Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
La malattia da Reflusso Istituto Leonardo da Vinci
GIORNATE MEDICHE FIORENTINE 2013 Seminario Arcivescovile Maggiore Firenze, 6/7/8 dicembre 2013 Coordinatori del Congresso: Simone Mininni, Mauro Vannucci La malattia da Reflusso Esofageo Giacomo Trallori Gastroenterologia Istituto Leonardo da Vinci Firenze 1

2
ESOFAGITE DA RELUSSO 2

3
Malattie acido-relate dell’esofago
Reflussi gastrici acidi sono normalmente presenti in esofago In caso di contatto troppo prolungato tali reflussi possono causare flogosi mucosale (esofagite) rilevabile endoscopicamente (malattia da reflusso gastro-esofageo: GERD) Spesso la malattia da reflusso e’ preceduta da una flogosi mucosale non-erosiva (NERD) priva di lesioni endoscopicamente rilevabili The primary symptom of acid-related diseases of the oesophagus is heartburn. The pain of heartburn can be severe and frightening for the patient. It can mimic the pain of a heart attack, so it is important to take seriously any symptoms with sudden onset. On examination, many patients with heartburn have oesophagitis – inflammation of the oesophagus that can be seen on endoscopy. Gastro-oesophageal reflux disease (GORD) is the pathological mechanism by which acid arrives in the oesophagus to cause inflammation/erosion of the oesophageal mucosa. Many patients do not have evidence of oesophagitis and are classified as having non-erosive reflux disease (NERD) – also referred to as endoscopy-negative reflux disease (ENRD) or symptomatic GORD. Barrett’s oesophagus is a pre-cancerous lesion. Throughout this presentation, GORD is equivalent to gastro-esophageal reflux disease, GERD. 3
 rilevabile endoscopicamente (malattia da reflusso gastro-esofageo: GERD) Spesso la malattia da reflusso e’ preceduta da una flogosi mucosale non-erosiva (NERD) priva di lesioni endoscopicamente rilevabili. The primary symptom of acid-related diseases of the oesophagus is heartburn. The pain of heartburn can be severe and frightening for the patient. It can mimic the pain of a heart attack, so it is important to take seriously any symptoms with sudden onset. On examination, many patients with heartburn have oesophagitis – inflammation of the oesophagus that can be seen on endoscopy. Gastro-oesophageal reflux disease (GORD) is the pathological mechanism by which acid arrives in the oesophagus to cause inflammation/erosion of the oesophageal mucosa. Many patients do not have evidence of oesophagitis and are classified as having non-erosive reflux disease (NERD) – also referred to as endoscopy-negative reflux disease (ENRD) or symptomatic GORD. Barrett’s oesophagus is a pre-cancerous lesion. Throughout this presentation, GORD is equivalent to gastro-esophageal reflux disease, GERD. 3.")
4
GERD/NERD: Epidemiologia
La malattia da reflusso gastro-esofageo e’ una delle più frequenti patologie del tratto gastrointestinale Il 15% della popolazione ha almeno una volta la settimana pirosi e/o rigurgito Incidenza maggiore nei maschi e > 50 anni Incidenza in aumento (obesità, stile di vita)
")
5
MECCANISMI ANTI-REFLUSSO
LES (Sfintere esofageo inferiore) Pilastri diaframmatici Angolo di His Peristalsi esofagea Gravità Saliva Barriera epiteliale Barriera anatomica anti-reflusso Clearance fisiologica esofagea
 Pilastri diaframmatici. Angolo di His. Peristalsi esofagea. Gravità. Saliva. Barriera epiteliale. Barriera anatomica anti-reflusso. Clearance fisiologica esofagea.")
6
GERD: patogenesi multifattoriale
Fattori gastrici Fattori esofagei Ritardato svuotamento gastrico Incoordinazione motoria gastro-duodenale (reflusso biliare) Rilasciamenti transitori ed inappropriati del LES Ipotonia del LES Ridotta clearance esofagea Diminuita resistenza della mucosa esofagea Altri fattori Discinesia colecistica Incoordinazione motoria intestinale SIBO/CBO Patologie del colon Patolgie del rachide 6
 Rilasciamenti transitori ed inappropriati del LES. Ipotonia del LES. Ridotta clearance esofagea. Diminuita resistenza della mucosa esofagea. Altri fattori. Discinesia colecistica. Incoordinazione motoria intestinale. SIBO/CBO. Patologie del colon. Patolgie del rachide. 6.")
7
GERD/NERD: Fattori di rischio
Età avanzata Obesità/ sovrappeso Familliarità Ernia hiatale Sclerodermia DIETA It is important to investigate the presence of possible risk factors for GORD. A German study among patients in general practice found that axial hiatus hernia, positive family history, advancing age, being overweight, female gender and treatment with NSAIDs or aspirin were significant risk factors in the development of GORD. Evidence also shows that smoking and psychological stress are risk factors for GORD symptoms. Some data suggest that caffeine consumption can aggravate symptoms of GORD but the evidence is inconclusive. A common cause of oesophagitis is drug-induced injury – particularly when medications are taken at bedtime or without fluids. Farmaci Fumo Stress psicologico 7

8
Sintomi tipici e atipici e complicazioni
Patologie esofagee acido-correlate Sintomi tipici e atipici e complicazioni 8

9
Modalità di presentazione del GERD
Sintomi tipici Pirosi Rigurgito The classic symptom of GORD is heartburn, with or without regurgitation. Patients may or may not have evidence of oesophagitis. There are also atypical symptoms, including chest pain, hoarseness and asthma, so it is important to consider GORD when patients present with these symptoms. Patients with GORD may develop complications, some of which are very serious. Background information on some of these symptoms is given in the next few slides. 9

10
Modalità di presentazione del GERD
Sintomi tipici Sintomi atipici Pirosi Dolore toracico Disfagia Rigurgito Raucedine (“laringite da reflusso”) The classic symptom of GORD is heartburn, with or without regurgitation. Patients may or may not have evidence of oesophagitis. There are also atypical symptoms, including chest pain, hoarseness and asthma, so it is important to consider GORD when patients present with these symptoms. Patients with GORD may develop complications, some of which are very serious. Background information on some of these symptoms is given in the next few slides. Asma, tosse cronica, dispnea Erosioni dei denti 10
 The classic symptom of GORD is heartburn, with or without regurgitation. Patients may or may not have evidence of oesophagitis. There are also atypical symptoms, including chest pain, hoarseness and asthma, so it is important to consider GORD when patients present with these symptoms. Patients with GORD may develop complications, some of which are very serious. Background information on some of these symptoms is given in the next few slides. Asma, tosse cronica, dispnea. Erosioni dei denti. 10.")
11
Meccanismi alla base dei sintomi asmatici causati da reflusso esofageo
Reflussi acidi esofagei con microaspirazioni bronchiali Aumentata reattività bronchiale con broncocostrizione Riflesso esofageo-bronchiale vago-mediato Oesophageal acid has two major effects on respiratory symptoms: bronchoconstriction increasing minute ventilation and respiratory rate. This results in a worsening of the symptoms of asthma. Reproduced with permission. 11

12
Effetti di una terapia antiacida sui sintomi polmonari e gastrici in pazienti con asma
14 Sintomi polmonari Sintomi gastrici (n=25) 12 Score dei sintomi 10 8 6 4 2 A double-blind, placebo-controlled, crossover study conducted with omeprazole 40 mg/day in 107 asthma patients with GORD. Weekly pulmonary (cough, dyspnoea and wheezing) and gastric (regurgitation, heartburn and chest pain) symptoms scores fell during omeprazole therapy. There was a significant improvement in the gastric symptom score with omeprazole compared to placebo (p=0.0001). While pulmonary symptom scores also improved with omeprazole compared to placebo, this improvement was not significant (p=0.14). There was a small but statistically significant improvement in night-time asthma (p=0.04). Note: Asthma is not an approved indication for omeprazole. Reproduced with permission. PPI (omeprazolo) Settimane Placebo Kiljander et al., Chest 1999; 16: 1257–64. 12
 12. Score dei sintomi A double-blind, placebo-controlled, crossover study conducted with omeprazole 40 mg/day in 107 asthma patients with GORD. Weekly pulmonary (cough, dyspnoea and wheezing) and gastric (regurgitation, heartburn and chest pain) symptoms scores fell during omeprazole therapy. There was a significant improvement in the gastric symptom score with omeprazole compared to placebo (p=0.0001). While pulmonary symptom scores also improved with omeprazole compared to placebo, this improvement was not significant (p=0.14). There was a small but statistically significant improvement in night-time asthma (p=0.04). Note: Asthma is not an approved indication for omeprazole. Reproduced with permission. PPI. (omeprazolo) Settimane. Placebo. Kiljander et al., Chest 1999; 16: 1257–")
13
Modalità di presentazione del GERD
Sintomi tipici Sintomi atipici Complicazioni Pirosi Dolore toracico Disfagia Erosioni esofagee e/o ulcere Rigurgito Raucedine (“laringite da reflusso”) Stenosi The classic symptom of GORD is heartburn, with or without regurgitation. Patients may or may not have evidence of oesophagitis. There are also atypical symptoms, including chest pain, hoarseness and asthma, so it is important to consider GORD when patients present with these symptoms. Patients with GORD may develop complications, some of which are very serious. Background information on some of these symptoms is given in the next few slides. Esofago di Barrett Asma, tosse cronica, dispnea Erosioni dei denti Adenocarcinoma esofageo 13
 Stenosi. The classic symptom of GORD is heartburn, with or without regurgitation. Patients may or may not have evidence of oesophagitis. There are also atypical symptoms, including chest pain, hoarseness and asthma, so it is important to consider GORD when patients present with these symptoms. Patients with GORD may develop complications, some of which are very serious. Background information on some of these symptoms is given in the next few slides. Esofago di. Barrett. Asma, tosse cronica, dispnea. Erosioni dei denti. Adenocarcinoma esofageo. 13.")
14
Complicazioni di un reflusso acido esofageo patologico
Emorragia Perforazione Stenosi esofagea Esofago di Barrett Adenocarcinoma esofageo Acute Croniche Most patients present to the GP with heartburn or other symptoms of GORD. Relatively few will present for the first time with the more serious complications of GORD. Serious complications of GORD are generally managed by a specialist. 14

15
Esofago di Barrett Sostituzione dell’epitelio squamoso esofageo con mucosa di tipo colonnare al di sopra del cardias anatomico (metaplasia intestinale con epitelio specializzato) Fenomeno di adattamento della mucosa esofagea allo stimolo cloridro-peptico cronico secondario a reflusso gastro- esofageo
 Fenomeno di adattamento della mucosa esofagea allo stimolo cloridro-peptico cronico secondario a reflusso gastro- esofageo.")
16
Esofago di Barrett: epidemiologia (Europa/USA)
Riscontro endoscopico di Barrett : 1–2% Riscontro di Barrett in caso di diagnosi di GERD: 10–15% Maggior frequenza nei maschi di razza bianca Incrementa il rischio di cancro esofageo da 50 a 100 volte Barrett’s oesophagus is a condition in which the normal squamous epithelium of the oesophagus is replaced by metaplastic columnar epithelium. This is a pre-malignant condition with a 50– to 100-fold (possibly even higher) increased risk of oesophageal cancer. About 10–15% of patients with GORD will have Barrett’s oesophagus. The condition is most common in white men. 20–40% of the adult population experiences heartburn, the primary symptom of GORD. Barrett’s oesophagitis, along with stricture, is one of the complications of GORD. Due to the increased risk of developing oesophageal adenocarcinoma, many gastroenterologists recommend regular (yearly or biennial) endoscopic screening with multiple biopsies to detect dysplasia in patients with Barrett’s oesophagus. 16
 increased risk of oesophageal cancer. About 10–15% of patients with GORD will have Barrett’s oesophagus. The condition is most common in white men. 20–40% of the adult population experiences heartburn, the primary symptom of GORD. Barrett’s oesophagitis, along with stricture, is one of the complications of GORD. Due to the increased risk of developing oesophageal adenocarcinoma, many gastroenterologists recommend regular (yearly or biennial) endoscopic screening with multiple biopsies to detect dysplasia in patients with Barrett’s oesophagus. 16.")
17
Malattia Esofagea da reflusso acido
Diagnosi 17

18
Diagnosi differenziale
Ernia hiatale Stenosi Cancro Dolore toracico cardiaco Dispepsia funzionale Patients presenting with symptoms of GORD may have a range of underlying conditions, so it is important to take a careful history, including the duration, location and severity of symptoms. If a simple trial of acid suppression is not successful in treating the symptoms, endoscopy will probably be required to establish a firm diagnosis. Nathoo, Int J Clin Pract 2001; 55: 465–9. 18

19
Diagnosi Clinica Sintomi tipici Sintomi atipici e/o di allarme
Strumentale Endoscopia Esame Rx con mezzo di contrasto esofago- gastrico Ph-metria delle 24 ore Manometria

20
Sintomi d’allarme Allarme Odinofagia Disfagia Sanguinamento Vomito
Alarm features for GORD include: Dysphagia – difficulty swallowing Odynophagia – pain on swallowing Bleeding, which may present as melaena or haematemesis or result in anaemia. Weight loss can also include anorexia. The presence of one or more of these symptoms might indicate: underlying cardiac disease that is presenting as heartburn blockage of the oesophagus, possibly due to stricture or adenocarcinoma of the oesophagus. Vomito Calo ponderale 20

21
Diagnosi Clinica Sintomi tipici Sintomi atipici e/o di allarme
Strumentale Endoscopia Esame Rx con mezzo di contrasto esofago- gastrico Ph-metria delle 24 ore Manometria

22
Impedenziometria Limiti Esame invasivo Necessità di ricovero
Durata esame Non valuta complicanze GER (es. esofagite) Riproducibilità ? Mancano i VALORI DI NORMALITA’ Potrebbe perdere RGE BREVI PERCIO’ AL MOMENTO PUO’ ESSERE UTILIZZATA PER VALUTARE L’INFLUENZA DI UNA VARIABILE (ESEMPIO PASTI, POSTURE, TERAPIA, ECC.) SUL REFLUSSO NELLO STESSO BAMBINO. ESISTONO VALORI NORMALI PER L’ADULTO
 Riproducibilità Mancano i VALORI DI NORMALITA’ Potrebbe perdere RGE BREVI. PERCIO’ AL MOMENTO PUO’ ESSERE UTILIZZATA PER VALUTARE. L’INFLUENZA DI UNA VARIABILE. (ESEMPIO PASTI, POSTURE, TERAPIA, ECC.) SUL REFLUSSO NELLO STESSO. BAMBINO. ESISTONO VALORI NORMALI. PER L’ADULTO.")
23
Il PPI Test nella diagnosi di MRGE
In assenza di un “gold standard” diagnostico per la diagnosi di malattia da reflusso gastro- esofageo (MRGE), oltre all’attenta raccolta dei sintomi, l'inibizione empirica della secrezione acida con un breve ciclo di terapia con inibitori di pompa protonica a dosi elevate (Proton Pump Inhibitor Test - PPI Test), che rientra nella diagnostica per l’identificazione dei sintomi, ben si presta ad essere inserita nella pratica ambulatoriale.
, oltre all’attenta raccolta dei sintomi, l inibizione empirica della secrezione acida con un breve ciclo di terapia con inibitori di pompa protonica a dosi elevate (Proton Pump Inhibitor Test - PPI Test), che rientra nella diagnostica per l’identificazione dei sintomi, ben si presta ad essere inserita nella pratica ambulatoriale.")
24
MALATTIA DA REFLUSSO GASTROESOFAGEO
Impatto sociale 24

25
Malattia da Reflusso Gastro-Esofageo:
Impatto sociale Condizione clinica cronica Può incidere sul lavoro e sulla qualità di vita Richiede indagini diagnostiche e terapie prolungate Implica l’impiego di rilevanti risorse economiche

26
Malattia da Reflusso Gastro-Esofageo:
Impatto sociale Ogni anno in Inghilterra il 4% della popolazione adulta consulta il medico di base per sintomi da reflusso Il 25% dei pazienti che esegue una EGDS ha segni di reflusso. Nel 2003 sono state eseguite EGDS per un totale di spesa pari a £ Un ulteriore 25% senza segni di esofagite esegue ph-metria e/o giunge a diagnosi di NERD attraverso i sintomi Mason, APT 2005

27
Malattia da reflusso gastroesofageo (GERD)
Terapia 27

28
Modifiche dello stile di vita Procinetici e farmaci motilizzanti
Terapia Modifiche dello stile di vita Antiacidi e alginato PPI Opzioni Anti-H2 For patients with typical GORD there are a number of long-term treatment approaches. In most patients the disease can be managed by lifestyle modifications and through the choice of appropriate antisecretory drug treatment (e.g. a PPI). Surgery is a last resort in GORD. Procinetici e farmaci motilizzanti Chirurgia 28
. Surgery is a last resort in GORD. Procinetici e farmaci motilizzanti. Chirurgia. 28.")
29
Norme comportamentali
Riduzione di peso Sollevamento della testata del letto Stop al fumo Stile di vita Basso consumo di sostanze pro-reflusso (es. alcool, caffè, cioccolata, menta…) Valutare modifiche farmacologiche (es. Teoflllina, anticolinergici) As in all fields of medicine, lifestyle modifications are effective in the short term, but in the long term they require the patient to be highly motivated. Changing diet, stopping smoking and losing weight are all difficult for patients to achieve long term. Often patients will require counselling support and the use of antisecretory agents to remove symptoms while the lifestyle changes take effect. Pasti piccoli, non mettersi a letto subito dopo I pasti, ridurre I cibi grassi 29
 Valutare modifiche farmacologiche (es. Teoflllina, anticolinergici) As in all fields of medicine, lifestyle modifications are effective in the short term, but in the long term they require the patient to be highly motivated. Changing diet, stopping smoking and losing weight are all difficult for patients to achieve long term. Often patients will require counselling support and the use of antisecretory agents to remove symptoms while the lifestyle changes take effect. Pasti piccoli, non mettersi a letto subito dopo I pasti, ridurre I cibi grassi. 29.")
30
Modifiche dello stile di vita Procinetici e farmaci motilizzanti
Terapia Modifiche dello stile di vita Antiacidi e alginato PPI Opzioni Anti-H2 For patients with typical GORD there are a number of long-term treatment approaches. In most patients the disease can be managed by lifestyle modifications and through the choice of appropriate antisecretory drug treatment (e.g. a PPI). Surgery is a last resort in GORD. Procinetici e farmaci motilizzanti Chirurgia 30
. Surgery is a last resort in GORD. Procinetici e farmaci motilizzanti. Chirurgia. 30.")
31
TERAPIA farmacologica della patologia acida gastro-esofagea
Fase acuta -step up -step down Fase di mantenimento Current American College of Gastroenterology guidelines recommend first-line empirical therapy with a PPI or other antisecretory agent for the majority of patients with a typical disease profile. 31

32
Antiacidi da contatto Innalzano il pH del contenuto gastrico
Rapido sollievo dei sintomi di lieve entità Poco efficaci per la terapia di esofagite da GERD Effetti collaterali: Accumulo nei pazienti con insufficienza renale Sindrome alcalinizzante (ad alte dosi) Stipsi Diarrea Antacids are effective for short-term relief of GORD symptoms, although their effectiveness has not been confirmed in controlled trials. Many patients, particularly those who have not consulted their GP, rely on self-medication with antacids to control their symptoms. 32
 Stipsi. Diarrea. Antacids are effective for short-term relief of GORD symptoms, although their effectiveness has not been confirmed in controlled trials. Many patients, particularly those who have not consulted their GP, rely on self-medication with antacids to control their symptoms. 32.")
33
Sono sostanze basiche che legano i protoni.
L’effetto neutralizzante può essere impiegato nella terapia dell’”iperacidità” gastrica da errori dietetici, abuso di alcool etc. e nelle forme lievi di esofagite da reflusso. Gli antiacidi usati più comunemente sono sali di alluminio e magnesio, da soli o, preferibilmente, in associazione poiché i sali di Al provocano stipsi e quelli di Mg provocano diarrea. E’ consigliabile evitare la somministrazione di altri antiacidi Alterando il pH gastrico e intestinale, si possono verificare interazioni con l’assorbimento di altri farmaci: intervallo di almeno 2 ore fra le somministrazioni dei farmaci.

34
Procinetici Incrementano il tono del LES e accellerano lo svuotamento gastrico Agiscono sul sintomo pirosi ma non guariscono l’esofagite sottostante La Cisapride e’ stata tolta dal commercio per effetti collaterali cardiologici Quelli presenti in commercio (Domperidone, Metoclopramide) sono generalmente poco efficaci o con effetti collaterali Motility-modifying agents relieve the symptoms of heartburn to a similar degree to H2RAs, but do not heal oesophagitis. Some agents have troublesome cardiac or CNS side effects. Cisapride has been withdrawn in some markets. Prokinetic motility agents can be useful in patients with GORD and other dyspeptic symptoms such as nausea or early satiety. 34
 sono generalmente poco efficaci o con effetti collaterali. Motility-modifying agents relieve the symptoms of heartburn to a similar degree to H2RAs, but do not heal oesophagitis. Some agents have troublesome cardiac or CNS side effects. Cisapride has been withdrawn in some markets. Prokinetic motility agents can be useful in patients with GORD and other dyspeptic symptoms such as nausea or early satiety. 34.")
35
Antagonisti dei recettori H2 (Anti-H2)
Inibiscono la stimolazione istaminica della cellula parietale gastrica, riducendo la secrezione acida Inizio d’azione ritardato ma di più lunga durata rispetto agli antacidi Piu’ potenti degli anticidi sia sui sintomi che sulle lesioni RANITIDINA, FAMOTIDINA, CIMETIDINA.. Before the development of the PPIs, the H2RAs were the mainstay of antisecretory therapy. Ranitidine is still extensively used by GPs in many countries, and remains on formularies and in local and national guidelines. However, there is good evidence that H2RAs provide poorer acid suppression than PPIs, and thus are less desirable for short- or long-term treatment. 35

36
Inibitori della pompa protonica (PPI)
Omeprazolo Lansoprazolo Pantoprazolo Rabeprazolo Esomeprazolo These are the main PPIs currently available in Europe 36

37
PPI e Malattia da reflusso gastroesofageo (diversa efficacia in NERD e EE!!)
Fass, JCG 2007

38
TERAPIA farmacologica della patologia acida gastro-esofagea
Fase acuta Fase di mantenimento Current American College of Gastroenterology guidelines recommend first-line empirical therapy with a PPI or other antisecretory agent for the majority of patients with a typical disease profile. 38

39
Terapia di mantenimento
Obiettivi: Controllo dei sintomi Assenza di lesioni esofagee Prevenzione delle complicanze Possibili scelte: Anti-H2/PPI a dosi standard o ad alte dosi On demand Cronicamente Chirurgia Tecniche endoscopiche (ancora sperimentale) The options for pharmacological treatment of GORD do not change in the longer term – PPIs and H2RAs remain the antisecretory agents of choice. Effective long-term therapy is essential to prevent the development of complications. Anti-reflux surgery eliminates the need for lifelong drug therapy, and may be preferred by some patients. Open anti-reflux surgery and long-term PPI therapy have been shown to be equally effective over 5-year follow up, although there is a small (0.2%) risk of mortality associated with surgery. Laparoscopic surgery is now popular, but maintenance of special surgical skills is required for consistent results. New endoscopic techniques, such as high frequency radiotherapy and the formulation of pliccae by sucking and stitching folds into the mucosa (Stretta method) aim to narrow the gastro-oesophageal junction and hence reduce the reflux of acid. Experience with these methods is still very limited and thus restricted to clinical research. 39
 The options for pharmacological treatment of GORD do not change in the longer term – PPIs and H2RAs remain the antisecretory agents of choice. Effective long-term therapy is essential to prevent the development of complications. Anti-reflux surgery eliminates the need for lifelong drug therapy, and may be preferred by some patients. Open anti-reflux surgery and long-term PPI therapy have been shown to be equally effective over 5-year follow up, although there is a small (0.2%) risk of mortality associated with surgery. Laparoscopic surgery is now popular, but maintenance of special surgical skills is required for consistent results. New endoscopic techniques, such as high frequency radiotherapy and the formulation of pliccae by sucking and stitching folds into the mucosa (Stretta method) aim to narrow the gastro-oesophageal junction and hence reduce the reflux of acid. Experience with these methods is still very limited and thus restricted to clinical research. 39.")
40
La terapia cronica con PPI deve essere prescritta con maggiore attenzione nei pazienti ad alto rischio - donne in postmenopausa con osteoporosi, pazienti anziani e persone ad alto rischio di caduta; - persone ad alto rischio di pneumopatie; - persone con carenza di ferro, vitamina B12 ed ipomagnesiemia; - è opportuno eseguire dei tests di routine per monitorare calcio, vitamina B12, magnesio e livelli di ferro negli utilizzatori a lungo termine PPI.

41
Reazioni avverse di potenziale importanza nell'anziano:
1. Ipomagnesemia 2. Riduzione assorbimento del calcio carbonato 3. Infezioni respiratorie 4. Diarrea da Cl.difficile 5. Poliposi gastrica 6. Gastrite atrofica in soggetti H. Pylori 41

42
L'uso a lungo termine di inibitori di pompa protonica appare associato ad un aumento del rischio di sviluppo di polipi gastrici, la cui istologia però rimane benigna e non preoccupante.

43
Note che definiscono la rimborsabilita’ dei PPI da parte del SSN
Malattia da reflusso gastroesofageo (GERD) Note che definiscono la rimborsabilita’ dei PPI da parte del SSN
 Note che definiscono la rimborsabilita’ dei PPI da parte del SSN.")
44
Spesa farmaceutica territoriale in Italia nel periodo 1985-2006

46
NOTA 1 Aifa, Bollettino d’informazione sui farmaci 1/08

47
NOTA 48 Aifa, Bollettino d’informazione sui farmaci 1/08

48
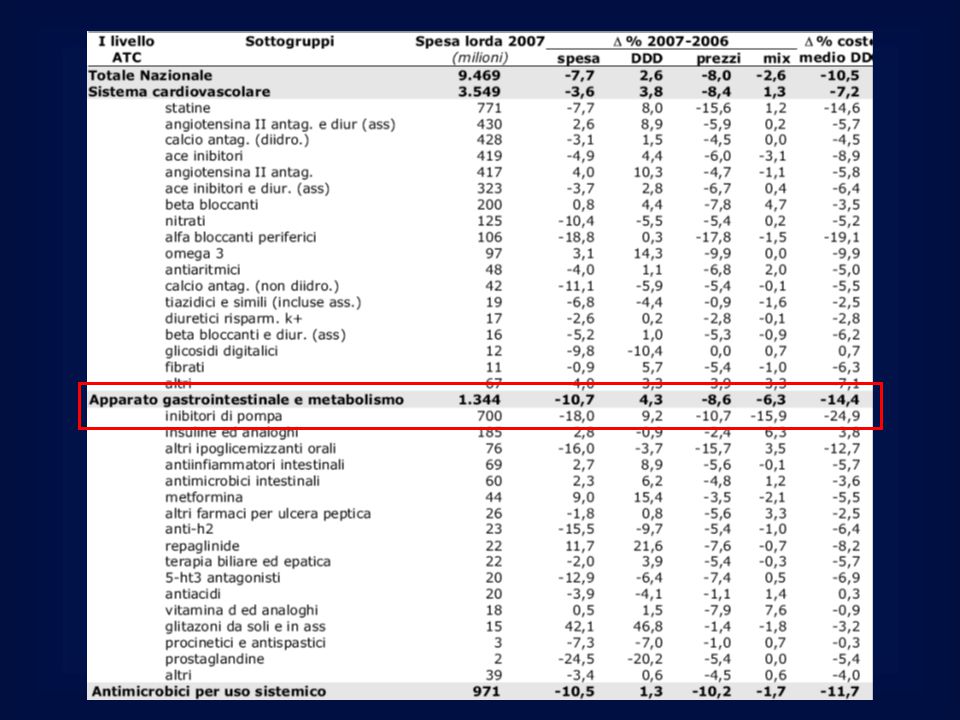
Come ridurre la spesa sanitaria in Italia?
Giunta Regionale, Regione Lazio 2007

49
Primi 30 principi attivi per spesa territoriale di classe A-SSN: confronto tra i primi 9 mesi del periodo Il lansoprazolo e’ passato dal 15°al 3°posto Sono arretrati esomeprazolo, omeprazolo e pantoprazolo

50
Costo efficacia dei trattamenti anti-reflusso
Costo/anno per pz trattato Induzione: Step up vs Step down Mantenimento: Intermittente vs continua Briggs, APT 2004 Ofman, APT 2002

51
Modifiche dello stile di vita Procinetici e farmaci motilizzanti
Terapia Modifiche dello stile di vita Antiacidi e alginato PPI Opzioni Anti-H2 For patients with typical GORD there are a number of long-term treatment approaches. In most patients the disease can be managed by lifestyle modifications and through the choice of appropriate antisecretory drug treatment (e.g. a PPI). Surgery is a last resort in GORD. Procinetici e farmaci motilizzanti Chirurgia 51
. Surgery is a last resort in GORD. Procinetici e farmaci motilizzanti. Chirurgia. 51.")
52
Malattia da Reflusso Gastro-Esofageo: Indicazioni alla chirurgia
Reflusso sintomatico ed evidenza manometrica di difetto meccanico del SEI in caso di fallimento della terapia medica Complicanze della MRGE esofagite persistente stenosi esofago di Barrett inalazione ricorrente Incapacità o rifiuto del paziente di assumere cronicamente farmaci

53
Terapia delle complicanze
The complications of GORD are: oesophageal stricture Barrett’s oesophagus ulceration or bleeding oesophageal adenocarcinoma. 53

54
Stenosi esofagea Profonda soppressione della secrezione acida
Dilatazione endoscopica: necessarie più sedute per alto tasso di recidive Oesophageal stricture is one of the complications of GORD. This complication can be treated by: dilatation of the oesophagus, which may need to be repeated as the recurrence of stricture following dilatation is high acid suppression with PPI therapy. Note: PPIs are not indicated for stricture in all countries. 54

55
Esofago di Barrett Soppressione acida
Sorveglianza endoscopico/istologica Ablazione (elettrocauterizzazione, laser o terapia fotodinamica)/EMR in combinazione con terapia di soppressione Resezione esofagea distale Barrett’s oesophagus is one of the complications of GORD. It can be managed in a number of ways, as listed here. Some of these management options are discussed in more detail in the following slides. Note: PPIs are not indicated for Barrett’s oesophagus in all countries. 55
/EMR in combinazione con terapia di soppressione. Resezione esofagea distale. Barrett’s oesophagus is one of the complications of GORD. It can be managed in a number of ways, as listed here. Some of these management options are discussed in more detail in the following slides. Note: PPIs are not indicated for Barrett’s oesophagus in all countries. 55.")
56
Malattia da reflusso gastroesofageo (GERD)
CONCLUSIONI NSAID-induced peptic ulcers are, ideally, managed by removal of the causative factor (the NSAID) and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.
 and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.")
57
CONCLUSIONI La malattia da reflusso gastroesofageo è tra le piu’ comuni patologie nel mondo occidentale E’ strettamente relata a stile di vita ed abitudini alimentari E’ cruciale individuare i fattori di rischio e effettuare una diagnosi differenziale con patologie maggiori La prima linea di trattamento e’ la correzione dello stile di vita Una terapia farmacologica con farmaci antiacidi puo’ essere utilizzata transitoriamente (on demand) che cronicamente NSAID-induced peptic ulcers are, ideally, managed by removal of the causative factor (the NSAID) and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.
 che cronicamente. NSAID-induced peptic ulcers are, ideally, managed by removal of the causative factor (the NSAID) and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.")
58
CONCLUSIONI Farmaci antiacidi da contatto, H2 antagonisti ed inibitori della pompa protonica sono le opzioni terapeutiche utilizzabili La scelta tra questi farmaci deve essere fatta in base all’entita’ dei sintomi e della efficacia La tollerabilita’ e l’efficacia sono spesso su base individuale La scelta della classe farmacologica e del dosaggio deve essere fatta con una strategia di STEP UP (crescita progressiva della potenza farmacologica) NSAID-induced peptic ulcers are, ideally, managed by removal of the causative factor (the NSAID) and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.
 NSAID-induced peptic ulcers are, ideally, managed by removal of the causative factor (the NSAID) and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.")
59
CONCLUSIONI E’ mandatorio evitare terapie long term con antiacidi se non strettamente necessario per evitare: 1. Costi 2. Overgrowth microbico intestinale e clinica ad esso correlato 2. Malassorbimento ….. NSAID-induced peptic ulcers are, ideally, managed by removal of the causative factor (the NSAID) and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.
 and suppression of acid secretion, to allow healing. NSAIDs can be replaced with less toxic agents such as COX-2 inhibitors. The use of mucosal protective agents (e.g. the prostaglandin E1 analogue, misoprostol) does prevent gastric injury by NSAIDs, but causes GI side effects at the doses needed to protect against NSAID-induced ulcers. Acid suppression with normal-dose PPIs or high-dose H2RAs is effective.")
Presentazioni simili