Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
HOT TOPICS IN BREAST CANCER Chieti, 11 Novembre 2009
OLD AND NEW ANTHRACYCLINES: a still valid option in breast cancer treatment A. Nuzzo U.O. di Oncologia Medica Ospedale Renzetti di Lanciano A. Nuzzo U.O. di Oncologia Medica ASL Lanciano-Vasto

2
che è stato isolato da Federico Arcamone nei laboratori di Farmitalia.
“Agosto Ho terminato di visitare i pazienti ricoverati e sto rientrando nel mio studio dove mi attende Aurelio Di Marco per illustrarmi le caratteristiche di un nuovo farmaco antitumorale che è stato isolato da Federico Arcamone nei laboratori di Farmitalia. Si chiama Adriamicina……”. Bonadonna G, Sursum corda. In: “Dall’altra parte” Ed. Rizzoli, 2006

3
EBCTCG Meta-analysis 2005-06 Breast cancer mortality
Taxanes > Anthra. > CMF > No Chemo. 50 10-y gain 4.3% (SE 1.0) Lorank 2p < 10-y gain 4.3% (SE 1.0) Lorank 2p < 10-y gain 5.1% (SE 1.6) Lorank 2p < Control 36.4% 40 CMF 31.3% Anthr. 31.0% 30 CMF 32.2% 20.5 19.9 20 Anthr. 27.0% Anche la CT-adiuvante contenente taxani, rispetto a quella contenete antracicline determina un vantaggio di OS a 10 anni del 5,1% 15.3 % + SE 17.8 Taxane 25.9% 16.5 10 12.8 Years Years Years 5 10 5 10 5 10 Death rates (% / year: total – rate in women without recurrence) & logrank analyses Peto R on behalf of the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Presented at SABCS 2007, December 13, San Antonio, TX.
 Lorank 2p < y gain 4.3% (SE 1.0) Lorank 2p < y gain 5.1% (SE 1.6) Lorank 2p < Control 36.4% 40. CMF 31.3% Anthr. 31.0% 30. CMF 32.2% Anthr. 27.0% Anche la CT-adiuvante contenente taxani, rispetto a quella contenete antracicline determina un vantaggio di OS a 10 anni del 5,1% % + SE Taxane 25.9% Years. Years. Years Death rates (% / year: total – rate in women without recurrence) & logrank analyses. Peto R on behalf of the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Presented at SABCS 2007, December 13, San Antonio, TX.")
4
a still valid option in breast cancer treatment? FALSE !!

5
Anthracyclines and Early Breast Cancer: The End of an Era. L
Anthracyclines and Early Breast Cancer: The End of an Era? L. Gianni, Journal of Clinical Oncology 2009 Anthracyclines are a mainstay of adjuvant therapy for breast cancer patients worldwide, but some research data suggest that not all patients benefit. Some of the latest studies suggest that a large majority of patients (70%–80%) might not benefit, Early Breast Cancer can be treated with less toxic but equivalent regimens.
 might not benefit, Early Breast Cancer can be treated with less toxic but equivalent regimens.")
6
Le antracicline sono farmaci tossici ?
leucemogene cardiotossiche

7
FEC intensive CMF per os DFS (§) 52% 45% OS 62% 58%
Randomized trial of intensive cyclophosphamide, epirubicin and fluorouracil chemotherapy compared to cyclophosphamide, emethotrexate and fluorouracil in premenopausal women with node-positive breast cancer. NCI of Canada Clinical Trials Group 710 donne in premenopausa, pN+ FEC (5FU 600 mg/mq 1° e 8° + EPI 60 mg/mq 1° e 8°, EDX per os 75 mg/mq 1°-14° ) vs CMF classico FU mediano 10 anni FEC intensive CMF per os DFS (§) 52% 45% OS 62% 58% (§) significativo Levine MN et al: J Clin Oncol 1998
 vs CMF classico. FU mediano 10 anni. FEC intensive. CMF per os. DFS (§) 52% 45% OS. 62% 58% (§) significativo. Levine MN et al: J Clin Oncol")
8
Risk of Acute Leukemia Following Epirubicin-Based Adjuvant Chemotherapy: A Report From the National Cancer Institute of Canada Clinical Trials Group M. Crump et al., J Clinical Oncology 2003

9
CARDIOTOSSICITA’ DA ANTRACICLINE: UN PROBLEMA CLINICO EMERGENTE
Più lunga sopravvivenza dei pazienti La potenziale guarigione di molti pazienti trattati con antracicline (neoplasie ematologiche, terapia adiuvante del ca. mammario, neoplasie pediatriche) Acquisizione di dati a lungo termine
 Acquisizione di dati a lungo termine.")
10
CARDIOTOSSICITA’: TIPO I e II
TIPO II FARMACO DOXORUBICINA TRASTUZUMAB DOSE CORRELATA SI NO MECCANISMO STRESS OSSIDATIVO INIBIZIONE HER-2 DANNO ULTRASTRUTTURA PRESENTE ASSENTE REVERSIBILITA’ RECHALLENGE POSSIBILE Ewer MS. JCO 2005;23:

11
“…Anthracycline cardiomyopathy is characterized by a dose-dependent progressive decrease in systolic left ventricular function often resulting in CHF. In the adult survivor, it is clinically indistinguishable from CHF due to other causes…” Journal of Clinical Oncology, Vol 25, No 25 (September 1), 2007: pp
, 2007: pp")
12
Tossicità cardiaca doxorubicina vs epirubicina
FEC x 3- Doce TAC x 6 Dose Ratio 1:1.7 AC-Tax AC x 4 mentre l’epirubicina rappresenta un analogo della doxorubicina ad efficacia equivalente presenta un rapporto di cardiotossicità equivalente rispetto alla doxorubicina per dosaggi cumulativi di 1,7:1 Mouridsen, Acta Onc ’90: 29;

13
CARDIOTOSSICITA’ TARDIVA DA DOXORUBICINA
CMF (363 pt) 1000 pts (3 studi di CT adj) CMF + doxorubicina (637: 300 mg/mq) CHF nel 0,6% tutte trattate con doxo: 1% Follow up mediano = 14 aa : mortalità per cardiopatia 0,4% 355 paz libere da malattia a 11 aa: alterazioni ECG = 23% alterazioni ecocardio = 34% < LVEF 8% in doxo vs 2% p=.032 Zambetti M et al, JCO 2001;19,37-43
 1000 pts. (3 studi di CT adj) CMF + doxorubicina (637: 300 mg/mq) CHF nel 0,6% tutte trattate con doxo: 1% Follow up mediano = 14 aa : mortalità per cardiopatia 0,4% 355 paz libere da malattia a 11 aa: alterazioni ECG = 23% alterazioni ecocardio = 34% < LVEF 8% in doxo vs 2% p=.032. Zambetti M et al, JCO 2001;19,")
14
Survival According to the Underlying Cause of Cardiomyopathy
1.00 Peripartum 0.75 Idiopathic Due to doxorubicin therapy Proportion of Patients Surviving 0.50 Due to ischemic heart disease Due to infiltrative myocardial disease 0.25 Due to HIV infection 0.00 5 10 15 Years Felker GM et al. N Engl J Med 2000;342:

15
Doxorubicine liposomaili disponibili
Non-pegylated liposomal doxorubicin (MYOCET) Pegylated liposomal doxorubicin (CAELYX) Doxorubicine-ammonium sulfate gel-like precipitate Liposomal membrane: soy HPC/DSPE/cholesterol Polyethylene glycol surface Diameter: 80 nm Doxorubicine-citrate linear polimer Liposomal membrane: egg PC/cholesterol Diameter: 150 nm
 Pegylated liposomal doxorubicin (CAELYX) Doxorubicine-ammonium sulfate gel-like precipitate. Liposomal membrane: soy HPC/DSPE/cholesterol. Polyethylene glycol surface. Diameter: 80 nm. Doxorubicine-citrate linear polimer. Liposomal membrane: egg PC/cholesterol. Diameter: 150 nm.")
16
van Dalen EC, Michiels EM, Caron HN, Kremer LC
van Dalen EC, Michiels EM, Caron HN, Kremer LC. Different anthracycline derivates for reducing cardiotoxicity in cancer patients. Cochrane Database Syst Rev Oct 18;(4):
:")
17
van Dalen EC, Michiels EM, Caron HN, Kremer LC
van Dalen EC, Michiels EM, Caron HN, Kremer LC. Different anthracycline derivates for reducing cardiotoxicity in cancer patients. Cochrane Database Syst Rev Oct 18;(4):
:")
18
van Dalen EC, Michiels EM, Caron HN, Kremer LC
van Dalen EC, Michiels EM, Caron HN, Kremer LC. Different anthracycline derivates for reducing cardiotoxicity in cancer patients. Cochrane Database Syst Rev Oct 18;(4):
:")
19
Meta-analisi degli studi di fase III Confronto tra Antracicline rispetto alla Cardiotossicità
Van Dalen et al. Cochrane Database Syst Rev Oct 18;(4):
:")
20
The Cochrane review “Based on the currently available evidence on heart failure, we conclude that in adults with a solid tumour liposomal-encapsulated doxorubicin should be favoured over doxorubicin.” “Until more evidence becomes available on tumour response and survival in patients treated with liposomal-encapsulated doxorubicin or doxorubicin in equimolar doses, we recommend the use of a higher cumulative liposomal-encapsulated doxorubicin dose as compared to the standard cumulative doxorubicin dose Van Dalen EC et al. The Cochrane Library 2006, Issue 4

21
Quante zampe ha questo elefante?
Fattori predittivi ?

22
Fattori predittivi Terapia efficace Fattori predittivi ?
Riduzione complessiva del 20% del rischio di recidiva Fattori predittivi ? Riduzione del 100% del rischio di recidiva Riduzione dello 0% del rischio di recidiva

23
The effect of genetic variability on drug response in conventional breast cancer treatment. Wiechec E, Hansen LL. Eur J Pharmacol Oct 18.

24
Prognosi molecolare MammaPrint® Oncotype DX ……….

25
Criteri di selezione ETA’ COMORBIDITA’ LVEF HER-2 Topoisomerasi IIα chromosome 17 polysomy (Bartlett et al, SABCS 2008)
 .")
26
DOSE CUMULATIVA E RISCHIO DI SCOMPENSO NEI PAZIENTI ANZIANI
Swain et al. Cancer. 2003: 97,

27
Identifying Breast Cancer Patients Who Won't Respond to Anthracyclines
TOPOISOMERASI II alfa Top II a Fig. 15 depliant Proteina di 170 kdalton Posizione 17 q 21-22 Riparazione DNA tramite legame covalente

28
AMPLIFICAZIONE DELLA TOP II α NEL CARCINOMA MAMMARIO
Co-amplificazione TOP II α / HER-2 35% delle pz con HER-2 amplificato (Slamon D, SABCS 2006) 37% delle pz con HER-2 amplificato (Tanner M, JCO 2006) Amplificazione TOP 2 II α / HER-2 non amplificato 1,7 – 10,3% (Knoop AS, JCO 2005)
 37% delle pz con HER-2 amplificato. (Tanner M, JCO 2006) Amplificazione TOP 2 II α / HER-2 non amplificato. 1,7 – 10,3% (Knoop AS, JCO 2005)")
29
Amplificazione TOP II α
Come fattore predittivo di risposta alle antracicline nel carcinoma della mammella Dal 2002, almeno 6 studi pubblicati hanno dimostrato l’associazione tra amplificazione TOP 2A e miglior outcome Slamon D, Brest Cancles Treat pz Adiuvante Tanner M, JCO pz Adiuvante Knoop AS, JCO pz Adiuvante Park K, EJC pz Neoadiuvante Coon JC, Clin Canc Res pz Neoadiuvante Di Leo A, Clin Canc Res pz Adiuvante Slamon D, SABCS Modificata

30
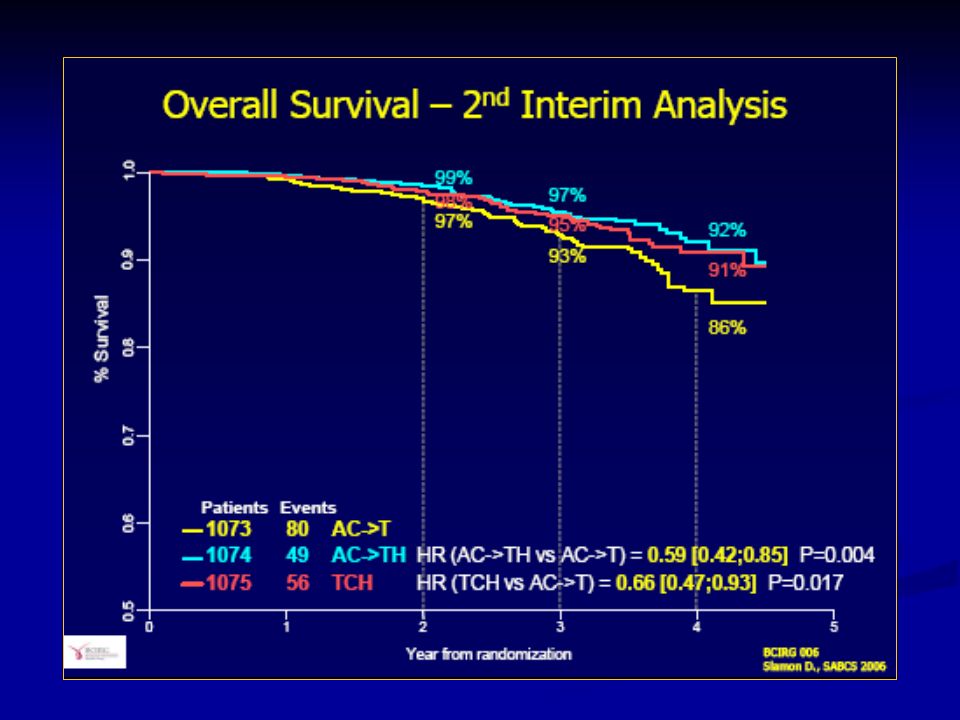
HER2 e antracicline Overall Survival
HER2 positive HER2 negative HER2 e antracicline Overall Survival Study HR 95% CI anthra better non anthra better NSABP B11 0.66 0.90 NSABP B15 0.82 1.07 GUN 3 0.85 1.64 Milan 0.61 1.26 DBCG-89-D 0.73 0.82 NCIC MA-5 0.65 1.06 Total 0.91 p = 0.056 p < Overall 0.73 1.03 p = 0.86 heterogeneity c25 = 5.2, p = 0.39 heterogeneity c25 = 5.5, p = 0.36 0.4 0.6 0.9 1 2 5 Test for interaction chi2 = 12.0, p < 0.001 A. Gennari SABCS 2006

31
The role of topoisomerase II alpha and HER-2 in predicting sensitivity to anthracyclines in breast cancer patients. Oakman C, Moretti E, Galardi F, Santarpia L, Di Leo A In the search for predictive biomarkers to refine clinical prescription of cytotoxic agents, both HER-2 and topo IIα are under exploration for their potential role in identifying individuals with early breast cancer who may benefit from anthracycline therapy. Whilst recent meta-analyses support a predictive role for HER-2 amplification, it remains unclear whether HER-2 is the critical biomarker or whether it is a surrogate marker for topo IIα alteration, a known drug target of anthracyclines. The major limitation in considering HER-2 as a single marker is heterogeneity within the subgroups of HER-2 positive and HER-2 negative disease. Cancer Treat Rev Sep 14.

32
The role of topoisomerase II alpha and HER-2 in predicting sensitivity to anthracyclines in breast cancer patients. Oakman C, Moretti E, Galardi F, Santarpia L, Di Leo A. For topo IIα, current data is inconclusive. Issues plaguing this field are technical variability in marker definition, complex regulation pathway of topo IIα and lack of prospective, adequately powered studies. With current evidence, neither HER-2 nor topo IIα gene status can be considered clinically valuable markers for anthracycline benefit. Cancer Treat Rev Sep 14.

33
factors associated with responsiveness to the anthracycline-containing regimen
amplification of the human epidermal growth-factor receptor type 2 (HER2) gene (K. Pritchard et al, N Engl J Med. 2006). alterations in the topoisomerase II alpha (TOP II α ) gene (K. Pritchard et al, JNCI 2009) “I do not use any of these data to guide my own treatment decision-making “ K. Pritchard
 gene (K. Pritchard et al, N Engl J Med. 2006). alterations in the topoisomerase II alpha (TOP II α ) gene (K. Pritchard et al, JNCI 2009) I do not use any of these data to guide my own treatment decision-making K. Pritchard.")
34
uomo barbuto o donna nuda ?
Abbiamo alternative migliori delle antracicline ?

36
Disease-free survival (DFS) and overall survival (OS) (A) DFS by treatment; (B) DFS by treatment and age; (C) OS by treatment: 1 day; (D) OS by treatment and age Jones, S. et al. J Clin Oncol; 27:

37
Summary of unplanned, exploratory analyses of disease-free survival hazard ratios (HR) and CI
Jones, S. et al. J Clin Oncol; 27:

42
Summing-up Anthracyclines remain a mainstay of EBC and ABC treatment
Cardiovascular and leukemogen risk however is not trivial and should not be overlooked Data suggest that only some subgroups may derive specific benefits from anthracyclines (although not conclusive) Available non-anthra-based regimens may help us manage uncertainty while further data accumulate M. de Laurentis, XII AIOM Milano 2009
 Available non-anthra-based regimens may help us manage uncertainty while further data accumulate. M. de Laurentis, XII AIOM Milano")
43
Clodoveo Masciarelli grazie

Presentazioni simili
















>")





