Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Asma e Allergopatie Respiratorie: “approccio olistico”
F. Braido Allergy & Respiratory Diseases Department University of Genoa

2
ASMA RINITE ALLERGICA RINOSINUSITE POLIPOSI OTITE DISTURBI DEL SONNO
CONGIUNTIVITE RINITE ALLERGICA RINOSINUSITE POLIPOSI OTITE DISTURBI DEL SONNO

3
Il legame bidirezionale asma rinite appare dunque piuttosto chiaro.

4
Associazione asma e rinite: dati epidemiologici
Studi trasversali: 70% (Ciprandi et al Int. Arch. Allergy Immunol.) 90% (Kapsali et al J. Allergy and Clin. Immunology) Dei pazienti asmatici allergici soffrono di rinite.
 90% (Kapsali et al J. Allergy and Clin. Immunology) Dei pazienti asmatici allergici soffrono di rinite.")
5
L’asma è significativamente più frequente nei soggetti rinitici
Prevalenza di asma nei pazienti rinitici: % Leynaert B, et al., JACI 2000; 106: S201-5

6
RINITE ALLERGICA ASMA ASMA
Oltre l’80% dei pazienti con Asma hanno Rinite Allergica RINITE ALLERGICA Paziente che si presenta con sintomi asmatici ASMA ASMA RINITE ALLERGICA ASMA e Paziente che si presenta con sintomi rinitici Capisci se quel paziente che oggi ha rinite ha anche asma e trattali entrambi Fino al 40% dei pazienti con Rinite Allergica hanno Asma

7
Results of an italian study ”
“ Is the prevalence of adult asthma and allergic rhinitis still increasing? Results of an italian study ” RINITE 21% P<0.01 15% 6876 pts ASMA 9.0% NS, P= .188 3.0% 91-93 98-00 91-93 98-00 Verlato G., et al. JACI 2003

8
Allergic inflammation is due to the release of mediators as a consequence of the interaction between allergen and allergen-specific IgE antibodies bound to mast cells and/or basophils Allergen IgE

9
La cascata allergica Istamina eFcRI Leucotriene Prostaglandine
Bradikinina, PAF Stiintomi allergici immediati eFcRI Mastociti Secrezioni nasali, starnutazione Broncocostrizione Edema/arros. cute IgE B Lymphocyte Allergene Leucotrieni Sintomi della fase ritardata IL-4 IL-13 VCAM-1 Congestione nasale Risposta broncospastica tardiva Orticaria APC CD80/86 CD28 Eosinfili Th2 IL-3, IL-5 GM-CSF Linfocita 9

10
Rapporti tra rinite ed asma: quali sono gli aspetti fisiopatologici?
1 - L ’infiammazione nasale è presente negli asmatici (con/senza sintomi nasali)? 2- Nella rinite è presente infiammazione bronchiale ? 3- L ’allergia è una malattia sistemica ? 10
 2- Nella rinite è presente infiammazione bronchiale 3- L ’allergia è una malattia sistemica 10.")
11
Biopsie nasali nell ’asmatico Gaga et al, Clin Exp Allergy 2000
60 A+ R+ 50 A + R - 40 controls Cellule positive per campo 30 20 10 EG2 CD4 CD8 11

12
Rapporti tra rinite ed asma: quali sono gli aspetti fisiopatologici?
1- L ’infiammazione nasale è presente negli asmatici (con/senza sintomi nasali)? 2- Nella rinite è presente infiammazione bronchiale? 3- L ’allergia è una malattia sistemica ? 12
 2- Nella rinite è presente infiammazione bronchiale 3- L ’allergia è una malattia sistemica 12.")
13
Biopsie bronchiali nei pazienti con rinite stagionale
Chakir et al, Allergy Clin Immunol 2000 60 CD4+ 50 CD8+ CD45RO+ 2 40 EG1+ Cell./mm 30 20 10 out in Stagione pollinica 13

14
Rapporti tra rinite ed asma: quali sono gli aspetti fisiopatologici?
1- L ’infiammazione nasale è presente negli asmatici (con/senza sintomi nasali)? 2- Nella rinite è presente infiammazione bronchiale ? 3- L’ allergia è una malattia sistemica? 14
 2- Nella rinite è presente infiammazione bronchiale 3- L’ allergia è una malattia sistemica 14.")
15
Infiammazione bronchiale a seguito di challenge nasale
Braunstahl et al, J Allergy Clin Immunol 2001 Eosinofili / mm2 % vasi ICAM+ 20 40 60 80 100 120 BMK+ cell. nella lamina propria T0 T +24 hr Tempo dal challenge 140 20 40 60 80 100 120 ICAM T0 T +24 hr controls AR patients + vasi Tempo dal challenge 15

16
La rinite è un fattore di rischio per l’asma
The Copenhagen Allergy Study Linneberg et al, Allergy 2002 734 pazienti 15-69 anni dal 1990 al 1998 30 no 25 20 Incidenza dell’asma (%) 15 10 5 polline ep. dom. acaro rinite al basale 16 16
 polline. ep. dom. acaro. rinite al basale")
17
La rinite è un fattore di rischio per l’asma
The Copenhagen Allergy Study Linneberg et al, Allergy 2002 30 OR=46.5 no 25 sì 20 OR=18.9 OR=8.1 incidence of asthma (%) 15 10 5 polline animale acaro rinite al basale 17 17
 polline. animale. acaro. rinite al basale")
18
Prevalenza dell’asma nei Leynaert et al, J Allergy Clin Immunol 2004
pazienti rinitici Leynaert et al, J Allergy Clin Immunol 2004 % con asma 18 16 14 12 10 8 6 4 2 No rinite 18 18

19
Prevalenza dell’asma nei Leynaert et al, J Allergy Clin Immunol 2004
pazienti rinitici Leynaert et al, J Allergy Clin Immunol 2004 % con asma 18 16 14 12 10 p<0.001 8 6 4 2 no rinite SAR 19 19

20
Prevalenza dell’asma nei Leynaert et al, J Allergy Clin Immunol 2004
pazienti rinitici Leynaert et al, J Allergy Clin Immunol 2004 % con asma 18 16 14 p=0.004 12 10 p<0.001 8 6 4 2 No rinite SAR PAR 20 20

21
Prevalenza dell’asma nei Leynaert et al, J Allergy Clin Immunol 2004
pazienti rinitici Leynaert et al, J Allergy Clin Immunol 2004 p=0.002 % con asma 18 16 14 p=0.004 12 10 p<0.001 8 6 4 2 No rhinite SAR + PAR SAR PAR 21 21

22
C.Lombardi, G.Passalacqua et al, Resp Med 2001

23
Evoluzione della malattia
C. Lombardi, G. Passalacqua et al, Resp Med 2001

24
Rinite - Sinusite Asma bronchiale Stimolazione allergenica nasale
Eosinofili IL-5 Basofili Degranulazione mastocitaria Stimolazione allergenica nasale Perdita della funzione filtrante Allergene Gocciolamento retronasale Riflesso naso-bronchi Precursori Citochine Midollo osseo Infezione virale Eosinofili ICAM-1 VCAM-1 Stimolazione allergenica bronchiale Asma bronchiale

25
La rinite allergica è fattore di rischio per lo sviluppo di asma
Shaaban, Lancet 2008

26
The Th1/Th2 paradigm 16th edition, 2004, p.1924
Harrison’s. Principles of Internal Medicine (adapted from Romagnani, 1999)
")
27
Mechanism of Airway Inflammation in Allergy and its markers

28
Human effector CD4+ T cells before 2000

29
Human effector CD4+ T cells in 2010 Human effector CD4+ T cells TODAY
29

30
Helper T cell differentiation.
IgE-mediated Respiratory Allergy Non IgE-mediated Allergy (Evolution to chronicity) Th17 cells can switch in vivo to pathogenetic Th17/Th1, Th17/Th2 or Th1 cells by using tissue IL-12 in the absence of any parallel upgrowth of Treg cells FLEXIBILITY AND PLASTICITY J J O’Shea, W E Paul Science 2010;327:
 Th17 cells can switch in vivo to pathogenetic Th17/Th1, Th17/Th2 or Th1 cells by using tissue IL-12 in the absence of any parallel upgrowth of Treg cells. FLEXIBILITY. AND. PLASTICITY. J J O’Shea, W E Paul Science 2010;327:")
31
Clinical Asthma Phenotypes and associated pathophysiological mechanisms
Requirement For Th2 cells Requirement For Th17 cells Mechanisms or Effector cells Allergic Yes Yes Th2 /Th17 associated molecules, IL-25, Il-33, TSLP Eo, MC, Ba, NKT cells Viral Infection No Variable IL-13, IL-17, IFN-a Alveolar Macrophages NKT cells Air Pollution, Smoke Diesel Particles, Ozone No Yes IL-17, Oxidative stress Neutrophils, NKT cells Aspirin No No Loss of PGE2, Leukotrienes Obesity No No Oxidative stress? Severe, CCS resistant No Yes IL-17, Neutrophils , NKT cells Exercise, Cold air No No/Yes Changes in mucosal osmolarity Cytokines? Intrinsic No No Smooth Muscle Irritability? From Kim HY et al, Nat Immunol, 2010 (modified) 31
 31.")
32
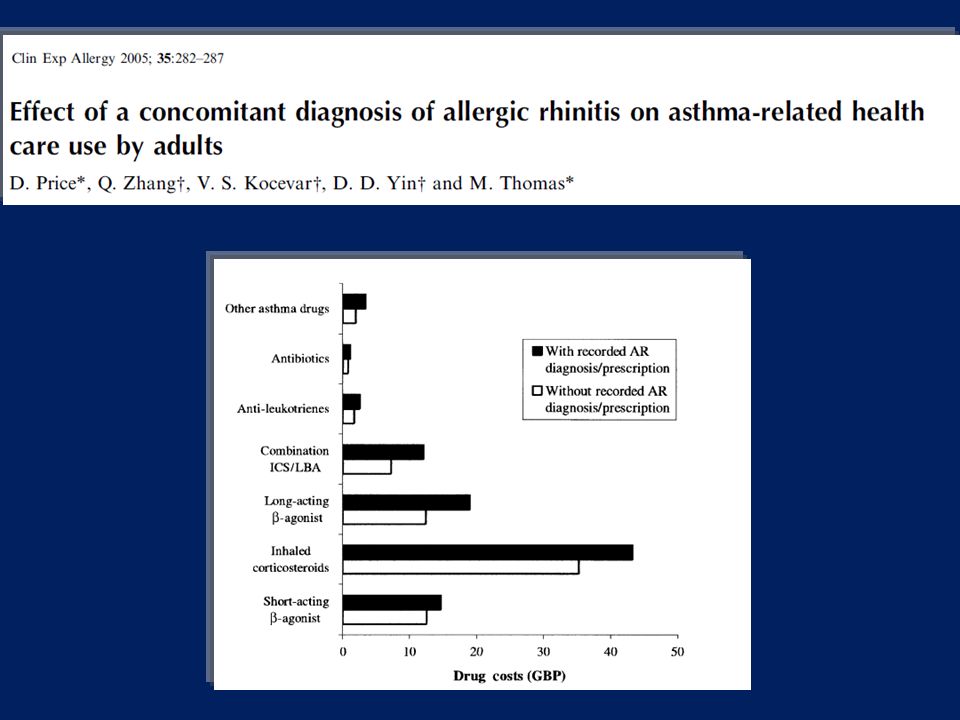
Further infromation about our study are now available on Clinical Experimental Allergy.

33
Clin Exp Allergy. 2007 May;37(5):788-93.
Allergic Rhinitis and Asthma ad hoc survey: Clinical and Psychological perspectives F. Braido, I. Baiardini, S. Brandi, A. Porcu, G.W. Canonica Allergy and Respiratory Diseases, DIMI, Genoa University, Genoa, Italy Clin Exp Allergy May;37(5): 504 asthmatic patients 27.8% of asthmatic patients experience three or less rhinitic symptoms, 41% from 4 to 6 symptoms, 31.2 % more than 6 symptoms. These symptoms deeply interfere with daily life causing sleep problems (87.3%), lack of concentration (78.9%), difficulties in spare time (71.8%) and sport (71.7%). 33
: asthmatic patients. 27.8% of asthmatic patients experience three or less rhinitic symptoms, 41% from 4 to 6 symptoms, 31.2 % more than 6 symptoms. These symptoms deeply interfere with daily life causing. sleep problems (87.3%), lack of concentration (78.9%), difficulties in spare time (71.8%) and sport (71.7%). 33.")
34
Indagine ad hoc su rinite allergica ed asma
(504 pazienti asmatici ) In presenza di sintomi rinitici, peggiora la vostra asma? F. Braido, G.W. Canonica et al. Allergic Rhinitis and Asthma ad hoc survey: Clinical and Psychological perspectivesClin Exp Allergy May;37(5):788-93 Tabella 2. Risposte di pazienti asmatici La vostra asma peggiora alla presenza di sintomi rinitici? Si (%) Frequenti risvegli notturni Peggioramento del respiro affannoso 59.0 Peggioramento della tosse Frequente dispnea Uso frequente di SABA Siete interessati ad un trattamento combinato per asma e rinite allergica? Si No 7.6 Braido et al. Clin Exp Allergy 2007
 In presenza di sintomi rinitici, peggiora la vostra asma F. Braido, G.W. Canonica et al. Allergic Rhinitis and Asthma ad hoc survey: Clinical and Psychological perspectivesClin Exp Allergy May;37(5): Tabella 2. Risposte di pazienti asmatici. La vostra asma peggiora alla presenza di sintomi rinitici Si (%) Frequenti risvegli notturni Peggioramento del respiro affannoso Peggioramento della tosse Frequente dispnea Uso frequente di SABA Siete interessati ad un trattamento combinato per asma e rinite allergica Si No 7.6. Braido et al. Clin Exp Allergy")
36
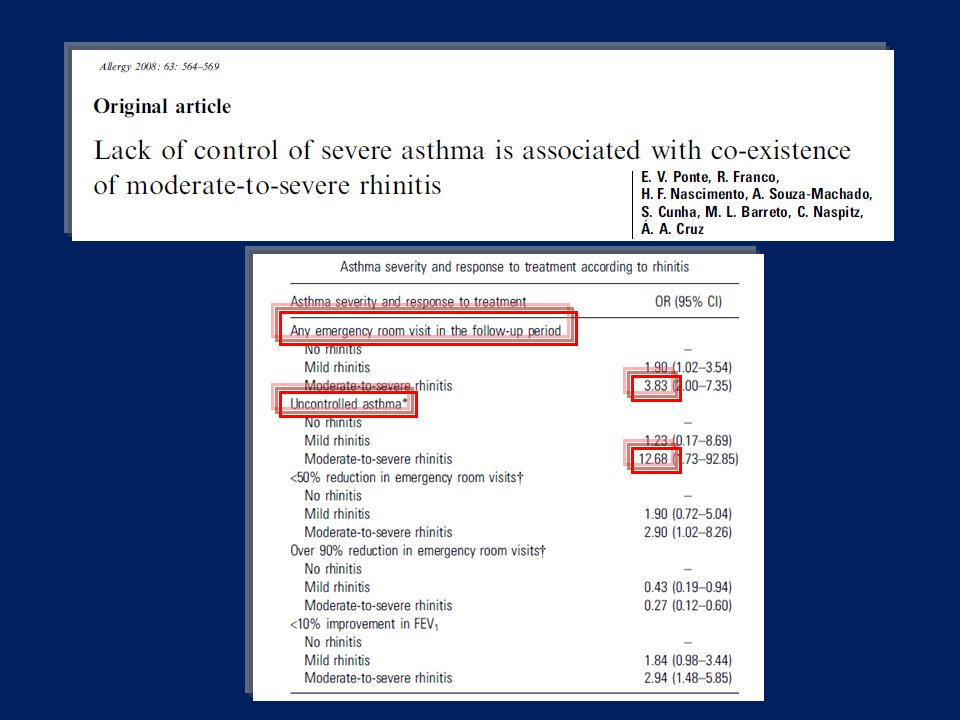
Results: Eighty-two (15%) patients had no rhinitis, 299 (54%) had mild rhinitis
and 176 (31%) moderate/severe rhinitis. In logistic regression models, moderate/ severe rhinitis was a predictor for any emergency room visit in the follow-up period [3.83 (2.00–7.35)], for the presence of uncontrolled asthma after 1 year of follow-up [12.68 (1.73–92.85)], for <10% improvement of the airway obstruction [2.94 (1.48–5.85)] and <50% reduction in the number of emergency room visits [2.90 (1.02–8.26)] in the year of follow-up. It was also associated with a smaller chance of more than 90% reduction in the number of emergency room visits in the year of follow-up [0.27 (0.12–0.60)]. In a multivariate linear regression model, severity of rhinitis was positively correlated with a score of asthma severity and inversely correlated to an index of quality of life. Conclusions: In a population with severe asthma, moderate/severe rhinitis is a strong predictor for greater severity of asthma.
 moderate/severe rhinitis. In logistic regression models, moderate/ severe rhinitis was a predictor for any emergency room visit in the follow-up. period [3.83 (2.00–7.35)], for the presence of uncontrolled asthma after 1 year of. follow-up [12.68 (1.73–92.85)], for <10% improvement of the airway obstruction. [2.94 (1.48–5.85)] and <50% reduction in the number of emergency room. visits [2.90 (1.02–8.26)] in the year of follow-up. It was also associated with a. smaller chance of more than 90% reduction in the number of emergency room. visits in the year of follow-up [0.27 (0.12–0.60)]. In a multivariate linear. regression model, severity of rhinitis was positively correlated with a score of. asthma severity and inversely correlated to an index of quality of life. Conclusions: In a population with severe asthma, moderate/severe rhinitis is a. strong predictor for greater severity of asthma.")
38
La rinite non trattata aumenta il rischio di attacchi asmatici e
Asma + rinite La rinite non trattata aumenta il rischio di attacchi asmatici e ricoveri per asma. Bousquet, Clin Exp Allergy 2005

39
Patienti con asma + rinite allergica
La rinite allergica raddoppia il rischio di visite al pronto soccorso in pazienti con asma bronchiale Analisi Post hoc degli accessi al pronto soccorso in pazienti asmatici con e senza rinite allergica concomitante in un arco di tempo di 52 settimane. % pazienti Patienti con asma + rinite allergica (n = 893) Patienti con asma (n = 597) 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 p = 0.029 1.7 3.6 Adattato da Bousquet J et coll. Poster presentato all’European Academy of Allergology and Clinical Immunology (EAACI), Giugno 12–16, 2004, Amsterdam. Poster 141.
 Patienti. con asma. (n = 597) p = Adattato da Bousquet J et coll. Poster presentato all’European Academy of. Allergology and Clinical Immunology (EAACI), Giugno 12–16, 2004, Amsterdam. Poster 141.")
40
40

41
Differenze nei domini riguardanti la qualità della vita tra pazienti controllati e non controllati
I pazienti con un’asma controllata (ACT >20) hanno una migliore qualità della vita rispetto ai soggetti non controllati 41
 hanno una migliore qualità della vita rispetto ai soggetti non controllati. 41.")
42
ACT vs GS 5 10 15 20 25 30 40 60 80 100 120 1- GS ACT

43
La presenza di sintomi rinitici influenza la qualità della vita del paziente asmatico?

44
Differenze nei domini del Rhinasthma sulla base del livello di sintomi rinitici come misurati dal T5SS p=0.001 p<0.0001 p<0.0001 p=0.07 Avere o non avere i sintomi cambia la qol e non solo per Per quanto riguarda le vie aeree superiori, la qualità della vita è quasi ottimale (6) nei pazienti privi di sintomi, mentre nei pazienti sintomatici trattati e non la qualità della vita è intorno a 35, indicando una considerevole riduzione del proprio benessere 44
 nei pazienti privi di sintomi, mentre nei pazienti sintomatici trattati e non la qualità della vita è intorno a 35, indicando una considerevole riduzione del proprio benessere. 44.")
45
La rinite influenza la qualità della vita nei pazienti controllati?
Anche se il controllo dell'asma viene raggiunto, la presenza di sintomi rinitici peggiora la qualità della vita del paziente

46
Quale è l'importanza relativa di controllo e di rinite, sintomi nell’influenzare i differenti domini della qualità della vita? Regressione Logistica

47
GOAL: Quality of life in controlled asthma patients (analisi post hoc dello studio GOAL)
La qualità della vita migliora raggiungendo livelli ottimali. Pazienti con un punteggio > 6: 61% con SSFC vs. 52% con FP). Bateman ED et al., ERJ 2007 47
. Bateman ED et al., ERJ")
48
Una qualità della vita ottimale è stata raggiunta da 78/209 (37
Una qualità della vita ottimale è stata raggiunta da 78/209 (37.32%) pazienti Il controllo dell’asma è significativamente associato con una qualità della vita ottimale (2=49.599; p<0.001). I pazienti ben controllati e totalmte controllati differiscono significativamente nel raggiungimento della qualità della vita ottimale (2= 7.617; p < 0.006) . Braido et Al PLOsone 2012 48
 pazienti. Il controllo dell’asma è significativamente associato con una qualità della vita ottimale (2=49.599; p<0.001). I pazienti ben controllati e totalmte controllati differiscono significativamente nel raggiungimento della qualità della vita ottimale (2= 7.617; p < 0.006) . Braido et Al PLOsone")
49
RAPP Rhinitis & Asthma Patient’s Perspective
RAPP scoring is simple: sum of responses to each item RAPP This is the final validated version of the rapp. For the patiens it is easy to complete the questionnaire, to calculate the total score, and to understend its meaning by using the picture reported on the right of the slide Braido et Al Submitted

50
Scoring Braido et Al Submitted
ROC analyses, using RHINASTHMA GS score < 20 or >20 as criterion measure, to determine the RAPP score that indicates optimal HRQoL. A cut-off point of 15 demonstrated the best sensitivity (88.3%) and specificity (84.6%) in discriminating the achievement of an optimal HRQoL, with a percentage of correctly classified patients of 87.3% Braido et Al Submitted
 and specificity (84.6%) in discriminating the achievement of an optimal HRQoL, with a percentage of correctly classified patients of 87.3% Braido et Al Submitted.")
51
Optimal QoL This is the final validated version of the rapp.
For the patiens it is easy to complete the questionnaire, to calculate the total score, and to understend its meaning by using the picture reported on the right of the slide Optimal QoL

52
Percentuale media di pazienti “Controllati” al termine della fase incrementale studio GOAL
Modified by Bateman et al, ARJCCM 2004 100 80 80 % di pazienti controllatti 63.6% (71-51) 60 60 31% (42-19) 40 40 Fig.1 20 20 Buon Controllo Controllo Totale
 % (42-19) Fig Buon Controllo. Controllo Totale.")
53
Percentuale media di pazienti “Controllati” al termine dello studio GOAL
Modified by Bateman et al, ARJCCM 2004 100 71.6% (78-62) 80 80 % di pazienti controllatti 60 60 41% (50-29) 40 40 Fig.1 20 20 Buon Controllo Controllo Totale
 % di pazienti controllatti % (50-29) Fig Buon Controllo. Controllo Totale.")
56
Miglioramento dell’iperreattività bronchiale
Lundback B.& Dahl R. Allergy 2007; 62: (data from ref Lundback B. et al. Resp Med 2006; 100: 2-10) 56
 56.")
57
La terapia continuativa ha infine
Lundback B. et al. Respiratory Medicine 2009; 103: RISULTATI A 3 ANNI Andamento temporale delle modificazioni della media geometrica della PC20 (mg/ml) La terapia continuativa ha infine comportato un continuo e progressivo miglioramento dell’iperreattività bronchiale Nel complesso una strategia basata su una terapia continuativa finalizzata al controllo della patologia, il cui aggiustamento della dose era guidato dal medico, ha consentito nei tre anni dello studio non solo di controllare i sintomi ma anche di migliorare costantemente il grado di iperreattività bronchiale (Grafico). A 36 mesi, 58 pazienti su 229 (25%) avevano una reattività normale dell’albero bronchiale (PC20 >8 mg/ml). Questi dati testimoniano che la terapia era stata aggiustata adeguatamente dal medico per ottenere il controllo dell’asma, poiché con tutti i regimi terapeutici sono stati raggiunti livelli simili di controllo della malattia.
 La terapia continuativa ha infine. comportato un continuo e progressivo miglioramento. dell’iperreattività. bronchiale. Nel complesso una strategia basata su una terapia continuativa finalizzata al controllo della patologia, il cui aggiustamento della dose era guidato dal medico, ha consentito nei tre anni dello studio non solo di controllare i sintomi ma anche di migliorare costantemente il grado di iperreattività bronchiale (Grafico). A 36 mesi, 58 pazienti su 229 (25%) avevano una reattività normale dell’albero bronchiale (PC20 >8 mg/ml). Questi dati testimoniano che la terapia era stata aggiustata adeguatamente dal medico per ottenere il controllo dell’asma, poiché con tutti i regimi terapeutici sono stati raggiunti livelli simili di controllo della malattia.")
58
Severe Refractory Asthma
Patients who remain difficult to control despite an extensive reevaluation of diagnosis, management, and an observational period of at least 6 months by an asthma specialist Chanez P et al. JACI 2007

59
Evaluation of patients with Refractory Asthma
Proceedings on Refractory Asthma AJRCCM 2000

60
Naso Bronchi NCS ICS Antiistaminici Immunoterapia specifica
Profilassi ambientale

61
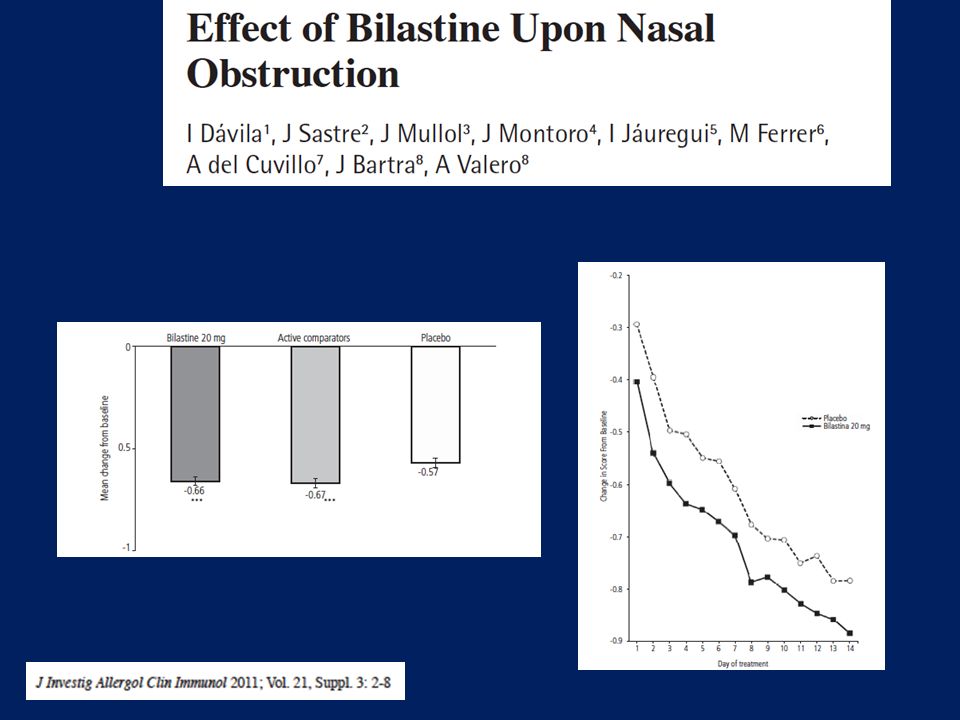
Antihistamines properties
EAACI ARIA Criteria

63
Evaluation of patients with Refractory Asthma
Proceedings on Refractory Asthma AJRCCM 2000

64
We published a couple of years ago a real life survey addressed to investigate the relationship between sleep disturbances and asthma control. We used a five points Likert scale sleep questionnaire and the asthma control test

65
122 patients The level of asthma control results to be inversely correlated to the presence of sleep disturbances Patients with good control report less frequent and less severe sleep disturbances compared to uncontrolled subjects. A significant percentage of subjects (11-20%) having achieved total control of asthma still report sleep disturbances, that contribute to increase the impact of the disease and to impair quality of life Obviously the level of asthma control results to be inversely correlated to the presence of sleep disturbances and well controlled patients reported less frequent and less severe sleep disturbances compared to uncontrolled subjects. More interesting is the evidence that a significant percentage of subjects (11-20%) having achieved total control of asthma still report sleep disturbances, that contribute to increase the impact of the disease and to impair quality of life. Two possible explanation of this evidence: ACT is not able to correctly identify asthma control or in controlled asthma patient sleep can be disturbed by other concomitant causes.
 having achieved total control of asthma still. report sleep disturbances, that contribute to. increase the impact of the disease and to. impair quality of life. Obviously the level of asthma control results to be inversely correlated to the presence of sleep disturbances and well controlled patients reported less frequent and less severe sleep disturbances compared to uncontrolled subjects. More interesting is the evidence that a significant percentage of subjects (11-20%) having achieved total control of asthma still report sleep disturbances, that contribute to increase the impact of the disease and to impair quality of life. Two possible explanation of this evidence: ACT is not able to correctly identify asthma control or in controlled asthma patient sleep can be disturbed by other concomitant causes.")
66
Michel Alkhalil described the potential links between asthma and OSAS
Michel Alkhalil described the potential links between asthma and OSAS. The increased upper airways collapsibility above described the nasal obstruction frequently accompaining asthma represents facilitating factors of OSA development in asthma patients

69
Odds Ratio for Chronic Nighttime Rhinitis Symptoms
Patients with Chronic Night-time Rhinitis Symptoms are More Likely to Snore Patients with chronic nighttime rhinitis symptoms were 2 times more likely to be a habitual snorer Sleep Problem Odds Ratio for Chronic Nighttime Rhinitis Symptoms P Value Snoring Never or rarely Occasional (1-3 nights/week) Habitual (>3 nights/week) 0.02 <0.0001 Chronic excessive daytime sleepiness 2.4 0.001 Chronic non-restorative sleep 2.2 <0.0001 Young et al. J Allergy Clin Immunol. 1997;99:S757.
 Habitual (>3 nights/week) < Chronic excessive daytime sleepiness Chronic non-restorative sleep < Young et al. J Allergy Clin Immunol. 1997;99:S757.")
70
Patients with Congestion Due to Allergy are More Likely to Snore
Patients with congestion due to allergy were 50% more likely to be a habitual snorer than patients without congestion AHI Odds Ratio for Congestion Due to Allergy P Value <5, non-snorer, no SDB <5, habitual snorer 5-15 >15 1.0 1.5 1.8 0.04 NS AHI=apnea/hypopnea index, determined as the total number of apnea and hypopnea episodes (assessed by polysomnography) divided by hours of sleep. Young et al. J Allergy Clin Immunol. 1997;99:S757.
 divided by hours of sleep. Young et al. J Allergy Clin Immunol. 1997;99:S757.")
71
Nasal Congestion in Patients with SAR is Associated with Obstructive Sleep Apneas*
Apneas were longer and more frequent in patients with obstruction than in those without obstruction 10 20 30 40 50 60 70 0.2 0.4 0.6 0.8 1.0 Increase in obstructive sleep apneas/hour Increase in nasal resistance (%) *5 men with SAR. McNicholas et al. Am Rev Respir Dis. 1982;126:625.
 *5 men with SAR. McNicholas et al. Am Rev Respir Dis. 1982;126:625.")
72
Progetto Emergenza Controllo
MMG : ritiene che il suo paziente soffre di rinite? 68,6% 1553 MMG 3488 pazienti asmatici Paziente : lamenta sintomi rinitici ? Si in 3153 pazienti (90,3%)
")
73
Rinite = 58.5% Asma = 39.65 STOP BANG > 3 = 53,9%
Campione totale di 3488 pazienti Nell’ultimo mese si è svegliato di notte perché non respirava bene a causa di Rinite = 58.5% Asma = 39.65 STOP BANG > 3 = 53,9%

74
RINITE ASMA OSAS

75
Asma e Allergopatie Respiratorie: “approccio olistico”
F. Braido Allergy & Respiratory Diseases Department University of Genoa

Presentazioni simili





 is a disease state characterized by airflow limitation that is not fully reversible. The.>")















