Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
LA COLLABORAZIONE INTERPROFESSIONALE
Claudio Po

2
E questo sarebbe già sufficente

3
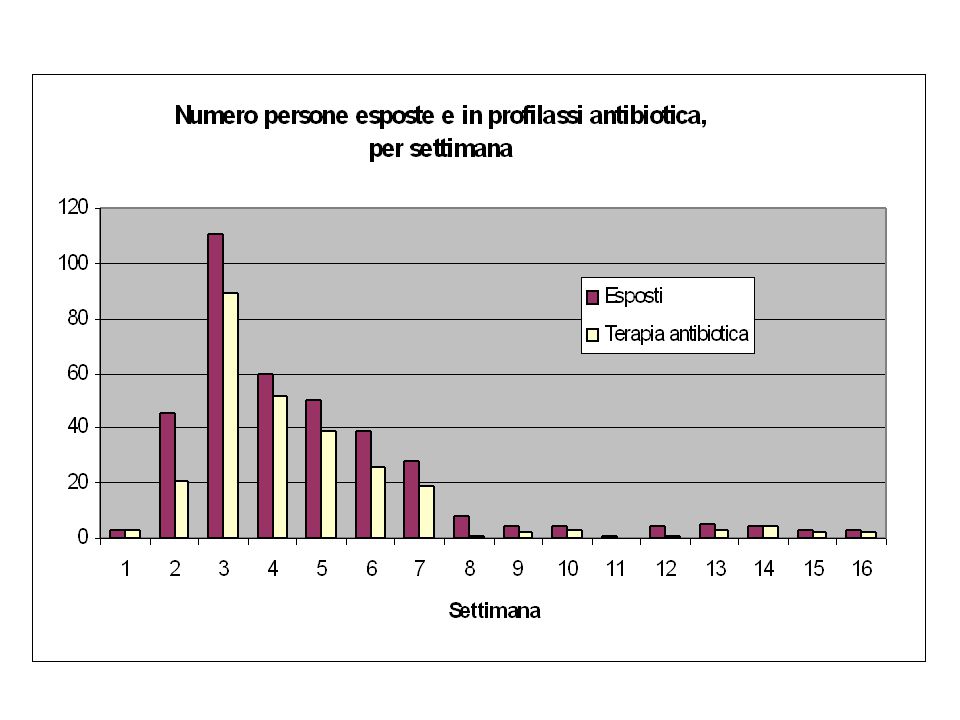
Distribuzione del numero delle Segnalazioni riguardanti il sospetto antrace, per settimana, dal 15 ottobre 2001

12
Scenario - 3 GRANDI MODELLI
MODELLO 3 - Rapido Inizio / Impatto diffuso Poco tempo per la preparazione, risposta reattiva e difensiva MODELLO 2 – Lento inizio / Impatto Moderato e Localizzato Acquisizione lenta dell’infettività nell’uomo. Dipende dall’evoluzione del virus può essere contenuto dopo il suo emergere. Può anche evolvere in una Pandemia Si Impatto Il virus influenzale umano diffonde rapidamente con molti casi ed un aumento della mortalità ? No MODELLO 1 – Estesa Fase 3 OMS / Continui Focolai Epidemici di Influenza Aviare Impatto economico dovuto all’eliminazione dei volatili Si Il virus aviare viene trasmesso efficentemente da uomo a uomo ? No Tempo

18
Reazione allo stress

19
SARS timeline Hotel Metropole Hong Kong Onset of symptoms
February March A B C D E F G H I J K L M The point of the next three slides about SARS is that we don’t know when a bioterrrorist attack actually begins. It happens on a rolling basis, with different start dates in different places. Let’s quickly review the timeline of the SARS epidemic. We believe it probably started in the Fall 2002, when an “Atypical pneumonia” began in Southern China. But, China did not formally announce the epidemic until February , when they announced there had been 305 cases/5 deaths in China. On March 12 WHO released 1st alert. On March 15 the first Canadian cases reported; also in early March, there media reports of New York City business man dying of respiratory illness in Hong Kong. So, when did the sars epidemic really begin? Was it fall 2002 or winter 2003? It depends where you were. In any bioterrorist attack, somebody in some health care facility somewhere will be the first to notice it. And other people in other urban settings around the world will be aware that something has happened – that there’s some infection out there – but maybe large scale procedures won’t have been implemented in your hospital yet. Let’s look at how this played out in SARS. One infected person stayed one night in a hotel in Hong Kong (point to red bar,) Patient A – this is when he stayed there, – and the epidemic spread to 12 people in 6 countries (point to patients B to M). So, patient H was there from Feb 15, and stayed through March 2, and the plus sign indicates when they developed symptoms (optional info on Hotel Metropole) Onset of symptoms Time stayed at Hotel M From Brendan Flannery, PhD, the CDC SARS Investigative Team
 Patient A – this is when he stayed there, – and the epidemic spread to 12 people in 6 countries (point to patients B to M). So, patient H was there from Feb 15, and stayed through March 2, and the plus sign indicates when they developed symptoms (optional info on Hotel Metropole) Onset of symptoms. Time stayed at Hotel M. From Brendan Flannery, PhD, the CDC SARS Investigative Team.")
20
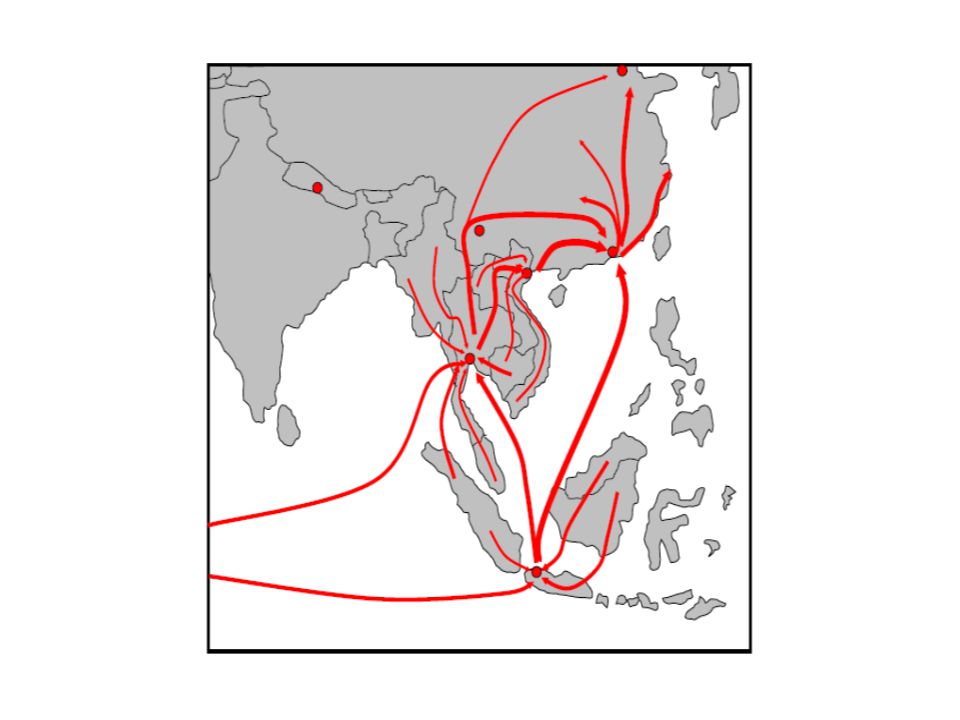
Guangdong Province, China
SARS transmission: Health Care Workers & Families F,G Canada 18 HCW 11 close contacts Guangdong Province, China A A K Ireland 0 HCW H,J A Hong Kong SAR 95 HCW >100 close contacts Hotel M Hong Kong United States 1 HCW I, L,M I,L,M This slide illustrates how an emerging epidemic like SARS – or a bioterrrorist event unfolds. It unfolds VERY DIFFERENTLY from other disasters. We are used to thinking of disasters as basically one time events, that occur once, and then everything else follows. But the disaster itself only occurs once. Think back on 9/11. It happened on one day. This hour period was the “impact phase” Then we have the Acute Phase – the month or so after the disaster. And then the post acute phase. I’m explaining this because in disaster mental health, we conceptualize mental health sequelae in phases. In other words, we often divide psychosocial issues into those you are likely to see in the IMPACT stage, and those you are likely to see in the POST ACUTE STAGE. But that isn’t going to apply so well to a bioterrorist attack because the disaster doesn’t happen once, but rather expands and unfolds. Take a look at this slide. SARS Patient A, that we saw on the last page, was from China, and stayed at the Hotel M on February 21, The disaster was already going on where he was from, in China, in the fall of 02. He went to Hong Kong, and infected patients H and J (point to yellow). 95 HCW were infected from those 3, in Hong Kong, and more than 100 close contacts. Now look at Patient B. He went home to Viet Nam and infected 37 HCW and 21 close contacts. And so forth. It didn’t really hit in Toronto (other side) in Canada until March. So. When was the acute stage? By the way, it actually went away in Toronto, and then new cases emerged in May. A second wave. What is that, another acute stage? My point here is that because of the ongoing expanding nature of a bioterrorist attack, you are likely to see what we think of as “acute stage” presentations of anxiety long after a month after the first infected patient is announced. By the way, in Toronto, there was around a 10% case fatality rate – probably lower in HCW. (Optional editorial comment: OK, NOW. Are you anxious yet?? ) B Vietnam 37 HCW 21 close contacts Singapore 34 HCW 37 close contacts C,D,E
. 95 HCW were infected from those 3, in Hong Kong, and more than 100 close contacts. Now look at Patient B. He went home to Viet Nam and infected 37 HCW and 21 close contacts. And so forth. It didn’t really hit in Toronto (other side) in Canada until March. So. When was the acute stage By the way, it actually went away in Toronto, and then new cases emerged in May. A second wave. What is that, another acute stage My point here is that because of the ongoing expanding nature of a bioterrorist attack, you are likely to see what we think of as acute stage presentations of anxiety long after a month after the first infected patient is announced. By the way, in Toronto, there was around a 10% case fatality rate – probably lower in HCW. (Optional editorial comment: OK, NOW. Are you anxious yet ) B. Vietnam. 37 HCW. 21 close contacts. Singapore. 34 HCW. 37 close contacts. C,D,E.")
21
Example: SARS 8437 Probable Cases
Canada: 250 (Toronto: 242) China: 5327 (Beijing: 2521) (Guangdong: 1511) H.K.: 1755 This slide describes the epidemiology of the SARS epidemic, when it was thought to have concluded in July Though we have used it to illustrate some of the psychosocial issues that would likely arise for ED staff in a bioterrorist attack, there are clearly important ways in which a bioterrorist attack would be very different. First of all, and perhaps most importantly, the SARS epidemic was not intentionally inflicted as an act of war. Also, it’s worth noting that it was a relatively small epidemic causing fewer deaths in 2003 than influenza. A BT attack could be much bigger. Taiwan: 671 Viet Nam: 63 Singapore: 206 As of July 11, Source: WHO
 China: (Beijing: 2521) (Guangdong: 1511) H.K.: This slide describes the epidemiology of the SARS epidemic, when it was thought to have concluded in July Though we have used it to illustrate some of the psychosocial issues that would likely arise for ED staff in a bioterrorist attack, there are clearly important ways in which a bioterrorist attack would be very different. First of all, and perhaps most importantly, the SARS epidemic was not intentionally inflicted as an act of war. Also, it’s worth noting that it was a relatively small epidemic causing fewer deaths in 2003 than influenza. A BT attack could be much bigger. Taiwan: 671. Viet Nam: 63. Singapore: 206. As of July 11, Source: WHO.")
22
Isolamento e Quarantena
Entrambi metodi di contenimento di una infezione Isolamento: separazione di una persona che ha una specifica malattia infettiva, la restrizione dei movimenti ferma la diffusione di una malattia infetiva. Quarantena: separazione e restrizione dei movimenti di una ersona che non è ancora ammalata, ma che è stata esposta ad un agente infettivo e può diventare infetta. Entrambi possono essere volontri o meno. So, let’s briefly touch on Quarantine and Isolation. These are actually legal terms. Quarantine and isolation laws were first enacted in the US in the late 17th century. There are both federal and state laws. States generally have authority to declare and enforce quarantine within their borders. This authority varies widely from stat to state, depending on state laws. The CDC, through its Division of Global Migration and Quarantine, is also empowered to detain, medically examine, or conditionally release persons suspected of carrying certain communicable diseases. (Optional Editorial Comment: Who knew that in New York during the SARS outbreak, there were two people who refused to accept isolation, and public health police were stationed outside their house, to restrict their movement?)
")
23
Total Staffperson-Days on Quarantine = 2035
Toronto Outbreak, Spring 2003 Paramedics on Quarantine Total Staffperson-Days on Quarantine = 2035 The possibility of quarantine and isolation create multiple psychosocial issues. This slide illustrates just one dimension of these issues -- the impact that quarantine can have on the health care work force. Between 80 and 100 paramedics were quarantined for ten days, creating a loss of work of 2,035 days. A big loss of staff, when you really don’t want to be short staffed. Overall, more than 16,000 contacts were placed on isolation in Toronto. 4 Hospitals in Toronto were closed to new pts. Think about the chaotic capacity issues that must have raised for Toronto’s ED’s.

24
Epidemia SARS 2003 Risposta Psicologica Acuta allo Stess
Reazioni dei pazienti: Isolamento, solitudine, stigma Ansietà associata alle puntate febbrili Paura e colpa circa il rischio al benessere di familiari e amici Insonnia Reazioni degli operatori sanitari: Conflitto tra responsabilità lavoro/famiglia Complessità organizzazione del alvoro – 60% assent. Diminuzione - libertà, controllo, autostima Mount Sinai Hospital in Toronto placed 19 cases of SARS in isolation during the first 4 weeks of the outbreak, 11 of these were healthcare workers (Maunder et al., 2003). Quarantine is no picnic. Psychological responses in these patients included boredom, loneliness, and feelings of stigmatization while in respiratory isolation; anxiety whenever their temperatures spiked; fear and guilt that their family and friends may have been exposed; sadness and longing for their families; and insomnia. Staff had a hard time. Issues among hospital staff caring for these patients included conflict between their duty to care for the patients and their worries for the risks this may pose for exposing their own families to SARS. And, they were confronted with the complex fear and challenge when they identify with the victim who is also a fellow health care workers. There was some absenteeism among essential staff. OK, that is the end of the “Real Life Lessons learned from SARS that might apply to a bioterrorist attack” part of our didactic. We’ll wrap up now by reviewing the four core competencies in a bit more detail – and get into the case. (Maunder et al, 2003)
. Quarantine is no picnic. Psychological responses in these patients included boredom, loneliness, and feelings of stigmatization while in respiratory isolation; anxiety whenever their temperatures spiked; fear and guilt that their family and friends may have been exposed; sadness and longing for their families; and insomnia. Staff had a hard time. Issues among hospital staff caring for these patients included conflict between their duty to care for the patients and their worries for the risks this may pose for exposing their own families to SARS. And, they were confronted with the complex fear and challenge when they identify with the victim who is also a fellow health care workers. There was some absenteeism among essential staff. OK, that is the end of the Real Life Lessons learned from SARS that might apply to a bioterrorist attack part of our didactic. We’ll wrap up now by reviewing the four core competencies in a bit more detail – and get into the case. (Maunder et al, 2003)")
25
Come diminuire lo stress ?
Prevedendolo nella Pianificazione e Preparazione Parlando delle paure, ansietà e incertezze con colleghi, amici, familiari Ma anche facendo una pianificazione personale e familiare Con un misurato senso di humor, ed evitando le trappole mediatiche (quickly read over the slide) Everyone has different preparedness needs. Some people like to know EVERYTHING, all about every agent, and every policy, and that’s how they make themselves feel prepared. Other people only want to know where to look up things in the event that they end up needing to know details which aren’t germane to their everyday functioning at this point. Whatever your style, the point is, we want to provide tools to help YOU prepare your OWN preparedness plan, or if you have one, to tailor it to specific issues you may face as an ED staffer.
 Everyone has different preparedness needs. Some people like to know EVERYTHING, all about every agent, and every policy, and that’s how they make themselves feel prepared. Other people only want to know where to look up things in the event that they end up needing to know details which aren’t germane to their everyday functioning at this point. Whatever your style, the point is, we want to provide tools to help YOU prepare your OWN preparedness plan, or if you have one, to tailor it to specific issues you may face as an ED staffer.")
26
GRAZIE PER L’ATTENZIONE

Presentazioni simili









 valorizzando il punto di vista dellindividuo, in linea.>")





>")





