Scaricare la presentazione
1
Problematiche mediche in UTIC Gestione del paziente settico
IV CONVENTION DELLE UTIC LOMBARDE Problematiche mediche in UTIC Gestione del paziente settico Dr. Alessandro Bozzano U.O.S. U.T.I.C. - Monza Gazzada 8-9 aprile 2011

2
Sepsi : stadi e definizioni
Sede imprecisata30% SEPSI GRAVE SHOCK SETTICO Sepsi SIRS Infezione, etc. Gli studi epidemiologici e clinici sulla sepsi sono stati ostacolati dall'assenza di esatti criteri diagnostici e di precise definizioni che ha reso difficile il confronto dei risultati dei vari studi (Opal, 1998). Anche l'eterogeneità dei soggetti con sepsi ha contribuito a complicare le cose.Si è riscontrato che solo il 60% circa dei casi di sepsi clinicamente documentati si associa ad una infezione microbica confermata (Cohen e Abraham, 1999). Nell'altro 40% dei casi, l'agente responsabile è sconosciuto oppure si ritiene che sia associato ad un trauma o ad una lesione. Inoltre, la gravità della sepsi non è stata correlata con l’esistenza di un'infezione documentata e i soggetti con sepsi e shock settico presentano colture negative in proporzioni equivalenti (Rangel-Frausto e coll., 1995). · I soggetti sono caratterizzati da infezioni in svariate sedi dell'organismo. I dati di un ampio studio multicentrico relativo a 455 pazienti con sepsi (Bernard e coll., 1997) indicano che i polmoni sono la sede più comune dell'infezione (47%), seguita dall'addome (15%) e dalle vie urinarie (10%). Nondimeno, in un numero relativamente vasto di pazienti (fino al 30%) non può essere indicata una sede precisa dell'infezione stessa (Wheeler e Bernard, 1999). D'altro canto, la sepsi ha un decorso imprevedibile: certi soggetti procedono rapidamente verso lo shock settico e altri oscillano attraverso uno spettro di vari gradi di insufficienza d’organo (Rangel-Frausto e coll., 1995). Inoltre, devono ancora essere accettati dei precisi marcatori biologici che potrebbero essere di ausilio per la diagnosi e la classificazione dei soggetti con sepsi. · Nel 1992, un Gruppo di Esperti dell'American College of Chest Physicians (ACCP) e della Society of Critical Care Medicine (SCCM) ha compiuto un primo tentativo per risolvere questi problemi, sostituendo definizioni vaghe e ambigue come setticemia e sindrome settica con tre termini esattamente definiti per la progressione dei segni e sintomi clinici della sepsi: sepsi, sepsi grave e shock settico. E' stata inoltre definita la sindrome della risposta infiammatoria sistemica (SIRS) iniziale che sembra precedere lo sviluppo della sepsi e della sepsi grave(Bone e coll., 1992; Wenzel e coll., 1996). Polmone 45% Addome 15% Decorso imprevedibile Vie urinarie 10% ACCP-Bone e coll. Chest. 1992;101:1644.
. Anche l eterogeneità dei soggetti con sepsi ha contribuito a complicare le cose.Si è riscontrato che solo il 60% circa dei casi di sepsi clinicamente documentati si associa ad una infezione microbica confermata (Cohen e Abraham, 1999). Nell altro 40% dei casi, l agente responsabile è sconosciuto oppure si ritiene che sia associato ad un trauma o ad una lesione. Inoltre, la gravità della sepsi non è stata correlata con l’esistenza di un infezione documentata e i soggetti con sepsi e shock settico presentano colture negative in proporzioni equivalenti (Rangel-Frausto e coll., 1995). · I soggetti sono caratterizzati da infezioni in svariate sedi dell organismo. I dati di un ampio studio multicentrico relativo a 455 pazienti con sepsi (Bernard e coll., 1997) indicano che i polmoni sono la sede più comune dell infezione (47%), seguita dall addome (15%) e dalle vie urinarie (10%). Nondimeno, in un numero relativamente vasto di pazienti (fino al 30%) non può essere indicata una sede precisa dell infezione stessa (Wheeler e Bernard, 1999). D altro canto, la sepsi ha un decorso imprevedibile: certi soggetti procedono rapidamente verso lo shock settico e altri oscillano attraverso uno spettro di vari gradi di insufficienza d’organo (Rangel-Frausto e coll., 1995). Inoltre, devono ancora essere accettati dei precisi marcatori biologici che potrebbero essere di ausilio per la diagnosi e la classificazione dei soggetti con sepsi. · Nel 1992, un Gruppo di Esperti dell American College of Chest Physicians (ACCP) e della Society of Critical Care Medicine (SCCM) ha compiuto un primo tentativo per risolvere questi problemi, sostituendo definizioni vaghe e ambigue come setticemia e sindrome settica con tre termini esattamente definiti per la progressione dei segni e sintomi clinici della sepsi: sepsi, sepsi grave e shock settico. E stata inoltre definita la sindrome della risposta infiammatoria sistemica (SIRS) iniziale che sembra precedere lo sviluppo della sepsi e della sepsi grave(Bone e coll., 1992; Wenzel e coll., 1996). Polmone 45% Addome 15% Decorso imprevedibile. Vie urinarie 10% ACCP-Bone e coll. Chest. 1992;101:1644.")
3
Sepsi : stadi e definizioni
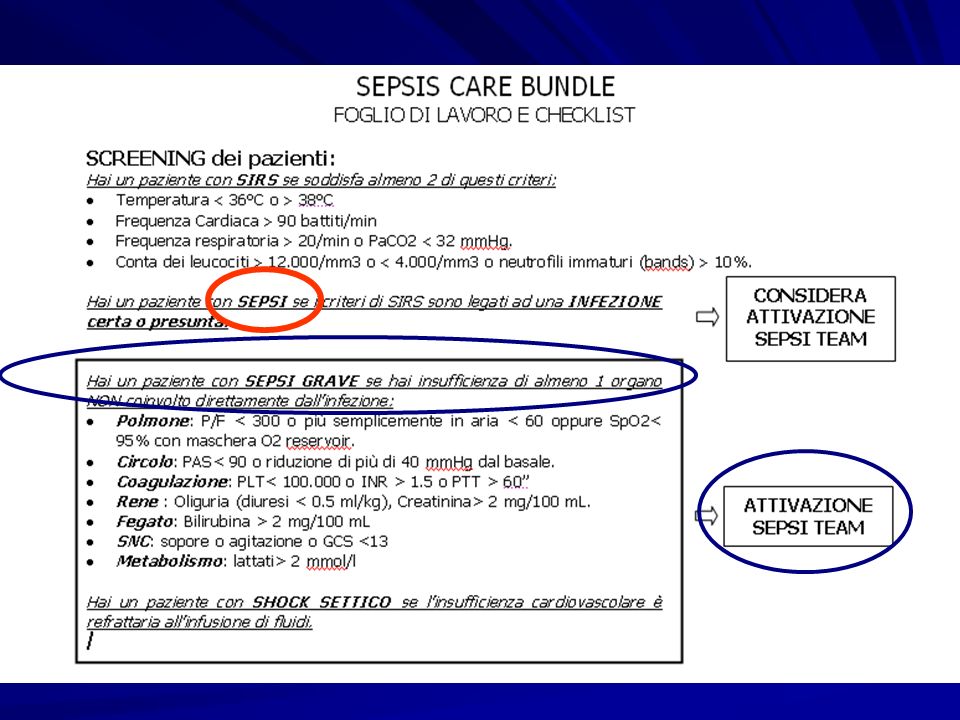
Infezione, etc. SIRS Sepsi Sepsi Grave Risposta clinica a un insulto aspecifico, in assenza di una infezione documentata, comprendente 2 criteri: Temperatura 38oC o 36oC Frequenza Cardiaca 90 battiti/min Frequenza respiratoria 20/min o PaCO2 32 mmHg. Conta dei leucociti /mm3 o 4.000/mm3 o neutrofili immaturi (bands) 10%. Questa struttura gerarchica si basa sull'ipotesi che diverse presentazioni di soggetti con uno stato settico costituiscono una continuità nel progredire della malattia, da meno acuta a più acuta. E' importante notare che queste definizioni non implicano una gravità progressiva dell'infezione, ma esprimono piuttosto un aumento progressivo della "gravità“ della risposta dell'ospite all'infezione (Rangel-Frausto e coll., 1995; Opal e Cohen, 1999). · Come si vede in questa diapositiva, la SIRS corrisponde alla presenza di due o più segni oggettivi di infiammazione sistemica in assenza di un’infezione documentata. Questa definizione va a sostegno delle osservazioni secondo le quali una risposta infiammatoria sistemica può verificarsi a seguito di una varietà di insulti come traumi, ustioni e pancreatite SIRS = sindrome della risposta infiammatoria sistemica Bone e coll. Chest. 1992;101:1644.
 10%. Questa struttura gerarchica si basa sull ipotesi che diverse presentazioni di soggetti con uno stato settico costituiscono una continuità nel progredire della malattia, da meno acuta a più acuta. E importante notare che queste definizioni non implicano una gravità progressiva dell infezione, ma esprimono piuttosto un aumento progressivo della gravità della risposta dell ospite all infezione (Rangel-Frausto e coll., 1995; Opal e Cohen, 1999). · Come si vede in questa diapositiva, la SIRS corrisponde alla presenza di due o più segni oggettivi di infiammazione sistemica in assenza di un’infezione documentata. Questa definizione va a sostegno delle osservazioni secondo le quali una risposta infiammatoria sistemica può verificarsi a seguito di una varietà di insulti come traumi, ustioni e pancreatite. SIRS = sindrome della risposta infiammatoria sistemica. Bone e coll. Chest. 1992;101:1644.")
4
Sepsi : stadi e definizioni
Infezione, etc. SIRS SEPSI Sepsi Grave SIRS con segni di infezione certa o presunta La sepsi è stata quindi definita una patologia in cui è presente la SIRS associata ad un processo infettivo presunto o confermato da colture o visione diretta es rottura di intestino con mat purulento in addome (Bone e coll., 1992).In generale, queste definizioni costituiscono un importante passo avanti verso una maggiore uniformità delle popolazioni di pazienti valutate negli studi clinici. Nondimeno, come è stato sottolineato da un certo numero di ricercatori (Vincent, 1997; Opal, 1998), la definizione della SIRS, in particolare, sembra troppo vaga e priva della specificità necessaria per raggiungere effettivamente l'obiettivo. Ad esempio, nel contesto delle Unità di Terapia Intensiva, in qualsiasi momento fino a 2/3 dei pazienti ricoverati possono soddisfare i criteri per la SIRS. Bone e coll. Chest. 1992;101:1644.
.In generale, queste definizioni costituiscono un importante passo avanti verso una maggiore uniformità delle popolazioni di pazienti valutate negli studi clinici. Nondimeno, come è stato sottolineato da un certo numero di ricercatori (Vincent, 1997; Opal, 1998), la definizione della SIRS, in particolare, sembra troppo vaga e priva della specificità necessaria per raggiungere effettivamente l obiettivo. Ad esempio, nel contesto delle Unità di Terapia Intensiva, in qualsiasi momento fino a 2/3 dei pazienti ricoverati possono soddisfare i criteri per la SIRS. Bone e coll. Chest. 1992;101:1644.")
5
Sepsi : stadi e definizioni
SEPSI GRAVE SHOCK SETTICO Infezione, etc. SIRS Sepsi Sepsi con insufficienza di > 1 organo non coinvolto direttamente dall’infezione Polmone: PaO2/FiO2 < 300 o PaO2 in aria < 60 o SpO2< 95% in O2 reservoir Circolo: PAS< 90 o ▼> 40 mmHg Coagulazione: PLT< o INR > 1.5 o PTT > 60” Rene : Oliguria (< 0.5 ml/kg/h), Creatinina > 2 mg/dL Fegato: Bilirubina > 2 mg/dL SNC: sopore o agitazione o GCS <13 Metabolismo: lattati > 2 mmol/l Bone e coll. Chest. 1992;101:1644.
, Creatinina > 2 mg/dL. Fegato: Bilirubina > 2 mg/dL. SNC: sopore o agitazione o GCS <13. Metabolismo: lattati > 2 mmol/l. Bone e coll. Chest. 1992;101:1644.")
6
SEPSI GRAVE SHOCK SETTICO
Infezione, etc. SIRS Sepsi Ipotensione con ipoperfusione refrattaria alla infusione di fluidi Shock settico refrattario : Necessità per mantenere PAm >60 mmHg (80 mmHg se precedente ipertensione) di: dopamina >15 mcg/kg/min, o NORA o adrenalina > 0.25 mcg/kg/min SHOCK SETTICO = Severe sepsis and one of the following conditions: systemic mean BP of <60 mm Hg (<80 mm Hg if previous hypertension) after 20 to 30 mL/kg starch or 40 to 60 mL/kg saline solution, or PCWP between 12 and 20 mm Hg; and need for dopamine of >5 mcg/kg/min, or norepinephrine or epinephrine of <0.25 mcg/kg/min to maintain mean BP at >60 mm Hg (80 mm Hg if previous hypertension) Bone e coll. Chest. 1992;101:1644.
 di: dopamina >15 mcg/kg/min, o. NORA o. adrenalina > 0.25 mcg/kg/min. SHOCK SETTICO = Severe sepsis and one of the following conditions: systemic mean BP of <60 mm Hg (<80 mm Hg if previous hypertension) after 20 to 30 mL/kg starch or 40 to 60 mL/kg saline solution, or PCWP between 12 and 20 mm Hg; and need for dopamine of >5 mcg/kg/min, or norepinephrine or epinephrine of <0.25 mcg/kg/min to maintain mean BP at >60 mm Hg (80 mm Hg if previous hypertension) Bone e coll. Chest. 1992;101:1644.")
7
Dimensione del problema
Incidenza di sepsi severa in USA: 3 casi su 1000 /anno (Angus Cr. Care Med 2001) Prevalenza di 2,26 casi per 100 dimissioni ospedaliere ; nel 68% casi ricovero in ICU ; 27% dei ricoveri in ICU ( Gao Critical Care 2005 ) Mortalità : % ( Angus Crit Care Med 2001) The Intensive Care National Audit and Research Centre: Case Mix Programme Database (interrogated January 2006) The mortality rate from severe sepsis has been estimated in a number of studies as between 28 and 50% . More recently, the SOAP study in Europe observed an overall hospital mortality of 36% . Data from ICNARC shows that patients admitted to Intensive Care Units in the United Kingdom with severe sepsis have a 39.8% risk of death. There are few disease processes with such a high mortality. An admission with severe sepsis places the patient at a level of risk around 6 times greater than if he were admitted with an acute myocardial infarction, and 4-5 times greater than if he had suffered an acute stroke. Critical Care Units (incorporating Intensive Care and High Dependency Care in most UK hospitals) comprise one of the most expensive areas to care for a patient. A large part of this expense- over 50%- arises from the high nurse-to-patient ratio needed to provide the required level of care. Most Units in the UK estimate that a typical bed day costs around £1500. The cost for patients with severe sepsis is likely to be higher due to their greater dependency. It has been estimated in European studies that a typical episode of severe sepsis costs a healthcare organisation approximately 25,000 euros. Assuming that we see 100,000 cases of severe sepsis per annum, this equates to a direct cost to the NHS of over £2.3 billion. The annual cost to Europe as a whole has been estimated to be approximately €7.6 billion1. Since sepsis is not a disease confined to the elderly, far greater costs to the community as a whole are realised in loss of productivity, with the real cost to the economy as a whole of each episode perhaps 4 or 5 times this sum. In summary, sepsis needs to be accepted as the second biggest killer in the United Kingdom, with a huge impact on health economy and on resources- at any one time, a third of our Critical Care capacity is occupied by patients with severe sepsis. The mortality from the condition remains unacceptably high, and has been compared to the mortality from acute myocardial infarction in the 1960s. We need to embrace interventions which have been shown to improve the outcome for these patients, and strive together as a healthcare community to both reduce the incidence of sepsis, and to implement processes to ensure that the highest standard of care is delivered to all patients at the earliest Costi annuali in Europa ~7.6 miliardi € (Davies A. Intensive Care Medicine 2001; 27(Suppl 2):S284.
 Prevalenza di 2,26 casi per 100 dimissioni ospedaliere ; nel 68% casi ricovero in ICU ; 27% dei ricoveri in ICU ( Gao Critical Care 2005 ) Mortalità : % ( Angus Crit Care Med 2001) The Intensive Care National Audit and Research Centre: Case Mix Programme Database (interrogated January 2006) The mortality rate from severe sepsis has been estimated in a number of studies as between 28 and 50% . More recently, the SOAP study in Europe observed an overall hospital mortality of 36% . Data from ICNARC shows that patients admitted to Intensive Care Units in the United Kingdom with severe sepsis have a 39.8% risk of death. There are few disease processes with such a high mortality. An admission with severe sepsis places the patient at a level of risk around 6 times greater than if he were admitted with an acute myocardial infarction, and 4-5 times greater than if he had suffered an acute stroke. Critical Care Units (incorporating Intensive Care and High Dependency Care in most UK hospitals) comprise one of the most expensive areas to care for a patient. A large part of this expense- over 50%- arises from the high nurse-to-patient ratio needed to provide the required level of care. Most Units in the UK estimate that a typical bed day costs around £1500. The cost for patients with severe sepsis is likely to be higher due to their greater dependency. It has been estimated in European studies that a typical episode of severe sepsis costs a healthcare organisation approximately 25,000 euros. Assuming that we see 100,000 cases of severe sepsis per annum, this equates to a direct cost to the NHS of over £2.3 billion. The annual cost to Europe as a whole has been estimated to be approximately €7.6 billion1. Since sepsis is not a disease confined to the elderly, far greater costs to the community as a whole are realised in loss of productivity, with the real cost to the economy as a whole of each episode perhaps 4 or 5 times this sum. In summary, sepsis needs to be accepted as the second biggest killer in the United Kingdom, with a huge impact on health economy and on resources- at any one time, a third of our Critical Care capacity is occupied by patients with severe sepsis. The mortality from the condition remains unacceptably high, and has been compared to the mortality from acute myocardial infarction in the 1960s. We need to embrace interventions which have been shown to improve the outcome for these patients, and strive together as a healthcare community to both reduce the incidence of sepsis, and to implement processes to ensure that the highest standard of care is delivered to all patients at the earliest. Costi annuali in Europa ~7.6 miliardi € (Davies A. Intensive Care Medicine 2001; 27(Suppl 2):S284.")
8
Mortalità N Engl J Med, Vol. 347, No. 13·September 26, 2002
Similarly, Angus et al reported that the annual mortality of severe sepsis in 1995 was 215,000. According to the American Heart Association, this is virtually identical to the number of people in the US who die suddenly of coronary heart disease without being hospitalized. N Engl J Med, Vol. 347, No. 13·September 26, 2002

9
Infezioni più frequenti
Tra i pazienti afferenti alle UTIC: Incidenza di infezioni: 0,9-20% (De Gaudio GIC 2010 ;11;274) Mediastiniti post chirurgiche : 0,4 -5% Infezioni di tasca PM / ICD : 0,8 – 5,7% Infezioni più frequenti Polmoniti IVU Correlate a cateteri Endocarditi Mediastiniti postchirurgiche Manca un registro obbligatorio Uptodate 2011
 Mediastiniti post chirurgiche : 0,4 -5% Infezioni di tasca PM / ICD : 0,8 – 5,7% Infezioni più frequenti. Polmoniti. IVU. Correlate a cateteri. Endocarditi. Mediastiniti postchirurgiche. Manca un registro obbligatorio. Uptodate")
10
Katz et Al - Duke University - Crit Care Med 2010 vol 38 n° 2
increasing prevalence of noncardiovascular critical illness, including sepsis, acute kidney injury, and respiratory failure, with a concomitant increase in mechanical ventilation, central venous catheterization, gastrointestinal endoscopy, and bronchoscopy.

11
Peculiarità in UTIC Fattori di rischio comuni al paziente critico
CVC , Swan Ganz catetere vescicale drenaggi percutanei cannule e.v e arteriose cannule endotracheali …….. Fattori di rischio peculiari cateterismo arterioso angioplastica coronarica elettrostimolazione provvisoria impianto definitivo di devices es. PM, ICD…. contropulsazione aortica impianto di valvole protesiche postumi di cardiochirurgia ECMO …….. Fattori Predisponenti Età avanzata Comorbidità Immunodepressione

12
che per la infezione stessa. ”
” Fatte rare eccezioni, i pazienti sembrano morire più per la risposta del proprio corpo all’infezione che per la infezione stessa. ” Sir William Osler – 1904 The Evolution of Modern Medicine

13
Risposta infiammatoria, immunitaria e coagulativa

14
Fisiopatologia Risposta pro ed antiinfiammatoria
Adattato da Bone RC. Ann Intern Med. 1991;115:

15
Sepsis initiates a brisk inflammatory response that directly and indirectly causes widespread tissue injury. Shown here are key components of this process and their interactions at the level of the microvasculature of a representative vital organ. Gram-positive and gram-negative bacteria, viruses, and fungi have unique cell-wall molecules called pathogen-associated molecular patterns that bind to pattern-recognition receptors (toll-like receptors [TLRs]) on the surface of immune cells. The lipopolysaccharide of gram-negative bacilli binds to lipopolysaccharide-binding protein, CD14 complex. The peptidoglycan of gram-positive bacteria and the lipopolysaccharide of gram-negative bacteria bind to TLR-2 and TLR-4, respectively. Binding of TLR-2 and TLR-4 activates intracellular signal-transduction pathways that lead to the activation of cytosolic nuclear factor κB (NF-κB). Activated NF-κB moves from the cytoplasm to the nucleus, binds to transcription initiation sites, and increases the transcription of cytokines such as tumor necrosis factor α (TNF-α), interleukin-1β, and interleukin-10. TNF-α and interleukin-1β are proinflammatory cytokines that activate the adaptive immune response but also cause both direct and indirect host injury. Interleukin- 10 is an antiinflammatory cytokine that inactivates macrophages and has other antiinflammatory effects. Sepsis increases the activity of inducible nitric oxide synthase (iNOS), which increases the synthesis of nitric oxide (NO), a potent vasodilator. Cytokines activate endothelial cells by up-regulating adhesion receptors and injure endothelial cells by inducing neutrophils, monocytes, macrophages, and platelets to bind to endothelial cells. These effector cells release mediators such as proteases, oxidants, prostaglandins, and leukotrienes. Key functions of the endothelium are selective permeability, vasoregulation, and provision of an anticoagulant surface. Proteases, oxidants, prostaglandins, and leukotrienes injure endothelial cells, leading to increased permeability, further vasodilation, and alteration of the procoagulant–anticoagulant balance. Cytokines also activate the coagulation cascade. Significant derangement in metabolic autoregulation, the process that matches oxygen availability to changing tissue oxygen needs, is typical of sepsis. Vasoactive mediators that are released with inflammation cause an appropriate vasodilation and an increase in microvascular permeability at the site of infection. Among these mediators are the vasodilators prostacyclin and nitric oxide (NO), produced by endothelial cells. A potential factor that may contribute to persistence of vasodilation is impaired compensatory secretion of antidiuretic hormone (vasopressin). In one report, plasma vasopressin levels were much lower in 19 patients with septic shock than in 12 with cardiogenic shock who had similar systemic blood pressures (3.1 versus 22.7 pg/mL) [47]. Why this might occur is not clear. However, numerous small studies have suggested that vasopressin may be helpful in improving hemodynamics and allowing other pressors to be withdrawn Russell NEJM 2006; 355 ; 1699
 on the. surface of immune cells. The lipopolysaccharide of gram-negative bacilli binds to lipopolysaccharide-binding protein, CD14 complex. The peptidoglycan of gram-positive bacteria and the lipopolysaccharide of gram-negative bacteria. bind to TLR-2 and TLR-4, respectively. Binding of TLR-2 and TLR-4 activates intracellular signal-transduction. pathways that lead to the activation of cytosolic nuclear factor κB (NF-κB). Activated NF-κB moves from the cytoplasm. to the nucleus, binds to transcription initiation sites, and increases the transcription of cytokines such as tumor. necrosis factor α (TNF-α), interleukin-1β, and interleukin-10. TNF-α and interleukin-1β are proinflammatory. cytokines that activate the adaptive immune response but also cause both direct and indirect host injury. Interleukin- 10 is an antiinflammatory cytokine that inactivates macrophages and has other antiinflammatory effects. Sepsis. increases the activity of inducible nitric oxide synthase (iNOS), which increases the synthesis of nitric oxide (NO), a. potent vasodilator. Cytokines activate endothelial cells by up-regulating adhesion receptors and injure endothelial. cells by inducing neutrophils, monocytes, macrophages, and platelets to bind to endothelial cells. These effector. cells release mediators such as proteases, oxidants, prostaglandins, and leukotrienes. Key functions of the endothelium. are selective permeability, vasoregulation, and provision of an anticoagulant surface. Proteases, oxidants, prostaglandins, and leukotrienes injure endothelial cells, leading to increased permeability, further vasodilation, and alteration. of the procoagulant–anticoagulant balance. Cytokines also activate the coagulation cascade. Significant derangement in metabolic autoregulation, the process that matches oxygen availability to changing tissue oxygen needs, is typical of sepsis. Vasoactive mediators that are released with inflammation cause an appropriate vasodilation and an increase in microvascular permeability at the site of infection. Among these mediators are the vasodilators prostacyclin and nitric oxide (NO), produced by endothelial cells. A potential factor that may contribute to persistence of vasodilation is impaired compensatory secretion of antidiuretic hormone (vasopressin). In one report, plasma vasopressin levels were much lower in 19 patients with septic shock than in 12 with cardiogenic shock who had similar systemic blood pressures (3.1 versus 22.7 pg/mL) [47]. Why this might occur is not clear. However, numerous small studies have suggested that vasopressin may be helpful in improving hemodynamics and allowing other pressors to be withdrawn. Russell NEJM 2006; 355 ;")
16
Sepsis initiates coagulation by activating endothelium to increase the expression of tissue factor. Activation of the coagulation cascade, and especially factors Va and VIIIa, leads to the formation of thrombin-α, which converts fibrinogen to fibrin. Fibrin binds to platelets, which in turn adhere to endothelial cells, forming microvascular thrombi. Microvascular thrombi amplify injury through the release of mediators and by microvascular obstruction, which causes distal ischemia and tissue hypoxia. Normally, natural anticoagulants (protein C and protein S), antithrombin III, and tissue factor–pathway inhibitor (TFPI) dampen coagulation, enhance fibrinolysis, and remove microthrombi. Thrombin-α binds to thrombomodulin on endothelial cells, which dramatically increases activation of protein C to activated protein C. Protein C forms a complex with its cofactor protein S. Activated protein C proteolytically inactivates factors Va and VIIIa and decreases the synthesis of plasminogen-activator inhibitor 1 (PAI-1). In contrast, sepsis increases the synthesis of PAI-1. Sepsis also decreases the levels of protein C, protein S, antithrombin III, and TFPI. Lipopolysaccharide and tumor necrosis factor α (TNF-α) decrease the synthesis of thrombomodulin and endothelial protein C receptor (EPCR), thus decreasing the activation of protein C. Sepsis further disrupts the protein C pathway because sepsis also decreases the expression of EPCR, which amplifies the deleterious effects of the sepsis- induced decrease in levels of protein C. Lipopolysaccharide and TNF-α also increase PAI-1 levels so that fibrinolysis is inhibited. The clinical consequences of the changes in coagulation caused by sepsis are increased levels of markers of disseminated intravascular coagulation and widespread organ dysfunction. t-PA denotes tissue plasminogen activator. Russell NEJM 2006; 355 ; 1699
, antithrombin. III, and tissue factor–pathway inhibitor (TFPI) dampen coagulation, enhance fibrinolysis, and remove microthrombi. Thrombin-α binds to thrombomodulin on endothelial cells, which dramatically increases activation of protein C to. activated protein C. Protein C forms a complex with its cofactor protein S. Activated protein C proteolytically inactivates. factors Va and VIIIa and decreases the synthesis of plasminogen-activator inhibitor 1 (PAI-1). In contrast, sepsis. increases the synthesis of PAI-1. Sepsis also decreases the levels of protein C, protein S, antithrombin III, and. TFPI. Lipopolysaccharide and tumor necrosis factor α (TNF-α) decrease the synthesis of thrombomodulin and endothelial. protein C receptor (EPCR), thus decreasing the activation of protein C. Sepsis further disrupts the protein. C pathway because sepsis also decreases the expression of EPCR, which amplifies the deleterious effects of the sepsis- induced decrease in levels of protein C. Lipopolysaccharide and TNF-α also increase PAI-1 levels so that fibrinolysis. is inhibited. The clinical consequences of the changes in coagulation caused by sepsis are increased levels of. markers of disseminated intravascular coagulation and widespread organ dysfunction. t-PA denotes tissue plasminogen. activator. Russell NEJM 2006; 355 ;")
17
Theoretical pressure–volume loops in normal controls, survivors
and non-survivors of septic shock. In non-survivors, failure to increase ventricular compliance results in inability to maintain stroke volume and hence cardiac output. Similar changes are seen in both right and left ventricle. In the central circulation, changes in both systolic and diastolic ventricular performance are early manifestations of sepsis [52]. Nevertheless, ventricular function may initially be able to increase the cardiac output through use of the Frank Starling mechanism. This increase in output is necessary to maintain the blood pressure in the presence of the systemic vasodilation that complicates sepsis. Patients with preexisting cardiac disease may be unable to increase their cardiac output appropriately. This may be a particular problem in elderly subjects. The classical cardiovascular response to septic shock is peripheral vasodilatation manifest as systemic hypotension, hyporesponsive to pressor agents. Although it has been recognised for many years that intrinsic myocardial dysfunction also occurs, this is commonly masked by the concomitant elevation in cardiac index. Survivors of septic shock were found to have decreased systolic function to an ejection fraction of about 33% and an increase in left ventricular end-diastolic diameter. These changes in left ventricular function were of rapid onset and reversible in survivors within 7 to 10 days. Paradoxically the changes seen were less profound in those who died, who were subdivided in subsequent studies into two groups: those with increased end-diastolic volume and stroke volume, but no increase in heart rate and ejection fraction; and patients with progressive ventricular dilatation, but no increase in stroke volume, heart rate and ejection fraction. Further studies of the response of the left ventricle to volume loading showed an abnormal increase in left ventricular end-diastolic diameter in the survivors of sepsis, implying increased ventricular compliance. Studies of right ventricular function have shown a similar pattern in septic shock, with decreased ejection fraction, and increased end-diastolic volume, occurring independently of the changes in pulmonary artery pressure. Le proprietà lusitrope del ventricolo influenzano la sopravvivenza : negli anziani queste sono ridotte In the regional circulation, the vascular hyporesponsiveness induced by sepsis leads to considerable heterogeneity in the normal distribution of systemic blood flow among organ systems. As an example, sepsis interferes with the normal ability to redistribute blood flow from the splanchnic organs to the core organs (heart and brain) when oxygen delivery is depressed S.Price EHJ 1999;20;715
 when oxygen delivery is depressed. S.Price EHJ 1999;20;715.")
19
pKraopBlaNnP-M) aetie trh ceu crvueto ffof rv aNlu-tee romf i6na,6l 2p4ro p-bgr/aminl natriuretic peptide (NTproBNP) at the cutoff value of 6,624 pg/ml. Kaplan-Meier analysis estimates the rate of death within intensive care unit (ICU) stay among septic shock patients according to NT-proBNP values above or below 6,624 pg/ml (cutoff value as determined by receiver operating characteristic curve analysis). The differences between the two groups were Mokart Crit.Care 2007;11;R37
 stay among septic. shock patients according to NT-proBNP values above or below. 6,624 pg/ml (cutoff value as determined by receiver operating characteristic. curve analysis). The differences between the two groups were. Mokart Crit.Care 2007;11;R37.")
20
Outcome è influenzato da:
Risposta dell’ ospite : febbre, leucopenia… Comorbidità : cirrosi, diabete , insuff. cardiaca, IRC… Età Sito di infezione : urosepsi vs infez. polmonare Risultato delle emocolture Tipo di MO : infezioni nosocomiali vs comunitarie - MRSA vs MSSA vs Pseudom. vs Acinetobacter Terapia antibiotica Sepsis care bundle nella sepsi severa Simple categorical descriptions of sepsis patients (eg, shock/nonshock, bacteremic/nonbacteremic, gram-positive/gram-negative) do not adequately characterize illness severity or accurately define the mortality risk. Multicenter, prospective studies of sepsis have suggested that there is a continuum of severity that has both infectious and inflammatory components. The clinical spectrum usually begins with infection that potentially leads to sepsis, organ dysfunction (ie, severe sepsis), and septic shock. While recognizing that the disease process forms a continuum of severity, clinical trials have found that definable phases exist on this continuum that characterize populations at increased risk of morbidity and mortality. As an example, one study evaluated the natural history of 2527 patients with SIRS [16]: 48 percent developed part of the sepsis continuum, including sepsis (26 percent), severe sepsis (18 percent), or septic shock (4 percent) The incidence of positive blood cultures increased along the continuum: 17 percent with sepsis to 69 percent with septic shock. Although the cause of culture-negative disease was often not established, the mortality rate within a category was not influenced by the culture results The mortality rate increased progressively along the continuum: 7 percent with SIRS alone, 16 percent with sepsis, 20 percent with severe sepsis, and 46 percent with septic shock The most common manifestations of severe organ dysfunction were acute respiratory distress syndrome, acute renal failure, and disseminated intravascular coagulation. Survival was reduced in patients with these complications Clinical trials in the 1980s and 1990s confirmed the prognostic importance of the definitions of the different sepsis syndromes. Patients with sepsis die at a significantly lower rate than those with severe sepsis or septic shock on admission or those who develop shock subsequent to study entry [22-25,29]. Categorical definitions, such as SIRS, severe sepsis, and septic shock, have important limitations [3,30]. They identify patients with a variable baseline or pretreatment risk, which contributes to the large range in mortality within a category in published trials. Furthermore, some patients with clinical evidence of sepsis may not fulfill the exact criteria for a categorical definition such as the sepsis syndrome. These limitations have led to recognition of the importance of physiologic derangements and individual patient characteristics in determining the outcome from sepsis [3]. Definitions of sepsis, severe sepsis, and septic shock are based on clinical experience (ie, "expert" advice) and the correlation of infection progression with appropriate physiologic OSPITE : Failure to develop a fever (or the occurrence of hypothermia) is associated with increased fatality rates in patients with sepsis [30,33,34]. In an analysis of 519 septic patients, for example, a temperature below 35.5ºC was found in 17 percent of nonsurvivors versus 5 percent of survivors [30]. Leukopenia (a white blood cell count less than 4000/mm3) was also more frequent in nonsurvivors (15 versus 7 percent in survivors) [34]. Thus, failure to develop a febrile response and the presence of leukopenia are characteristic of severe disease, and probably represent anomalies in the host's inflammatory response. Underlying disease — The presence of underlying diseases and the functional health status of the patient are important determinants of outcome in severe sepsis [30]. Risk factors for mortality from sepsis include age above 40 years and comorbid conditions at the time of diagnosis of sepsis, such as AIDS, hepatic failure, cirrhosis, cancer, alcohol dependence, and/or immune suppression [30,35-38]. Age — Older patients are at increased risk of severe sepsis, in part because of comorbid illness and impaired immunologic response to infection [7,10,39]. Malnutrition, increased exposure to potentially resistant bacterial pathogens in nursing homes, and utilization of medical devices including indwelling catheters and central venous lines also contribute to this increased risk [39]. Older patients are at increased risk of morbidity and mortality following the development of sepsis [7,10]. In the United States, patients ≥65 years of age account for nearly 60 percent of all episodes of severe sepsis. This percentage is likely to increase over the next 20 years [7,10,40]. Site of infection — The site of infection in patients with sepsis may be an important determinant of outcome, with urosepsis being associated with lower mortality rates [30,41]. One study, for example, found mortality rates from sepsis between 50 and 55 percent when the source of infection was unknown or was gastrointestinal or pulmonary; in comparison, the mortality rate was only 30 percent when the source was the urinary tract [41]. Blood culture results — Approximately 50 percent of patients with severe sepsis demonstrate bacteremia at the time of diagnosis [42]. However, the presence or absence of a positive blood culture does not appear to influence outcome, suggesting that the prognosis may be more related to the severity of sepsis rather than to the severity of any underlying infection [4]. Microorganism — Nosocomial infections have higher mortality than community-acquired infection (15 versus 10 percent) [43]. This likely reflects the culprit microorganism, since increased mortality is associated with bloodstream infections due to methicillin-resistant staphylococcus aureus (odds ratio 2.70, 95% CI ), non-candidal fungus (odds ratio 2.66, 95% CI ), candida (odds ratio % CI ), methicillin-sensitive staphylococcus aureus (odds ratio 1.9, 95% CI ), polymicrobial (odds ratio 1.69, 95% CI ), and pseudomonas (odds ratio 1.6, 95% CI ) [43]. When bloodstream infections become severe (ie, severe sepsis or septic shock), gram-negative and gram-positive bacteria have similar outcomes [22,44]. Antimicrobial therapy — The influence of antimicrobial therapy on the prognosis of bacteremic and non-bacteremic sepsis is uncertain, although some studies have shown a benefit of appropriate antibiotic therapy on bacteremic sepsis prognosis. In one report, for example, early institution of adequate therapy was associated with a 50 percent reduction in fatality rate compared to that observed in patients treated with antibiotics to which the infecting organisms were resistant [34]. LONG-TERM SURVIVAL — A systematic review of 30 studies (>38,000 patients) found that mortality was significantly higher at one-year among patients who had been in the ICU with sepsis compared to those who had been in the ICU for reasons unrelated to infection [45]. While mortality remains increased at one-year among patients who had sepsis, it appears that most of the deaths may occur within the first six months [46,47]. Finally, patients who had sepsis also appear to have a persistent decrement in their quality of life [45].
 do not adequately characterize illness severity or accurately define the mortality risk. Multicenter, prospective studies of sepsis have suggested that there is a continuum of severity that has both infectious and inflammatory components. The clinical spectrum usually begins with infection that potentially leads to sepsis, organ dysfunction (ie, severe sepsis), and septic shock. While recognizing that the disease process forms a continuum of severity, clinical trials have found that definable phases exist on this continuum that characterize populations at increased risk of morbidity and mortality. As an example, one study evaluated the natural history of 2527 patients with SIRS [16]: 48 percent developed part of the sepsis continuum, including sepsis (26 percent), severe sepsis (18 percent), or septic shock (4 percent) The incidence of positive blood cultures increased along the continuum: 17 percent with sepsis to 69 percent with septic shock. Although the cause of culture-negative disease was often not established, the mortality rate within a category was not influenced by the culture results. The mortality rate increased progressively along the continuum: 7 percent with SIRS alone, 16 percent with sepsis, 20 percent with severe sepsis, and 46 percent with septic shock. The most common manifestations of severe organ dysfunction were acute respiratory distress syndrome, acute renal failure, and disseminated intravascular coagulation. Survival was reduced in patients with these complications. Clinical trials in the 1980s and 1990s confirmed the prognostic importance of the definitions of the different sepsis syndromes. Patients with sepsis die at a significantly lower rate than those with severe sepsis or septic shock on admission or those who develop shock subsequent to study entry [22-25,29]. Categorical definitions, such as SIRS, severe sepsis, and septic shock, have important limitations [3,30]. They identify patients with a variable baseline or pretreatment risk, which contributes to the large range in mortality within a category in published trials. Furthermore, some patients with clinical evidence of sepsis may not fulfill the exact criteria for a categorical definition such as the sepsis syndrome. These limitations have led to recognition of the importance of physiologic derangements and individual patient characteristics in determining the outcome from sepsis [3]. Definitions of sepsis, severe sepsis, and septic shock are based on clinical experience (ie, expert advice) and the correlation of infection progression with appropriate physiologic. OSPITE : Failure to develop a fever (or the occurrence of hypothermia) is associated with increased fatality rates in patients with sepsis [30,33,34]. In an analysis of 519 septic patients, for example, a temperature below 35.5ºC was found in 17 percent of nonsurvivors versus 5 percent of survivors [30]. Leukopenia (a white blood cell count less than 4000/mm3) was also more frequent in nonsurvivors (15 versus 7 percent in survivors) [34]. Thus, failure to develop a febrile response and the presence of leukopenia are characteristic of severe disease, and probably represent anomalies in the host s inflammatory response. Underlying disease — The presence of underlying diseases and the functional health status of the patient are important determinants of outcome in severe sepsis [30]. Risk factors for mortality from sepsis include age above 40 years and comorbid conditions at the time of diagnosis of sepsis, such as AIDS, hepatic failure, cirrhosis, cancer, alcohol dependence, and/or immune suppression [30,35-38]. Age — Older patients are at increased risk of severe sepsis, in part because of comorbid illness and impaired immunologic response to infection [7,10,39]. Malnutrition, increased exposure to potentially resistant bacterial pathogens in nursing homes, and utilization of medical devices including indwelling catheters and central venous lines also contribute to this increased risk [39]. Older patients are at increased risk of morbidity and mortality following the development of sepsis [7,10]. In the United States, patients ≥65 years of age account for nearly 60 percent of all episodes of severe sepsis. This percentage is likely to increase over the next 20 years [7,10,40]. Site of infection — The site of infection in patients with sepsis may be an important determinant of outcome, with urosepsis being associated with lower mortality rates [30,41]. One study, for example, found mortality rates from sepsis between 50 and 55 percent when the source of infection was unknown or was gastrointestinal or pulmonary; in comparison, the mortality rate was only 30 percent when the source was the urinary tract [41]. Blood culture results — Approximately 50 percent of patients with severe sepsis demonstrate bacteremia at the time of diagnosis [42]. However, the presence or absence of a positive blood culture does not appear to influence outcome, suggesting that the prognosis may be more related to the severity of sepsis rather than to the severity of any underlying infection [4]. Microorganism — Nosocomial infections have higher mortality than community-acquired infection (15 versus 10 percent) [43]. This likely reflects the culprit microorganism, since increased mortality is associated with bloodstream infections due to methicillin-resistant staphylococcus aureus (odds ratio 2.70, 95% CI ), non-candidal fungus (odds ratio 2.66, 95% CI ), candida (odds ratio % CI ), methicillin-sensitive staphylococcus aureus (odds ratio 1.9, 95% CI ), polymicrobial (odds ratio 1.69, 95% CI ), and pseudomonas (odds ratio 1.6, 95% CI ) [43]. When bloodstream infections become severe (ie, severe sepsis or septic shock), gram-negative and gram-positive bacteria have similar outcomes [22,44]. Antimicrobial therapy — The influence of antimicrobial therapy on the prognosis of bacteremic and non-bacteremic sepsis is uncertain, although some studies have shown a benefit of appropriate antibiotic therapy on bacteremic sepsis prognosis. In one report, for example, early institution of adequate therapy was associated with a 50 percent reduction in fatality rate compared to that observed in patients treated with antibiotics to which the infecting organisms were resistant [34]. LONG-TERM SURVIVAL — A systematic review of 30 studies (>38,000 patients) found that mortality was significantly higher at one-year among patients who had been in the ICU with sepsis compared to those who had been in the ICU for reasons unrelated to infection [45]. While mortality remains increased at one-year among patients who had sepsis, it appears that most of the deaths may occur within the first six months [46,47]. Finally, patients who had sepsis also appear to have a persistent decrement in their quality of life [45].")
21
Trattamento tempestivo
Il “Sepsis Bundle” è un “Pacchetto di interventi” composto da un gruppo di azioni che, se poste in atto insieme, comportano un outcome migliore rispetto al loro utilizzo individuale. Diagnosi clinica Trattamento tempestivo Serie di azioni da eseguire entro le prime 6 ore - 24 ore Mortality Gao F, Melody T, Daniels DF, et al. The impact of compliance with 6-hour and 24-hour sepsis bundles on hospital mortality in patients with severe sepsis: a prospective observational study. Crit Care. 2005; 9:R764-R770. I componenti di un “Pacchetto” possono essere facilmente misurati come completamente o incompletamente attuati. Forniscono una “pressione” al team di lavoro Compliant Non compliant

22
Crit Care Med 2008; 36;

23
Gestione iniziale- EGDT ( early goal directed therapy)
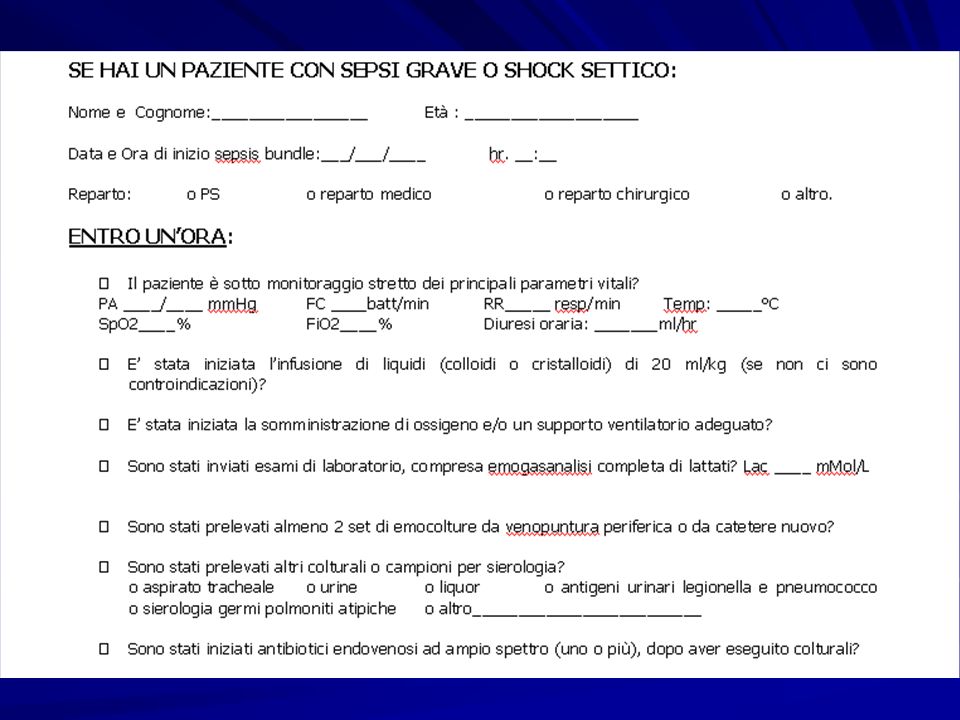
Riconoscimento precoce Ottimizzazione metabolismo/perfusione (SvO2 > 65%) Entro le prime 6h Emocolture prima dell’antibiotico Priorità : Precoce inizio delle terapie di supporto Distinzione tra SIRS e sepsi perché se esiste infezione, va identificata e trattata tempestivamente ricorrendo a sua rimozione se possibile ( es. ascesso) e antibiotici adeguatamente Bonifica della sede infettiva Terapia antibiotica entro 1 h Diagnosi e terapia Rivers et al. NEJM :
 Entro le prime 6h. Emocolture prima dell’antibiotico. Priorità : Precoce inizio delle terapie di supporto. Distinzione tra SIRS e sepsi perché se esiste infezione, va identificata e trattata tempestivamente ricorrendo a sua rimozione se possibile ( es. ascesso) e antibiotici adeguatamente. Bonifica della sede infettiva. Terapia antibiotica entro 1 h. Diagnosi e terapia. Rivers et al. NEJM :")
24
Gestione iniziale della sepsi severa e dello shock settico
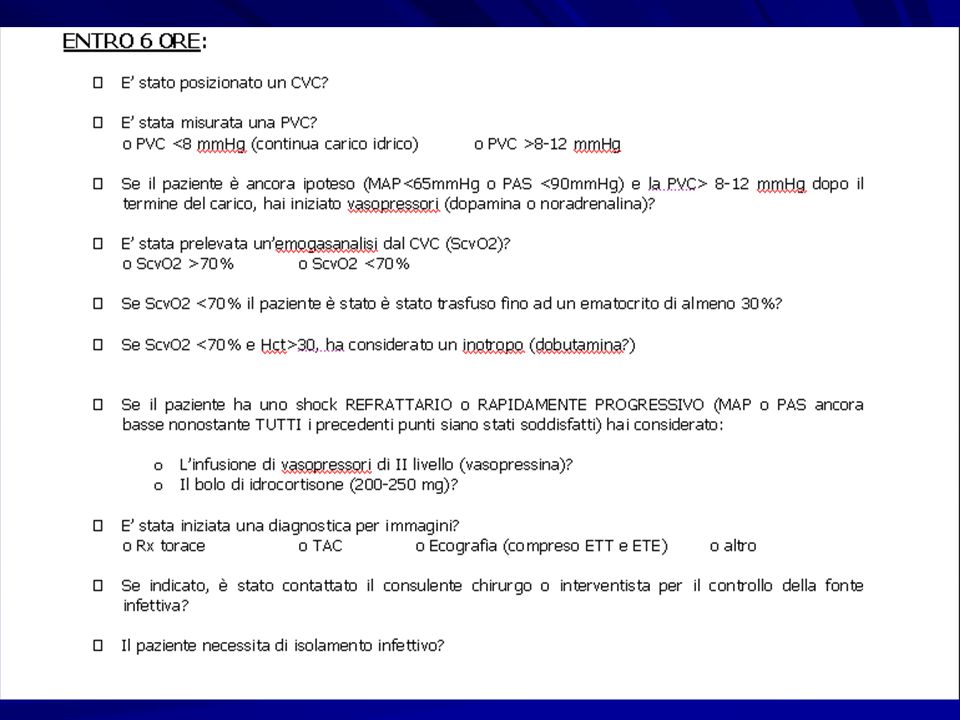
Stabilizzare il respiro con goal SvO2 > 65% : RX torace ed EGA – O2 - NIV - eventuale sedazione ed intubazione Valutare la perfusione : Diuresi, ottundimento o agitazione, PA invasiva, perfusione periferica, lattati ( target < 4 mMol/L) , fc CVC Ripristinare la perfusione : ScvcO2 > 70 % ( o SvO2 > 65%) MAP > 65 mmHg PVC 8-12 mmHg ( se VAM 12-15) QU > 0,5 mL/kg/h utilizzando : 1° : Fluidi ev : Challenge con cristalloidi ml in 30’ 2° : Vasopressori : ( NORA o DOPA) se resta ipotensione o sviluppo di EPA – (ADR – Vasopressina seconda scelta) 3° : Inotropi : se disfunzione miocardica ( Dobutamina se volemia e MAP adeguate) 4° : Trasfusione di emazie concentrate se ScvcO2 < 70, fino ad Ht > 30 ( nell’anziano , diabetico o con β-bloccante < tachicardia da ipotensione) Perfusione è ridotta per : perdita di volume nello spazio interstiziale, ipotono vascolare, depressione miocardica La ScvcO2 indica la relazione fra Disponibilità di Ossigeno e Consumo dell’Ossigeno.
 , fc. CVC. Ripristinare la perfusione : ScvcO2 > 70 % ( o SvO2 > 65%) MAP > 65 mmHg PVC 8-12 mmHg ( se VAM 12-15) QU > 0,5 mL/kg/h. utilizzando : 1° : Fluidi ev : Challenge con cristalloidi ml in 30’ 2° : Vasopressori : ( NORA o DOPA) se resta ipotensione o sviluppo di EPA – (ADR – Vasopressina seconda scelta) 3° : Inotropi : se disfunzione miocardica ( Dobutamina se volemia e MAP adeguate) 4° : Trasfusione di emazie concentrate se ScvcO2 < 70, fino ad Ht > 30. ( nell’anziano , diabetico o con β-bloccante < tachicardia da ipotensione) Perfusione è ridotta per : perdita di volume nello spazio interstiziale, ipotono vascolare, depressione miocardica. La ScvcO2 indica la relazione fra Disponibilità di Ossigeno e Consumo dell’Ossigeno.")
25
Gestione iniziale- EGDT ( early goal directed therapy)
Riconoscimento precoce Somministrazione di fluidi Ottimizzazione metabolismo (ScvO2>70%) Entro le prime 6h Emocolture prima dell’antibiotico Priorità : Precoce inizio delle terapie di supporto Distinzione tra SIRS e sepsi perché se esiste infezione, va identificata e trattata tempestivamente ricorrendo a sua rimozione se possibile ( es. ascesso) e antibiotici adeguatamente Terapia antibiotica empirica entro 1 h Bonifica della sede infettiva se possibile Diagnosi e terapia Rivers et al. NEJM :
 Entro le prime 6h. Emocolture prima dell’antibiotico. Priorità : Precoce inizio delle terapie di supporto. Distinzione tra SIRS e sepsi perché se esiste infezione, va identificata e trattata tempestivamente ricorrendo a sua rimozione se possibile ( es. ascesso) e antibiotici adeguatamente. Terapia antibiotica empirica entro 1 h. Bonifica della sede infettiva se possibile. Diagnosi e terapia. Rivers et al. NEJM :")
26
Diagnosi – identificazione del focus settico
Esami colturali prima di ABT : se possibile prelievi da fonti di infezione (… tasca infetta,urina,broncoaspirato, feci, liquido dei drenaggi…) Emocolture : prima di ABT : percutanee , + 1 da ogni catetere in sede da > 48 h. Venipuntura tempestiva, indipendentemente dalla T° 3 aerobi + 3 anaerobi Prelevare 30 ml e inoculare 5-7 mL per flacone Se già in ABT , prelievo al livello ematico minimo di ABT Ag urinari per Pneumococco e Legionella P1 Imaging ( RX , ecografie…) quanto prima Biomarkers (?)( procalcitonina, PCR) Upper respiratory tract Pharyngeal inflammation plus exudate ± swelling and lymphadenopathy Throat swab for aerobic culture Lower respiratory tract Productive cough, pleuritic chest pain, consolidative auscultatory findings Sputum of good quality, quantitative culture of protected brush or bronchoalveolar lavage Urinary tract Fever, urgency, dysuria, loin painUrine microscopy >50 WBC/hpf plus:midstream urine >100,000 cfu/mL catheter urine >100,000 cfu/mLSuprapubic aspirate >1000 cfu/mL Wound or burnInflammation, edema, erythema, discharge of pusGram stain and culture of draining pus, wound culture not reliable Skin/soft tissueErythema, edema, lymphangitisCulture blister fluid or draining pus; role of tissue aspirates not proven Central nervous systemSigns of meningeal irritationCSF microscopy, protein, glucose, culture, bacterial antigen test GastrointestinalAbdominal pain, distension, diarrhea, and vomitingStool culture for Salmonella, Shigella, and Campylobacter IntraabdominalSpecific abdominal symptoms/signsAerobic and anaerobic culture of percutaneously or surgically drained abdominal fluid collections Peritoneal dialysis (PD) infectionsCloudy PD fluid, abdominal pain, feverCell count and culture of PD fluid Genital tractLow abdominal pain, vaginal dischargeEndocervical and high vaginal swabs onto selective media Dopo poche ore dalla I° dose di ATB le emocolture si sterilizzano Procalcitonina Pro-ormone della calcitonina , prodotto in risposta a stimoli pro-infiammatori, quali i prodotti di degradazione batterica. Indicatore della risposta infiammatoria sistemica in corso di sepsi Diagnosi e monitoraggio di sepsi Aumenta 6-12 h dopo sepsi vn < 0,05 ng/mL , zona grigia tra 0,5 e 2 ( ripetere l’esame dopo 6-24h) , se > 2 suggestivo per sepsi Costi + Falsi positivi es. shock cardiogeno prolungato > sensibilità (85%) e specificità (91%) rispetto a PCR, IL2, IL6,IL8 , TNFα per differenziare SIRS da sepsi
 Emocolture : prima di ABT : percutanee , + 1 da ogni catetere in sede da > 48 h. Venipuntura tempestiva, indipendentemente dalla T° 3 aerobi + 3 anaerobi. Prelevare 30 ml e inoculare 5-7 mL per flacone. Se già in ABT , prelievo al livello ematico minimo di ABT. Ag urinari per Pneumococco e Legionella P1. Imaging ( RX , ecografie…) quanto prima. Biomarkers ( )( procalcitonina, PCR) Upper respiratory tract Pharyngeal inflammation plus exudate ± swelling and lymphadenopathy Throat swab for aerobic culture. Lower respiratory tract Productive cough, pleuritic chest pain, consolidative auscultatory findings Sputum of good quality, quantitative culture of protected brush or bronchoalveolar lavage. Urinary tract Fever, urgency, dysuria, loin painUrine microscopy >50 WBC/hpf plus:midstream urine >100,000 cfu/mL catheter urine >100,000 cfu/mLSuprapubic aspirate >1000 cfu/mL. Wound or burnInflammation, edema, erythema, discharge of pusGram stain and culture of draining pus, wound culture not reliable. Skin/soft tissueErythema, edema, lymphangitisCulture blister fluid or draining pus; role of tissue aspirates not proven. Central nervous systemSigns of meningeal irritationCSF microscopy, protein, glucose, culture, bacterial antigen test. GastrointestinalAbdominal pain, distension, diarrhea, and vomitingStool culture for Salmonella, Shigella, and Campylobacter. IntraabdominalSpecific abdominal symptoms/signsAerobic and anaerobic culture of percutaneously or surgically drained abdominal fluid collections. Peritoneal dialysis (PD) infectionsCloudy PD fluid, abdominal pain, feverCell count and culture of PD fluid. Genital tractLow abdominal pain, vaginal dischargeEndocervical and high vaginal swabs onto selective media. Dopo poche ore dalla I° dose di ATB le emocolture si sterilizzano. Procalcitonina. Pro-ormone della calcitonina , prodotto in risposta a stimoli pro-infiammatori, quali i prodotti di degradazione batterica. Indicatore della risposta infiammatoria sistemica in corso di sepsi. Diagnosi e monitoraggio di sepsi. Aumenta 6-12 h dopo sepsi. vn < 0,05 ng/mL , zona grigia tra 0,5 e 2 ( ripetere l’esame dopo 6-24h) , se > 2 suggestivo per sepsi. Costi + Falsi positivi es. shock cardiogeno prolungato. > sensibilità (85%) e specificità (91%) rispetto a PCR, IL2, IL6,IL8 , TNFα per differenziare SIRS da sepsi.")
27
Terapia tempestiva VS tardiva
ATB e.v quanto prima e sempre entro la prima ora dalla diagnosi di sepsi grave o di shock settico Usare ATB (1 o +) ad ampio spettro Terapia appropriata VS inappropriata Terapia tempestiva VS tardiva RAHAL et Al. Critical Care 2008, 12(suppl 4): S5 KUMAR et al.Crit Care Med 2006;34:1589
 ad ampio spettro. Terapia appropriata VS inappropriata. Terapia tempestiva VS tardiva. RAHAL et Al. Critical Care 2008, 12(suppl 4): S5. KUMAR et al.Crit Care Med 2006;34:1589.")
28
Terapia AB empirica precoce
Dose piena di carico di ATB e.v. Monitoraggio [ ] seriche ( insuff.epatica o renale – aumento del volume di distribuzione ) Scelta in base a: - anamnesi (es. recente ABT) - comorbidità - contesto clinico (infez. comunità [ricovero < 48 h] o ospedaliere) - sito di infezione sospettato - patterns di resistenze locali - Gram stain e MIC - caratteristiche Pk/Pd
 Scelta in base a: - anamnesi (es. recente ABT) - comorbidità. - contesto clinico. (infez. comunità [ricovero < 48 h] o ospedaliere) - sito di infezione sospettato. - patterns di resistenze locali. - Gram stain e MIC. - caratteristiche Pk/Pd.")
29
Diffusibilità degli AB

30
Caratteristiche farmacodinamiche degli antibiotici
1 Tempo dipendenti Beta-lattamine Glicopeptidi Linezolid Macrolidi 2 Concentrazione-dipendenti Fluorochinoloni, Daptomicina Aminoglicosidi; Ketolidi L’elemento guida nella scelta della terapia è rappresentato dalla valutazione della sensibilità in vitro all’antibiotico, caratteristica espressa dalla minima concentrazione inibente (MIC). La terapia deve, infatti, mirare al raggiungimento della MIC non solo nel plasma, ma soprattutto nel sito di infezione Per le molecole con attività tempo-dipendente il maggior determinante dell’efficacia terapeutica è il tempo (t) durante il quale la concentrazione plasmatica rimane superiore alla MIC (t>MIC). gli antibiotici tempo- dipendenti hanno inoltre uno scarso effetto post-antibiotico L’efficacia degli antibiotici concentrazione-dipendenti correla con i livelli di picco plasmatico del farmaco e la loro attività è descritta dal rapporto tra concentrazione massima (Cmax) e MIC e dal rapporto fra area sotto la curva concentrazione plasmatica-tempo (AUC) e MIC.
. La terapia deve, infatti, mirare al raggiungimento della. MIC non solo nel plasma, ma soprattutto nel sito di infezione. Per le molecole con attività tempo-dipendente il maggior. determinante dell’efficacia terapeutica è il tempo (t) durante. il quale la concentrazione plasmatica rimane superiore alla. MIC (t>MIC). gli antibiotici tempo- dipendenti hanno inoltre uno scarso effetto post-antibiotico. L’efficacia degli antibiotici concentrazione-dipendenti. correla con i livelli di picco plasmatico del farmaco e la loro. attività è descritta dal rapporto tra concentrazione massima. (Cmax) e MIC e dal rapporto fra area sotto la curva concentrazione. plasmatica-tempo (AUC) e MIC.")
31
Tempo di risposta delle emocolture
Durata della ATB : gg; > se risposta clinica lenta o foci di infezioni non drenabili o immunodeficienze Terapia empirica di combinazione iniziale: se sepsi grave/shock settico oppure sospetto di Pseudomonas o neutropenia Dopo AB gramma ( 3-5 gg ) restringere lo spettro di azione (de-escalation) . Tempo di risposta delle emocolture BSI = blood stream infection 85 % delle BSI positive entro 24 ore di incubazione in termostato Per Candida e anaerobi come Clostridi e Bacteroides giorni di incubazione Il tempo di incubazione standard di 6 giorni consente la crescita del 99% dei batteri La ATB raddoppia o triplica i tempi di crescita o impedisce tot. le crescite
 restringere lo spettro di azione (de-escalation) . Tempo di risposta delle emocolture. BSI = blood stream infection. 85 % delle BSI positive entro 24 ore di incubazione in termostato. Per Candida e anaerobi come Clostridi e Bacteroides giorni di incubazione. Il tempo di incubazione standard di 6 giorni consente la crescita del 99% dei batteri. La ATB raddoppia o triplica i tempi di crescita o impedisce tot. le crescite.")
32
SEPSI GRAVE / SHOCK SETTICO
ABT ad ampio spettro empirica : attiva su Gram + e Gram- : Vancomicina : Cefalosporina 3° o 4° gen. ( Ceftriaxone o Cefotaxime) o Bettalattamico/betalattamasi inib.(Piperacillina/TZ o Ticarcillina/Clav.) o Carbapenemico (Meropenem, Imipenem) Se sospetto di Pseudomonas usare Vancomicina + 2 dei seguenti: Cefalosporine antiPseudom. ( Ceftazidime, Cefepime) o Cefalosporina 3° o 4° gen. ( Ceftriaxone o Cefotaxime) o Bettalattamico/betalattamasi inib.(Piperacillina/TZ oTicarcillina/Clav.) o Carbapenemico (Meropenem, Imipenem) o Fluorochinolone attivo su Pseudo (Ciprofloxacina) o Aminoglicoside (Gentamicina, Amikacina) o Monobactam (Aztreonam) Staphylococcus aureus is associated with significant morbidity if not treated early in the course of infection [59]. There is growing recognition that methicillin-resistant S. aureus (MRSA) is a cause of sepsis not only in hospitalized patients, but also in community dwelling individuals without recent hospitalization [60,61]. Many of these staphylococci have the Panton-Valentine leukocidin virulence factor, which causes severe, necrotizing infections [62]. For these reasons, we recommend that severely ill patients presenting with sepsis of unclear etiology be treated with intravenous vancomycin (adjusted for renal function) until the possibility of MRSA sepsis has been excluded. Linezolid is a reasonable alternative if there are contraindications to vancomycin. After culture results and antimicrobial susceptibility data return, we recommend that therapy be pathogen- and susceptibility-directed, even if there has been clinical improvement while on the initial antimicrobial regimen. Gram-negative pathogens have historically been covered with two agents from different antibiotic classes. However, several clinical trials and two meta-analyses have failed to demonstrate superior overall efficacy of combination therapy compared to monotherapy with a third generation cephalosporin or a carbapenem [55,63-67]. Furthermore, one meta-analysis found double coverage was associated with an increased incidence of adverse events [66,67]. For this reason, we recommend use of a single agent with proven efficacy and the least possible toxicity, except in patients who are either neutropenic or whose severe sepsis is due to a known or suspected Pseudomonas infection [7,65]. (See "Pseudomonas aeruginosa bacteremia and endocarditis" and "Treatment of Pseudomonas aeruginosa infections".) Regardless of the antibiotic regimen selected, patients should be observed closely for toxicity, evidence of response, and the development of nosocomial superinfection [68]. The duration of therapy is typically 7 to 10 days, although longer courses may be appropriate in patients who have a slow clinical response, an undrainable focus of infection, or immunologic deficiencies [7]. In patients who are neutropenic, antibiotic treatment should continue until the neutropenia has resolved. In non-neutropenic patients in whom infection is thoroughly excluded, antibiotics should be discontinued to minimize colonization or infection with drug-resistant microorganisms and superinfection with other pathogens. Schmitd Uptodate 2011
 o. Bettalattamico/betalattamasi inib.(Piperacillina/TZ o Ticarcillina/Clav.) o. Carbapenemico (Meropenem, Imipenem) Se sospetto di Pseudomonas usare Vancomicina + 2 dei seguenti: Cefalosporine antiPseudom. ( Ceftazidime, Cefepime) o. Cefalosporina 3° o 4° gen. ( Ceftriaxone o Cefotaxime) o. Bettalattamico/betalattamasi inib.(Piperacillina/TZ oTicarcillina/Clav.) o. Carbapenemico (Meropenem, Imipenem) o. Fluorochinolone attivo su Pseudo (Ciprofloxacina) o. Aminoglicoside (Gentamicina, Amikacina) o. Monobactam (Aztreonam) Staphylococcus aureus is associated with significant morbidity if not treated early in the course of infection [59]. There is growing recognition that methicillin-resistant S. aureus (MRSA) is a cause of sepsis not only in hospitalized patients, but also in community dwelling individuals without recent hospitalization [60,61]. Many of these staphylococci have the Panton-Valentine leukocidin virulence factor, which causes severe, necrotizing infections [62]. For these reasons, we recommend that severely ill patients presenting with sepsis of unclear etiology be treated with intravenous vancomycin (adjusted for renal function) until the possibility of MRSA sepsis has been excluded. Linezolid is a reasonable alternative if there are contraindications to vancomycin. After culture results and antimicrobial susceptibility data return, we recommend that therapy be pathogen- and susceptibility-directed, even if there has been clinical improvement while on the initial antimicrobial regimen. Gram-negative pathogens have historically been covered with two agents from different antibiotic classes. However, several clinical trials and two meta-analyses have failed to demonstrate superior overall efficacy of combination therapy compared to monotherapy with a third generation cephalosporin or a carbapenem [55,63-67]. Furthermore, one meta-analysis found double coverage was associated with an increased incidence of adverse events [66,67]. For this reason, we recommend use of a single agent with proven efficacy and the least possible toxicity, except in patients who are either neutropenic or whose severe sepsis is due to a known or suspected Pseudomonas infection [7,65]. (See Pseudomonas aeruginosa bacteremia and endocarditis and Treatment of Pseudomonas aeruginosa infections .) Regardless of the antibiotic regimen selected, patients should be observed closely for toxicity, evidence of response, and the development of nosocomial superinfection [68]. The duration of therapy is typically 7 to 10 days, although longer courses may be appropriate in patients who have a slow clinical response, an undrainable focus of infection, or immunologic deficiencies [7]. In patients who are neutropenic, antibiotic treatment should continue until the neutropenia has resolved. In non-neutropenic patients in whom infection is thoroughly excluded, antibiotics should be discontinued to minimize colonization or infection with drug-resistant microorganisms and superinfection with other pathogens. Schmitd Uptodate")
33
Scelta appropriata della ATB nella sepsi
E’ decisiva nelle infezioni gravi e deve essere: RAPIDA (1 h) ma dopo una opportuna ricerca microbiologica (BAL, emocolture…) “Hit early” APPROPRIATA: Spettro allargato “Hit hard” Ricercare il sito di infezione e fattori predisponenti (Rx – ecografie….) Modificare la terapia quando disponibile un dato colturale compatibile (DE-ESCALING) Un ampio numero di pazienti con la sepsi non avrà comunque un isolamento microbiologico
 ma dopo una opportuna ricerca microbiologica (BAL, emocolture…) Hit early APPROPRIATA: Spettro allargato Hit hard Ricercare il sito di infezione e fattori predisponenti (Rx – ecografie….) Modificare la terapia quando disponibile un dato colturale compatibile (DE-ESCALING) Un ampio numero di pazienti con la sepsi non avrà comunque un isolamento microbiologico.")
34
Interventi di gestione successiva e terapie addizionali
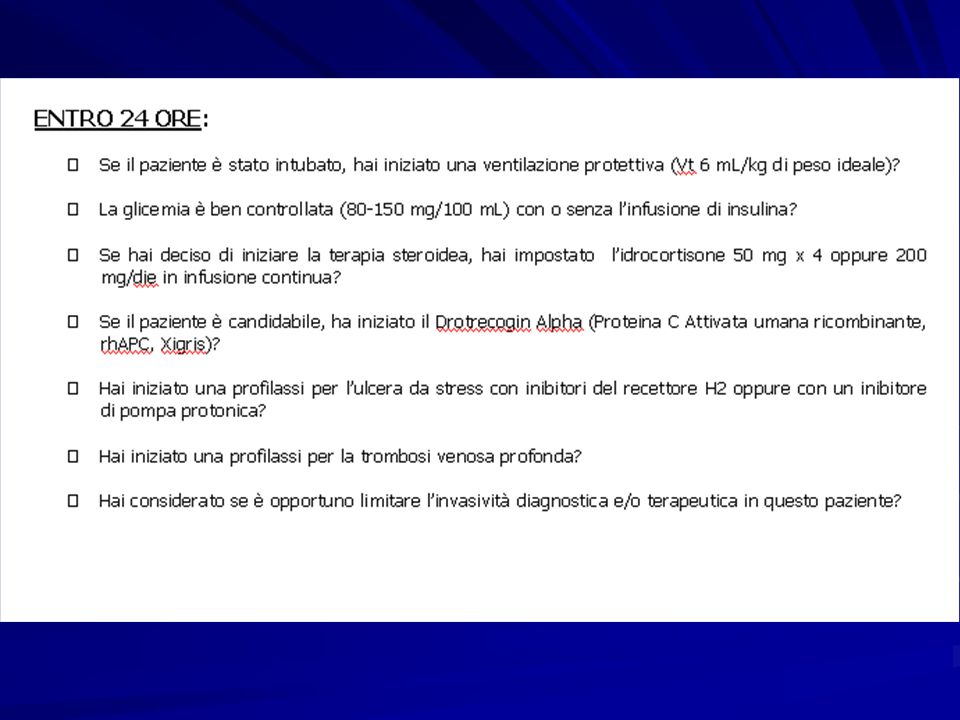
Steroidi se shock rhAPC Entro le prime 24 h ALI = adullt lung injury Ventilazione protettiva se ALI/ARDS Glicemia <150 mg/dl

35
Terapie addizionali Corticosteroidi :
Idrocortisone mg/die solo se ipotensione < 90 mmHg malgrado fluidi e vasopressori (GRADE2B) Durata 5-7 gg , tapering opzionale (GRADE2C) Recombinant human activated protein C (rhAPC, also called drotrecogin alfa) is a protein that promotes fibrinolysis and inhibits thrombosis. The initial clinical trials that evaluated the effects of rhAPC in sepsis were prompted by three major observations: sepsis induces a procoagulant response, rhAPC modulates procoagulant effects, and protein C supplementation may benefit patients with purpura fulminans [1-4]. Despite the large body of evidence that has accumulated since the earliest trials, the balance of potential desirable and undesirable effects remains controversial and is the subject of ongoing clinical research. GRADE 2b = evidenza debole moderata
 Durata 5-7 gg , tapering opzionale (GRADE2C) Recombinant human activated protein C (rhAPC, also called drotrecogin alfa) is a protein that promotes fibrinolysis and inhibits thrombosis. The initial clinical trials that evaluated the effects of rhAPC in sepsis were prompted by three major observations: sepsis induces a procoagulant response, rhAPC modulates procoagulant effects, and protein C supplementation may benefit patients with purpura fulminans [1-4]. Despite the large body of evidence that has accumulated since the earliest trials, the balance of potential desirable and undesirable effects remains controversial and is the subject of ongoing clinical research. GRADE 2b = evidenza debole moderata.")
36
Meccanismi di azione di RhAPC
Anticoagulante Fibrinolitico Antinfiammatorio Bernard GR et al. NEJM 2001; 344: 699

37
Terapie addizionali RhAPC ( drotrecogin alfa) : modula la risposta procoagulante alle infezioni Usarla solo se sepsi grave o shock settico con danno multiplo di organo (APACHE > 25) (GRADE 2B)(2C se chirurgici) Se usata, meglio entro h No se rischio emorragico (PP < 30000, sanguinamenti in atto, epatopatia grave, patologia intracranica, scoagulazione) Recombinant human activated protein C (rhAPC, also called drotrecogin alfa) is a protein that promotes fibrinolysis and inhibits thrombosis. The initial clinical trials that evaluated the effects of rhAPC in sepsis were prompted by three major observations: sepsis induces a procoagulant response, rhAPC modulates procoagulant effects, and protein C supplementation may benefit patients with purpura fulminans [1-4]. Despite the large body of evidence that has accumulated since the earliest trials, the balance of potential desirable and undesirable effects remains controversial and is the subject of ongoing clinical research. Dellinger Crit.Care Med 2008
 (GRADE 2B)(2C se chirurgici) Se usata, meglio entro h. No se rischio emorragico (PP < 30000, sanguinamenti in atto, epatopatia grave, patologia intracranica, scoagulazione) Recombinant human activated protein C (rhAPC, also called drotrecogin alfa) is a protein that promotes fibrinolysis and inhibits thrombosis. The initial clinical trials that evaluated the effects of rhAPC in sepsis were prompted by three major observations: sepsis induces a procoagulant response, rhAPC modulates procoagulant effects, and protein C supplementation may benefit patients with purpura fulminans [1-4]. Despite the large body of evidence that has accumulated since the earliest trials, the balance of potential desirable and undesirable effects remains controversial and is the subject of ongoing clinical research. Dellinger Crit.Care Med")
38
Terapie addizionali Controllo glicemico Target 140-180 mg/dL
Nutrizione Fabbisogno calorico aumentato nel paziente settico : usare 20Kcal/kg/die nella prima settimana con 1.5 g/kg proteine/die e poi 30 Kcal/kg/die Preferire NE a meno di peritoniti diffuse, vomito incoercibile, diarrea profusa, ileo paralitico e insufficienza intestinale Precoce somministrazione ( h) Decubito con elevazione della testa di 30° per prevenzione ab ingestis La richiesta calorica del paziente critico nella prima settimana è pari a kcal/kg/die, mentre nei pazienti settici il fabbisogno cresce fino a 35 kcal/kg/die a partire dalla seconda settimana Sulla base di queste osservazioni, lo schema nutrizionale proposto per la maggior parte dei pazienti prevede 20 kcal/kg/die durante la prima settimana e successivamente l’incremento fino a 30 kcal/kg/die in caso di sepsi. Da evitare fenomeni di apporto calorico eccessivo, il quale può alterare i precari equilibri metabolici del paziente critico. Una nutrizione eccessivamente ricca di carboidrati, infatti, determina un aumento della produzione di CO2, con aumento del lavoro respiratorio necessario per eliminarla. Pertanto, la somministrazione di proteine e calorie non proteiche deve essere attuata con gradualità e in modo progressivo fino al raggiungimento del fabbisogno stabilito e non deve prescindere dal supplemento di vitamine (A, C, gruppo B, K, E), oligoelementi (selenio, zinco) ed elettroliti (magnesio, fosforo). I fabbisogni nutrizionali possono essere soddisfatti attraverso il tratto digestivo con la nutrizione enterale (EN) o, attraverso una via venosa, con la nutrizione parenterale (PN) Dellinger Crit.Care Med 2008
 Decubito con elevazione della testa di 30° per prevenzione ab ingestis. La richiesta calorica del paziente critico nella prima settimana è. pari a kcal/kg/die, mentre nei pazienti settici il fabbisogno. cresce fino a 35 kcal/kg/die a partire dalla seconda settimana. Sulla base di queste osservazioni, lo schema nutrizionale. proposto per la maggior parte dei pazienti prevede 20. kcal/kg/die durante la prima settimana e successivamente l’incremento. fino a 30 kcal/kg/die in caso di sepsi. Da evitare. fenomeni di apporto calorico eccessivo, il quale può alterare. i precari equilibri metabolici del paziente critico. Una nutrizione. eccessivamente ricca di carboidrati, infatti, determina un. aumento della produzione di CO2, con aumento del lavoro respiratorio. necessario per eliminarla. Pertanto, la somministrazione. di proteine e calorie non proteiche deve essere attuata. con gradualità e in modo progressivo fino al raggiungimento. del fabbisogno stabilito e non deve prescindere dal. supplemento di vitamine (A, C, gruppo B, K, E), oligoelementi. (selenio, zinco) ed elettroliti (magnesio, fosforo). I fabbisogni nutrizionali possono essere soddisfatti attraverso. il tratto digestivo con la nutrizione enterale (EN) o, attraverso. una via venosa, con la nutrizione parenterale (PN) Dellinger Crit.Care Med")
39
Terapie addizionali Disfunzione renale e dialisi
Equivalenti la dialisi intermittente e la CVVH, preferibile nel paziente con instabilità emodinamica Inutile usare Bicarbonato per trattare ipoperfusione con lattacidemia e pH > 7,15 Profilassi di TVP Usare UHF o LMWH se non controindicati Usare calze compressive se anticoagulanti controindicati Usare entrambi se alto rischio di TVP Profilassi di ulcera da stress AntiH2 ev o PPI ev con benefici da bilanciare con maggior rischio di polmoniti da VAM Dellinger Crit.Care Med 2008

40
Terapie addizionali Emoderivati Non raccomandata ATIII
Piastrine se < 5000/mm3 anche senza sanguinamento Tra 5000 e solo se rischio alto di sanguinamento Garantire > se necessaria procedura chirurgica o invasiva Target Hb 7- 9 g/dL (1B) , > se ischemia miocardica , ipossiemia severa Ventilazione Meccanica se ALI/ARDS indotte da sepsi (P/F < 300) Tidal volume bassi : 6 mL/kg di peso corporeo ideale (1B) P plateau < 30 cm H2O Consentire paCO2 > per minimizzare Tidal e P plateau (1C) ALI = acute lung injuri Dellinger Crit.Care Med 2008
 , > se ischemia miocardica , ipossiemia severa. Ventilazione Meccanica se ALI/ARDS indotte da sepsi (P/F < 300) Tidal volume bassi : 6 mL/kg di peso corporeo ideale (1B) P plateau < 30 cm H2O. Consentire paCO2 > per minimizzare Tidal e P plateau (1C) ALI = acute lung injuri. Dellinger Crit.Care Med")
41
Sepsi team ! Check list !

47
SEPSI ATB empirica sec . patologia De Gaudio GIC 2010; 11;274

48
SEPSI ATB empirica sec . patologia De Gaudio GIC 2010; 11;274







 ha smesso nel Impiegato. Diabete mellito tipo 2 noto dal 1993, in trattamento con ipoglicemizzanti.>")















 RELATORE DR. ADOLFO.>")