Scaricare la presentazione
1
Luca Cindolo

2
Nuove evidenze in tema di IPB

4
ostruzione ipertrofia Prostatismo Sintomi irritativi Sintomi ostruttivi Lower Urinary Tract Symptoms Disturbo urinario del paziente senza implicazione di causa o sito di origine Abrams P et al 1994

5
BPH – LUTS – BPE – BPO il mondo ideale
All men > 40yrs BPH BPE BOO LUTS 5

6
BPH – LUTS – BPE – BPO la realtà
All men > 40yrs BPH BPE BPO LUTS 6

7
Lower Urinary Tract Symptoms
Riempimento Vuotamento Potminzionali Urgenza Esitazione Gocciolamento Frequenza Flusso scarso Tenesmo Nicturia Intermittenza Incontinenza da urgenza Sforzo Altra incontinenza Gocciolamento terminale According to the International Continence Society (ICS), lower urinary tract symptoms (LUTS) can be classified into 3 major categories: Storage symptoms include increased daytime frequency, nocturia, urgency, and various types of urinary incontinence (UI). Frequency is a subjective complaint where the patient believes that he/she voids too often during the day. Nocturia is a complaint that the individual has to arise 1 or more times at night to void. UI is any involuntary leakage of urine.1 Voiding symptoms include slow stream, splitting or spraying, intermittent stream of urine, hesitancy (difficulty in starting), and straining to initiate, maintain, or improve the urine stream.1 Post-micturition symptoms in men are experienced immediately after micturition, usually after leaving the toilet, and include a feeling of incomplete emptying and terminal dribble—a prolonged final part of micturition.1 It is important for the clinician to carefully evaluate male patients presenting with LUTS to determine the root of the problem because symptoms reported by men, especially those related to storage, can be attributed to overactive bladder (OAB), bladder outlet obstruction (BOO), or both.2 References 1. Abrams P, Cardozo L, Fall M, et al. The standardisation terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21: 2. Abdel-Aziz KF, Lemack GE. Overactive bladder in the male patient: bladder, outlet, or both? Curr Urol Rep. 2002;3: Abrams P et al. Neurol Urodyn. 2002;21:
, lower urinary tract symptoms (LUTS) can be classified into 3 major categories: Storage symptoms include increased daytime frequency, nocturia, urgency, and various types of urinary incontinence (UI). Frequency is a subjective complaint where the patient believes that he/she voids too often during the day. Nocturia is a complaint that the individual has to arise 1 or more times at night to void. UI is any involuntary leakage of urine.1. Voiding symptoms include slow stream, splitting or spraying, intermittent stream of urine, hesitancy (difficulty in starting), and straining to initiate, maintain, or improve the urine stream.1. Post-micturition symptoms in men are experienced immediately after micturition, usually after leaving the toilet, and include a feeling of incomplete emptying and terminal dribble—a prolonged final part of micturition.1. It is important for the clinician to carefully evaluate male patients presenting with LUTS to determine the root of the problem because symptoms reported by men, especially those related to storage, can be attributed to overactive bladder (OAB), bladder outlet obstruction (BOO), or both.2. References. 1. Abrams P, Cardozo L, Fall M, et al. The standardisation terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21: Abdel-Aziz KF, Lemack GE. Overactive bladder in the male patient: bladder, outlet, or both Curr Urol Rep. 2002;3: Abrams P et al. Neurol Urodyn. 2002;21:")
8
La gran parte dei maschi presenta LUTS misti
Reimpimento + vuotamento/ postminzionali Vuotamento/ postminzionali 67% Riempimento Calculation of Men with Storage and Voiding/Post-micturition Symptoms Of those who reported storage symptoms, 8.8%, 8.5%, and 3.7% (total of 21%) also reported voiding symptoms, voiding and post-micturition symptoms, and post-micturition symptoms, respectively. Voiding symptoms only were reported by 6.2%, 2.2% reported voiding and post-micturition symptoms both, and 2.1% reported post-micturition symptoms only (total of 10.5%). Therefore, the percentage of men with voiding and post-micturition symptoms who report at least 1 storage symptom is calculated by 21%/(21% %) = 67%. Reference Irwin DE, Milsom I, Hunskaar S, et al. population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50: Irwin DE et al. Eur Urol. 2006;50: Abrams P et al. Urology. 2003;61:37-49.
 also reported voiding symptoms, voiding and post-micturition symptoms, and post-micturition symptoms, respectively. Voiding symptoms only were reported by 6.2%, 2.2% reported voiding and post-micturition symptoms both, and 2.1% reported post-micturition symptoms only (total of 10.5%). Therefore, the percentage of men with voiding and post-micturition symptoms who report at least 1 storage symptom is calculated by 21%/(21% %) = 67%. Reference. Irwin DE, Milsom I, Hunskaar S, et al. population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50: Irwin DE et al. Eur Urol. 2006;50: Abrams P et al. Urology. 2003;61:")
10
EQ-5D: Percentage of Respondents Reporting Any Problems—Men
Gli uomini con vescica iperattiva riferiscono maggiore fastidio e danno alla QoL EQ-5D: Percentage of Respondents Reporting Any Problems—Men Control male OAB without UI OAB with UI 45 * 40 35 * 30 25 Patients, % * * 20 * 15 * Men with symptoms of OAB report a lower health-related QOL (HRQL) than those without symptoms of OAB. The proportion of men reporting any impairment within each of the EQ-5D domains was higher in men with OAB than in controls. Significantly lower EQ-5D scores were reported for all domains (mobility, self care, usual activities, pain/discomfort, anxiety/depression) for men with OAB and urgency urinary incontinence (UUI). Reference Irwin DE. Presented at: the 36th Annual Meeting of the International Incontinence Society; November 27-December 1, 2006; Christchurch, New Zealand. 10 5 Mobility Self-care Usual activities Pain/ discomfort Anxiety depression The EQ-5D is a 5-item generic QOL instrument used to measure overall QOL. *P ≤ .05 OAB with UI vs controls and OAB without UI vs controls. HRQL = health-related quality of life; QOL = quality of life; UI = urinary incontinence. Irwin DE. ICS 2006.
 than those without symptoms of OAB. The proportion of men reporting any impairment within each of the EQ-5D domains was higher in men with OAB than in controls. Significantly lower EQ-5D scores were reported for all domains (mobility, self care, usual activities, pain/discomfort, anxiety/depression) for men with OAB and urgency urinary incontinence (UUI). Reference. Irwin DE. Presented at: the 36th Annual Meeting of the International Incontinence Society; November 27-December 1, 2006; Christchurch, New Zealand Mobility. Self-care. Usual activities. Pain/ discomfort. Anxiety depression. The EQ-5D is a 5-item generic QOL instrument used to measure overall QOL. *P ≤ .05 OAB with UI vs controls and OAB without UI vs controls. HRQL = health-related quality of life; QOL = quality of life; UI = urinary incontinence. Irwin DE. ICS")
11
Nuova etiologia e nesso causale tra sintomi e LUTS

13
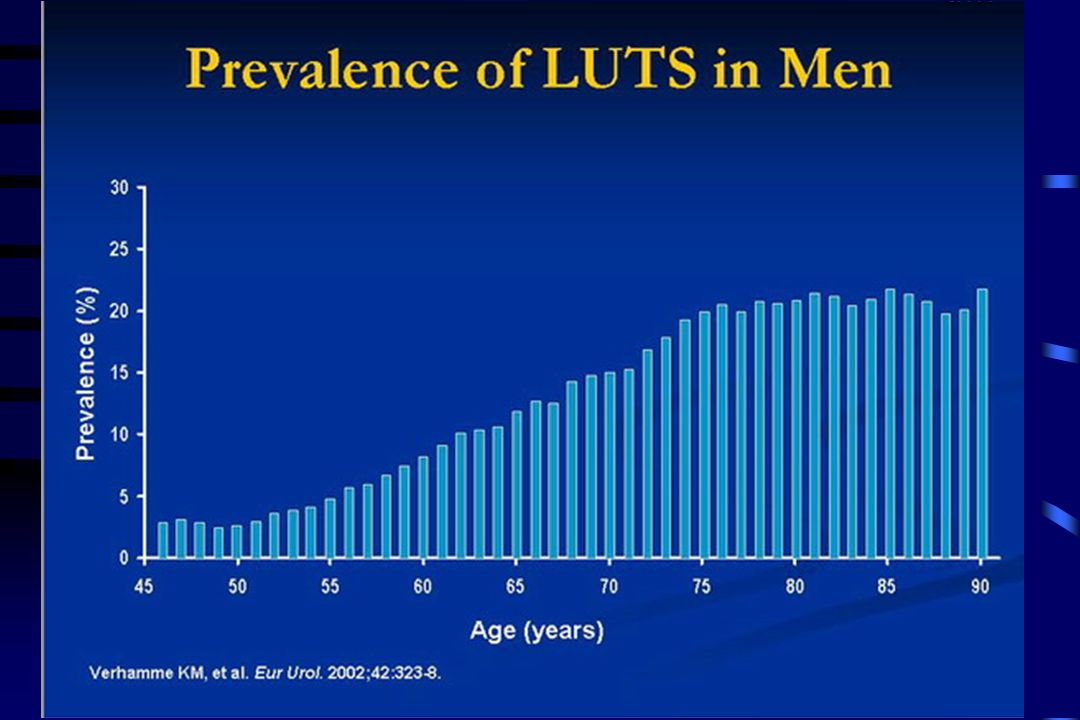
Epidemiology of BPH : age-specific prevalence
Adapted from Guess, 1990

14
Comparison of Data From the SIFO Study 1997 and the EPIC Study 2005
Sintomi irritativi sono prevalenti in uomini e donne con l’aumento dell’età Comparison of Data From the SIFO Study and the EPIC Study 2005 40 35 Men – SIFO 1997 16.6% Women – SIFO 1997 30 Men – 2005 25 Women ̶ 2005 11.8% Prevalence, % 20 15 Prevalence of OAB is similar in men and women and increases with age.1-2 These results were demonstrated through 2 multi-national prevalence studies conducted in 1997 (Milsom et al) and 2005 (Irwin et al).1-2 The overall prevalence of OAB was 16.6% in the SIFO study and 11.8% in the EPIC study.1-2 References Milsom I, Abrams P, Cardozo L, Roberts RG, Thüroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int. 2001;87: Irwin DE, Milsom I, Hunskaar S, et al. population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50: 10 5 18-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70+ Age, years Milsom I et al. BJU Int. 2001;87: Irwin DE et al. Eur Urol. 2006;50:
 and 2005 (Irwin et al).1-2 The overall prevalence of OAB was 16.6% in the SIFO study and 11.8% in the EPIC study.1-2. References. Milsom I, Abrams P, Cardozo L, Roberts RG, Thüroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed A population-based prevalence study. BJU Int. 2001;87: Irwin DE, Milsom I, Hunskaar S, et al. population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50: Age, years. Milsom I et al. BJU Int. 2001;87: Irwin DE et al. Eur Urol. 2006;50:")
15
LUTS etiologia Vescica iperattiva Ostruzione Ipertrofia Altro?

17
LUTS & disfunzione sessuale: legami ipotetici
L’età è il fattore comune?? L’impatto dei LUTS sulla QoL produce ED? Esiste una fisiopatologia comune? BPH LUTS BPO

18
A Ponholzer and S Maderbacher, 2007

19
LUTS e sindrome metabolica
ATP III: cental obesity (waist circum >102), HDL less than 40, triglycerides more than 150 mg/dl, BP more than 135/85, fasting plasma glucose more than 110 mg/dl. BACH study (boston area 1890 pts) A recent study by Kupelian et al. [27] examined the association between LUTS and metabolic syndrome in 1899 men in the Boston Area CommunityHealth (BACH) survey. Using the ATP III guideline to characterize metabolic syndrome and the American Urologic Association symptom index (AUA-SI) to quantify LUTS, the investigators found a statistically significant association between metabolic syndrome and voiding, rather than storage symptoms. Furthermore, increased odds of metabolic syndrome in men with mild symptoms were analogous to the result observed inmenwith more severe symptoms.These observed associationswere more prevalent inmen younger than 60 years of age compared with older patients [27]. The BACH survey data examined the relative risk of having metabolic syndrome as a function of the severity of LUTS. The overall prevalence of metabolic syndrome was 29%, comparable with previously published rates from NHANESIII. Comparable with previously reported rates, the overall prevalence of moderate-to-severe LUTS (AUA-SI 8) was 19.3%; a trend toward increasing prevalence of metabolic syndrome with increasing AUA-SI was seen (Fig. 1). The lowest prevalence (20%) of metabolic syndrome was seen in men reporting no symptoms or one symptom of LUTS. This increased to 40% with mild LUTS (AUA-SI 2–7); however, no further increase was seen with moderate/severe LUTS (AUA-SI 8). The present study also demonstrated the association between metabolic syndrome and AUA-SI (Table 1) is also observed when comparing patients with mild and moderate/severe symptoms to those with an AUA-SI less than one [age-adjusted odds ratio (OR)¼1.83, 95% con- fidence interval (CI): 1.29, 2.60]. The authors found this association to be significant following multivariate analysis (multivariate OR¼1.68, 95% CI: 1.21, 2.35). Combined, these results demonstrate that LUTS, assessed by the AUA-SI, are associated with metabolic syndrome. Possible pathophysiologic mechanisms at play to explain the relationship with metabolic syndrome include the influence of sustained hyperglycemia on the viability of parasympathetic neurons in the pelvic ganglion. AUA SI ≥8; OR: 1.85 ( ) AUA SI Voiding ≥5; OR: 1.82 (1.1, 3.01) AUA SI Storage ≥ 4; OR 1.35 (0.96, 1.91) Moul S and Mc Vary T, Curr Op Urol 2009
, HDL less than 40, triglycerides more than 150 mg/dl, BP more than 135/85, fasting plasma glucose more than 110 mg/dl. BACH study (boston area 1890 pts) A recent study by Kupelian et al. [27] examined the association between LUTS and metabolic syndrome in 1899 men in the Boston Area CommunityHealth (BACH) survey. Using the ATP III guideline to characterize metabolic syndrome and the American Urologic Association symptom index (AUA-SI) to quantify LUTS, the investigators found a statistically significant association between metabolic syndrome and voiding, rather than storage symptoms. Furthermore, increased odds of metabolic syndrome in men with mild symptoms were analogous to the result observed inmenwith more severe symptoms.These observed associationswere more prevalent inmen younger than 60 years of age compared with older patients [27]. The BACH survey data examined the relative risk of having metabolic syndrome as a function of the severity of LUTS. The overall prevalence of metabolic syndrome was 29%, comparable with previously published rates from NHANESIII. Comparable with previously reported rates, the overall prevalence of moderate-to-severe LUTS (AUA-SI 8) was 19.3%; a trend toward increasing prevalence of metabolic syndrome with increasing AUA-SI was seen (Fig. 1). The lowest prevalence (20%) of metabolic syndrome was seen in men reporting no symptoms or one symptom of LUTS. This increased to 40% with mild LUTS (AUA-SI 2–7); however, no further increase was seen with moderate/severe LUTS (AUA-SI 8). The present study also demonstrated the association between metabolic syndrome and AUA-SI (Table 1) is also observed when comparing patients with mild and moderate/severe symptoms to those with an AUA-SI less than one [age-adjusted odds ratio (OR)¼1.83, 95% con- fidence interval (CI): 1.29, 2.60]. The authors found this association to be significant following multivariate analysis (multivariate OR¼1.68, 95% CI: 1.21, 2.35). Combined, these results demonstrate that LUTS, assessed by the AUA-SI, are associated with metabolic syndrome. Possible pathophysiologic mechanisms at play to explain the relationship with metabolic syndrome include the influence of sustained hyperglycemia on the viability of parasympathetic neurons in the pelvic ganglion. AUA SI ≥8; OR: 1.85 ( ) AUA SI Voiding ≥5; OR: 1.82 (1.1, 3.01) AUA SI Storage ≥ 4; OR 1.35 (0.96, 1.91) Moul S and Mc Vary T, Curr Op Urol")
20
Infiammazione e LUTS * * * * Moul S and Mc Vary T, Curr Op Urol 2009
A recent study by Kupelian et al. [35] examined the relationship between C-reactive protein (CRP) levels, an inflammatory marker, and LUTS, as assessed by the AUA-SI. Working with the BACH Survey and a multistage stratified design, 5502 adults ages 30–79 years were recruited. The investigators obtained blood samples for 3757 participants. Analyses and CRP levels were performed in 1898 men and 1854 women. The authors found a statistically significant association between CRP levels and overall LUTS among both men and women; however, the pattern of association between CRP levels and individual symptoms varied by sex (Fig. 2) [36]. In men, nocturia and straining were associated with higher CRP levels; in women, incomplete emptying and weak stream vvvv * * C-reactive protein levels Moul S and Mc Vary T, Curr Op Urol 2009
 levels, an inflammatory marker, and LUTS, as assessed by the AUA-SI. Working with the BACH Survey and a multistage stratified design, 5502 adults ages 30–79 years were recruited. The investigators obtained blood samples for 3757 participants. Analyses and CRP levels were performed in 1898 men and 1854 women. The authors found a statistically significant association between CRP levels and overall LUTS among both men and women; however, the pattern of association between CRP levels and individual symptoms varied by sex (Fig. 2) [36]. In men, nocturia and straining were associated with higher CRP levels; in women, incomplete emptying and weak stream. vvvv. * * C-reactive protein levels. Moul S and Mc Vary T, Curr Op Urol")
21
LUTS Renal CNS BPO OAB Pituitary Cardiac Metabolic
CNS BPO OAB But LUTS is really multifactorial. Pituitary Cardiac Metabolic

22
Legami possibili tra sintomi ostruttivi ed irritativi
Supersensibilità alla Ach Ridotta risposta alla stimolazione intramurale nervosa Ipertrofia detrusore Aumento NGF Denervazione parziale Ischemia Aumento accoppiamento elettrico Ipertrofia/iperplasia Instabilità del potenziale di membrana Alterata regolazione Intracellulare Ca2+ Ostruzione Iperattività Symptoms of OAB and DO may develop secondary to BOO in men. There are several potential etiologies for this relationship. BOO can result in partial denervation or abnormal expression of nerve growth factor or can affect the detrusor muscle itself. These potential etiologies can cause a cascade of events that lead to OAB/DO in men. Reference Steers WD. Rev Urol. 2002;4:S7-S18. Ri-organizzazione dei riflesso minzioanle (C-fibre mediated) Alterata funzione/espressione dei canali del sodio Ipertrofia dei neuroni afferenti ed effeernti Steers WD. Rev Urol. 2002;4:S7-S18.
 Alterata funzione/espressione. dei canali del sodio. Ipertrofia dei neuroni. afferenti ed effeernti. Steers WD. Rev Urol. 2002;4:S7-S18.")
23
Punto della situazione
LUTS sono progressivi, legati all’età, non sesso o organo specifici Numerose eziologie Nuove terminologie Necessità di cambiare approccio ai sintomi e alle terapie

24
Associazioni di farmaci 1
Certezze

25
STUDIO COMBAT (Roehrborn, Siami, Europ. Urol, 2010)
4844 PAZIENTI IPB SOPRA I 50 ANNI (MEDIA 66) TUTTI CON IPB (OSTRUZIONE >5 e < 15 ml/s) PSA COMPRESO TRA 1,5 e 10 (MEDIA 4) ATTIVI SESSUALMENTE 73% IPSS > 12 DIMENSIONE MEDIA PROSTATA 49 CM3
 TUTTI CON IPB (OSTRUZIONE >5 e < 15 ml/s) PSA COMPRESO TRA 1,5 e 10 (MEDIA 4) ATTIVI SESSUALMENTE 73% IPSS > 12. DIMENSIONE MEDIA PROSTATA 49 CM3.")
26
Protocollo studio Combat 4 anni

27
STUDIO COMBAT obiettivo principale
vedere se e quanto si riducono i casi di ritenzione urinaria acuta e di chirurgia IPB-correlata nel braccio di associazione rispetto le singole terapie

28
NUMERO CUMULATIVO DI CASI DI RITENZIONE - CHIRURGIA
1 episodio prevenuto ogni 15 pazienti 1 episodio prevenuto ogni 13 pazienti

29
RISULTATI A 4 ANNI LA TERAPIA DI COMBINAZIONE RIDUCE IL RISCHIO DI RITENZIONE URINARIA ACUTA O DI CHIRURGIA DEL 65,8% RISPETTO AL SOLO TAMSULOSIN (dato associato*) LA TERAPIA CON SOLO DUTASTERIDE HA RISULTATI SOVRAPPONIBILI CON QUELLA DI ASSOCIAZIONE : LA DIFFERENZA NON E’ STATISTICAMENTE SIGNIFICATIVA TRA GRUPPO DI ASSOCIAZIONE E GRUPPO SOLO DUTASTERIDE
 LA TERAPIA CON SOLO DUTASTERIDE HA RISULTATI SOVRAPPONIBILI CON QUELLA DI ASSOCIAZIONE : LA DIFFERENZA NON E’ STATISTICAMENTE SIGNIFICATIVA TRA GRUPPO DI ASSOCIAZIONE E GRUPPO SOLO DUTASTERIDE.")
30
*La ritenzione si riduce del 67,6 %
*La chirurgia correlata all’IPB del 70,6 %

31
Altri dati: questionario IPSS (STATO DI SALUTE PERCEPITO)
")
32
Altri dati: uroflussimetria

33
EFFETTI COLLATERALI (%):
ì TUTTI GLI EVENTI AVVERSI GRAVI CORRELATI ALLE TERAPIE: TAM. <1 DUT. <1 COMB. <1 TUTTI GLI EVENTI AVVERSI CORRELATI ALLE TERAPIE CHE PORTANO ALL’USCITA DALLA SPERIMENTAZIONE: TAM. 6 DUT. 4 COMB. 4

34
EFFETTI COLLATERALI SULLA SESSUALITA’ (%):
Disfunzione erettile TAM. 5 DUT. 7 COMB. 9 Eiaculazione retrograda TAM. 1 DUT. <1 COMB. 4 Diminuzione della libido TAM. 2 DUT. 3 COMB. 4 Perdita della libido TAM. 1 DUT. 1 COMB. 2

35
Quesito

36
2 meglio di 1 ? COMBAT PLESS MTOPS

37
Nuovi farmaci

38
silodosina Silodosina: nuovo alfabloccante che riduce l’IPSS soprattutto nei pazienti con sintomi gravi Inizio rapido di azione 3-4gg Innalzamento Q max entro 2-6ore Retroejaculazione 22–28% E’capace di migliorare l’ostruzione e anche l’iperattività del detrusore Marks LS, J Urol 2009; Djavan B, Curr Opin Urol 2011

39
anticolinergici Uso di anticolinergici (in particolare tolterodina formulazione rilascio prolungato) associato con con tamsulosina è in grado di migliorare : Urgenza e Incontinenza da urgenza Frequenza diurna e Nicturia IPSS e QoL I pazienti con prostate più piccole (<29ml), con sintomi più gravi e con sintomi da vescica iperattiva beneficiano molto dell’uso di tolterodina Anche se alfalitico + dutasteride, la tolterodina riduce i sintomi irritativi Chung DE, Urology 2010; Djavan B, Curr Opin Urol 2011
 associato con con tamsulosina è in grado di migliorare : Urgenza e Incontinenza da urgenza. Frequenza diurna e Nicturia. IPSS e QoL. I pazienti con prostate più piccole (<29ml), con sintomi più gravi e con sintomi da vescica iperattiva beneficiano molto dell’uso di tolterodina. Anche se alfalitico + dutasteride, la tolterodina riduce i sintomi irritativi. Chung DE, Urology 2010; Djavan B, Curr Opin Urol")
40
inibitori 5fosfodiesterasi
Inibitori della PDE5 non agiscono solo nel corpo cavernoso ma anche nel collo vescicale, uretra e prostata Tadalafil è in grado di migliorare : funzione erettiva punteggio sintomatologico IPSS residuo postminzionale Proposto uso quotidiano di Tadalafil nel trattamento di LUTS con ED Dmochowski R, J Urol 2010 Wang C. Curr Opin Urol 2010 Djavan B, Curr Opin Urol 2011

41
nuovi inibitori 5fosfodiesterasi
UK-369,003 UK-369,003 è un nuovo e potente cGMP-specific PDE5 inhibitor. Altissima selettività per la PDE5 In uno studio vs placebo alta tolleranza e ottimo incremento del flusso massimo in confronto con altri farmaci analoghi Djavan B, Curr Opin Urol 2011

42
Saranno necessari studi preclinici
antagonisti GH La presenza di recettori per il GH nelle cellule di prostata suggerisce l’uso di antagonisti del GHRH nella IPB Saranno necessari studi preclinici Djavan B, Curr Opin Urol 2011

43
Possiamo seguire i sintomi per la terapia?
Combination therapy Life style intervention

44
Possiamo seguire i sintomi per la terapia?
Gravas S, Curr Op Urol 2009

45
Djavan B, Curr Op Urol 2011

46
Djavan B, Curr Op Urol 2011

48
YU X., et al., The Journal of Urology, 2008

49
TUNA rilascia energia a microonde direttamente nella prostata

50
TUNA Generatore a radiofrquenze 18 F cistoscopio dedicato

51
TUNA 2 aghi flessibili, inseribili nella prostata, emergendo dalla punta del cistoscopio

52
TUNA Radiofrequency Heat (70– 110 °C) Necrosis (460 kHz)
Baermoshe S., et al., World J Urol, 2006 Energy is delivered by needles into the prostate and produces localized necrotic lesions in the hyperplastic tissue Baermoshe S., World J Urol, 2006

53
TUNA Lesions are performed symmetrically on each side of the prostate starting from the bladder neck Baermoshe S., World J Urol, 2006






















>")

