Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Paziente medico e chirurgico: schemi di trattamento
Walter Ageno Dipartimento di Medicina Clinica Università dell’Insubria - Varese

3
Main clinical trials in medical patients
MEDENOX (enoxaparin) age ≥ 40 years, hospitalization ≥ 6 days and CHF (NYHA III/IV) Acute resp. disease Infectious disease, acute rheumatic and IBD + 1 predefined RF * PREVENT (dalteparin) age ≥ 40 years, hospitalization ≥ 6 days and CHF (NYHA III/IV) Acute resp. disease Infectious disease, acute rheumatic and IBD + 1 predefined RF * ARTEMIS (fondaparinux) age ≥ 60 years, hospitalization ≥6 days and CHF (NYHA III/IV) Acute and chronic resp. disease Acute infectious or inflammatory disease No additional RF age> 75 years, cancer, VTE history, obesity, varicose veins, oral contraceptives, chronic heart failure, chronic respiratory failure
 age ≥ 40 years, hospitalization ≥ 6 days. and. CHF (NYHA III/IV) Acute resp. disease. Infectious disease, acute rheumatic and IBD. + 1 predefined RF * PREVENT. (dalteparin) age ≥ 40 years, hospitalization ≥ 6 days. and. CHF (NYHA III/IV) Acute resp. disease. Infectious disease, acute rheumatic and IBD. + 1 predefined RF * ARTEMIS. (fondaparinux) age ≥ 60 years, hospitalization ≥6 days. and. CHF (NYHA III/IV) Acute and chronic resp. disease. Acute infectious or inflammatory disease. No additional RF. age> 75 years, cancer, VTE history, obesity, varicose veins, oral contraceptives, chronic heart failure, chronic respiratory failure.")
4
NINE SELECTED STUDIES → 19,958 PATIENTS
Thromboprophylaxis in medical patients: meta-analysis on treatment period NINE SELECTED STUDIES → 19,958 PATIENTS PE RR = 0.43; 95% CI: Fatal PE RR = 0.38; 95% CI: Symptomatic DVT RR = 0.47; 95% CI: Mortality RR = 0.97; 95% CI: Major bleeding RR = 1.32; 95% CI: Dentali F et al. Ann Intern Med 2007; 146:

6
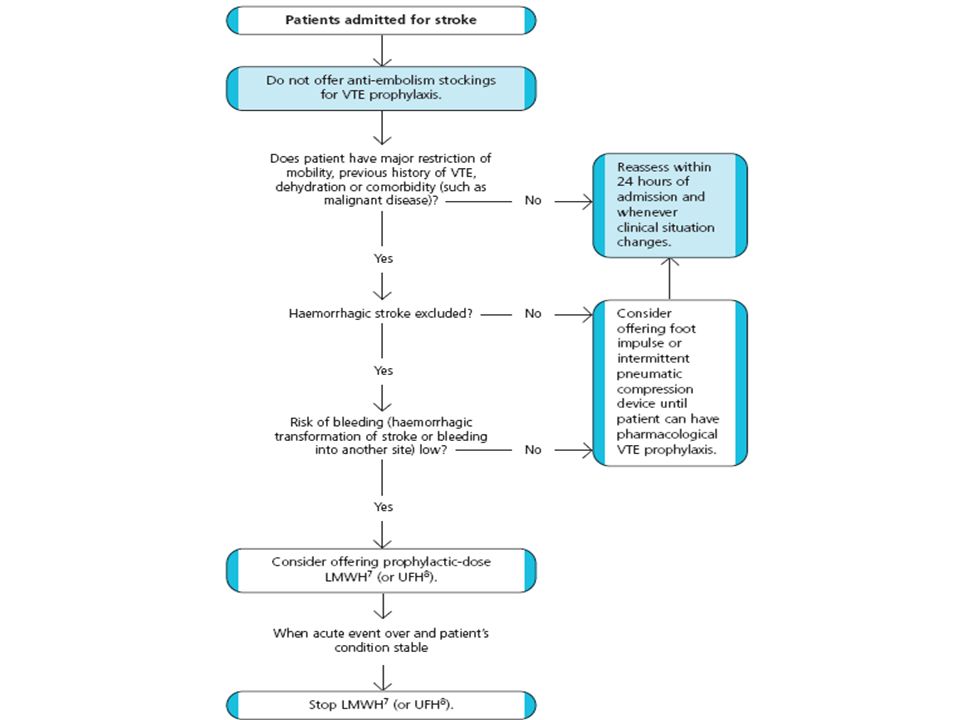
Linee guida SPREAD 2010: stroke ischemico
Grado B: In pazienti a rischio elevato (pazienti plegici, con alterazione dello stato di coscienza, obesi, con pregressa patologia venosa agli arti inferiori) è indicato l’uso di eparina calcica non frazionata 5000 UI x 2 o eparina a basso peso molecolare In pazienti non a rischio elevato di trombosi venose profonde, il ricorso sistematico all’eparina comporta un bilancio beneficio/rischio di complicanze emorragiche intracerebrali e/o sistemiche inaccettabile
 è indicato l’uso di eparina calcica non frazionata 5000 UI x 2 o eparina a basso peso molecolare. In pazienti non a rischio elevato di trombosi venose profonde, il ricorso sistematico all’eparina comporta un bilancio beneficio/rischio di complicanze emorragiche intracerebrali e/o sistemiche inaccettabile.")
7
GCS NO 11.5% 11.7% Skin breaks/ulcers/blisters/skin necrosis 64 (5.1%) - 16 (1.3%) OR 4.18 (2.40–7.27)
 - 16 (1.3%) OR 4.18 (2.40–7.27) .")
9
Pharmacological prevention of thrombosis in surgical patients
Efficacy of low-dose unfractionated heparin (UFH) in prevention of DVT after major surgery s.c. low-dose UFH pre-operative and b.i.d.post-operative 78 ‘high-risk’ patients Patients with DVT (%) p < 0.001 42 8 Kakkar VV et al. Lancet 1972;2:101-6.
 in prevention of DVT after major surgery. s.c. low-dose UFH pre-operative and b.i.d.post-operative. 78 ‘high-risk’ patients. Patients with DVT (%) p < Kakkar VV et al. Lancet 1972;2:")
10
LMWH for the prevention of VTE in general surgery
LMWH vs. no treatment or placebo (8 studies, 5520 patients) RR [CI 95%] DVT (n=513) [0.14–0.54] Clinical PE (n=5456) [0.08–0.79] Clinical VTE (n=4890) [0.11–0.73] Major bleeding (n=5456) [1.37–3.01] Death (n=5142 ) [0.27–1.10] Relative risk 0.5 1 2 3 LMWH better Placebo/No treatment better Mismetti P et al. Br J Surg 2001;88:
 RR [CI 95%] DVT (n=513) 0.28 [0.14–0.54] Clinical PE (n=5456) 0.25 [0.08–0.79] Clinical VTE (n=4890) 0.29 [0.11–0.73] Major bleeding (n=5456) 2.03 [1.37–3.01] Death (n=5142 ) 0.54 [0.27–1.10] Relative risk LMWH better. Placebo/No treatment better. Mismetti P et al. Br J Surg 2001;88:")
11
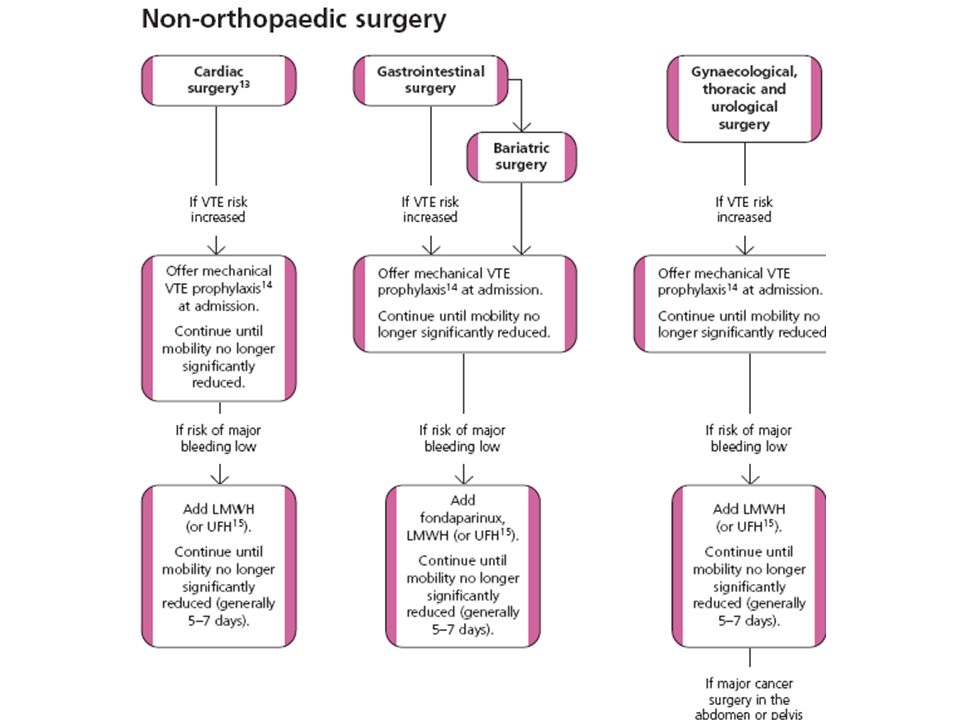
Guidelines: Prophylaxis of VTE in surgical patients
For moderate-risk general surgery patients who are undergoing a major procedure for benign disease, we recommend thromboprophylaxis with LMWH, LDUH, or fondaparinux (each Grade 1A). For higher-risk general surgery patients who are undergoing a major procedure for cancer, we recommend thromboprophylaxis with LMWH, LDUH three times a day, or Fondaparinux (each Grade 1A)1 Setting No risk factors Risk factors General Mechanical Mechanical surgery + LMWH or fondaparinux NICE guidelines UK Geerts WH et al. Chest 2008 Hill J et al BMJ 2007
. For higher-risk general surgery patients who. are undergoing a major procedure for cancer, we recommend thromboprophylaxis with. LMWH, LDUH three times a day, or. Fondaparinux (each Grade 1A)1. Setting No risk factors Risk factors. General Mechanical Mechanical. surgery + LMWH or fondaparinux. NICE guidelines. UK. Geerts WH et al. Chest Hill J et al BMJ")
13
Extended prophylaxis with LMWH after cancer surgery
Incidence of Total DVT* Incidence of VTE** p=0.012 p=0.02 16.3% 12.0% 10 Total DVT (%) VTE (%) 7.3% 4.8% 5 1 week 4 weeks 1 week 4 weeks ENOXACAN II1 FAME 2 Enoxaparin: n=165 Dalteparin: n=343 60% cancer surgery in 1 week group 56% cancer surgery in 4 weeks group *Deep Vein Thrombosis ** Venous Thromboembolism Berqvist D et al. New Engl J Med 2002;346: Rasmussen MS et al. J Thromb Haemost 2006;4:
 VTE (%) 7.3% 4.8% 5. 1 week. 4 weeks. 1 week. 4 weeks. ENOXACAN II1. FAME 2. Enoxaparin: n=165. Dalteparin: n= % cancer surgery in 1 week group. 56% cancer surgery in 4 weeks group. *Deep Vein Thrombosis. ** Venous Thromboembolism. Berqvist D et al. New Engl J Med 2002;346: Rasmussen MS et al. J Thromb Haemost 2006;4:")
14
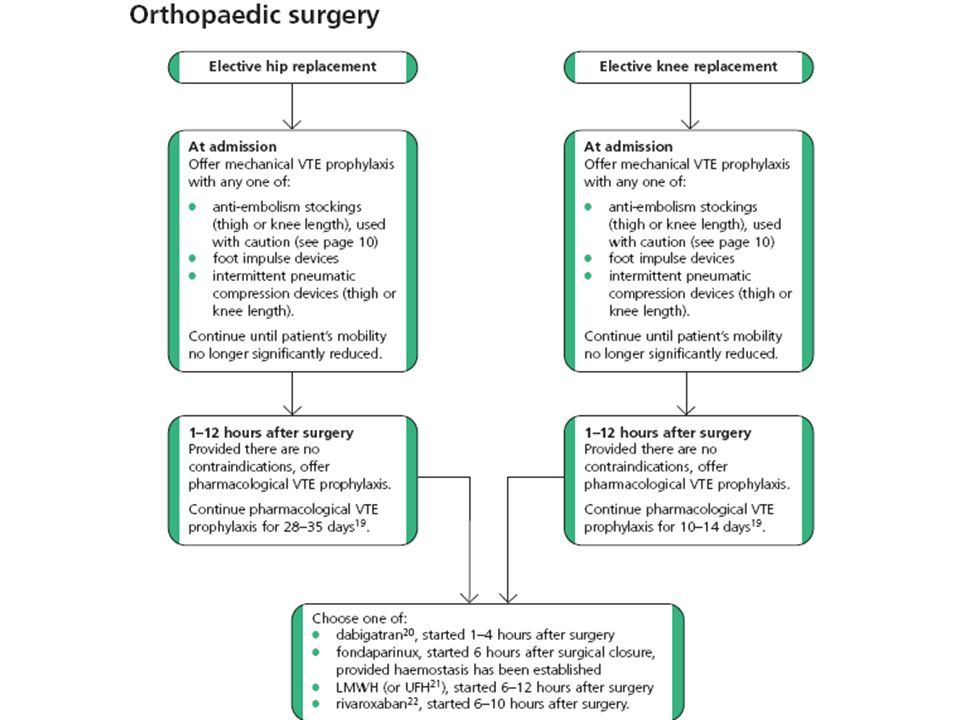
Recommendations: Elective Hip and Knee Replacement
We recommend the routine use of one of the following options: (1) LMWH (at a usual high-risk dose); (2) Fondaparinux (2.5 mg); (3) Adjusted dose VKA started preoperatively or the evening of the surgical day (INR target, 2.5; INR range, 2.0 to 3.0) (all Grade 1A) Geerts et al Chest 2008
 LMWH (at a usual high-risk dose); (2) Fondaparinux (2.5 mg); (3) Adjusted dose VKA started preoperatively or the evening. of the surgical day (INR target, 2.5; INR range, 2.0 to 3.0) (all Grade 1A) Geerts et al Chest")
16
Timing of the first prophylactic dose of LMWH: results of a meta-analysis
14 Studies patients EFFICACY 19.2% (17-21) DVT % 14.4% (12-17) 12.4% (10-14) LMWH 12 h preop LMWH periop. LMWH h post-op Strebel, Arch Int Med, 2002
 DVT % 14.4% (12-17) 12.4% (10-14) LMWH 12 h preop. LMWH periop. LMWH h post-op. Strebel, Arch Int Med,")
17
Timing of Thromboprophylaxis Initiation
For patients receiving LMWH as thromboprophylaxis in major orthopedic surgery, we recommend starting either preoperatively or postoperatively (Grade 1A). For patients receiving fondaparinux as thromboprophylaxis in major orthopedic surgery, we recommend starting either 6 to 8 h after surgery or the next day (Grade 1A). Geerts et al Chest 2008
. For patients receiving fondaparinux as thromboprophylaxis in major orthopedic surgery, we recommend starting either 6 to 8 h after surgery or the next day (Grade 1A). Geerts et al Chest")
18
Extended thromboprophylaxis: rationale
OR HEP C 1.3% % 0.38 Symptomatic VTE JW Eikelboom et al. Lancet 2001

19
Duration of Thromboprophylaxis
For patients undergoing THR, TKR, or HFS, we recommend thromboprophylaxis with one of the recommended options for at least 10 days (Grade 1A). We recommend that thromboprophylaxis be extended beyond 10 days and up to 35 days after surgery (Grade 1A THR, Grade 2B TKR, Grade 1A HFS). The recommended options for extended thromboprophylaxis in THR include LMWH, a VKA, or fondaparinux. Geerts et al Chest 2008
. We recommend that thromboprophylaxis be extended beyond 10 days and up to 35 days after surgery (Grade 1A THR, Grade 2B TKR, Grade 1A HFS). The recommended options for extended thromboprophylaxis in THR include. LMWH, a VKA, or fondaparinux. Geerts et al Chest")
20
Renal Impairment and Anticoagulant Dosing
We recommend that renal function be considered when making decisions about the use and/or the dose of LMWH, fondaparinux, and other antithrombotic drugs that are cleared by the kidneys, particularly in elderly patients, patients with diabetes mellitus, and those at high risk for bleeding (Grade 1A). Depending on the circumstances, we recommend one of the following options in this situation: avoiding the use of an anticoagulant that bioaccumulates in the presence of renal impairment, using a lower dose of the agent, or monitoring the drug level or its anticoagulant effect (Grade 1B). Geerts et al Chest 2008
. Depending on the circumstances, we recommend one of the following options in this situation: avoiding the use of an anticoagulant that bioaccumulates in the presence of renal impairment, using a lower dose of the agent, or monitoring the drug level or its anticoagulant effect (Grade 1B). Geerts et al Chest")
Presentazioni simili














>")




