Scaricare la presentazione
1
C. Giannattasio HEART FAILURE & Co. Milano 9 - 10 aprile 2010
Tenth International Symposium HEART FAILURE & Co. CARDIOLOGY SCIENCE UPDATE FEMALE DOCTORS SPEAKING ON FEMALE DISEASES Milano aprile 2010 C. Giannattasio

2
Prevalence of Cardiovascular Disease in Americans Age 20 and Older by Age and Sex NHANES III: GRAPHIC SOURCE: Heart Disease and Stroke Statistics-2004 Update, American Heart Association. Cardiovascular diseases are more prevalent in younger men. By the age of 65, however, the prevalence of cardiovascular disease begins to be higher in women (1). (1) Heart Disease and Stroke Statistics-2004 Update, American Heart Association. Source: © American Heart Association 2004 2
. (1) Heart Disease and Stroke Statistics-2004 Update, American Heart Association. Source: © American Heart Association")
3
Adjusted cumulative incidence Adjusted cumulative incidence
Cumulative Incidence of CVD Adjusted for the Competing Risk of Death for Men and Women according to Aggregate Risk Factor (RF) Burden at 50 Years of Age Men Women 69% ≥ 2 major RFs 1 major RF ≥ 1 Elevated RF ≥ 1 Not optimal RF All optimal RFs 50% 50% 46% 39% Adjusted cumulative incidence Adjusted cumulative incidence 36% 27% 8% 5% Attained age Attained age Lloyd-Jones DM et al., Circulation 2006; 113: 791 12640 M 3
 Burden at 50 Years of Age. Men. Women. 69% ≥ 2 major RFs. 1 major RF. ≥ 1 Elevated RF. ≥ 1 Not optimal RF. All optimal RFs. 50% 50% 46% 39% Adjusted cumulative incidence. Adjusted cumulative incidence. 36% 27% 8% 5% Attained age. Attained age. Lloyd-Jones DM et al., Circulation 2006; 113: M. 3.")
4
Vi è anche, nelle società occidentali, un’evidente associazione dell’ipertensione con l’età a causa del globale incremento dei valori medi di pressione arteriosa con l’invecchiamento: ciò riguarda soprattutto l’ipertensione sistolica isolata.

5
Distribuzione dei fattori di rischio in Italia in rapporto al sesso
(dati Istituto Superiore di Sanità, anno 2003) 5
 5.")
6
CVD Mortality Trends for Males and Females
(United States: ) Deaths in thousands Years Males Females Rosamond W et al., Circulation 2007; 115: e69 12576 M 6
 Deaths in thousands. Years. Males. Females. Rosamond W et al., Circulation 2007; 115: e M. 6.")
7
Deaths by Cause, Women, Latest Available Year, EU
Respiratory disease 8% Other cancer 12% Injuries and poisoning 4% Breast cancer 4% Lung cancer 2% Colo-rectal cancer 3% Other causes 20% Stomach cancer 1% Other CVD 17% CHD 15% Stroke 14% European Cardiovascular Disease Statistics, 2000 6979 M 7

8
Acute MI Mortality by Age and Sex
SLIDE INFORMATION SOURCE: Vaccarino V. et al. Sex-based differences in early mortality after myocardial infarction. National registry of myocardial infarction 2 participants. N Engl J Med 1999; 341(4): Based on national registry data including 155,565 women and 229,313 men enrolled between June 1994 and January 1998, overall in-hospital mortality during hospitalization for myocardial infarction is 16.7% for women, compared to 11.5% for men(1) Among persons less than 50 years of age, the rate of mortality for women is twice the rate of mortality for men (1). In contrast, for persons over the age of 74 years, there is no statistically significant difference in mortality rates between women and men(1). (1) Vaccarino V. et al. Sex-based differences in early mortality after myocardial infarction. National registry of myocardial infarction 2 participants. N Engl J Med 1999; 341(4): Source: Adapted from Vaccarino N Engl J Med 1999; 341(4): 8
: Based on national registry data including 155,565 women and 229,313 men enrolled between June 1994 and January 1998, overall in-hospital mortality during hospitalization for myocardial infarction is 16.7% for women, compared to 11.5% for men(1) Among persons less than 50 years of age, the rate of mortality for women is twice the rate of mortality for men (1). In contrast, for persons over the age of 74 years, there is no statistically significant difference in mortality rates between women and men(1). (1) Vaccarino V. et al. Sex-based differences in early mortality after myocardial infarction. National registry of myocardial infarction 2 participants. N Engl J Med 1999; 341(4): Source: Adapted from Vaccarino N Engl J Med 1999; 341(4):")
9
Prognosis After MI 38% of women die within first year
Compared to 25% of men 35% of women will have second MI within 6 years Compared to 18% of men SLIDE INFORMATION SOURCE: Wenger NK. Cardiovascular health and disease in women problems and prospects. Circulation 2004; 109: Source: Wenger Circulation 2004; 109: 9

10
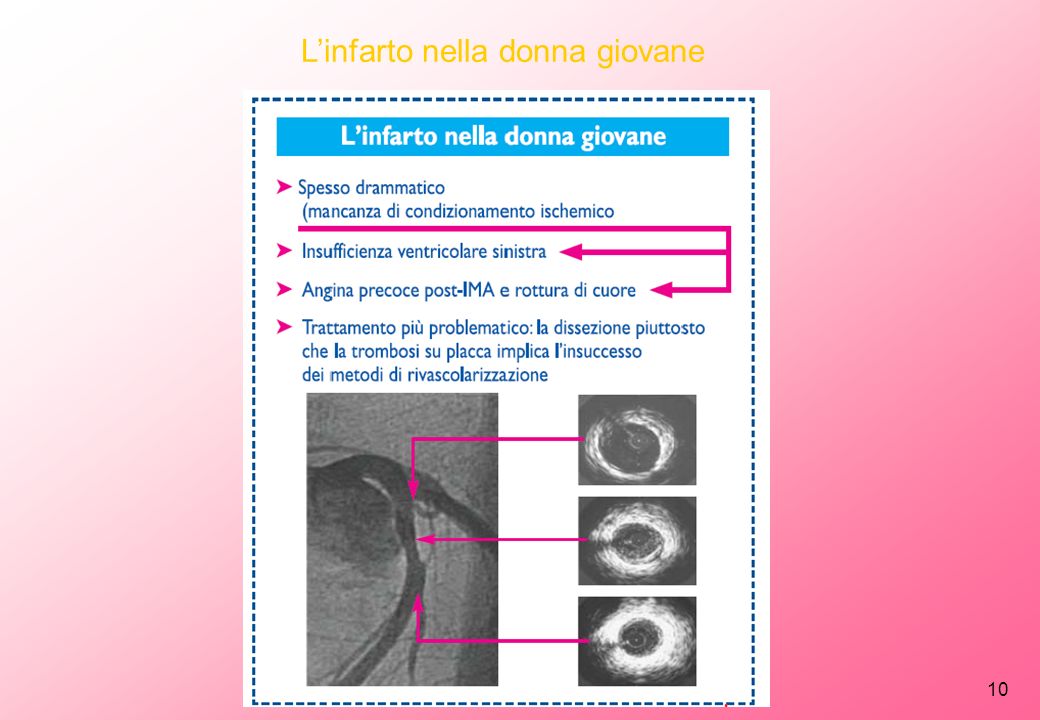
L’infarto nella donna giovane
10 10
11
Diagnosis of Coronary Artery Disease in Women
Chest pain is experienced by most women with CHD, but non-chest pain presentations are more common in women than men Other Presenting Symptoms Upper abdominal pain, fullness, burning sensation Shortness of breath Nausea Neck, back, jaw pain Associations Precipitated by exertion Precipitated by emotional distress SLIDE INFORMATION SOURCES: Charney P. Presenting symptoms and diagnosis of coronary heart disease in women. J Cardiovasc Risk 2002, 9: Goldberg RJ, O’Donnell C, Yarzebski J, et al. Sex differences in symptoms presentation associated with acute myocardial infarction: a population-based perspective. Am Heart J : Coronary artery disease presents more frequently with atypical symptoms in women compared to men (1,2). Gender, race, and other perceptions may affect physicians’ assessment of whether a patient has CHD. Studies using tapes of actresses reading from a script describing CHD symptoms have shown that physicians are less likely to assess CHD in African American women compared to white women and men, and in women with a “hysterical” style compared to those with a more “business-like” presentation(1). (1) Charney P. Presenting symptoms and diagnosis of coronary heart disease in women. J Cardiovasc Risk 2002, 9: (2) Goldberg RJ, O’Donnell C, Yarzebski J, et al. Sex differences in symptoms presentation associated with acute myocardial infarction: a population-based perspective. Am Heart J : Source: Charney Cardiovasc Risk 2002, 9: , Goldberg Am Heart J : 11
. Gender, race, and other perceptions may affect physicians’ assessment of whether a patient has CHD. Studies using tapes of actresses reading from a script describing CHD symptoms have shown that physicians are less likely to assess CHD in African American women compared to white women and men, and in women with a hysterical style compared to those with a more business-like presentation(1). (1) Charney P. Presenting symptoms and diagnosis of coronary heart disease in women. J Cardiovasc Risk 2002, 9: (2) Goldberg RJ, O’Donnell C, Yarzebski J, et al. Sex differences in symptoms presentation associated with acute myocardial infarction: a population-based perspective. Am Heart J : Source: Charney Cardiovasc Risk 2002, 9: , Goldberg Am Heart J :")
12
Value of the Exercise ECG in Women
77 80 68 70 70 61 60 50 40 Men Women 30 20 SLIDE INFORMATION SOURCE: Kwok Y, et al. Meta-analysis of exercise testing to detect coronary artery disease in women.. This meta-analysis found that exercise ECG is less accurate in women than in men (1). Mechanisms such as digoxin-like effect of estrogen, different catecholamine response to exercise in women, a higher incidence of mitral valve prolapse, and different chest wall anatomy in women have also been proposed as explanations for accuracy differences (1) . In addition, methods for performing the exercise ECG were developed using men, and the thresholds for abnormal were established almost exclusively in men (1). (1) Kwok Y, et al. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol (5): 10 Sensitivity Specificity Source: Kwok Y, Am J Cardiol (5): 12
. Mechanisms such as digoxin-like effect of estrogen, different catecholamine response to exercise in women, a higher incidence of mitral valve prolapse, and different chest wall anatomy in women have also been proposed as explanations for accuracy differences (1) . In addition, methods for performing the exercise ECG were developed using men, and the thresholds for abnormal were established almost exclusively in men (1). (1) Kwok Y, et al. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol (5): Sensitivity. Specificity. Source: Kwok Y, Am J Cardiol (5):")
13
Women Receive Less Interventions to Prevent and Treat Heart Disease
Less cholesterol screening Less lipid-lowering therapies Less use of heparin, beta-blockers and aspirin during myocardial infarction Fewer referrals to cardiac rehabilitation SLIDE INFORMATION SOURCES: Chandra NC, et al. Observations of the treatment of women in the United States with myocardial infarction; a report from the National Registry of Myocardial Infarction-I. Arch Intern Med 1998; 158: ; Nohria A, et al. Gender differences in coronary artery disease in women: gender differences in mortality after myocardial infarction: why women fare worse than men. Cardiol Clin 1998; 16: Scott LB, Allen JK. Providers perceptions of factors affecting women’s referral to outpatient cardiac rehabilitation programs: an exploratory study. J Cardiopulm Rehab 2004; 24: O’Meara JG, et al. Ethnic and sex differences in the prevalence, treatment, and control of dyslipidemia among hypertensive adults in the GENOA study. Arch Intern Med 2004; 164: Hendrix KH, et al. Ethnic, gender, and age-related differences in treatment and control of dyslipidemia in hypertensive patients. Ethn Dis 2005; 15:11-16. Source: Chandra 1998, Nohria 1998, Scott 2004, O’Meara 2004, Hendrix 2005 13

14
14

15
Mortality in Recent Cohort Studies of Patients Hospitalized
with Heart Failure according to LVEF % death Follow-up (years) 11368 M Hogg et al., JACC 2004; 43: 317 15
 M. Hogg et al., JACC 2004; 43:")
16
Processes Underlying Diastolic Dysfunction
Hypertension Aging Atherosclerosis Diabetes Blood Vessels Hypertrophy Fibrosis Altered elastin & collagen calcification Endothelial dysfunction Loss of compliance Myocardium Hypertrophy (LVH) Fibrosis Cellular dysfunction Ischemia Increased stiffness Impaired relaxation Diastolic Dysfunction Heart Failure with Preserved Systolic Function 9421 M 16
 Fibrosis. Cellular dysfunction. Ischemia. Increased stiffness. Impaired relaxation. Diastolic Dysfunction. Heart Failure with Preserved Systolic Function M. 16.")
18
18 18

19
19

20
20

21
21 21

22
70 70 60 60 50 50 40 40 30 30 Coronary Risk Chart MEN
Risk of Coronary Heart Disease WOMEN Risk of Coronary Heart Disease Non-smoker Smoker Non-smoker Smoker mg/dl 150 200 250 300 mg/dl 150 200 250 300 mg/dl 150 200 250 300 mg/dl 150 200 250 300 mmol/l 4 5 6 7 8 mmol/l 4 5 6 7 8 mmol/l 4 5 6 7 8 mmol/l 4 5 6 7 8 180 age 70 180 180 age 70 180 160 160 160 160 140 140 140 140 120 120 120 120 180 age 60 180 180 age 60 180 160 160 160 160 140 140 140 140 120 120 120 120 SBP (mmHg) 180 180 180 age 50 SBP (mmHg) 180 age 50 160 160 160 160 140 140 140 140 120 120 120 120 180 age 40 180 180 age 40 180 160 160 160 160 140 140 140 140 120 120 120 120 10 Year Risk Level 180 age 30 180 180 Very high High Moderate Mild Low over 40% 20% to 40% 10% to 20% 5% to 10% under 5% age 30 180 160 160 160 160 140 140 140 140 120 120 120 120 mmol/l 4 5 6 7 8 mmol/l 4 5 6 7 8 mmol/l 4 5 6 7 8 mmol/l 4 5 6 7 8 mg/dl 150 200 250 300 mg/dl 150 200 250 300 mg/dl 150 200 250 300 mg/dl 150 200 250 300 Cholesterol Cholesterol Cholesterol Cholesterol 5334 M 22
 age. 50. SBP (mmHg) 180. age age age Year Risk Level age Very high. High. Moderate. Mild. Low. over 40% 20% to 40% 10% to 20% 5% to 10% under 5% age mmol/l mmol/l mmol/l mmol/l mg/dl mg/dl mg/dl mg/dl Cholesterol. Cholesterol. Cholesterol. Cholesterol M. 22.")
23
Staessen JA, 1983 AM J Edipemiol
23

24
Focus sulla sindrome metabolica in menopausa
24

25
Age-Specific Prevalence of the Metabolic Syndrome
among 8814 US Adults, NHANES III, 20-29 30-39 40-49 50-59 60-69 > 70 10 20 30 40 50 Men Women Prevalence (%) Age (years) Ford S et al., JAMA 2002 2328 G
 Age (years) Ford S et al., JAMA G.")
26
Terapia dell’ipertensione nella donna
--I benefici del trattamento antipertensivo sono simili nei due sessi. È tuttavia sconsigliato l’impiego di ACE-inibitori e sartani nelle donne durante il periodo fertile e la gestazione per i potenziali effetti teratogeni Contraccettivi orali La terapia con contraccettivi orali a basso contenuto di estrogeni si associa ad un incremento del rischio di ipertensione,ictus e infarto del miocardio…… Terapia ormonale sostitutiva Le informazioni disponibili suggeriscono che gli unici vantaggi della terapia ormonale sostitutiva sono rappresentati da una minor frequenza di fratture ossee e di neoplasie del colon, mentre è aumentato il rischio di eventi coronarici e tromboembolici, ictus… Linee Guida ESH/ESC 2007

27
Treatment (2) ….Che farmaco usare?
Tutti i farmaci antiipertensivi attraversano la placenta Dati comparativi tra i diversi farmaci riguardanti sia l’efficacia sia la sicurezza fetale e materna sono ancora inadeguati ACE inibitori e ARB controindicati perché teratogeni: stopparli anche nelle donne fertili che stanno programmando una gravidanza! METILDOPA (simpaticolitico centrale). Aldomet os 250 mg x 2/die, max 3 g/die Sicuro per madre e feto, blando antiipertensivo. Effetti collaterali: stipsi, depressione, sonnolenza, secchezza fauci LABETALOLO* (alfa 1 bloccante e beta bloccante non selettivo) 100 mg x 2/die, max 2.4 g/die I beta bloccanti cardioselettivi Beta1 (atenololo) possono ridurre la crescita fetale e placentare. I beta bloccanti non selettivi (propranololo) possono interferire con il rilassamento miometriale (processo beta2 relato) Calcio antagonisti (Adalat* mg/die max 120 mg/die) Sicuri per madre e feto, sebbene non esistano molti studi per Ca antagonisti non diidropiridinici (verapamil, diltiazem), ed amlodipina. Maggiori informazioni per nifedipina * Consigliati anche durante l’allattamento
. Aldomet os 250 mg x 2/die, max 3 g/die. Sicuro per madre e feto, blando antiipertensivo. Effetti collaterali: stipsi, depressione, sonnolenza, secchezza fauci. LABETALOLO* (alfa 1 bloccante e beta bloccante non selettivo) 100 mg x 2/die, max 2.4 g/die. I beta bloccanti cardioselettivi Beta1 (atenololo) possono ridurre la crescita fetale e placentare. I beta bloccanti non selettivi (propranololo) possono interferire con il rilassamento miometriale (processo beta2 relato) Calcio antagonisti (Adalat* mg/die max 120 mg/die) Sicuri per madre e feto, sebbene non esistano molti studi per Ca antagonisti non diidropiridinici (verapamil, diltiazem), ed amlodipina. Maggiori informazioni per nifedipina. * Consigliati anche durante l’allattamento.")









>")






 sottoposto a CABG.>")



