anni) (>6 anni) Anziani (>65 anni) (studi di PK) (dati limitati) Insufficienza renale. Insufficienza epatica. Somministrazione dopo il pasto. Uso in microinfusori. Somministrazione per via endovenosa. ( con limitazioni) Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro.")
7
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Detemir Glargine Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) Anziani (>65 anni) (studi di PK ) Insufficienza renale (studi di PK) Insufficienza epatica Riassunto della caratteristiche di prodotto Insulina Detemir, Insulina Glargine
 (dati retrospettivi) Pediatria. (>2 anni) Anziani (>65 anni) (studi di PK ) Insufficienza renale. (studi di PK) Insufficienza epatica. Riassunto della caratteristiche di prodotto Insulina Detemir, Insulina Glargine.")
8
(Nessun limite specificato)
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Aspart Glulisine Lispro Detemir Glargine Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) (>6 anni) (Nessun limite specificato) (> 2 anni) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale Insufficienza epatica Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine
 (dati retrospettivi) Pediatria. (>2 anni) (>6 anni) (Nessun limite specificato) (> 2 anni) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale. Insufficienza epatica. Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine.")
9
Diabetes in pregnancy and risk of complications
Dunne et al. Diabetes Care 2009;32:1205–6

10
Blood glucose control is linked with outcomes in diabetic pregnancy
Speaker notes The Diabetes Control and Complications Trial was a multicentre controlled clinical trial that compared intensive with conventional therapy in insulin-dependent diabetes mellitus. Intensive therapy, with the aim of achieving normal glycaemic control, was initiated in women originally assigned to conventional therapy who actively sought to become pregnant or who became pregnant. The above graph shows median HbA1c for DCCT pregnancies in intensive treatment group for pregnancies with normal and abnormal outcomes. Overall the median HbA1c was higher in women who had abnormal outcomes (p=0.05). *At 3 months before conception and at month 5 there were significant differences in median HbA1c levels for the pregnancies with normal outcomes versus those with abnormal outcomes. Diabetes Control and Complications Trial. Am J Obstet Gynecol 1996;174(4):1343–53
. *At 3 months before conception and at month 5 there were significant differences in median HbA1c levels for the pregnancies with normal outcomes versus those with abnormal outcomes. Diabetes Control and Complications Trial. Am J Obstet Gynecol 1996;174(4):1343–53.")
11
Major Hypoglycemia in type 1 diabetic pregnancy

12
Fetal and perinatal outcomes in type 1 diabetes pregnancy

13
Mathiesen et al. Diabetes Care 2012
Major hypoglycaemia during pregnancy was similar with insulin detemir and NPH insulin Most subjects in both treatment groups (approximately 94%) had one or more hypoglycaemic episodes during pregnancy. The rate of episodes during pregnancy was similar in the two treatment groups. Major hypoglycaemic episodes during pregnancy occurred in slightly more subjects in the NPH group than in the IDet group (21% of the subjects vs. 16%). The rate was similar in the two groups (1.1–1.2 episodes/year). During the pre-pregnancy period, the rate of major hypoglycaemic episodes was higher in the IDet group (rate of 1.5 vs. 0.2 episodes/year). Major episodes pre-pregnancy occurred in a relatively low number of subjects (8 in the IDet group vs. 4 in the NPH group), so data should be interpreted with caution. Major diurnal hypoglycaemic episodes during pregnancy occurred in more subjects in the NPH group than in the IDet group (19% vs. 11% of the subjects). The rate was similar in the two treatment groups. Approximately 80% of the subjects in both treatment groups had one or more nocturnal hypoglycaemic episodes during pregnancy. The rate was similar in the two groups (approximately 18 episodes/year). Nocturnal major hypoglycaemic episodes during pregnancy occurred at a similar frequency in the two treatment groups (IDet 9%, NPH 6% of subjects). The rate was approximately 0.3 episodes/year in both treatment groups. Mathiesen et al. Diabetes Care 2012 NPH, neutral protamine Hagedorn 13
 had one or more hypoglycaemic episodes during pregnancy. The rate of episodes during pregnancy was similar in the two treatment groups. Major hypoglycaemic episodes during pregnancy occurred in slightly more subjects in the NPH group than in the IDet group (21% of the subjects vs. 16%). The rate was similar in the two groups (1.1–1.2 episodes/year). During the pre-pregnancy period, the rate of major hypoglycaemic episodes was higher in the IDet group (rate of 1.5 vs. 0.2 episodes/year). Major episodes pre-pregnancy occurred in a relatively low number of subjects (8 in the IDet group vs. 4 in the NPH group), so data should be interpreted with caution. Major diurnal hypoglycaemic episodes during pregnancy occurred in more subjects in the NPH group than in the IDet group (19% vs. 11% of the subjects). The rate was similar in the two treatment groups. Approximately 80% of the subjects in both treatment groups had one or more nocturnal hypoglycaemic episodes during pregnancy. The rate was similar in the two groups (approximately 18 episodes/year). Nocturnal major hypoglycaemic episodes during pregnancy occurred at a similar frequency in the two treatment groups (IDet 9%, NPH 6% of subjects). The rate was approximately 0.3 episodes/year in both treatment groups. Mathiesen et al. Diabetes Care NPH, neutral protamine Hagedorn. 13.")
14
Composite fetal endpoint
There was no statistically significant difference between the treatment groups for the compiled composite pregnancy endpoint. CI, confidence interval; GW, gestational week; IDet, insulin detemir; NPH, neutral protamine Hagedorn Hod et al. Diabetes 2011:Abstract 62-LB and and ADA 2011 poster presentation 14

15
Farmaci in gravidanza: classificazione FDA
Aspart Detemir Lispro Insulina umana Glargine Glulisine

16
(Nessun limite specificato)
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Aspart Glulisine Lispro Detemir Glargine Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale Insufficienza epatica Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine
 (dati retrospettivi) Pediatria. (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale. Insufficienza epatica. Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine.")
17
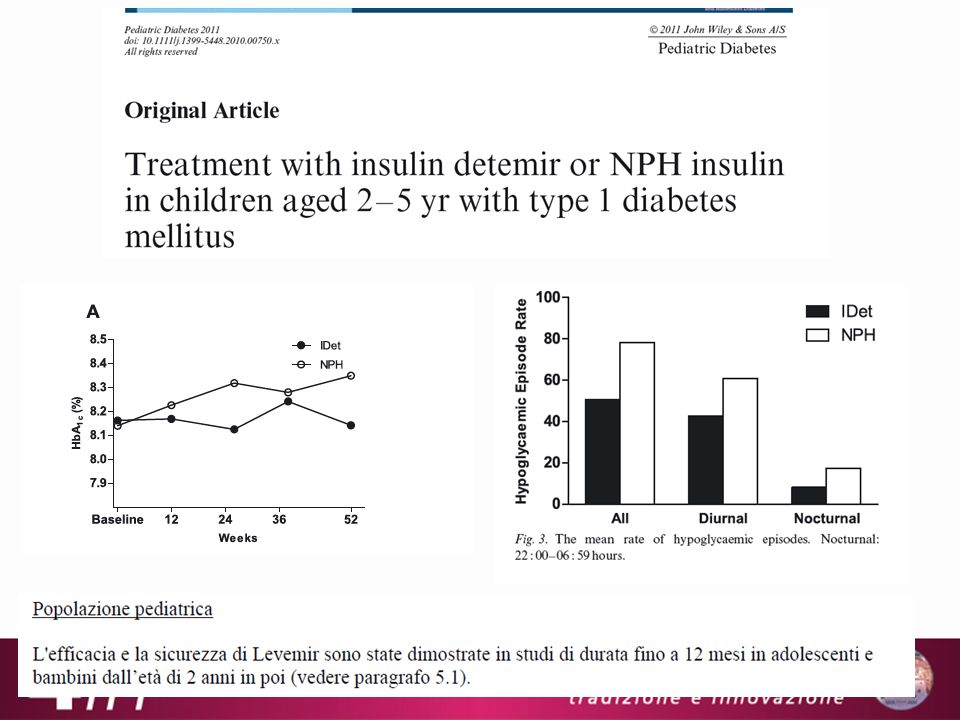
Aspart in children aged 2–6 years
Danne et al, Diabetes Care Aug;26(8):
:")
19
(Nessun limite specificato)
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Aspart Glulisine Lispro Detemir Glargine Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale Insufficienza epatica Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine
 (dati retrospettivi) Pediatria. (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale. Insufficienza epatica. Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine.")
20
Preserved pharmacokinetic profile of insulin aspart vs
Preserved pharmacokinetic profile of insulin aspart vs. human insulin in the elderly IAsp RHI 800 * 700 600 NS 500 Exogenous serum insulin (pmol/l) 400 300 200 100 Cmax, INS was higher and occurred earlier (tmax, INS) with IAsp than with RHI (p < 0. 01, for both). The AUCINS (0-60 min), AUCINS (0-120 min) and AUCINS (0-300 min) were greater with IAsp than with RHI (p < 0.01, for all). AUCINS ( min) was less for IAsp than for RHI; however, the difference was not statistically significant (p = ). Nominal time (min) *= AUCINS(0-300 min) was greater with IAsp than RHI (p<0.0001) Krones et al. Diabetes Obes Metab 2009;11(1):41-4.
 Cmax, INS was higher and occurred earlier (tmax, INS) with IAsp than with RHI (p < 0. 01, for both). The AUCINS (0-60 min), AUCINS (0-120 min) and AUCINS (0-300 min) were greater with IAsp than with RHI. (p < 0.01, for all). AUCINS ( min) was less for IAsp than for RHI; however, the difference was not statistically significant (p = ). Nominal time (min) *= AUCINS(0-300 min) was greater with IAsp than RHI (p<0.0001) Krones et al. Diabetes Obes Metab 2009;11(1):41-4.")
21
Insulina detemir nei soggetti anziani con diabete tipo 2
Paolo: si può graficare questa tabella?

22
(Nessun limite specificato)
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Aspart Glulisine Lispro Detemir Glargine Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale Insufficienza epatica Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine
 (dati retrospettivi) Pediatria. (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale. Insufficienza epatica. Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine.")
23
Holmes et al. Br J Clin Pharmacol 2005;60(5):469-76
Mean plasma concentration vs. time for insulin aspart by degree of renal impairment 60 Normal Mild Moderate Severe concentration (mU/L) 50 40 Mean insulin aspart 30 20 10 Time (mins) Regression analyses showed no significant difference in PK endpoints between normal and variable degrees of renal impairment Ln(Cmax), ln(AUC0-360) and t1/2(mins): p=0.92, p=0.78 and p=0.65, respectively. Holmes et al. Br J Clin Pharmacol 2005;60(5):469-76
 Mean insulin aspart Time (mins) Regression analyses showed no significant difference in PK endpoints between normal and variable degrees of renal impairment. Ln(Cmax), ln(AUC0-360) and t1/2(mins): p=0.92, p=0.78 and p=0.65, respectively. Holmes et al. Br J Clin Pharmacol 2005;60(5):")
24
Pharmacokinetics of Insulin Detemir in Subjects with Renal Impairment
L.V. Jacobsen1, G. Popescu2, A. Plum3 1Copenhagen, Denmark; 2Munich, Germany; and 3Copenhagen, Denmark

25
(Nessun limite specificato)
Terapia insulinica: indicazioni terapeutiche in sottogruppi di pazienti o condizioni patologiche specifiche Aspart Glulisine Lispro Detemir Glargine Uso in gravidanza (dati prospettici) (dati retrospettivi) Pediatria (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale Insufficienza epatica Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine
 (dati retrospettivi) Pediatria. (>2 anni) (>6 anni) (Nessun limite specificato) Anziani (>65 anni) (studi di PK) (dati limitati) (studi di PK ) Insufficienza renale. Insufficienza epatica. Riassunto della caratteristiche di prodotto Insulina Aspart, Insulina Glulisine, Insulina Lispro, Insulina Detemir, Insulina Glargine.")
26
Terapia insulinica: rischi

27
1,3 eventi / anno / paziente
Il 36,7% con almeno un episodio, il 21,3% con due o più episodi Il 5% giustifica il 54% degli episodi, il 10% il 69% 0,44 eventi / anno / paziente 16,5% con almeno un episodio Akram K. et al, Diabet Med (2006) 23: 750-6 Pedersen-Bjergaard U. et al, Diabetes Metab Res Rev (2004) 20:
 23: Pedersen-Bjergaard U. et al, Diabetes Metab Res Rev (2004) 20:")
28
Epidemiology of hypoglycaemia in UK
29/03/ :35 Epidemiology of hypoglycaemia in UK ADA definition of severe hypos: An event requiring assistance of another person to actively administer carbohydrate, glucagons, or other resuscitative actions. These episodes may be associated with sufficient neuroglycopenia to induce seizure or coma. Plasma glucose measurements may not be available during such an event, but neurological recovery attributable to the restoration of plasma glucose to normal is considered sufficient evidence that the event was induced by a low plasma glucose concentration. The UK Hypoglycaemia Study was an observational study over 9–12 months in six UK secondary care diabetes centres. Altogether, 383 patients were involved. Patients were divided into the following three treatment groups for type 2 diabetes: SUs Insulin for <2 years Insulin for >5 years and into two treatment groups for type 1 diabetes, namely <5 years’ disease duration and >15 years’ disease duration. Self-reported (mild and major) episodes were recorded. Hypoglycaemia is a common, unpredictable and potentially dangerous side effect of insulin therapy for both types of diabetes and patients both on insulin but also on OADs. In the UK Hypoglycaemia Study, the risk of hypoglycaemia in type 2 diabetes increased considerably with the duration of insulin treatment and as type 2 diabetes progressed the rate of severe hypos began to match the rate seen early in patients with type 1 diabetes, therefore highlighting the importance and magnitude of hypoglycaemia. The priority for care is to combine effective glycaemic control to prevent diabetic complications, with (in light of recent findings of large studies e.g. ACCORD) freedom from hypoglycaemia; providing the healthcare professional and patient with an insulin that allows for comparable glycaemic control, to current basal insulins, but better control of hypoglycaemic events without compromising on safety. The data depicted is the proportion of each group experiencing at least one severe self-reported hypoglycaemic episode during 9–12 months of follow-up. They reported an incidence of severe hypoglycaemia of 110–320 episodes per 100 patient-years in patients with type 1 diabetes. Although hypoglycaemia was less frequent in type 2 diabetes, it becomes progressively more frequent and limiting to glycaemic control later in the course of the disease. Comparing treatment with insulin for 2 years vs. 5 years: Severe hypoglycaemia prevalence was 7 and 25%, respectively, and incidence was 10 and 70 episodes per 100 patient-years, respectively, whereas mild hypoglycaemia prevalence was 51 and 64%, respectively, and incidence was 410 and 1020 episodes per 100 patient-years, respectively. SU, sulphonylurea UK Hypoglycaemia Study Group. Diabetologia 2007;50:1140–7 28
 episodes were recorded. Hypoglycaemia is a common, unpredictable and potentially dangerous side effect of insulin therapy for both types of diabetes and patients both on insulin but also on OADs. In the UK Hypoglycaemia Study, the risk of hypoglycaemia in type 2 diabetes increased considerably with the duration of insulin treatment and as type 2 diabetes progressed the rate of severe hypos began to match the rate seen early in patients with type 1 diabetes, therefore highlighting the importance and magnitude of hypoglycaemia. The priority for care is to combine effective glycaemic control to prevent diabetic complications, with (in light of recent findings of large studies e.g. ACCORD) freedom from hypoglycaemia; providing the healthcare professional and patient with an insulin that allows for comparable glycaemic control, to current basal insulins, but better control of hypoglycaemic events without compromising on safety. The data depicted is the proportion of each group experiencing at least one severe self-reported hypoglycaemic episode during 9–12 months of follow-up. They reported an incidence of severe hypoglycaemia of 110–320 episodes per 100 patient-years in patients with type 1 diabetes. Although hypoglycaemia was less frequent in type 2 diabetes, it becomes progressively more frequent and limiting to glycaemic control later in the course of the disease. Comparing treatment with insulin for 2 years vs. 5 years: Severe hypoglycaemia prevalence was 7 and 25%, respectively, and incidence was 10 and 70 episodes per 100 patient-years, respectively, whereas mild hypoglycaemia prevalence was 51 and 64%, respectively, and incidence was 410 and 1020 episodes per 100 patient-years, respectively. SU, sulphonylurea. UK Hypoglycaemia Study Group. Diabetologia 2007;50:1140–")
29
29 Impaired awareness of hypoglycaemia is associated with higher rate of severe hypoglycaemia (type 1 or type 2) Incidence of severe hypoglycaemia in individuals with impaired awareness of hypoglycaemia Impaired awareness of hypoglycaemia (IAH) is an acquired complication of insulin therapy, which affects people with type 1 and insulin-treated type 2 diabetes, whereby the ability to perceive the onset of hypoglycaemia becomes diminished or absent. Deficiencies of the counter-regulatory hormonal responses to hypoglycaemia usually co-exist. The development of IAH and counter-regulatory failure greatly increases the risk of severe hypoglycaemia. Scoring systems have been developed that can be used in the clinical setting and assist with identification of this group of individuals at risk of severe hypoglycaemia. The mainstay of treatment of IAH is the scrupulous avoidance of hypoglycaemia. Graveling & Frier. Diabetes Metab 2010;36(Suppl. 3):S64–74
 is an acquired complication of insulin therapy, which affects people with type 1 and insulin-treated type 2 diabetes, whereby the ability to perceive the onset of hypoglycaemia becomes diminished or absent. Deficiencies of the counter-regulatory hormonal responses to hypoglycaemia usually co-exist. The development of IAH and counter-regulatory failure greatly increases the risk of severe hypoglycaemia. Scoring systems have been developed that can be used in the clinical setting and assist with identification of this group of individuals at risk of severe hypoglycaemia. The mainstay of treatment of IAH is the scrupulous avoidance of hypoglycaemia. Graveling & Frier. Diabetes Metab 2010;36(Suppl. 3):S64–74.")
30
Patient fear of hypoglycaemia increases with increased severity of hypoglycaemia
HFS: Hypoglycaemia Fear Survey Marrett et al. Diabetes 2008;57(suppl. 1):A174
:A174.")
31
Patients rank fear of severe hypoglycaemia as high as fear of developing chronic complications
Key message: Patients with T1DM ranked their fear of hypoglycaemia as highly as they ranked fear of long-term complications from diabetes, such as blindness and kidney complications. This study evaluated the frequency of mild and severe symptomatic hypoglycaemia in 459 randomly selected outpatients with T1DM on insulin, using a hypoglycaemia survey that was filled out by the patient at home between 2 visits. Methods: Frequency and severity of severe hypoglycaemia were assessed using a survey received by mail that included the number of mild and severe hypoglycaemic episodes within the last week and month prior to receiving the questionnaire, history and present treatment of diabetes, hypoglycaemic symptoms, and personal attitude towards hypoglycaemia indicated on a visual analog scale. Patients were also asked to record the severity and symptoms of hypoglycaemic episodes in a diary for 1 week. Inclusion criteria: Patients were included if they were ≥15 years old, prone for ketosis, on insulin therapy from the time of diagnosis, administered 1 to 3 insulin injections daily, and free of persistent proteinuria. Results: The prospective frequencies of mild and severe hypoglycaemic episodes were 1.8 and patient-1 week-1 Symptomatic hypoglycaemia was more frequent: On working days than during weekends (1.8:1) In the morning than during the afternoon, evening and night (4.5:2.2:1.4:1) The symptoms of hypoglycaemia were nonspecific, heterogeneous and weakened with increasing duration of diabetes 36% of the patients experienced hypoglycaemic coma The frequency of hypoglycaemia was positively, but weakly, correlated with insulin dose, number of injections, percentage unmodified insulin of the total dose and HbA1c The frequency was negatively, but weakly, correlated with age and HbA1c, but not correlated with sex, duration of diabetes or patients’ ratings of worries about mild and severe hypoglycaemia In terms of patients’ attitudes toward hypoglycaemic episodes (ie, worries about developing late diabetic manifestations in the eyes and kidneys or general concern about diabetes during everyday life): Men were less worried than women (p<0.001–0.05) except for severe hypoglycaemic episodes (0.05<p<0.10) Mild hypoglycaemic episodes did not cause much worry Patients expressed almost equal anxiety concerning hypoglycaemic episodes and the risk of late complications of diabetes *Based on patient (n=411, type 1 diabetes) attitudes to hypoglycaemia using a visual analogue scale Pramming et al. Diabetes Med 1991;8:217–22
 In the morning than during the afternoon, evening and night (4.5:2.2:1.4:1) The symptoms of hypoglycaemia were nonspecific, heterogeneous and weakened with increasing duration of diabetes. 36% of the patients experienced hypoglycaemic coma. The frequency of hypoglycaemia was positively, but weakly, correlated with insulin dose, number of injections, percentage unmodified insulin of the total dose and HbA1c. The frequency was negatively, but weakly, correlated with age and HbA1c, but not correlated with sex, duration of diabetes or patients’ ratings of worries about mild and severe hypoglycaemia. In terms of patients’ attitudes toward hypoglycaemic episodes (ie, worries about developing late diabetic manifestations in the eyes and kidneys or general concern about diabetes during everyday life): Men were less worried than women (p<0.001–0.05) except for severe hypoglycaemic episodes (0.05<p<0.10) Mild hypoglycaemic episodes did not cause much worry. Patients expressed almost equal anxiety concerning hypoglycaemic episodes and the risk of late complications of diabetes. *Based on patient (n=411, type 1 diabetes) attitudes to hypoglycaemia using a visual analogue scale. Pramming et al. Diabetes Med 1991;8:217–22.")
32
Hypoglycaemia represents a psychological barrier to effective glycaemic control
Physicians and patients express fear of hypoglycaemia, which may impede effective diabetes management1 To avoid hypoglycaemia, some patients intentionally maintain a state of hyperglycaemia2 Fear of hypoglycaemia extends to family members2 Hypoglycaemia are associated with significantly lower treatment satisfaction and barriers to adherence3 Key message: Fear of hypoglycaemia is pervasive and affects physicians, patients, and patients’ family members. This fear can prevent some physicians from aggressively treating patients to goal and often results in reduced adherence and treatment satisfaction among patients with diabetes. Physicians and patients express fear of hypoglycaemia, which may be an impediment to effective diabetes management1 Desire to avoid hypoglycaemia leads some patients to intentionally compromise glycaemic control and maintain a state of hyperglycaemia2 Fear of hypoglycaemia extends to family members who have had to assist an affected relative during a hypoglycaemic event on previous occasions2 Patient reports of hypoglycaemic symptoms are associated with significantly lower treatment satisfaction and barriers to adherence3 1. Nakar et al. J Diabetes Complications 2007;21:220–6; 2. Frier. Diabetes Metab Res Rev 2008;24:87–92; 3. Alvarez Guisasola et al. Diabetes Obes Metab 2008;10(Suppl. 1):25–32
:25–32.")
33
Higher rate of severe hypoglycaemia with intensive glycaemic control*
*Intensive glycaemic control was defined differently in these trials †Hypoglycaemia requiring any assistance in glucose-lowering trials Conv, conventional therapy; gly, glibenclamide; HR, hazard ratio; ins, insulin; int, intensive therapy; std, standard therapy Key message: although higher rates of severe hypoglycaemia were seen with intensive therapy in these large clinical trials, it is a relatively uncommon event. UKPDS: A randomised, non-blinded clinical trial that investigated the effects of intensive control of blood glucose and blood pressure on micro- and macrovascular complications of T2DM. Participants (n=5102; 58% male) were aged 25–65 years and had fasting plasma glucose >6 mmol/L (108 mg/dL) on two occasions. Participants were randomised to either conventional therapy (dietary restriction) or intensive therapy (either SU or insulin, or in overweight patients, metformin). Severe hypoglycaemia was defined as an event when patients were unable to treat themselves unaided and required third-party help or medical intervention. Significantly more hypoglycaemic episodes were seen in the insulin group vs. the conventional group (p<0.0001).1 ADVANCE: Designed to assess the effects on major vascular outcomes of lowering HbA1c to a target of 6.5% or less in a broad cross-section of patients with T2DM. In this study, 11,140 patients were randomised to receive either standard control (n=5569) or intensive control (n=5571). Participants entered a 6-week run-in period, during which they continued their usual methods of glucose control and received a fixed combination of perindopril and indapamide. Those who tolerated and were adherent with the treatment during the run-in period were randomly assigned to receive continued therapy with either perindopril and indapamide or matching placebo as well as intensive therapy to control HbA1c at ≤6.5% or standard glucose control. Intensive therapy consisted of gliclazide (modified release, 30–120 mg daily); patients who were assigned to this strategy were required to discontinue any other SU. Patients randomised to receive standard therapy and who were taking gliclazide (modified release) when they entered the study were required to replace this drug with another SU if continued therapy was required. Severe hypoglycaemia was more common in the intensive treatment group (p<0.001 vs. standard group).2 ACCORD: Designed to determine whether intensively lowering blood sugar (target HbA1c levels of <6% compared with target HbA1C levels of 7–7.9%) in the setting of aggressive or normal blood pressure (BP) control (systolic BP <120 mmHg, or systolic BP <140 mmHg, respectively), or aggressive low-density lipoprotein cholesterol lowering, with or without triglyceride lowering and high-density lipoprotein cholesterol increasing medication, would reduce the risk of CV events such as heart attack, stroke or CV mortality in people with T2DM with high risk of CV events. The high rate of mortality in the intensive therapy group led to the early termination of the treatment group at 3.5 years. Severe hypoglycaemia was defined as any hypoglycaemia requiring medical assistance. Severe hypoglycaemia was defined as blood glucose <50 mg/dL and transient dysfunction of the central nervous system who were unable to treat themselves and required help from another person. A significantly greater rate of hypoglycaemia occurred in patients in the intensive therapy group (p<0.001 vs. standard therapy).3 VADT: An open-label study targeting 1791 military veterans who had suboptimal response to T2DM therapy. The average age of patients was 60.4 years, and the average disease duration was 11.5 years. Participants were randomised to standard or intensive therapy based on BMI. Patients were stratified to one of four treatment groups: 1. intensive therapy targeting HbA1c 6%, and obesity (BMI ≥27 kg/m2) on oral agents alone; 2. intensive, for lean patients (BMI <27) on OAD; 3. standard therapy targeting HbA1c 8–9% and obesity (BMI ≥27) on OAD; 4. standard therapy, for lean patients (BMI <27) on OAD. Insulin was added for patients in the standard group who did not have HbA1c <9% and in the intensive therapy group <6%.4 Intensive glycaemic control was defined as follows in the above trials: UKPDS1=blood glucose control with either SU or insulin to FPG <108 mg/dL and, in insulin-treated patients, premeal glucose of 72–126 mg/dL; ADVANCE2=use of gliclazide plus other drugs as required to achieve HbA1c ≤6.5%; ACCORD3=comprehensive therapy targeting HbA1c <6.0%; VADT4=in the intensive group, patients were started on maximal doses of 2 OADs (metformin + rosiglitizone if BMI ≥27, glimepiride + rosiglitazone if BMI <27) and, prior to any change in OAD, insulin was added if HbA1c <6% was not achieved. The goal in the intensive group was an absolute reduction in HbA1c of 1.5% compared with the standard control group. References UKPDS Group. Lancet 1998;352:837–53. Patel et al.; ADVANCE Collaborative Group. N Engl J Med 2008;358:2560–72. Gerstein et al.; ACCORD Study Group. N Engl J Med 2008;358:2545–59. Duckworth et al. N Engl J Med 2009;360:129–39. 1. UKPDS Group. Lancet 1998;352:837–53; 2. Patel et al; ADVANCE Collaborative Group. N Engl J Med 2008;358:2560–72; 3. Gerstein et al; ACCORD Group. N Engl J Med 2008;358:2545–59; 4. Duckworth et al. N Engl J Med 2009;360:129–39
 were aged 25–65 years and had fasting plasma glucose >6 mmol/L (108 mg/dL) on two occasions. Participants were randomised to either conventional therapy (dietary restriction) or intensive therapy (either SU or insulin, or in overweight patients, metformin). Severe hypoglycaemia was defined as an event when patients were unable to treat themselves unaided and required third-party help or medical intervention. Significantly more hypoglycaemic episodes were seen in the insulin group vs. the conventional group (p<0.0001).1. ADVANCE: Designed to assess the effects on major vascular outcomes of lowering HbA1c to a target of 6.5% or less in a broad cross-section of patients with T2DM. In this study, 11,140 patients were randomised to receive either standard control (n=5569) or intensive control (n=5571). Participants entered a 6-week run-in period, during which they continued their usual methods of glucose control and received a fixed combination of perindopril and indapamide. Those who tolerated and were adherent with the treatment during the run-in period were randomly assigned to receive continued therapy with either perindopril and indapamide or matching placebo as well as intensive therapy to control HbA1c at ≤6.5% or standard glucose control. Intensive therapy consisted of gliclazide (modified release, 30–120 mg daily); patients who were assigned to this strategy were required to discontinue any other SU. Patients randomised to receive standard therapy and who were taking gliclazide (modified release) when they entered the study were required to replace this drug with another SU if continued therapy was required. Severe hypoglycaemia was more common in the intensive treatment group (p<0.001 vs. standard group).2. ACCORD: Designed to determine whether intensively lowering blood sugar (target HbA1c levels of <6% compared with target HbA1C levels of 7–7.9%) in the setting of aggressive or normal blood pressure (BP) control (systolic BP <120 mmHg, or systolic BP <140 mmHg, respectively), or aggressive low-density lipoprotein cholesterol lowering, with or without triglyceride lowering and high-density lipoprotein cholesterol increasing medication, would reduce the risk of CV events such as heart attack, stroke or CV mortality in people with T2DM with high risk of CV events. The high rate of mortality in the intensive therapy group led to the early termination of the treatment group at 3.5 years. Severe hypoglycaemia was defined as any hypoglycaemia requiring medical assistance. Severe hypoglycaemia was defined as blood glucose <50 mg/dL and transient dysfunction of the central nervous system who were unable to treat themselves and required help from another person. A significantly greater rate of hypoglycaemia occurred in patients in the intensive therapy group (p<0.001 vs. standard therapy).3. VADT: An open-label study targeting 1791 military veterans who had suboptimal response to T2DM therapy. The average age of patients was 60.4 years, and the average disease duration was 11.5 years. Participants were randomised to standard or intensive therapy based on BMI. Patients were stratified to one of four treatment groups: 1. intensive therapy targeting HbA1c 6%, and obesity (BMI ≥27 kg/m2) on oral agents alone; 2. intensive, for lean patients (BMI <27) on OAD; 3. standard therapy targeting HbA1c 8–9% and obesity (BMI ≥27) on OAD; 4. standard therapy, for lean patients (BMI <27) on OAD. Insulin was added for patients in the standard group who did not have HbA1c <9% and in the intensive therapy group <6%.4. Intensive glycaemic control was defined as follows in the above trials: UKPDS1=blood glucose control with either SU or insulin to FPG <108 mg/dL and, in insulin-treated patients, premeal glucose of 72–126 mg/dL; ADVANCE2=use of gliclazide plus other drugs as required to achieve HbA1c ≤6.5%; ACCORD3=comprehensive therapy targeting HbA1c <6.0%; VADT4=in the intensive group, patients were started on maximal doses of 2 OADs (metformin + rosiglitizone if BMI ≥27, glimepiride + rosiglitazone if BMI <27) and, prior to any change in OAD, insulin was added if HbA1c <6% was not achieved. The goal in the intensive group was an absolute reduction in HbA1c of 1.5% compared with the standard control group. References. UKPDS Group. Lancet 1998;352:837–53. Patel et al.; ADVANCE Collaborative Group. N Engl J Med 2008;358:2560–72. Gerstein et al.; ACCORD Study Group. N Engl J Med 2008;358:2545–59. Duckworth et al. N Engl J Med 2009;360:129– UKPDS Group. Lancet 1998;352:837–53; 2. Patel et al; ADVANCE Collaborative Group. N Engl J Med 2008;358:2560–72; 3. Gerstein et al; ACCORD Group. N Engl J Med 2008;358:2545–59; 4. Duckworth et al. N Engl J Med 2009;360:129–39.")
34
Int. Diab. Monitor, 2009;21(6):
:")
35
Adverse outcomes among patients with type 2 diabetes experiencing severe hypoglycaemia
Key message: Severe hypoglycaemia has been associated with an increased risk for diabetes-related complications. The median time from an hypoglycaemic episode to a related adverse event or death was ≤1.6 years. The above data originate from the ADVANCE study. ADVANCE was a factorial trial with two randomised comparisons: a double-blind assessment of the efficacy of perindopril–indapamide in lowering blood pressure, as compared with placebo, and an open-label assessment of the effects of intensive glucose lowering with the use of a modified release formulation of gliclazide as compared with standard, guideline-based glucose lowering on the risks of vascular outcomes and death among patients with type 2 diabetes. During a median follow-up period of 5 years, 231 patients (2.1%) had at least one severe hypoglycaemic episode; 150 had been assigned to intensive glucose control (2.7% of the 5571 patients in that group), and 81 had been assigned to standard glucose control (1.5% of the 5569 patients in that group). This study evaluated the association between severe hypoglycaemia and the risk of diabetes-related complications in patients with T2DM (n=11,140). Methods: Patients were recruited from 215 centres in 20 countries and were included if they had a diagnosis received after the age of 30 years with a history of micro- or macrovascular disease or at least one other cardiovascular risk factor. Glucose control was not part of entry criteria, but patients were excluded if they had a clear indication for long-term insulin use at entry. Patients were randomised to receive blood-pressure lowering medication or placebo and either standard or intensive glucose control with extended-release localised or a standard guideline-based treatment strategy. Severe hypoglycaemia was defined as blood glucose <50 mg/dL and transient dysfunction of the central nervous system, where patients were unable to treat themselves and required help from another person. Results: During the follow-up period of 48 months, 2125 patients had a micro- or macrovascular event, 1031 patients died (45 who reported severe hypoglycaemia) and 87 patients reported severe hypoglycaemia. The events are plotted on the chart above and the median times from the severe hypoglycaemic episode to the event were: first major macrovascular event, 1.56 years; first major microvascular event, 0.99 years; death, 1.05 years; death from a cardiovascular event, 1.31 years; death from a non-cardiovascular cause, 0.74 years. Zoungas. N Engl J Med 2010;363:1410–8, for the ADVANCE Collaborative Group
 had at least one severe hypoglycaemic episode; 150 had been assigned to intensive glucose control (2.7% of the 5571 patients in that group), and 81 had been assigned to standard glucose control (1.5% of the 5569 patients in that group). This study evaluated the association between severe hypoglycaemia and the risk of diabetes-related complications in patients with T2DM (n=11,140). Methods: Patients were recruited from 215 centres in 20 countries and were included if they had a diagnosis received after the age of 30 years with a history of micro- or macrovascular disease or at least one other cardiovascular risk factor. Glucose control was not part of entry criteria, but patients were excluded if they had a clear indication for long-term insulin use at entry. Patients were randomised to receive blood-pressure lowering medication or placebo and either standard or intensive glucose control with extended-release localised or a standard guideline-based treatment strategy. Severe hypoglycaemia was defined as blood glucose <50 mg/dL and transient dysfunction of the central nervous system, where patients were unable to treat themselves and required help from another person. Results: During the follow-up period of 48 months, 2125 patients had a micro- or macrovascular event, 1031 patients died (45 who reported severe hypoglycaemia) and 87 patients reported severe hypoglycaemia. The events are plotted on the chart above and the median times from the severe hypoglycaemic episode to the event were: first major macrovascular event, 1.56 years; first major microvascular event, 0.99 years; death, 1.05 years; death from a cardiovascular event, 1.31 years; death from a non-cardiovascular cause, 0.74 years. Zoungas. N Engl J Med 2010;363:1410–8, for the ADVANCE Collaborative Group.")
36
36 36 Link between hypoglycaemia and acute cardiovascular events in type 2 diabetes Retrospective, observational study (n=860,845) assessing association between hypoglycaemic events and acute cardiovascular events 3.1% patients had a hypoglycaemic event during the evaluation period (1 year) Patients with hypoglycaemic events had 79% higher odds of acute cardiovascular events than patients without hypoglycaemic events The final study cohort comprised 860,845 patients with type 2 diabetes. Patients with hypo events in the evaluation period were significantly older than patients without such events (average age of 64.0 years vs years; p<0.001). Johnston et al. Diabetes Care 2011;34:1164–70
 assessing association between hypoglycaemic events and acute cardiovascular events. 3.1% patients had a hypoglycaemic event during the evaluation period (1 year) Patients with hypoglycaemic events had 79% higher odds of acute cardiovascular events than patients without hypoglycaemic events. The final study cohort comprised 860,845 patients with type 2 diabetes. Patients with hypo events in the evaluation period were significantly older than patients without such events (average age of 64.0 years vs years; p<0.001). Johnston et al. Diabetes Care 2011;34:1164–70.")
37
Pathophysiological cardiovascular consequences of hypoglycaemia
Key message: Hypoglycaemia may cause abnormalities in the cardiovascular system that may increase the risk for cardiovascular events in patients with diabetes. Hypoglycaemia may affect cardiovascular events through increased inflammation, endothelial dysfunction, abnormal sympathoadrenal responses and blood coagulation abnormalities. Inflammatory responses trigger the release of multiple inflammatory markers (C-reactive protein, vascular endothelial growth factor and interleukin-6) and increase the overall levels of inflammatory cytokines that can lead to endothelial injuries and abnormalities in coagulation. The activation of the fibrinolytic system and increased epinephrine levels can also lead to blood coagulation abnormalities through increased neutrophil activation, platelet activation and increased factor VII. The sympathoadrenal response leads to increased catecholamine release, which increases myocardial contractility, workload and cardiac output. Endothelial dysfunction can lead to decreased vasodilation and can place an even greater strain on the cardiovascular system and perpetuate the inability to meet oxygen demands. CRP, C-reactive protein; IL-6, interleukin 6 VEGF, vascular endothelial growth factor Desouza et al. Diabetes Care 2010;33:1389–94
 and increase the overall levels of inflammatory cytokines that can lead to endothelial injuries and abnormalities in coagulation. The activation of the fibrinolytic system and increased epinephrine levels can also lead to blood coagulation abnormalities through increased neutrophil activation, platelet activation and increased factor VII. The sympathoadrenal response leads to increased catecholamine release, which increases myocardial contractility, workload and cardiac output. Endothelial dysfunction can lead to decreased vasodilation and can place an even greater strain on the cardiovascular system and perpetuate the inability to meet oxygen demands. CRP, C-reactive protein; IL-6, interleukin 6 VEGF, vascular endothelial growth factor. Desouza et al. Diabetes Care 2010;33:1389–94.")
38
Laitinen et al. Ann Noninvasive Electrocardiol 2008;13:97–105
Int. Diab. Monitor, 2009;21(6): Abnormalities in: atrioventricular conduction ventricular depolarisation ventricular repolarisation R-wave amplification associated with norepinephrine counter-regulatory response T-wave flattening associated with epinephrine counter-regulatory response Laitinen et al. Ann Noninvasive Electrocardiol 2008;13:97–105
: Abnormalities in: atrioventricular conduction. ventricular depolarisation. ventricular repolarisation. R-wave amplification associated with norepinephrine counter-regulatory response. T-wave flattening associated with epinephrine counter-regulatory response. Laitinen et al. Ann Noninvasive Electrocardiol 2008;13:97–105.")
39
Cardiovascular mortality
In trials in which the reduction of HbA1c was obtained with a higher incidence of hypoglycaemia, CV MORTALITY is increased

40
Multiple logistic regression of acute CV events as a function of hypoglycaemic events
Key message: In a managed care database analysis, hypoglycaemic events led to an increased risk for acute cardiovascular events. A retrospective observational analysis of 860,845 US managed care patients ≥18 years of age with T2DM examined the impact of hypoglycaemic events on acute cardiovascular events over the course of 2 consecutive years of data (2006–2008). A 1-year baseline period identified eligible patients and collected information on clinical and demographic characteristics from September 2006 to September An evaluation period identified hypoglycaemic events and acute cardiovascular events from October 2007 to October 2008. The study examined the association between ICD-9 coded outpatient hypoglycaemic events and acute cardiovascular events (acute myocardial infarction, coronary artery bypass grafting, revascularisation, percutaneous coronary intervention and incident unstable angina). Within the evaluation time period, 3.1% of patients experienced hypoglycaemic events as coded by ICD-9. After controlling for important confounders, this study found that patients with documented outpatient hypoglycaemic events had a 79% higher regression-adjusted odds (odds ratio=1.79; confidence interval= ) of acute cardiovascular events than patients without documented hypoglycaemic events. Further variables such as age, presence of diabetic complications and prior cardiovascular events are shown above. Johnston et al. Diabetes Care 2011;34:1164–70
. A 1-year baseline period identified eligible patients and collected information on clinical and demographic characteristics from September 2006 to September An evaluation period identified hypoglycaemic events and acute cardiovascular events from October 2007 to October The study examined the association between ICD-9 coded outpatient hypoglycaemic events and acute cardiovascular events (acute myocardial infarction, coronary artery bypass grafting, revascularisation, percutaneous coronary intervention and incident unstable angina). Within the evaluation time period, 3.1% of patients experienced hypoglycaemic events as coded by ICD-9. After controlling for important confounders, this study found that patients with documented outpatient hypoglycaemic events had a 79% higher regression-adjusted odds (odds ratio=1.79; confidence interval= ) of acute cardiovascular events than patients without documented hypoglycaemic events. Further variables such as age, presence of diabetic complications and prior cardiovascular events are shown above. Johnston et al. Diabetes Care 2011;34:1164–70.")
41
Hypoglycemia Rates with Basal Insulin Analogs
Little et al., Diab Tech & Ther 2011, Volume 13, Supplement 1, S53

42
Relationship of hypoglycaemia rate and HbA1c target
NPH Basal Insulin Analogues Target Profile Basal Insulin Analogues Basal Insulin Analogues Adapted from Kolendorf et al. Diabetes 2005; 54 (Suppl 2): P489
: P489.")
43
Conclusion Hypoglycaemia is:
a common side effect of diabetes treatment in both type 1 and type 2 diabetes feared by both physicians and patients linked with cardiovascular and neurological pathophysiology a barrier to effective glycaemic management

Presentazioni simili
 Brussels, 26 settembre 2013.>")













>")

 N. Pazienti in Dialisi (2002: 308.910)>")


