Scaricare la presentazione
1
MSO, School of Oncology Optimal approach to medical management of synchronous colorectal liver metastases Roma, 4 marzo 2011 Dott.ssa Angela Torsello Angela TORSELLO Oncologia Medica A Istituto Regina Elena, Roma

2
Colorectal cancer liver metastases

3
Colorectal cancer liver metastases
25% synchronous with the primary tumor 20% metachronous Mets sinchronous : More often bilobar and greater in number/size Poorer survival Different management (i.e. the resection time of primary tumor and liver metastases represent an important issue) Tan EK et al, Ann Acad Med 2010
 Tan EK et al, Ann Acad Med")
4
Treatment of Colorectal Liver Metastases
In patients with liver metastases the main topic is to evaluate lesions resectability or the possibility of the lesions to became resectable after neoadjuvant chemotherapy: Strangl R et al. Lancet 1994

5
5-y Survival Liver resection= Possibility to cure
Resected patients: 25-40% Liver resection= Possibility to cure Adam R.

6
Synchronous Colorectal Liver Metastases I
Should primary tumor be resected before starting sistemic treatment? This could represent a problem in the control of disease (delayed sistemic treatment) BUT….. Importance of patient symptoms: subocclusion/occlusion, bleeding…
 BUT….. Importance of patient symptoms: subocclusion/occlusion, bleeding…")
7
Synchronous Colorectal Liver Metastases II
Should liver metastases be resected at the same time as the primary tumor? a) Importance of primary tumor site: - right sided tumors could be better resected at the same time of liver metastases in selected patients; left sided tumor (especially rectal cancer) present more thecnically difficulties and post-operative risks b) A delayed (3-6 months) liver resection and chemotherapy administration permits a “test of time”: selection of patients who really benefits of liver resection with curative intention
 Importance of primary tumor site: - right sided tumors could be better resected at the same time of liver metastases in selected patients; left sided tumor (especially rectal cancer) present more thecnically difficulties and post-operative risks. b) A delayed (3-6 months) liver resection and chemotherapy administration permits a test of time : selection of patients who really benefits of liver resection with curative intention.")
8
Surgery in synchronous colorectal liver metastases
The optimal timing of synchronous metastases resction is not well defined Surgical strategy are defined as combined (combined resection of primary and liver), classic (primary before liver) and reverse (liver before primary) These surgical strategies are associated with similar outcomes The combined strategy is considered safe with no different in morbidity and mortality rates or in severity of complications, compared with staged resection
, classic (primary before liver) and reverse (liver before primary) These surgical strategies are associated with similar outcomes. The combined strategy is considered safe with no different in morbidity and mortality rates or in severity of complications, compared with staged resection.")
9
Reverse approach Recently this kind of surgical approach is considered for rectal cancer with synchronous liver metastases The treatment sequence proposed is the following: Systemic chemotherapy followed by liver resection Chemoradiation followed by rectal resection Van der Pool et al, ASCO 2010 abs e14027

10
Postoperative outcome of 142 pts with different surgical strategy for synchronous liver mets
Combined (n=43) Classic (n=72) Reverse (n=27) p Margin status for resection of primary (%) R0 41 (95) 68 (94) 25 (93) NS R1 2 (5) 4 (6) 2 (7) Type of liver resection ≥3 liver segments, n (%) 15 (35) 48 (66) 24 (89) <0.01 Margin status for resection of metastases 40 (93) 62 (86) 23 (85) 3 (7) 9 (13) 4 (15 Blood transfusion requirement, n (%) 7 (16) 30-d postoperative mortality 2 (3) 90-d postoperative mortality 1 (4) Overall postoperative morbidity 20 (47) 37 (51) 10 (37) Cumulative major postoperative complication 8 (19) 12 (17) Brouquet A et al, J Am Coll Surg 2010
 Classic (n=72) Reverse (n=27) p. Margin status for resection of primary (%) R0. 41 (95) 68 (94) 25 (93) NS. R1. 2 (5) 4 (6) 2 (7) Type of liver resection. ≥3 liver segments, n (%) 15 (35) 48 (66) 24 (89) <0.01. Margin status for resection of metastases. 40 (93) 62 (86) 23 (85) 3 (7) 9 (13) 4 (15. Blood transfusion requirement, n (%) 7 (16) 30-d postoperative mortality. 2 (3) 90-d postoperative mortality. 1 (4) Overall postoperative morbidity. 20 (47) 37 (51) 10 (37) Cumulative major postoperative complication. 8 (19) 12 (17) Brouquet A et al, J Am Coll Surg")
11
The impact of multidisciplinary management
100 2009 chemotherapy Median survival >24 months 5 year survival % 2009 overall (Surgery + Chemo) Median survival ~36 months 5 year survival % % surviving 50 2019? 1999 20% 9% 3% Years after diagnosis of colorectal metastases Poston GJ. EJSO 2005; 31:
 Median survival ~36 months. 5 year survival 20 % % surviving % 9% 3% Years after diagnosis of colorectal metastases. Poston GJ. EJSO 2005; 31:")
12
Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial Nordlinger et al, Lancet 2008

13
Postoperative complications Peri-op Surg
Number in group Reversible postoperative complications† (25%) (16%) Cardio-pulmonary failure (2%) (1%) Bleeding (2%) (2%) Biliary fistula (8%) (4%) Output >100 mL/day for >10 days (6%) (1%) Hepatic failure (7%) (5%) Bilirubin >100 mg/day for >3 days (6%) (3%) Wound infection (3%) (2%) Intra-abdominal infection (7%) (2%) Need for reoperation (3%) (2%) Urinary infection (3%) Pleural effusion (2%) (1%) Pulmonary embolism/deep-venous thrombosis (1%) (1%) Pneumopathy (1%) Neutropenia (1%) Ascites (1%) (1%) Ileus (1%) (1%) Cardiac arrhythmia (1%) Renal failure (1%) Other (3%) (2%) Postoperative death (1%) (1%)
 27 (16%) Cardio-pulmonary failure 3 (2%) 2 (1%) Bleeding 3 (2%) 3 (2%) Biliary fistula 13 (8%) 7 (4%) Output >100 mL/day for >10 days 9 (6%) 2 (1%) Hepatic failure 11 (7%) 8 (5%) Bilirubin >100 mg/day for >3 days 10 (6%) 5 (3%) Wound infection 5 (3%) 4 (2%) Intra-abdominal infection 11 (7%) 4 (2%) Need for reoperation 5 (3%) 3 (2%) Urinary infection 4 (3%) 0. Pleural effusion 3 (2%) 1 (1%) Pulmonary embolism/deep-venous thrombosis 2 (1%) 1 (1%) Pneumopathy 2 (1%) 0. Neutropenia 2 (1%) 0. Ascites 1 (1%) 1 (1%) Ileus 2 (1%) 1 (1%) Cardiac arrhythmia 0 1 (1%) Renal failure 0 1 (1%) Other 4 (3%) 4 (2%) Postoperative death 1 (1%) 2 (1%)")
14
The timing of chemotherapy and surgery
Liver mets resectable at presentation: the perioperative chemotherapy has become the standard treatment in many institutions (to be performed after maximum 6 cycles of chemotherapy) Liver mets initially not resectable: monitoring patients during chemotherapy to perform surgery as soon as the metastases become resectable Nordlinger et al, Clin Colorectal Can 2010 and Ann Oncol 2009
 Liver mets initially not resectable: monitoring patients during chemotherapy to perform surgery as soon as the metastases become resectable. Nordlinger et al, Clin Colorectal Can 2010 and Ann Oncol")
15
Liver metastases treatment
85% non resectable 15% resectable Neoadjuvant chemotherapy Potentially resectable (4-30%) R0 R0 uncertain more? FA/FU FU/OXA o CPT11 FA/OXA/CPT11 (Triplet) Target therapies
 R0. R0 uncertain. more FA/FU. FU/OXA o CPT11. FA/OXA/CPT11. (Triplet) Target therapies.")
16
Topics of liver metastases neoadiuvant chemotherapy
Patients selection Type of treatment (systemic; hepatic intra-arterial) and schedule (new biological drugs) Liver damage Respose to treatment (complete vs partial response)
 and schedule (new biological drugs) Liver damage. Respose to treatment (complete vs partial response)")
17
PATIENTS SELECTION

18
What does it mean “resectable disease”?
Traditional controindications: ≥ 4 metastases Size Extrahepatic disease Ilar disease Resection margin< 1 cm Incomplete resection Adam R., et al. Ann Surg Onc 2000 9 48 12 26 10 20 30 40 50 large Multi-nodular ill-located extra-hepatic Now is admitted: Resection margin≤ 1 cm Number Size Extrahepatic disease Need standard resection criteria

19
French Recommendations 2003
Potentially resectable= class I (involvement max 4 anatomic segments; non-involvement of cava vein, almost one of hepatic veins and controlateral portal pedunculus)* Potentially resectable= classe II (involvement of 5-6 anatomic segments and/or major controlateral vascular structures)* Not resectble that became resectable= classe III Never resectable= classe IV *Classe I = easily resectable Classe II= resectable with difficult
* Potentially resectable= classe II (involvement of 5-6 anatomic segments and/or major controlateral vascular structures)* Not resectble that became resectable= classe III. Never resectable= classe IV. *Classe I = easily resectable. Classe II= resectable with difficult.")
21
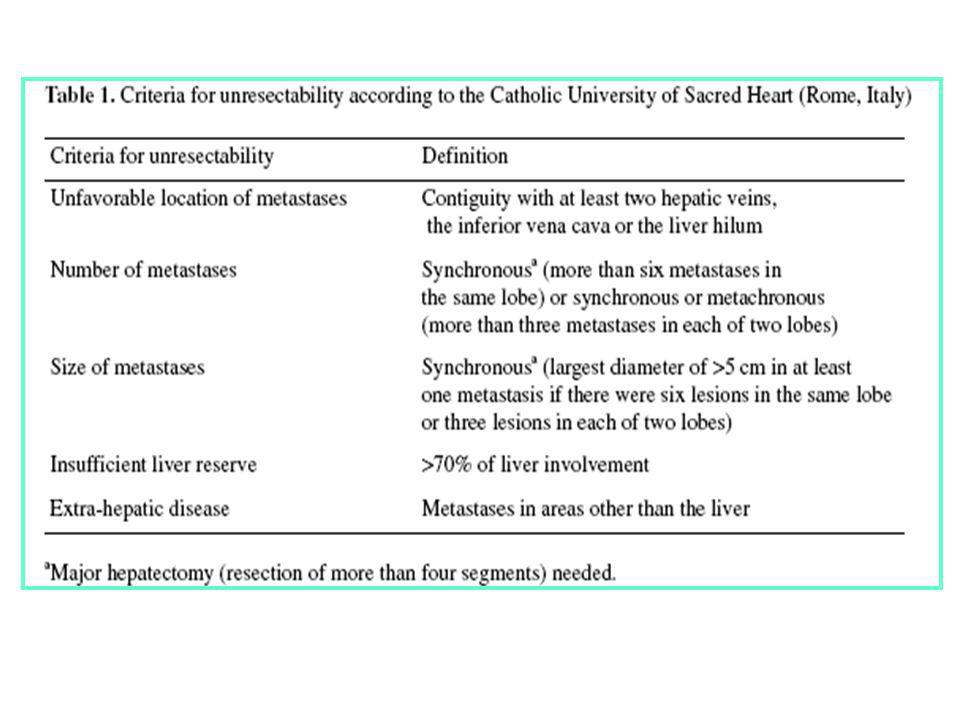
Criteri di non resecabilità (IRE):
Size Multinodular Ilar location Extraepatic disease Patients with >3 metastases who receive chemotherapy in order to stabilize liver disease before surgery Patients who present with huge resectable liver metastases at the time of resection of the primary tumor and need extended liver surgery

22
CRC Staging: IV Stage (Consensus 2006)
Stage IVa: “easily resectable liver metastases” Stage IVb: “resectable liver metastases” Stage IVc: “liver metastases thet may become resectable after downsizing” Stage IVd: “liver metastases that are unlikely to become resectable”* Stage Va: “resectable disease outside the liver” Stage Vb: “unresectable disease outside the liver”* *never resectable EJC, 2006

23
It is important: Staging of metastastic patients (TC, US, RMN, PET) Resection criteria Prognostic factors (outcome predictors)
 .")
24
NEOADJUVANT CHEMOTHERAPY

25
Response rate and surgery of metastases
(First line 5-FU, LV and l-OHP) 40 93-94 Chrono 4-10 30 90-93 94-96 20 Complete resection of metastases (%) Chrono 5-16 90-93 10 Flat 5-16 r = 0.96 ; p = 30 40 50 60 70 Objective responses (%) Secondary surgery of metastases : major prognostic factor of survival
 Chrono Complete resection of metastases (%) Chrono Flat r = 0.96 ; p = Objective responses (%) Secondary surgery of metastases : major prognostic factor of survival.")
26
Resection rate of metastases and tumor response
Folprecht G, et al. Ann Oncol 2005;16:1311–1319 Studies including selected patients (liver metastases only, no extrahepatic disease) (r=0.96; p=0.002) 0.6 0.5 0.4 Studies including nonselected patients with mCRC (solid line) (r=0.74; p<0.001) Resection rate 0.3 0.2 0.1 Phase III studies including nonselected patients with mCRC (dashed line) (r=0.67; p=0.024) 0.3 0.4 0.5 0.6 0.7 0.8 0.9 Response rate
 (r=0.96; p=0.002) Studies including nonselected patients with mCRC (solid line) (r=0.74; p<0.001) Resection rate Phase III studies including. nonselected patients with mCRC (dashed line) (r=0.67; p=0.024) Response rate.")
27
Which Regimen: doublets or triplets?
Pozzo C. et al Cancer Treat Rev, 2008

28
Triplets 1) Activity and efficacy increase 2) Resection rate increase
3) Balance between activity and toxicity 4) Acute toxicity acceptable
 Balance between activity and toxicity. 4) Acute toxicity acceptable.")
29
Treatment of metastatic CRC New drugs and new combinations
Oral 5-FUs (capecitabine, UFT) Irinotecan Oxaliplatin Cetuximab Bevacizumab Tumor response rates typically >50−60% …and even 72% 29
 Irinotecan. Oxaliplatin. Cetuximab. Bevacizumab. Tumor response rates typically >50−60% …and even 72% 29.")
30
Cetuximab and resection rate in first-line FOLFIRI-based regimen
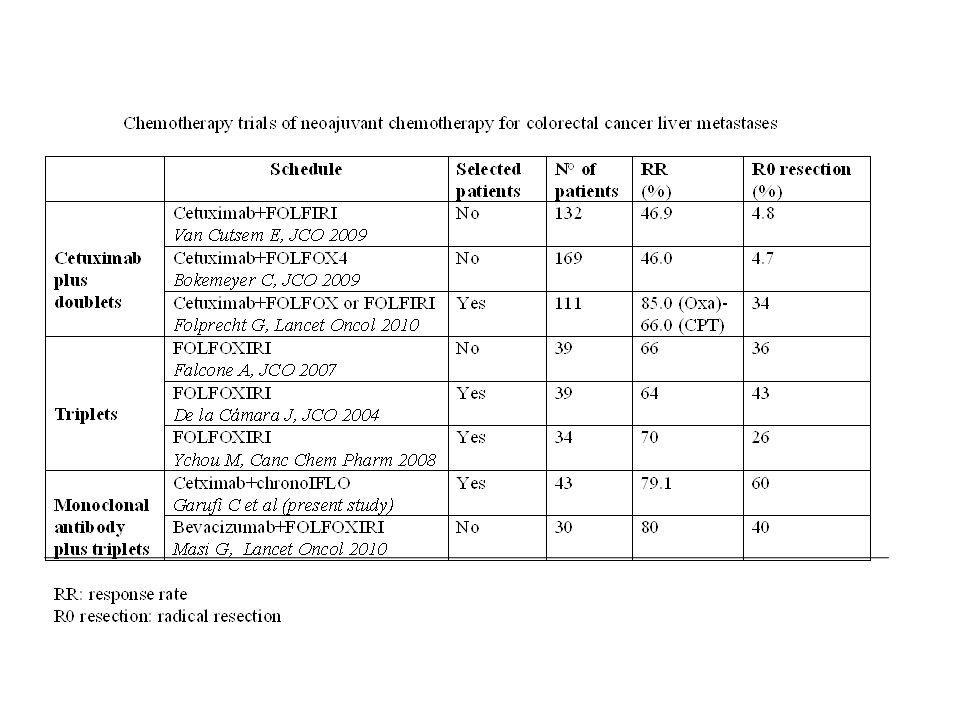
Folprecht et al 2006 Peeters et al 2005 Van Cutsem et al 2007 Trial Phase I/II Phase III Treatment regimen Cetuximab + irinotecan/AIO FOLFIRI No. of patientsa 21 42 599 Overall response rate (%) 67 45 47 Disease control rate (%) 96 83 84 Resection rate (%) 24b 24 6 R0 Resection rate (%) 19 4 (10c) - These studies report resection rates of between 6% and 61%.[1-7] Folprecht et al [2] reported 5 patients eligible for resection but one of these declined surgery. - An earlier analysis has shown that resection rates correlate with response rates in selected patients.[6] - The highest resection rate, reported by Garufi et al[5], was in patients with colorectal liver only metastases selected for treatment. The other studies were in unselected patient populations. - In the CRYSTAL study [3], the R0 resection rate for patients with liver limited disease was 9.8%. 1. Peeters M, Raoul J-L, Van Laethem J-L, et al. Eur J Cancer 2005;Supplement 3:Abstract 664 2. Folprecht G, Lutz M, Schoeffski et al. Ann Oncol 2006;17: 3. Van Cutsem Bodoky G, Kyung Roh J, et al. Eur J Cancer Suppl 2007;5:235 (Abstract O-3001). Updated information presented at ECCO 2007 4. Tabernero J, Van Cutsem E, Diaz-Rubio E, et al. J Clin Oncol 2007;25: 5. Garufi C, Tumolo S, Torsello A, et al.ASCO 2008 Gastrointestinal Cancers Symposium (Abstract No: 367) 6. Folprecht G, Grothey A, Alberts S, et al. Ann Oncol 2005;16(8): 7. Bokemeyer C, Staroslawska E, Mahkson A, et al. Eur J Cancer Suppl 2007;5:236 (Abstract O-3004). Updated information presented at ECCO 2007 A Patients in ERBITUX arm; b5 patients became eligible for resection, 4 underwent surgery; cR0 resection rate in patients with liver limited disease
 Disease control rate (%) Resection rate (%) 24b R0 Resection rate (%) (10c) - These studies report resection rates of between 6% and 61%.[1-7] Folprecht et al [2] reported 5 patients eligible for resection but one of these declined surgery. - An earlier analysis has shown that resection rates correlate with response rates in selected patients.[6] - The highest resection rate, reported by Garufi et al[5], was in patients with colorectal liver only metastases selected for treatment. The other studies were in unselected patient populations. - In the CRYSTAL study [3], the R0 resection rate for patients with liver limited disease was 9.8%. 1. Peeters M, Raoul J-L, Van Laethem J-L, et al. Eur J Cancer 2005;Supplement 3:Abstract Folprecht G, Lutz M, Schoeffski et al. Ann Oncol 2006;17: Van Cutsem Bodoky G, Kyung Roh J, et al. Eur J Cancer Suppl 2007;5:235 (Abstract O-3001). Updated information presented at ECCO Tabernero J, Van Cutsem E, Diaz-Rubio E, et al. J Clin Oncol 2007;25: Garufi C, Tumolo S, Torsello A, et al.ASCO 2008 Gastrointestinal Cancers Symposium (Abstract No: 367) 6. Folprecht G, Grothey A, Alberts S, et al. Ann Oncol 2005;16(8): Bokemeyer C, Staroslawska E, Mahkson A, et al. Eur J Cancer Suppl 2007;5:236 (Abstract O-3004). Updated information presented at ECCO A Patients in ERBITUX arm; b5 patients became eligible for resection, 4 underwent surgery; cR0 resection rate in patients with liver limited disease.")
31
CRYSTAL: resection rate ITT
Cetuximab raddoppia i pazienti portati alla chirurgia e triplica le % di R0 Curative liver resections Resection rate (%) CRYSTAL FOLFIRI ERBITUX + FOLFIRI Response rate (%) Response rates R R0 7 4.8 3.7 1.8
 CRYSTAL. FOLFIRI. ERBITUX + FOLFIRI. Response rate (%) Response rates. R. R")
32
Cetuximab and resection rate in first-line FOLFOX-based regimen
Bokemeyer et al 2007 Tabernero et al Colucci et al Trial Phase II Treatment regimen Cetuximab + FOLFOX-4 FOLFOX4 No. of patientsa 169 43 67 Overall response rate (%) 46 72 64 Disease control rate (%) 85 95 NR Resection rate (%) 7 23 - R0 Resection rate (%) 5 21 - These studies report resection rates of between 6% and 61%.[1-7] Folprecht et al [2] reported 5 patients eligible for resection but one of these declined surgery. - An earlier analysis has shown that resection rates correlate with response rates in selected patients.[6] - The highest resection rate, reported by Garufi et al[5], was in patients with colorectal liver only metastases selected for treatment. The other studies were in unselected patient populations - In the CRYSTAL study [3], the R0 resection rate for patients with liver limited disease was 9.8%. 1. Peeters M, Raoul J-L, Van Laethem J-L, et al. Eur J Cancer 2005;Supplement 3:Abstract 664 2. Folprecht G, Lutz M, Schoeffski et al. Ann Oncol 2006;17: 3. Van Cutsem Bodoky G, Kyung Roh J, et al. Eur J Cancer Suppl 2007;5:235 (Abstract O-3001). Updated information presented at ECCO 2007 (CRYSTAL) 4. Tabernero J, Van Cutsem E, Diaz-Rubio E, et al. J Clin Oncol 2007;25: (ACROBAT) 5. Garufi C, Tumolo S, Torsello A, et al. ASCO 2008 Gastrointestinal Cancers Symposium (Abstract 367) 6. Folprecht G, Grothey A, Alberts S, et al. Ann Oncol 2005;16(8): 7. Bokemeyer C, Staroslawska E, Mahkson A, et al. Eur J Cancer Suppl 2007;5:236 (Abstract O-3004). Updated information presented at ECCO 2007 (OPUS) aPatients in ERBITUX arm; bR0 resection rate in patients with liver limited disease; NR, not reported
 Disease control rate (%) NR. Resection rate (%) R0 Resection rate (%) These studies report resection rates of between 6% and 61%.[1-7] Folprecht et al [2] reported 5 patients eligible for resection but one of these declined surgery. - An earlier analysis has shown that resection rates correlate with response rates in selected patients.[6] - The highest resection rate, reported by Garufi et al[5], was in patients with colorectal liver only metastases selected for treatment. The other studies were in unselected patient populations. - In the CRYSTAL study [3], the R0 resection rate for patients with liver limited disease was 9.8%. 1. Peeters M, Raoul J-L, Van Laethem J-L, et al. Eur J Cancer 2005;Supplement 3:Abstract Folprecht G, Lutz M, Schoeffski et al. Ann Oncol 2006;17: Van Cutsem Bodoky G, Kyung Roh J, et al. Eur J Cancer Suppl 2007;5:235 (Abstract O-3001). Updated information presented at ECCO 2007 (CRYSTAL) 4. Tabernero J, Van Cutsem E, Diaz-Rubio E, et al. J Clin Oncol 2007;25: (ACROBAT) 5. Garufi C, Tumolo S, Torsello A, et al. ASCO 2008 Gastrointestinal Cancers Symposium (Abstract 367) 6. Folprecht G, Grothey A, Alberts S, et al. Ann Oncol 2005;16(8): Bokemeyer C, Staroslawska E, Mahkson A, et al. Eur J Cancer Suppl 2007;5:236 (Abstract O-3004). Updated information presented at ECCO 2007 (OPUS) aPatients in ERBITUX arm; bR0 resection rate in patients with liver limited disease; NR, not reported.")
33
OPUS: resection rate ITT
Cetuximab raddoppia i pazienti portati a resezione e le % di resezioni R0

34
Panitumumab (pmab) with FOLFIRI as first-line treatment of patients (pts) with metastatic colorectal cancer (mCRC): Resections and curative surgery in a phase II single arm, multicenter study ( ). R. Hofheinz, L. Mineur, R. Greil, C. Kohne, H. Letocha, J. Thaler, E. Fernebro, E. Gamelin, L. DeCosta, M. Karthaus KRAS/WT KRAS/MT Response rate 56% 38% Resection rate 15% 7% ASCO 2010, abs 3545

35
CETUXIMAB and resection rate in pretreated patients
Aloia et al 2007 Karaboue Levi Treatment regimen Ctuximab various CT Cetuximab + chronomodulated CT Chronomodulated IFO (ia) +/- Cetuximab Treatment line > 2nd-line 3rd-line Heavily pretreated No. of patients* 151 56 32 Overall response rate, % NR 34 Resection rate, % 18 (27/151) 18 (n=8 R0, n=2 R1) 13 (n=3 R0, n=1 R1) Survival in resected patients 10 disease-free at 22 months follow-up Median PFS 11.7 months Survival estimate 80% at 21 months Median survival (all patients) 18.4 months - In the first study[1], 27 patients underwent surgery after a median of 6 cycles of treatment (data not shown): 20 of these patients had received ERBITUX + irinotecan: -- 18/27 patients (67%) had failed more than one line of therapy -- 25 patients underwent hepatectomy. - Chronomodulated chemotherapy based on irinotecan or oxaliplatin, or both, in combination with ERBITUX was investigated bu Karaboue et al.[2]: -- although patients were receiving third-line treatment, the chemotherapy regimen and the resulting surgical resection enabled survival times that were similar to those with earlier-line treatment. - The third study[3] used the hepatic arterial route for chemotherapy administration. Only 3 patients received ERBITUX in addition to triplet chemotherapy but the combination appeared to be feasible and is to be further investigated in a European study. 1. Aloia T, Levi F, Wicherts DA, et al. J Clin Oncol 2007;25(18S):Abstract Updated information presented at ASCO 2007 2. Karaboue A, Bouchahda M, Adam R, et al. J Clin Oncol 2007;25(18S):Abstract 14505 3. Levi F, Adam R, Innominato P, et al. J Clin Oncol 2007;25(18S):Abstract 14554 IFO=irinotecan/5-FU/FA/oxaliplatin; NR=not reported
 +/- Cetuximab. Treatment line. > 2nd-line. 3rd-line. Heavily pretreated. No. of patients* Overall response rate, % NR. 34. Resection rate, % 18 (27/151) 18 (n=8 R0, n=2 R1) 13 (n=3 R0, n=1 R1) Survival in resected patients. 10 disease-free at 22 months follow-up. Median PFS 11.7 months. Survival estimate 80% at 21 months. Median survival (all patients) 18.4 months. - In the first study[1], 27 patients underwent surgery after a median of 6 cycles of treatment (data not shown): 20 of these patients had received ERBITUX + irinotecan: -- 18/27 patients (67%) had failed more than one line of therapy patients underwent hepatectomy. - Chronomodulated chemotherapy based on irinotecan or oxaliplatin, or both, in combination with ERBITUX was investigated bu Karaboue et al.[2]: -- although patients were receiving third-line treatment, the chemotherapy regimen and the resulting surgical resection enabled survival times that were similar to those with earlier-line treatment. - The third study[3] used the hepatic arterial route for chemotherapy administration. Only 3 patients received ERBITUX in addition to triplet chemotherapy but the combination appeared to be feasible and is to be further investigated in a European study. 1. Aloia T, Levi F, Wicherts DA, et al. J Clin Oncol 2007;25(18S):Abstract Updated information presented at ASCO Karaboue A, Bouchahda M, Adam R, et al. J Clin Oncol 2007;25(18S):Abstract Levi F, Adam R, Innominato P, et al. J Clin Oncol 2007;25(18S):Abstract IFO=irinotecan/5-FU/FA/oxaliplatin; NR=not reported.")
36
Studio EMR 604-CELIM RESECTION (n=54) R (n=54)
Patients with technically unresectable/ ≥5 liver metastases without extrahepatic disease RESECTION ERBITUX + FOLFOX (n=54) Adjuvant therapy for 6 cycles (same schedule as pre-operatively) Technically resectable R ERBITUX + FOLFIRI (n=54) Technically unresectable 4 further treatment cycles Primary endpoint: Response rate 8 cycles (~4 months) Started December 2004
 Adjuvant therapy for 6 cycles (same schedule as pre-operatively) Technically resectable. R. ERBITUX. + FOLFIRI. (n=54) Technically unresectable. 4 further treatment cycles. Primary endpoint: Response rate. 8 cycles (~4 months) Started December")
37
Patient characteristics
FOLFOX6 + FOLFIRI + All ERBITUX patients n=56 n=55 n=111 KRAS (n=99) Wild-type 70% 71% Primary tumour site Rectal cancer 36% 52% 44% Primary tumour stage T3/4 89% 83% 86% Adjuvant chemotherapy 9% 23% 16% Adjuvant radiotherapy 4% 15% 8%
 Wild-type. 70% 71% Primary tumour site. Rectal cancer. 36% 52% 44% Primary tumour stage. T3/4. 89% 83% 86% Adjuvant chemotherapy. 9% 23% 16% Adjuvant radiotherapy. 4% 15% 8%")
38
Resections by patient subgroup
Technically ≥ 5 liver KRAS non-resectable metastases wild-type n=57 n=48 n=67 All resections 40% 44% 43% (23 pts) (21 pts) (29 pts) R0 resections 32% 34% (18 pts) (19 pts) Comparison of R0 resections between strata technically non-resectable and ≥ 5 liver mets: p=0.4
 (21 pts) (29 pts) R0 resections. 32% 34% (18 pts) (19 pts) Comparison of R0 resections between strata technically non-resectable and ≥ 5 liver mets: p=0.4.")
39
POCHER STUDY RESECTION for 4-6 courses 4 further treatment cycles
Patients with unresectable liver metastases +/- extrahepatic disease RESECTION Adjuvant therapy for 4-6 courses (same schedule as pre-operatively) Technically resectable ERBITUX + CPT-FFL ~ (n=43) for 4-6 courses Technically unresectable 4 further treatment cycles Primary endpoint: Response rate 8 cycles (~4 months) Started December 2004
 Technically resectable. ERBITUX. + CPT-FFL ~ (n=43) for 4-6 courses. Technically unresectable. 4 further treatment cycles. Primary endpoint: Response rate. 8 cycles (~4 months) Started December")
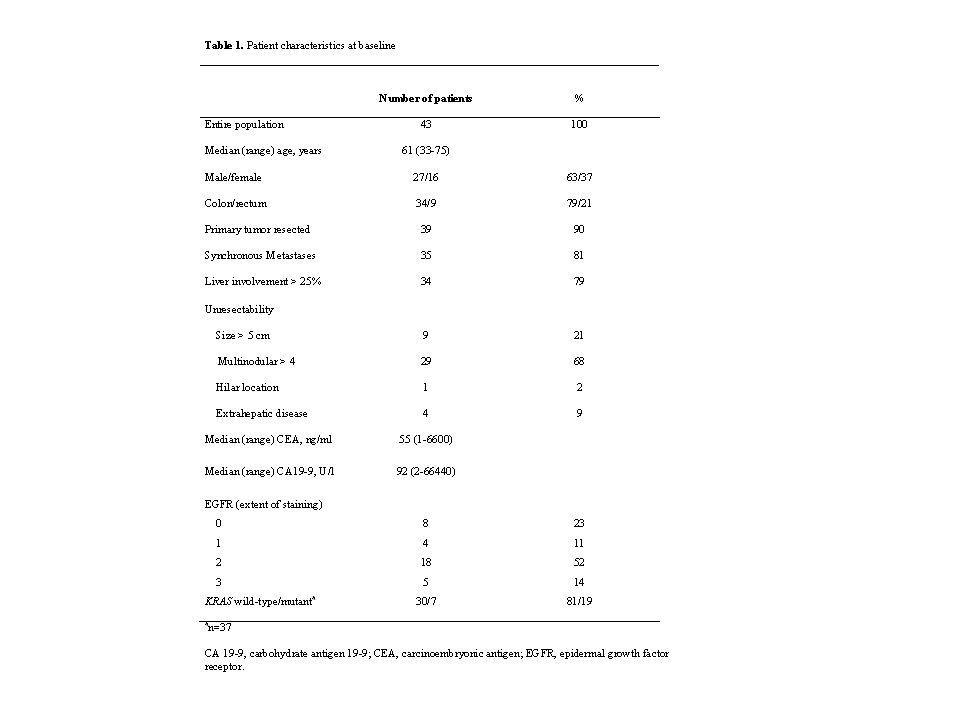
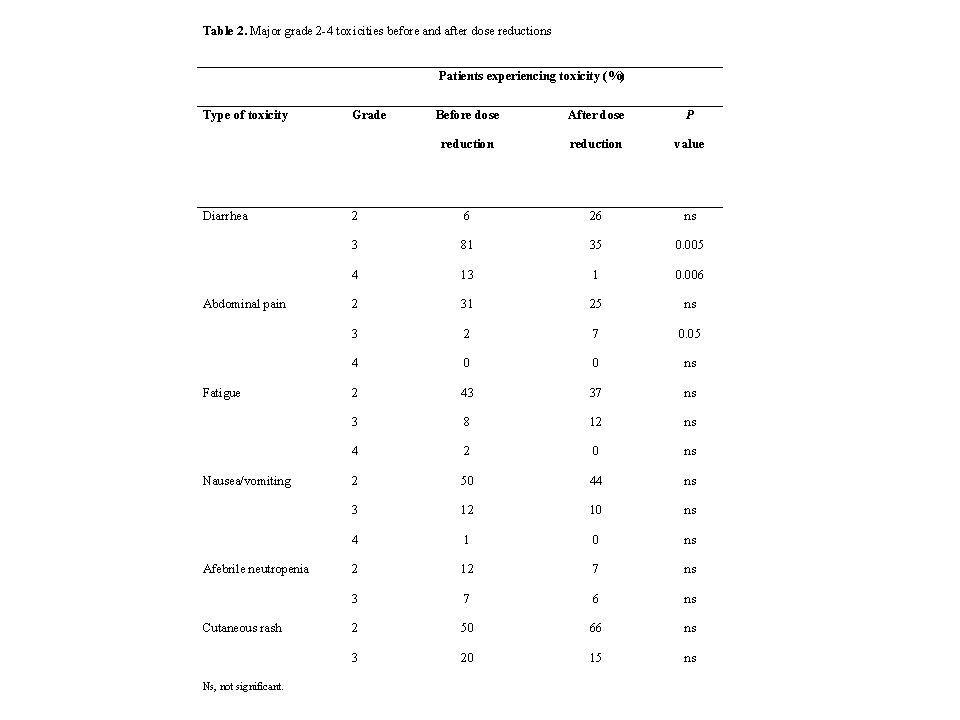
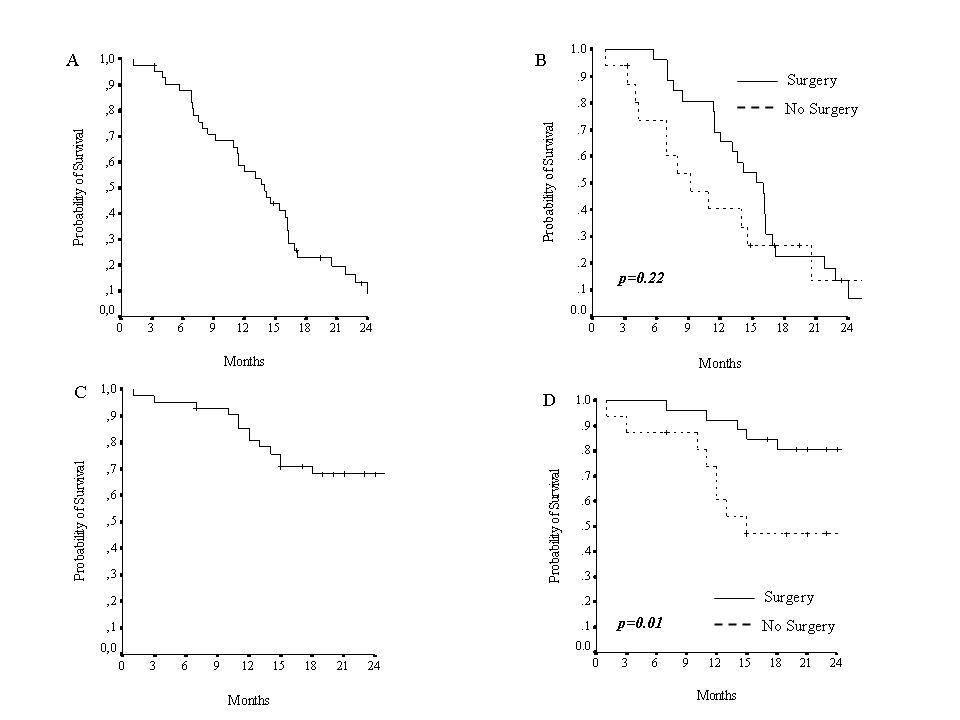
41
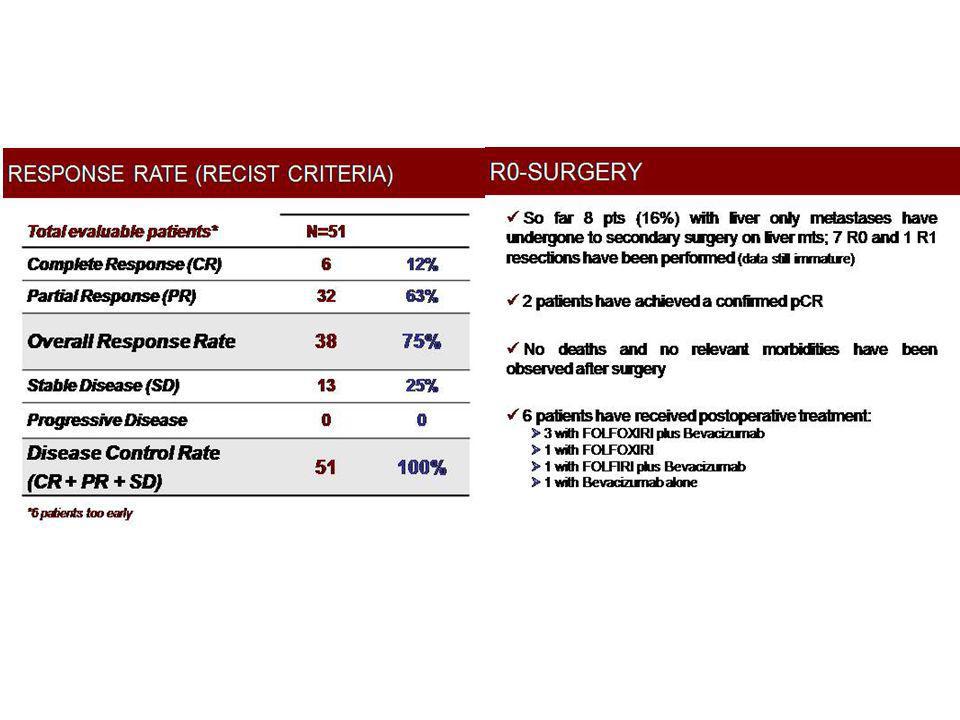
POCHER RESULTS Response rate Resection (R0) Follow-up (median)
(%) Response rate Resection (R0) Follow-up (median) Median PFS (months) resected Median PFS (months) not resected Median OS (months) all population 34 26 22 (1-43) 15 (CI95% ) 9 (CI95% 1-17) 37(CI95% 21-53) 79 (CI95% ) 60 (CI95% )
 Response rate. Resection (R0) Follow-up (median) Median PFS (months) resected. Median PFS (months) not resected. Median OS (months) all population (1-43) 15 (CI95% ) 9 (CI95% 1-17) 37(CI95% 21-53) 79 (CI95% ) 60 (CI95% )")
45
Bevacizumab + CAPOX ORR = 78% BEV ACIZUMAB+ Capecitabine
+ L-OHP: ORR = 78% Patient with colorectal liver metastases± primary tumor Surgery: Resection rate 40%in pts with metachronous mets - Reasection rate 67% in pts with synchronous mets Wong R et al, Ann oncol 2011 ESMO 2006

50
Bevacizumab in synchronous metastases
In patients with asimptomatic primary tumour and synchronous metastases, Bevacizumab (plus FOLFOX6) can be used without increased risks of bleeding/perforation (McCahill et al, ASCO 2010 abs 3527) In neoadjuvant setting of liver metastases, Bevacizumab (plus Xelox) can be used safely without increased risks and with efficacy also in patients with primary insitu (Gruenberger T et al, ASCO 2010 abs e14032)
 can be used without increased risks of bleeding/perforation (McCahill et al, ASCO 2010 abs 3527) In neoadjuvant setting of liver metastases, Bevacizumab (plus Xelox) can be used safely without increased risks and with efficacy also in patients with primary insitu (Gruenberger T et al, ASCO 2010 abs e14032)")
51
Anti EGFRab in synchronous metastases
Safe use of Cetuximab or Panitumumab in advanced CRC No data are reported in the principal studies (Crystal, Opus) respect an increased toxicity/morbidity/mortality during treatment of patients with primary tumor insitu
 respect an increased toxicity/morbidity/mortality during treatment of patients with primary tumor insitu.")
52
Chemioterapia intra-arteriosa (IA) epatica I
Risposte 40-80%; resecabilità variabile dal 10 al 40%, tuttavia le esperienze in neoadiuvante con la terapia IA epatica sono limitate E’ possibile utilizzare alternativamente la chemioterapia sistemica e intra-arteriosa epatica o in combinazione (eventualmente con nuovi farmaci) Non è comunque possibile definire l’approccio ottimale per la difficoltà a comparare studi di chemioterapia neoadiuvante sistemica e intra-arteriosa epatica (eterogeneità): necessità di studi randomizzati
 Non è comunque possibile definire l’approccio ottimale per la difficoltà a comparare studi di chemioterapia neoadiuvante sistemica e intra-arteriosa epatica (eterogeneità): necessità di studi randomizzati.")
53
Terapia sistemica + Terapia Locoregionale
Pazienti: 44 pre-CPT-11 ev: 70% HAI+ SYS OXAL –5-FAFU RR: 82% Resect: 20-36% Leonard GD, et al. ASCO ’04 abs 3542

54
LIVER DAMAGE

55
Quale è il danno sul fegato “sano”?
Fibrosi (portale, porto-portale, settale, cirrosi) Lesioni vascolari (dilatazione e congestione sinusoidale, peliosi, necrosi emorragica centrolobulare, iperplasia nodulare rigenerativa Steatosi macrovacuolare (lieve <30% epatociti, moderata 30-60% epatociti e severa >60% epatociti) Oxaliplatino= danno vascolare CPT-11= steatoepatite
 Lesioni vascolari (dilatazione e congestione sinusoidale, peliosi, necrosi emorragica centrolobulare, iperplasia nodulare rigenerativa. Steatosi macrovacuolare (lieve <30% epatociti, moderata 30-60% epatociti e severa >60% epatociti) Oxaliplatino= danno vascolare. CPT-11= steatoepatite.")
56
Vascular hepatic damage
Aloia T et al., JCO 2006

57
Complete response to chemotherapy
Benoist S, JCO 2006

58
CONCLUSIONS Actually there are not guideline on the use of chemotherapy and surgery in synchronous colorecltal liver metastases (clinical signs are important) There is not a chemotherapy schedule indicated as standard treatment in neoadjuvant setting of colorectal liver metastases: all schedules could be used Triplet seems to be more effective Adding molecular drugs, there is an activity increase in term of response rate and resectability Prospective studies on predictive factors of response and resectability could be useful to select the better treatment for each patient
 There is not a chemotherapy schedule indicated as standard treatment in neoadjuvant setting of colorectal liver metastases: all schedules could be used. Triplet seems to be more effective. Adding molecular drugs, there is an activity increase in term of response rate and resectability. Prospective studies on predictive factors of response and resectability could be useful to select the better treatment for each patient.")
59
KL, nata in Ucraina il , Anam Fam: negativa Anam. Fisiol: 3 gravidanze Anam Patol Remota: negativa Osservata il , da 4 mesi tenesmo ed astenia. Rettoscopia: sulla superficie laterale del retto neoplasia a 3 cm da OA, occupando il 50% del lume e si estende per 7 cm in lunghezza TC ( ): Tumore del retto con met epatiche bilaterali massive e polmonari
: Tumore del retto con met epatiche bilaterali massive e polmonari.")
60
KL TC pre terapia:

61
KL TC pre terapia:

62
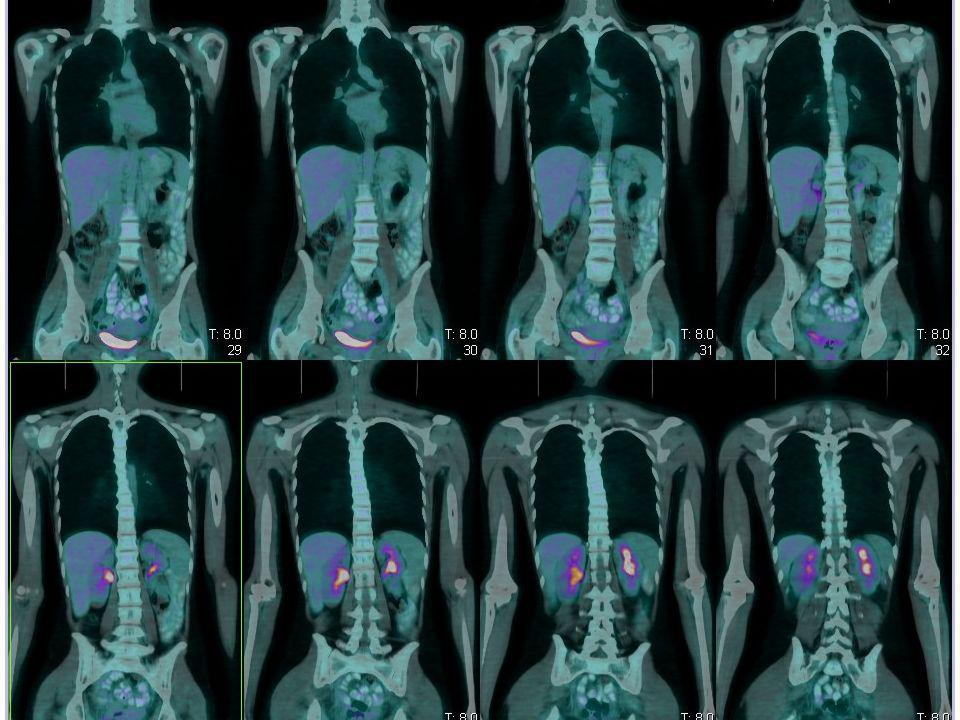
KL PET/TC pre terapia:

63
Neoplasia del retto con metastasi epatiche : KL n. 17.4.1972
: Inizia chrono-IFLO + Cetuximab per 4 cicli (2 mesi) : RP >80% su T ed M Cetuximab mg/m2 day1 CPT mg/m2day 1 peak 13:00 C. Garufi et al Br J Cancer 2010
 : RP >80% su T ed M. Cetuximab mg/m2 day1. CPT mg/m2day 1. peak 13:00. C. Garufi et al Br J Cancer")
64
Ecoendo: 11.11.2010 risposta dopo 4 cicli di chrono-IFLO

65
TC: 23.11.2010 risposta dopo 4 cicli di chrono-IFLO

66
Neoplasia del retto con metastasi epatiche : KL n 17.4.1972
Dal al RT 25 Gy “short course” sul retto Resezione del retto in VLS con anastomosi colo anale ed ileostomia di protezione ypT3N1a, TRG 1 sec Ryan

67
Neoplasia del retto con metastasi epatiche : KL n 17.4.1972
Esame istologico: “ … tratto di grosso intestino sede di residui di adenocarcinoma rappresentati da occasionali aggregati cellulari neoplastici nel contesto di alcuni laghi di muco infiltranti il tessuto fibroso perirettale ed il margine radiale (circonferenziale) di resezione chirurgica. La neoplasia si associa a marcata fibrosi e focali calcificazioni, Si segnala angioinvasione dei vasi extramurali e modificazioni riferibili a terapia neoadiuvante. … Metastasi in 1/8 linfonodi perirettali repertati, mentre i restanti 7 mostrano modificazioni riferibili a terapia neoadiuvante. Residui neoplastici in2/7 noduli fibrosi repertati nel tessuto fibroadiposo perirettale, mentre i rimanenti 5 noduli mostrano fibrosi, occasionali calcificazioni e modificazioni riferibili a terapia neoadiuvante. Margine prossimale indenne da infiltrazione neoplastica”
 di resezione chirurgica. La neoplasia si associa a marcata fibrosi e focali calcificazioni, Si segnala angioinvasione dei vasi extramurali e modificazioni riferibili a terapia neoadiuvante. … Metastasi in 1/8 linfonodi perirettali repertati, mentre i restanti 7 mostrano modificazioni riferibili a terapia neoadiuvante. Residui neoplastici in2/7 noduli fibrosi repertati nel tessuto fibroadiposo perirettale, mentre i rimanenti 5 noduli mostrano fibrosi, occasionali calcificazioni e modificazioni riferibili a terapia neoadiuvante. Margine prossimale indenne da infiltrazione neoplastica")
68
Neoplasia del retto con metastasi epatiche : KL n 17.4.1972
Dal al continua ancora per 3 cicli con chrono-IFLO (7 cicli totale) chiusura colostomia PET: RC fegato
 chiusura colostomia PET: RC fegato.")
70
Neoplasia del retto con metastasi epatiche : KL n 17.4.1972
epatectomia dx allargata al IV segmento + resezione met epatica a sinistra FOLFIRI + Cetuximab x 6 cicli conclude chemioterapia

71
Neoplasia del retto con metastasi epatiche : KL n 17.4.1972
Esame istologico: 1. Lobo destro : al taglio nel parenchima epatico si apprezzano tre neoformazioni …. Del diametro rispettivamente di cm 1,5 A,B; di cm 1,8 C,D; di cm 2,7 E,F. Non alterazioni nel parenchima circostante G,H “Fegato sede di metastasi di adenocarcinoma moderat differenziato, coerente con primitività colica. I noduli metastatici sono costituiti solo in parte minore da tessuto neoplastico vitale (circa il 30% in A,B; circa il 10% in C,D; circa il 40% in E,F) prevalendo in tutti la necrosi el’organizzazione sclero-cicatriziale di questa. Margine chirugico libero da neoplasia. Non modificazioni di rilevo del parenchima non lesionale.” 2. Formazione lobo sinistro “ frammento di parenchima epatico sede di metastasi di adenocarcinoma con aspetti morfologici sovrapponibili, in parziale (circa il 50%) sostitutuzione sclero-calcifica”
 prevalendo in tutti la necrosi el’organizzazione sclero-cicatriziale di questa. Margine chirugico libero da neoplasia. Non modificazioni di rilevo del parenchima non lesionale. 2. Formazione lobo sinistro. frammento di parenchima epatico sede di metastasi di adenocarcinoma con aspetti morfologici sovrapponibili, in parziale (circa il 50%) sostitutuzione sclero-calcifica")
72
KL, nata in Ucraina il TC

73
Neoplasia del retto con metastasi epatiche : KL n 17.4.1972
Conclusione 14 mesi di trattamenti integrati 13 cicli di chemioterapia, 7 chrono-IFLO + 4 FOLFIRI, sempre con Cetuximab 5 sedute di RT 3 interventi chirurgici: resezione colo-anale, chiusura colostomia, epatectomia allargata al IV Paziente senza segni di malattia ad oggi