Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Saverio G Parisi Università degli Studi di Padova
HPV Saverio G Parisi Università degli Studi di Padova

2
Malattie Sessualmente Trasmesse….
Candida Chlamydia trachomatis HBV Herpes (HSV, CMV, EBV, HHV6, HHV8) HIV Neisseria gonorrhoeae Sifilide Tricomonas Vaginosi batterica …………………..
 HIV. Neisseria gonorrhoeae. Sifilide. Tricomonas. Vaginosi batterica. …………………..")
4
Malattie Sessualmente Trasmesse….HPV
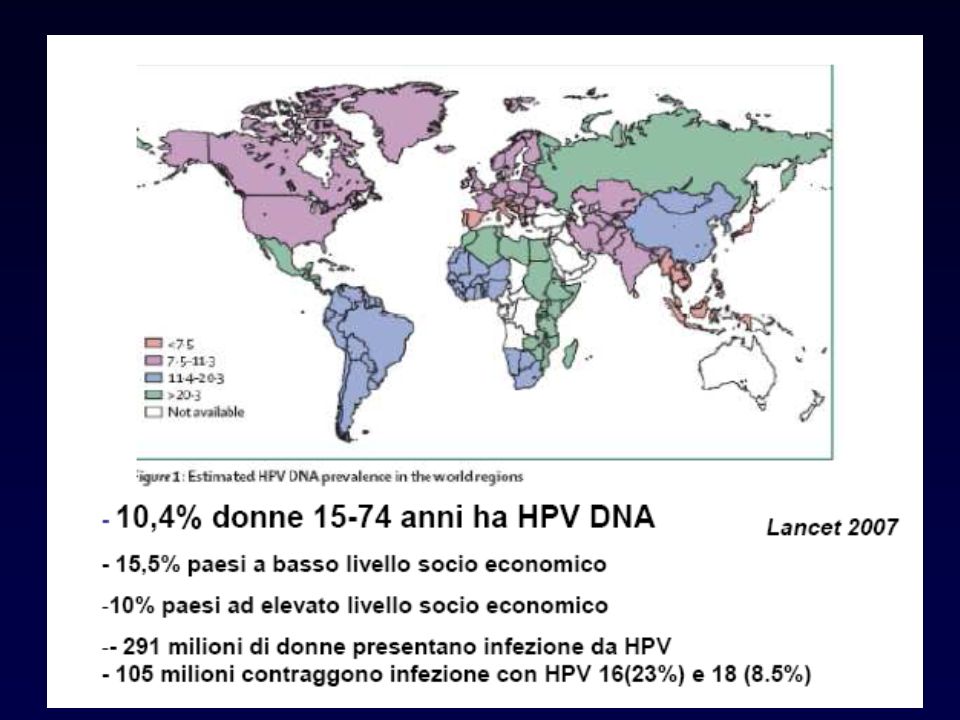
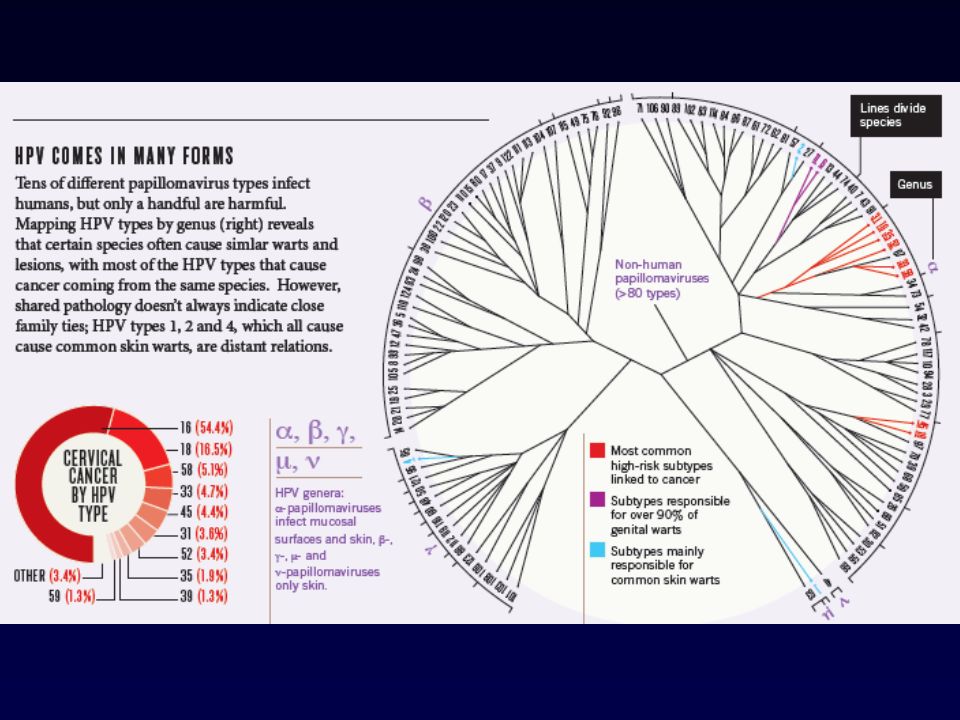
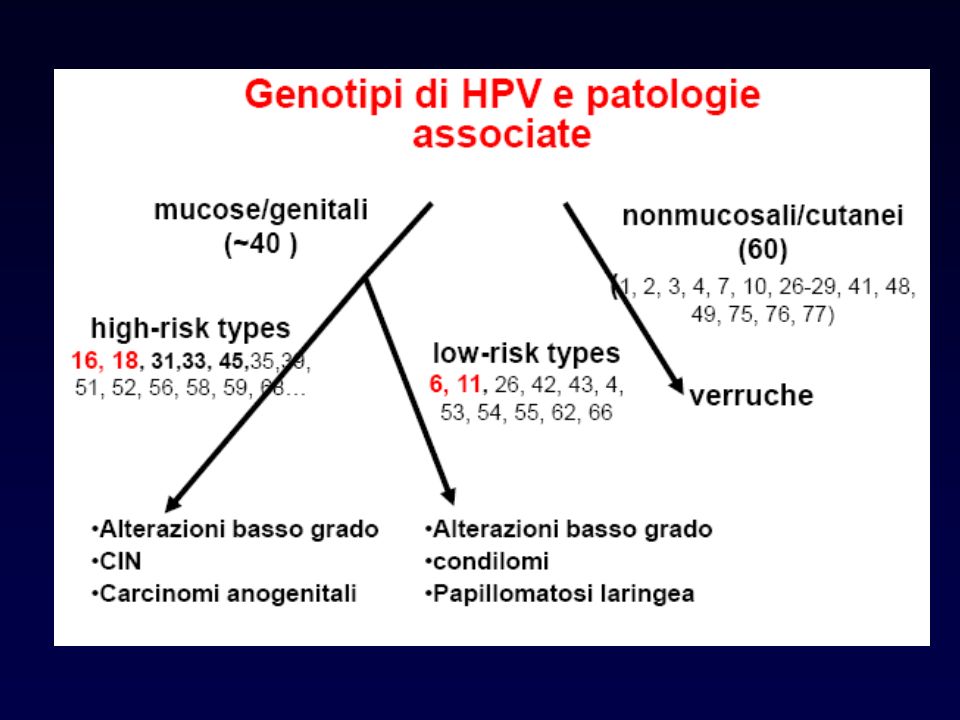
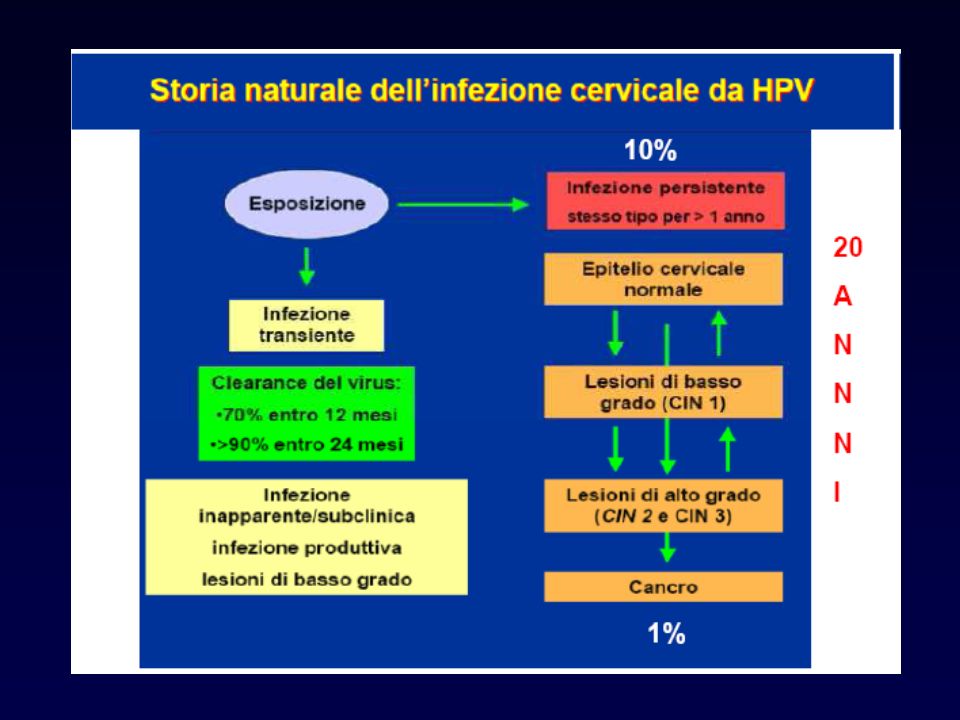
Sono stati identificati più di 100 tipi; circa 40 infettano la regione ano-genitale. Questi sono stati classificati in tipi a basso rischio, associati con verruche ano-genitali e displasia moderata, e tipi ad alto rischio, associati con displasia di alto grado e cancro ano-genitale. Le infezioni ano-genitali da HPV sono la più comune infezione sessualmente trasmessa: La maggioranza delle infezioni sono asintomatiche o subcliniche e divengono non determinabili con il tempo.

17
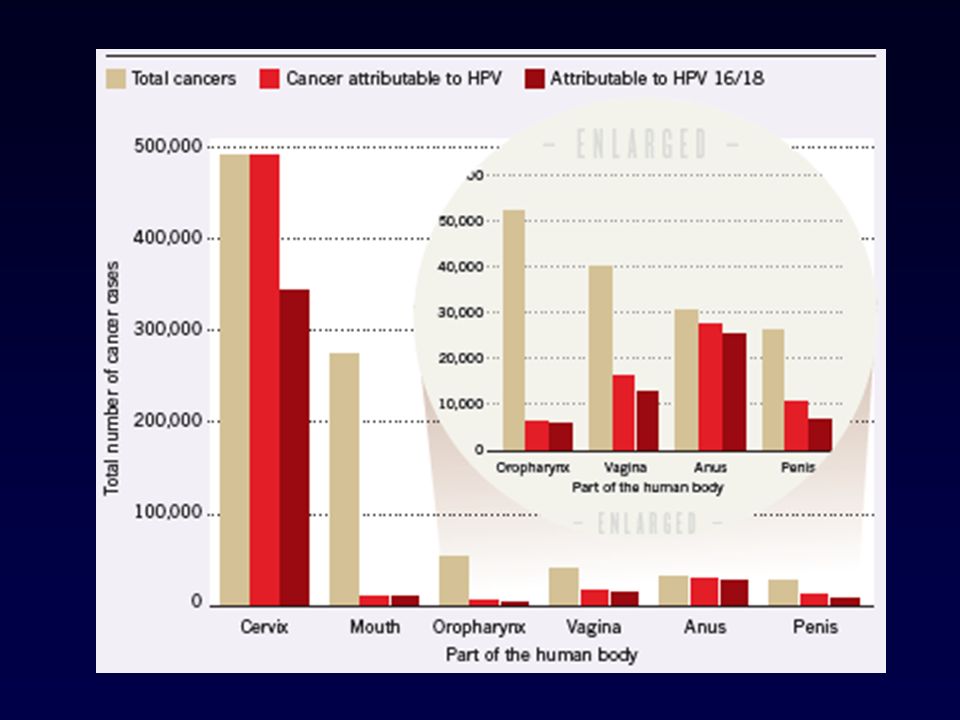
HPV has been definitely associated with human cancers
50% Penile 90% Nonmelanoma skin/cutaneous squamous cell § 20% Oropharyngeal >70% Anal >50% Vulvar* Vaginal* >99% Cervical° % associated with certain HPV types Cancer ° most common cancer in developing countries * includes cancer and intraepithelial neoplasia § immunocompromised patients

28
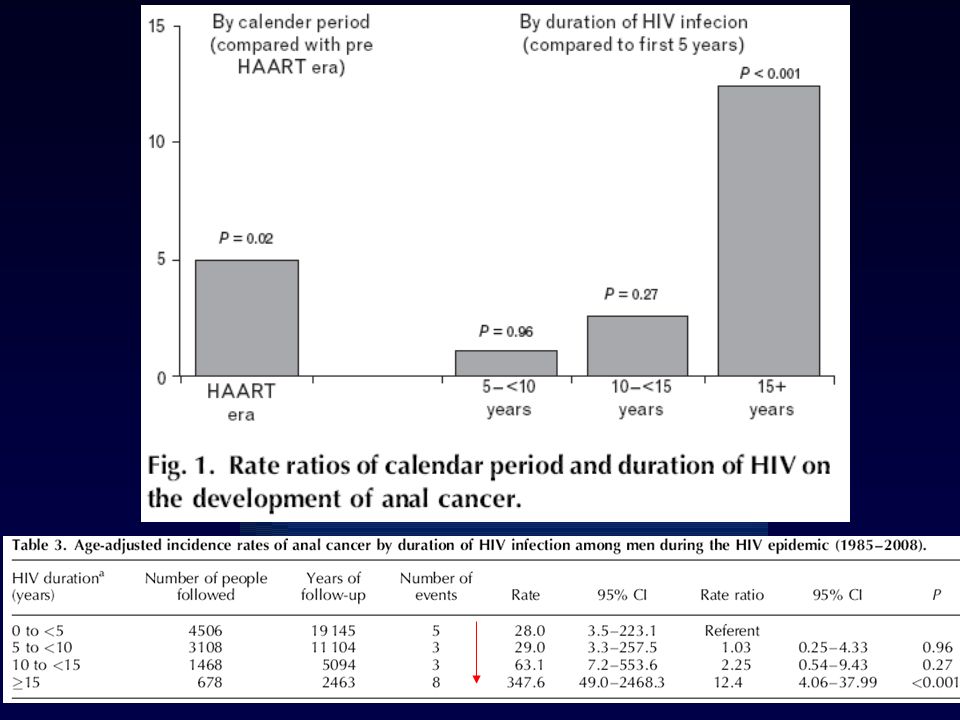
Duration of HAART use was not significantly associated with a decreased risk of anal cancer
Anal cancer among HIV+ is primarily a disease of younger men (median age 42y in this study). This mirrors other studies [Chiao 2008, Piketty 2008] among HIV-positive persons with median ages of 43–49 years and among transplant recipients [Penn 1986]. These ages are significantly younger than the age of occurrence (generally, the sixth decade) among HIV-uninfected persons. Among the general population, only 12% of anal cancers occur at an age of less than 44 years [Horner 2009]; In this study 63% of cases occurred in this age category.
. This mirrors other studies [Chiao 2008, Piketty 2008] among HIV-positive persons with median ages of 43–49 years and among transplant recipients [Penn 1986]. These ages are significantly younger than the age of occurrence (generally, the sixth decade) among HIV-uninfected persons. Among the general population, only 12% of anal cancers occur at an age of less than 44 years [Horner 2009]; In this study 63% of cases occurred in this age category.")
29
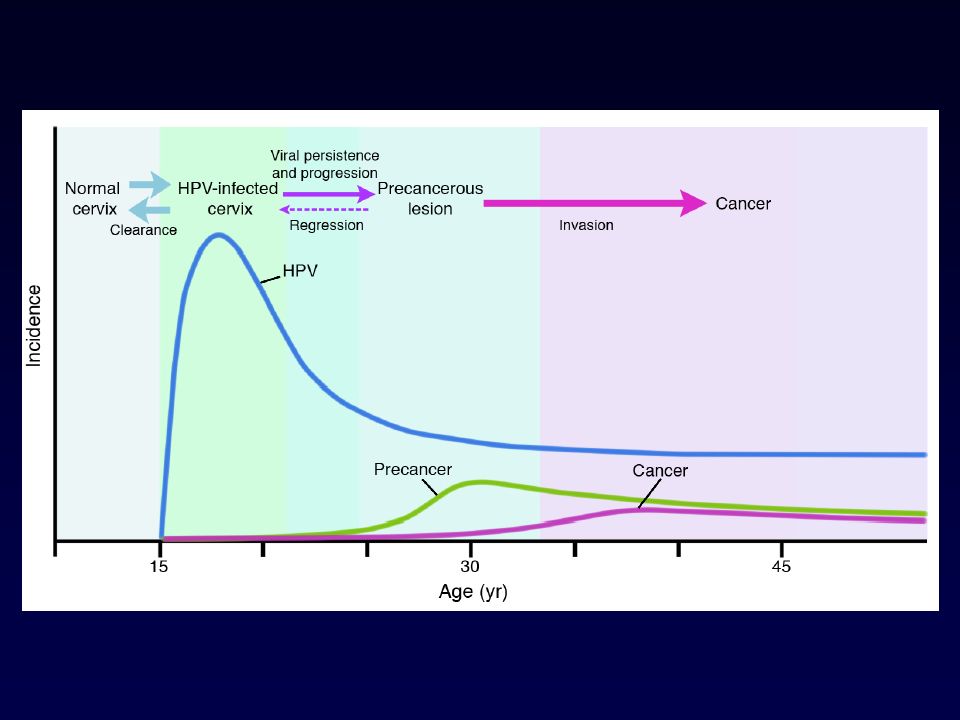
Among persons 18–49 years of age, the standardized rate of anal cancer was 95 per person-years in this HIV cohort as compared with 0.47 in the general population [Joseph 2008]. This suggests that HIV-infected persons may have a shorter time to the development of anal cancer than the general population; immunosuppression and persistent coinfection may accelerate the rate of progression from HPV to cancer. The estimated latency from time of HPV infection to cancer is 5–40 years in general population [Diamond 2005]. Although the time period among HIV-infected persons has not yet been defined, it may be significantly shorter.
![Among persons 18–49 years of age, the standardized rate of anal cancer was 95 per person-years in this HIV cohort as compared with 0.47 in the general population [Joseph 2008].](http://slideplayer.it/slide/1007182/3/images/29/Among+persons+18%E2%80%9349+years+of+age%2C+the+standardized+rate+of+anal+cancer+was+95+per+person-years+in+this+HIV+cohort+as+compared+with+0.47+in+the+general+population+%5BJoseph+2008%5D..jpg "This suggests that HIV-infected persons may have a shorter time to the development of anal cancer than the general population; immunosuppression and persistent coinfection may accelerate the rate of progression from HPV to cancer. The estimated latency from time of HPV infection to cancer is 5–40 years in general population [Diamond 2005]. Although the time period among HIV-infected persons has not yet been defined, it may be significantly shorter.")
33
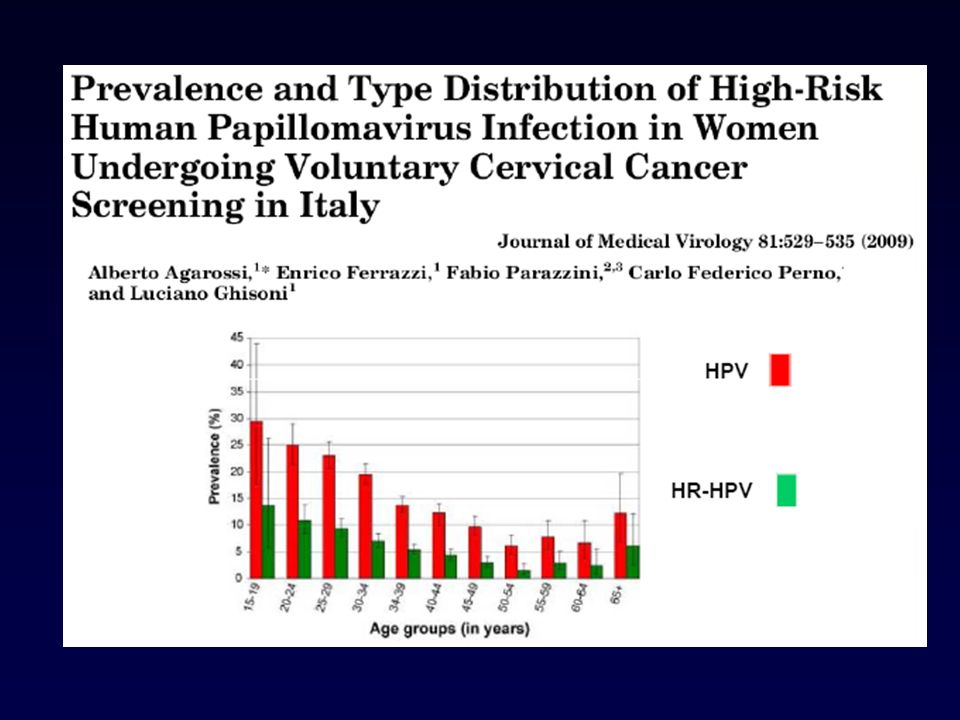
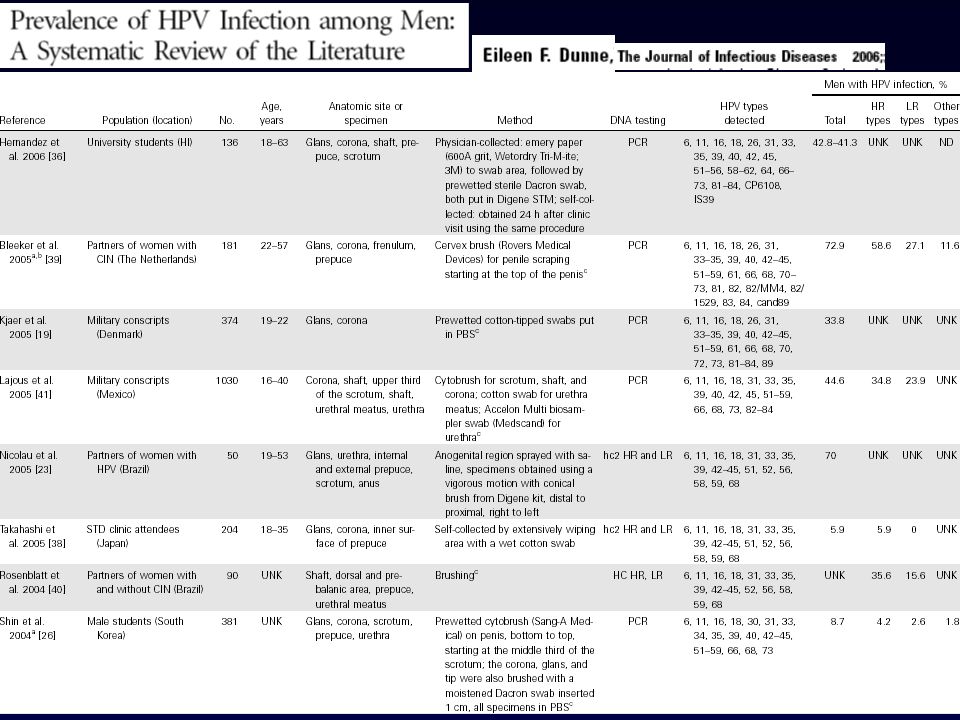
I reali tassi di prevalenza ed incidenza dell’infezione e delle varie manifestazioni cliniche sono di difficile valutazione, in ragione della diversa diffusione, anche nel mondo occidentale, dei programmi di screening nella donna e della differente sensibilità nei vari paesi alla notifica di questa patologia ai sistemi di sorveglianza. Risulta difficile stimare l’infezione senza correlato anatomo-patologico e l’entità del fenomeno nel maschio, che non è sottoposto a programmi di prevenzione e viene diagnosticato solamente in occasione di manifestazioni clinicamente rilevabili. In Italia, dal 1991 al 2005, sono stati segnalati all’ Istituto Superiore di Sanità casi di condilomi genitali, il 74,1% dei quali nel sesso maschile.

39
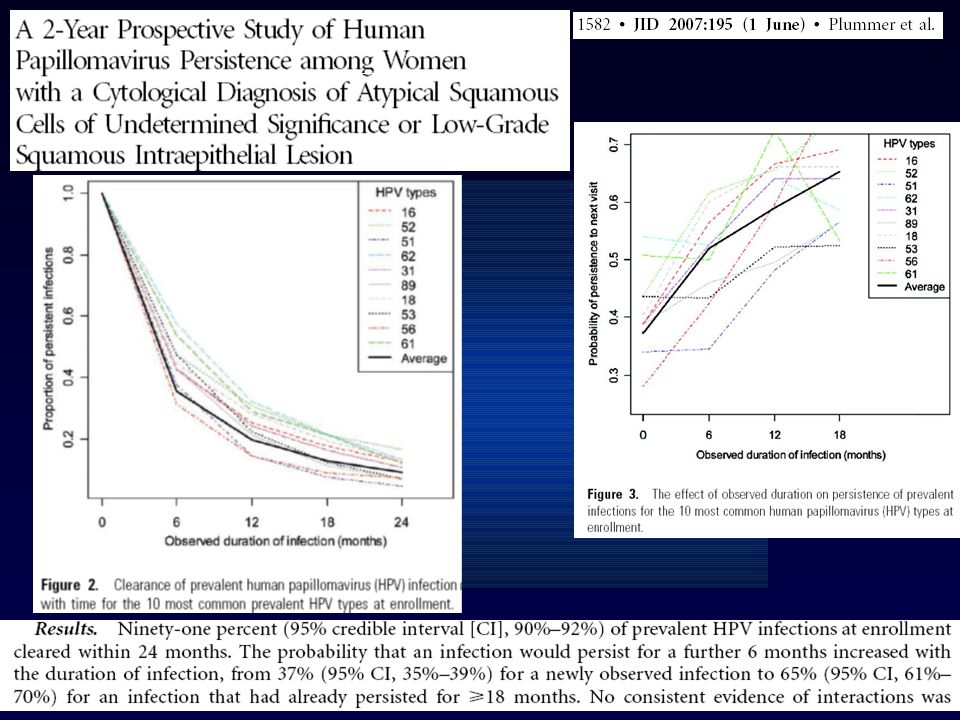
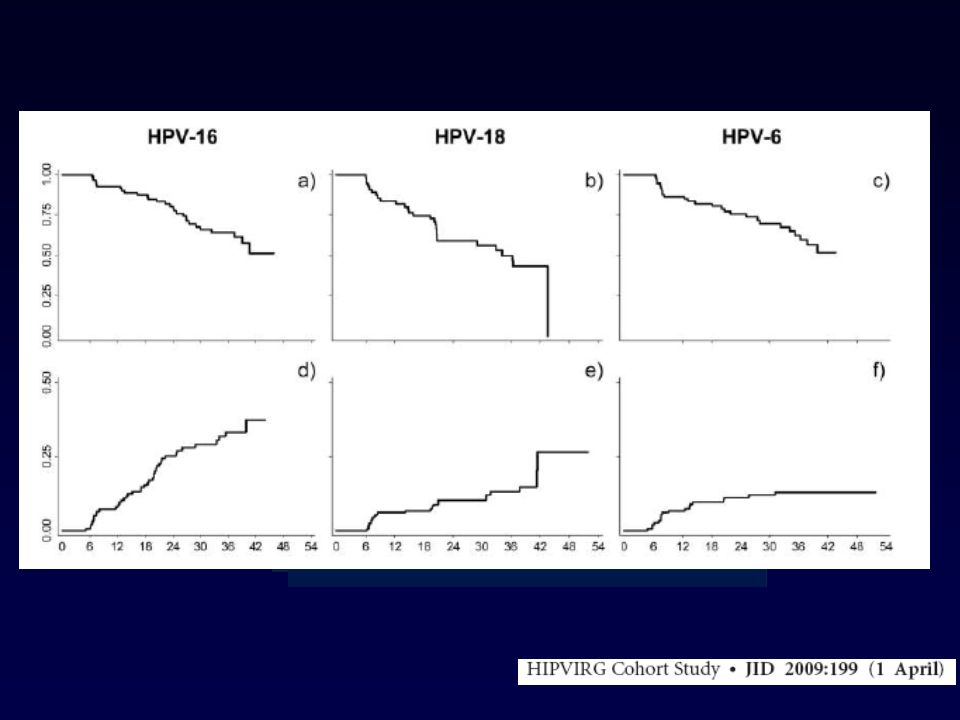
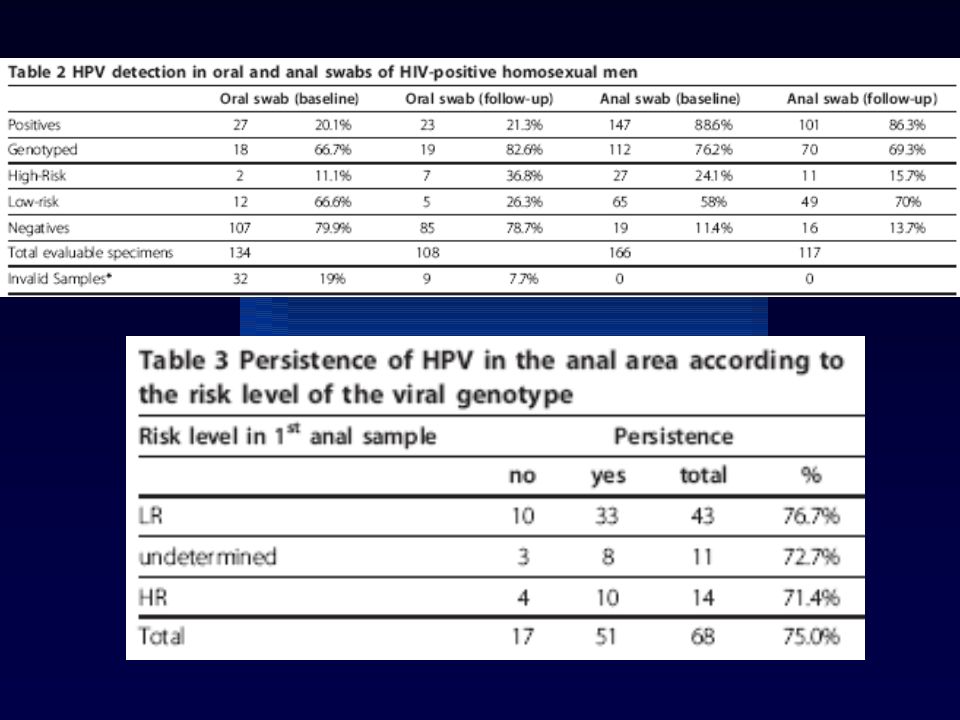
HPV infection was present in 97.9% of the 247 participants at baseline. Most patients (90.9%) were infected with multiple HPV types, with a median number of 5 types per sample (range, 0–18). The median number of high-risk HPVtypes was 3 per sample (range, 0–12) The most prevalent genotypes were HPV-16 (38.2%), HPV-6 (35.3%), HPV-42 (28.6%), HPV-18 (24.5%), HPV-11 (23.2%), HPV-52 (21.6%), HPV-45 (21.2%), and HPV-84 (21.2%) Prevalent HPV-16 infections had the lowest clearance rate and a mean retention time of 36 months
 were infected with multiple HPV types, with a median number of 5 types per sample (range, 0–18). The median number of high-risk HPVtypes was 3 per sample (range, 0–12) The most prevalent genotypes were HPV-16 (38.2%), HPV-6 (35.3%), HPV-42 (28.6%), HPV-18 (24.5%), HPV-11 (23.2%), HPV-52 (21.6%), HPV-45 (21.2%), and HPV-84 (21.2%) Prevalent HPV-16 infections had the lowest clearance rate and a mean retention time of 36 months.")
41
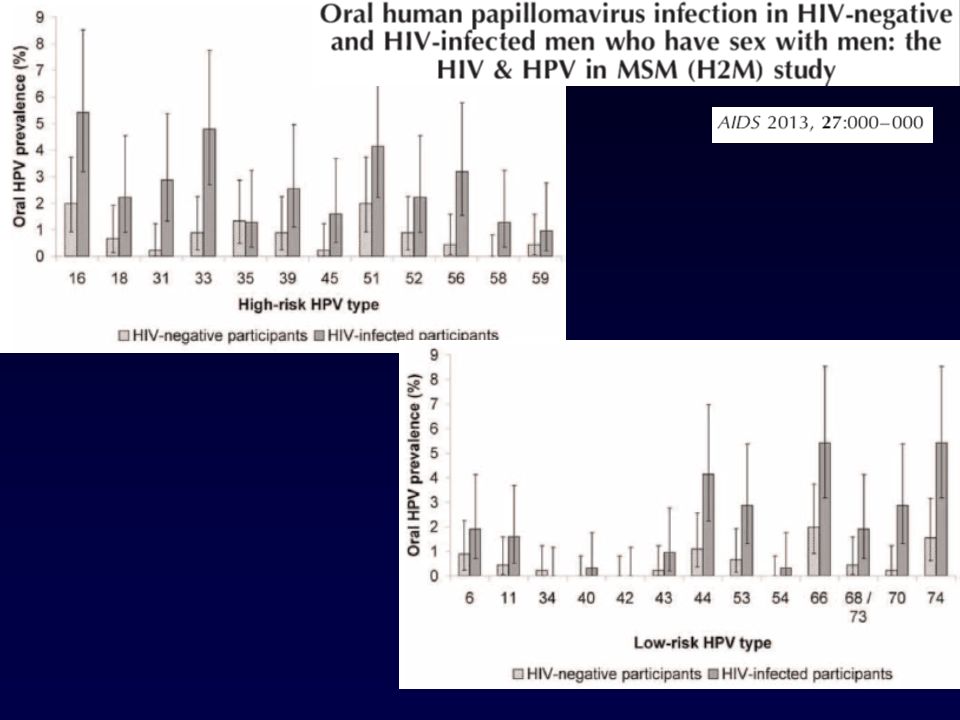
A comparative study in HIV+ and HIV-ve adults showed that HIV+ individuals were more likely
- to have an oral HPV infection (25.3 vs. 7.6%), - to be infected with a HR HPV type (13.7 vs. 4.5%), - to be infected with multiple HPV types (5.8 vs. 1.5%). Oral mucosa abnormalities such as leukoplakia, erythroplakia, and papillomas were also more frequent in HIV+. In multiple logistic regression, the odds of oral HPV infection in HIV+ patients increased with low CD4 cell counts (<200 cells/ml), HSV-2 seropositivity, mucosa abnormalities, and more than one oral sex partner within the last year
, - to be infected with a HR HPV type (13.7 vs. 4.5%), - to be infected with multiple HPV types (5.8 vs. 1.5%). Oral mucosa abnormalities such as leukoplakia, erythroplakia, and papillomas were also more frequent in HIV+. In multiple logistic regression, the odds of oral HPV infection in HIV+ patients increased with low CD4 cell counts (<200 cells/ml), HSV-2 seropositivity, mucosa abnormalities, and more than one oral sex partner within the last year.")
42
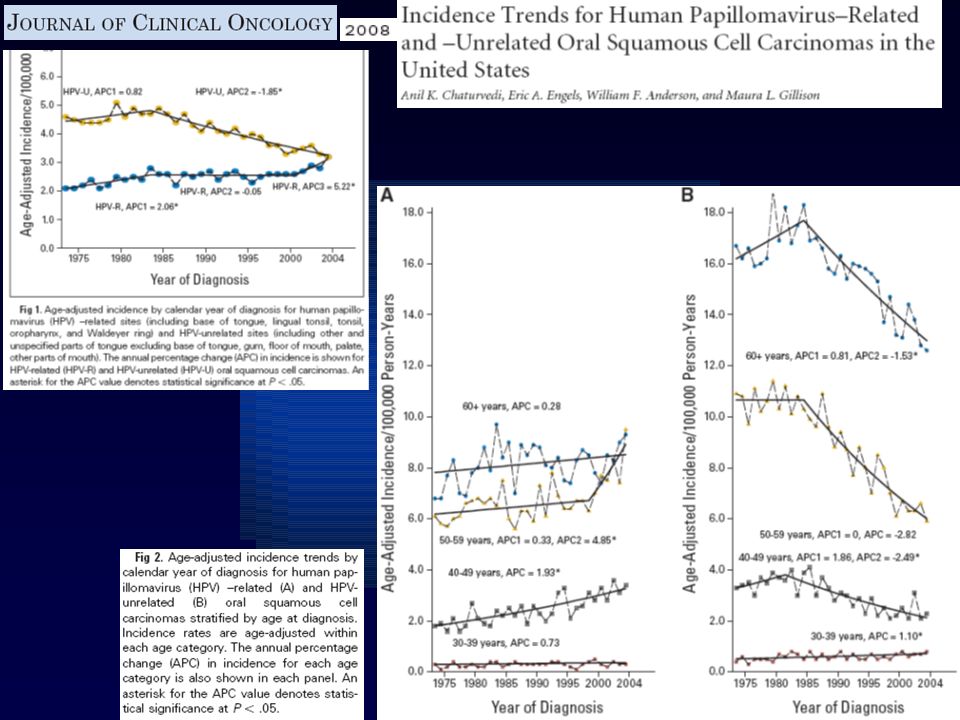
HPV infection is associated with a subset of oral squamous cell carcinoma (OSCC), especially those
arising from the base of the tongue and tonsils. Although the incidence of HPV-unrelated OSCCs associated with tobacco and alcohol use has been shown to decline over the last decades, OSCCs related to HPV significantly increased, particularly among white men and at younger ages [Chaturvedi 2008]. This seems to be a result of changes in sexual behaviors. Given the standardized incidence ratios of 2.32 for OSCCs in HIV+ persons, attention should be paid to this particular type of oral cancer, especially in HIV+ MSM [Grulich 2007].

45
HPV infection in HIV infected Man who Have sex with Man (MSM) and correlation with HHV8 shedding ICAAC To evaluate HPV genotypes circulation and persistence or re-infection over time in different sampling sites among HIV-MSM To evaluate other co-infections, i.e. HHV8 oral shedding and syphilis

46
Methods Samples obtained from rectal mucosa (RS) and pharyngeal-swabs (PhS) of 166 MSM HIV-pts, prospectively recruited from December 2007 to August 2009, were studied for presence of HPV-DNA. Amplification products were sequenced by in-house method using ABI PRISM 3130 XL. Exclusion criteria were being already diagnosed or treated for HPV-anal lesions. In paired samples HHV8-DNA oral shedding was studied.

47
A study including subjects was performed to investigate the frequency and persistence over a 6-month interval

51
Centro Med Prev VR M Cruciani Mal Infettive Mestre A Barelli Mal Infettive Padova R Scaggiante Microbiologia Padova G Palù C Boldrin S Andreis S Pagni F Dal Bello

60
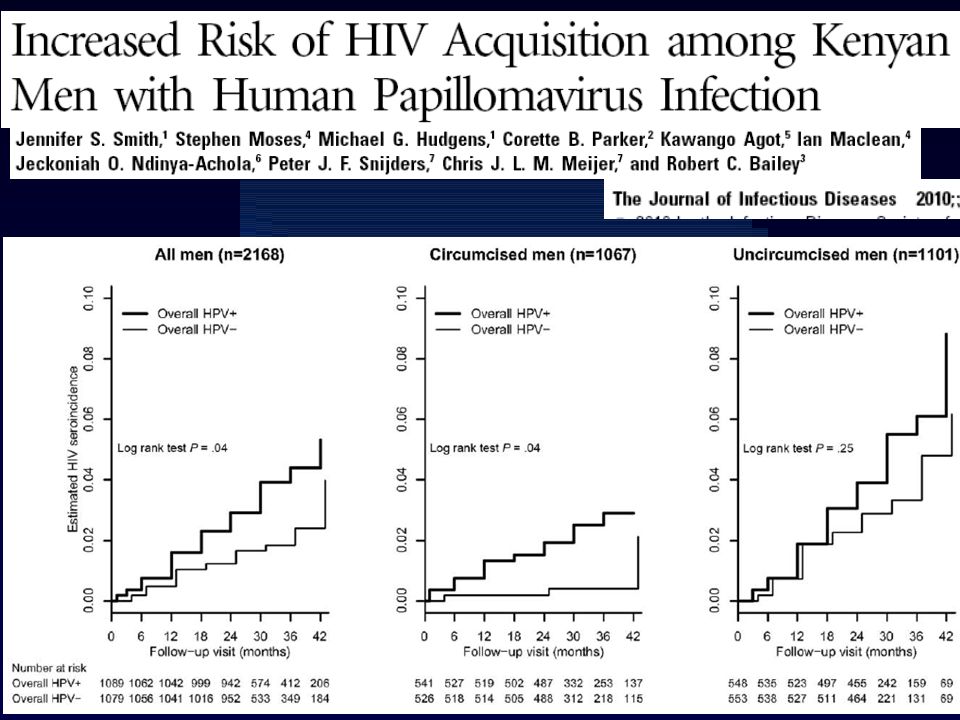
In terms of biological plausibility, HPV infection, unlike many other sexually transmitted infections, is localized to epithelial cells, thus limiting exposure of the virus to the immune system. Although HPV infection alone is not generally characterized by the induction of notable inflammatory responses, an up-regulation of T cells has been observed during the clearance of genital warts and cervical lesions in women, thus resulting in a higher number of HIV-susceptible cells. Alternatively, HPV-associated flat lesions and penile intraepithelial neoplasia in men are characterized by inflammatory infiltrates with hyperemic blood vessels, which may potentially enhance susceptibility to HIV infection by creating portals of HIV entry. HPV and HPV-associated genital lesions may also induce the local production of specific cytokines (ie, macrophage inflammatory protein 3 and interleukin 8), which may in turn increase HIV susceptibility. Bias: HPV infection rather than the detection of HPV-associated clinical outcomes,
, which may in turn increase HIV susceptibility. Bias: HPV infection rather than the detection of HPV-associated clinical outcomes,")
61
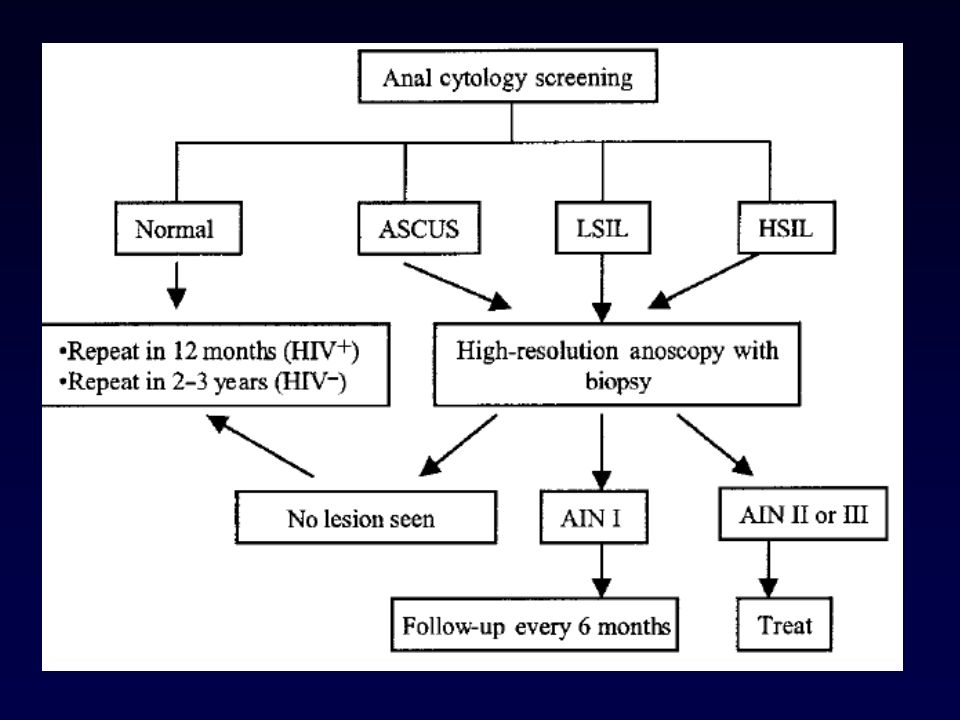
In considerazione della prevalenza dell’infezione, nel maschio HIV+ marcatamente aumentata, è stato proposto, tra gli altri, un protocollo per lo screening della AIN [Palefsky JAIDS 1997] consistente in un esame citologico seguito da una conferma dello stadio di malattia attraverso anoscopia ad alta risoluzione e biopsia ad opera di uno specialista in presenza di un rilievo di anormalità (ASCUS, LG-AIN, HG-AIN). Il grado di severità della AIN deve infatti essere confermato con analisi istopatologica/bioptica, non essendo sempre sufficiente l’esame citologico, soprattutto per le lesioni più lievi.
![In considerazione della prevalenza dell’infezione, nel maschio HIV+ marcatamente aumentata, è stato proposto, tra gli altri, un protocollo per lo screening della AIN [Palefsky JAIDS 1997]](http://slideplayer.it/slide/1007182/3/images/61/In+considerazione+della+prevalenza+dell%E2%80%99infezione%2C+nel+maschio+HIV%2B+marcatamente+aumentata%2C+%C3%A8+stato+proposto%2C+tra+gli+altri%2C+un+protocollo+per+lo+screening+della+AIN+%5BPalefsky+JAIDS+1997%5D.jpg "consistente in un esame citologico seguito da una conferma dello stadio di malattia attraverso anoscopia ad alta risoluzione e biopsia ad opera di uno specialista in presenza di un rilievo di anormalità (ASCUS, LG-AIN, HG-AIN). Il grado di severità della AIN deve infatti essere confermato con analisi istopatologica/bioptica, non essendo sempre sufficiente l’esame citologico, soprattutto per le lesioni più lievi.")
62
- MSM, indipendentemente dalla sierologia per HIV [Palefsky],
Sono state proposte linee guida per lo screening di specifiche popolazioni a rischio, quali: - MSM, indipendentemente dalla sierologia per HIV [Palefsky], - donne con cancro della cervice, malattia vulvare di alto grado o cancro, tutti i soggetti, uomini e donne, infetti da HIV, soggetti con condilomi acuminati dell’ano, soggetti riceventi trapianto [Sillman FH Ann Transplant 1997].
![- MSM, indipendentemente dalla sierologia per HIV [Palefsky],](http://slideplayer.it/slide/1007182/3/images/62/-+MSM%2C+indipendentemente+dalla+sierologia+per+HIV+%5BPalefsky%5D%2C.jpg "Sono state proposte linee guida per lo screening di specifiche popolazioni a rischio, quali: - MSM, indipendentemente dalla sierologia per HIV [Palefsky], - donne con cancro della cervice, malattia vulvare di alto grado o cancro, tutti i soggetti, uomini e donne, infetti da HIV, soggetti con condilomi acuminati dell’ano, soggetti riceventi trapianto. [Sillman FH Ann Transplant 1997].")
75
Grazie dell’attenzione

Presentazioni simili























>")






