Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
e strategie di trattamento
Anemia, insufficienza renale e scompenso cardiaco: patogenesi comune e strategie di trattamento Gessica Italiani, Cardiologia Pescia

2
Insuff. Ventricolare sx
STADI MALATTIA RENALE e CARDIOVASCOLARE Insuff. Renale cronica terminale Scompenso cardiaco Stadio finale Insuff. Renale Cronica (FG) Eventi/malattia cardiovascolare Progressione Albuminuria Proteinuria Insuff. Ventricolare sx Inizio Più volte è stato sottolineato che la malattia cardiovascolare è molto simile a quella renale cronica nei vari stadi evolutivi. Età, obesità Diabete Mellito, Ipertensione Età, obesità Diabete Mellito, Ipertensione “A rischio” Malattia Renale Cronica Malattia Cardiovascolare Sarnak MJ & Levey AS, Am J Kidney Dis, 2000
 Eventi/malattia cardiovascolare. Progressione. Albuminuria. Proteinuria. Insuff. Ventricolare sx. Inizio. Più volte è stato sottolineato che la malattia cardiovascolare è molto simile a quella renale cronica nei vari stadi evolutivi. Età, obesità. Diabete Mellito, Ipertensione. Età, obesità. Diabete Mellito, Ipertensione. A rischio Malattia Renale Cronica. Malattia Cardiovascolare. Sarnak MJ & Levey AS, Am J Kidney Dis,")
3
INSUFFICIENZA RENALE CRONICA
CARDIACA CRONICA

4
Alta morbidità e mortalità
INSUFFICIENZA CARDIACA e INSUFFICIENZA RENALE Alta prevalenza Alta morbidità e mortalità Alti costi Singolarmente Invecchiamento popolazione > Incidenza diabete, obesità, IA, altri fattori di rischio Cause

5
PREVALENZA ASSOCIAZIONE IR-IC
Registro Scompenso Cardiaco Acuto

7
FATTORI di RISCHIO CV TRADIZIONALI CORRELATI A IRC Età avanzata
Sesso maschile Ipertensione Ipertrofia ventricolare sinistra Dislipidemia Diabete mellito Fumo Inattività fisica Menopausa Storia familiare di CVD Sovraccarico volume liquido extracellulare (ECFV) Anemia Alterato metabolismo Ca/P Infiammazione/Malnutrizione Stress ossidativo Iperomocisteinemia Fattori trombogenici Proteinuria Sono elencati i fattori di rischio tradizionali e quelli correlati con l’IRC. Modificato da Am J Kidney Disease 39 (S 1): 2002
 Anemia. Alterato metabolismo Ca/P. Infiammazione/Malnutrizione. Stress ossidativo. Iperomocisteinemia. Fattori trombogenici. Proteinuria. Sono elencati i fattori di rischio tradizionali e quelli correlati con l’IRC. Modificato da Am J Kidney Disease 39 (S 1):")
8
Sottogruppo (972 pz) del PRIME II
LEVF NYHA

9
Metanalisi su 53460 pazienti

10
Sindrome Cardiorenale: definizione
Section 2: Pathophysiology of Acute Decompensated Heart Failure Sindrome Cardiorenale: definizione Interazione tra RENI ed altri compartimenti circolatori Aumento del volume circolante Peggioramento del compenso Accelerazione della progressione di malattia “Cardiorenal Dysregulation”: la terapia per ridurre la congestione non funziona per ulteriore declino della funzione renale1 Cardiorenal syndrome is a general term that is frequently used to describe the often dysfunctional interaction between the heart and the kidney in ADHF. There does not exist a consensus definition of this term, however a recent group of investigators1 led by Lynne Warner Stevenson convened to try and further characterize this interaction. Interactions between the heart and the kidney have been garnering increasing focus because of epidemiological evidence indicating that even a mild deterioration of renal function is an important risk factor for poor outcome in patients with congestive HF. NHLBI Working Group: Cardio-Renal Connections in Heart Failure and Cardiovascular Disease, August 20, 2004 Executive Summary The National Heart, Lung, and Blood Institute convened a Working Group of investigators on August 20, 2004, in McLean, Virginia, to evaluate the current state of knowledge regarding interactions between the cardiovascular system and the kidney, to identify critical gaps in our knowledge, understanding, and application of research tools, and to develop specific recommendations for NHLBI in cardiorenal interactions related to HF and other cardiovascular diseases such as congenital heart disease. Discussion The Working Group focused on cardiorenal connections in which abnormalities of cardiac function were not preceded by a known diagnosis of chronic kidney disease, such that acute and chronic renal responses are due to primary impairment of cardiac function. Among patients hospitalized for decompensated HF, worsening renal function predicts adverse cardiovascular outcomes. Since these patients are routinely excluded, clinical HF trials provide little evidence or information on which to base therapy for HF patients experiencing worsening renal function. As a result, treatment for these patients is largely empirical. The lack of formal interaction across clinical disciplines, with insight into the diverse factors that affect both cardiac and renal function, has also limited our recognition, understanding, and potential therapies for cardiorenal dysregulation in HF. New and effective therapies need to be identified for the treatment and prevention of this challenging syndrome. The deliberations and considerations of this Working Group should broaden the perspective and enhance understanding across traditional specialty boundaries. A working definition of cardiorenal dysregulation was introduced and served as the basis of subsequent discussion and recommendations. In HF, it is the result of interactions between the kidneys and other circulatory compartments that increase circulating volume and symptoms of heart failure and disease progression are exacerbated. Continued on next page NHLBI Working Group. April 30, 2005.

11
Fisiopatologia Sindrome Cardiorenale
La ritenzione idroelettrolitica compensa la riduzione del “volume ematico efficace” dovuta al deficit di pompa (relazione di Frank Starling). Quando l’espansione di volume non riesce più a sopperire al deficit di pompa si sviluppa congestione sistemica
. Quando l’espansione di volume non riesce più a sopperire al deficit di pompa si sviluppa congestione sistemica.")
12
Bongartz, L. G. et al. Eur Heart J 2005 26:11-17
GUYTON MODEL

13
La Sindrome Cardiorenale
Section 2: Pathophysiology of Acute Decompensated Heart Failure Disfunzione VS Terapia Diuretica Aumento Morbidità E Mortalità Attivazione Neurormonale Sviluppo di Diuretico resistenza Diminuito Flusso Disfunzione Renale Diminuita Perfusione Renale

14
Scompenso Cardiaco Acuto
Section 2: Pathophysiology of Acute Decompensated Heart Failure Scompenso Cardiaco Acuto Insult Cardiac Dysfunction LV Remodeling Neurohormonal Activation RAAS Catecholamine Endothelin Hemodynamic Decompensation Preload Afterload Cardiac Output This diagram shows the relationship between the primary myocardial insult and subsequent events that contribute to the clinical syndrome of CHF.1 The pathophysiology of HF involves hemodynamic abnormalities, neurohumoral abnormalities, and myocardial cellular alterations. Left ventricular (LV) dysfunction results from myocardial injury. Neurohumoral activation, which includes activation of the sympathetic nervous system (SNS) and the renin-angiotensin-aldosterone system (RAAS), occurs in response to acute hemodynamic alterations and myocardial injury. This neurohumoral activation is counterproductive in patients with HF. Changes occur in cardiac function and peripheral circulation that contribute to the symptoms and drive the progression of HF. Neurohumoral activation results in an excess of vasoconstrictors—those in the SNS and the RAAS, as well as endothelin—which increase afterload and preload by retention of salt and water. Vasodilators—hormones in the endogenous natriuretic peptide system (NPS)—work to unload the left ventricle and promote natriuretic actions, but they are overwhelmed by the excess of vasoconstricting neurohomones. Vasodilators are ultimately beneficial counterregulatory hormones.2-4 Neurohumoral activation results in progressive dilation and dysfunction of the left ventricle (remodeling). There are also fundamental abnormalities at the cellular level, including myocyte dysfunction, programmed cell death (apoptosis), fetal gene expression, hypertrophy, and myocardial fibrosis.5 Other circulating proinflammatory cytokines, such as interleukin-6 and TNF-alpha, can lead to a progressive wasting of lean tissue, fat, and bone mass.4 Based on this model, hemodynamic decompensation and neurohormonal activation may give rise to either acute impairment of LV function or chronic progression of disease, or both, in a vicious cycle. References: Colucci WS, Braunwald E. In: Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine. 5th ed. Philadelphia: Saunders; 1997: Stevenson W. J Am Coll Cardiol. 2005;45: Weber. J Am Coll Cardiol. 2004:44(6): Anker et al. Am J Cardiol. 1999;83: Shah M et al. Rev Cardiovasc Med. 2001;2(suppl 2):S2-S6. Renal Vasoconstriction/Fluid Retention Fluid Overload Symptoms Morbidity Death Colucci WS, Braunwald E. Heart Disease: A Textbook of Cardiovascular Medicine. 5th ed. 1997:394.
 dysfunction results from myocardial injury. Neurohumoral activation, which includes activation of the sympathetic nervous system (SNS) and the renin-angiotensin-aldosterone system (RAAS), occurs in response to acute hemodynamic alterations and myocardial injury. This neurohumoral activation is counterproductive in patients with HF. Changes occur in cardiac function and peripheral circulation that contribute to the symptoms and drive the progression of HF. Neurohumoral activation results in an excess of vasoconstrictors—those in the SNS and the RAAS, as well as endothelin—which increase afterload and preload by retention of salt and water. Vasodilators—hormones in the endogenous natriuretic peptide system (NPS)—work to unload the left ventricle and promote natriuretic actions, but they are overwhelmed by the excess of vasoconstricting neurohomones. Vasodilators are ultimately beneficial counterregulatory hormones.2-4. Neurohumoral activation results in progressive dilation and dysfunction of the left ventricle (remodeling). There are also fundamental abnormalities at the cellular level, including myocyte dysfunction, programmed cell death (apoptosis), fetal gene expression, hypertrophy, and myocardial fibrosis.5 Other circulating proinflammatory cytokines, such as interleukin-6 and TNF-alpha, can lead to a progressive wasting of lean tissue, fat, and bone mass.4 Based on this model, hemodynamic decompensation and neurohormonal activation may give rise to either acute impairment of LV function or chronic progression of disease, or both, in a vicious cycle. References: Colucci WS, Braunwald E. In: Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine. 5th ed. Philadelphia: Saunders; 1997: Stevenson W. J Am Coll Cardiol. 2005;45: Weber. J Am Coll Cardiol. 2004:44(6): Anker et al. Am J Cardiol. 1999;83: Shah M et al. Rev Cardiovasc Med. 2001;2(suppl 2):S2-S6. Renal Vasoconstriction/Fluid Retention. Fluid Overload Symptoms. Morbidity. Death. Colucci WS, Braunwald E. Heart Disease: A Textbook of Cardiovascular Medicine. 5th ed. 1997:394.")
15
Fisiopatologia Sindrome cardio renale
Dal 27% al 45% dei pazienti con scompenso cardiaco in stadio III-IV mostrano peggioramento acuto della funzione renale Il monitoraggio emodinamico dimostra che la riduzione acuta della funzione renale non dipende da un diminuito output cardiaco AHJ , AGOSTO 1999, J Card Fail SMITH GL et al.

16
Fisiopatologia Sindrome cardio renale
Riduzione dell’attività dei peptidi natriuretici: baroreceptor adaptation con ridotta sensibilità Potenziamento RAAS Peggioramento IPONATRIEMIA (concausa i diuretici): fattore prognostico negativo
: fattore prognostico negativo.")
17
Manifestazioni Cliniche e Mortalità
Iponatriemia Manifestazioni Cliniche e Mortalità Cefalea Irritabilità Nausea e Vomito Confusione mentale Disorientamento Stupor/Coma Convulsioni Arresto Respiratorio

18
TAC cerebrale Normale Iponatriemia fatale

19
Admitted Patients and Volume Overload
Section 1: Epidemiology and Demographics At Hospitalization—ADHERE®1 Any dyspnea – 89% Pulmonary congestion (CXR) – 74% Rales – 67% Dyspnea at rest – 34% Peripheral edema – 65% Data from the ADHERE (Acute Decompensated Heart Failure National Registry) study show a high percentage of patients at time of admission have symptoms of both pulmonary congestion and volume overload.1,2 References: The ADHERE Registry. First Quarter National Benchmark Registry Fremont, CA: Scios Inc; 2003. 2. Friedman MM. Older adults’ symptoms and their duration before hospitalization for heart failure Heart Lung. 1997;26: The Majority of These Patients Have Failed Treatment With Oral Diuretics2 ADHERE Registry. 3rd Qtr 2003 National Benchmark Report. 2. Adams et al. Am Heart J. 2005;149:
 – 74% Rales – 67% Dyspnea at rest – 34% Peripheral edema – 65% Data from the ADHERE (Acute Decompensated Heart Failure National Registry) study show a high percentage of patients at time of admission have symptoms of both pulmonary congestion and volume overload.1,2. References: The ADHERE Registry. First Quarter National Benchmark Registry. Fremont, CA: Scios Inc; Friedman MM. Older adults’ symptoms and their duration before hospitalization for heart failure. Heart Lung. 1997;26: The Majority of These Patients Have Failed Treatment With Oral Diuretics2. ADHERE Registry. 3rd Qtr 2003 National Benchmark Report. 2. Adams et al. Am Heart J. 2005;149:")
20
TERAPIA: Diuretici Ridurre il volume del fluido extracellulare (FEC) incrementando l’eliminazione di urine, in particolare di SODIO, principale determinante del FEC.
 incrementando l’eliminazione di urine, in particolare di SODIO, principale determinante del FEC.")
21
Con i diuretici è rimovibile al massimo il 20% del carico filtrato di SODIO
Brater D; Am J Med Sci 2000

22
Aumento Neurormoni provoca Diuretico-Resistenza
Section 3: Diuretic Therapy in Acute Decompensated Heart Failure Glomerulo Norepinephrine (and endothelin) diminuiscono il flusso renale e GRF Tubulo prossimale Ang II aumenta il riassorbimento di sodio There are 2 types of diuretic resistance—short-term tolerance (“braking”), which may be mediated by activation of angiotensin II (Ang II) or the sympathetic nervous system (SNS), or long-term tolerance, in which sodium that escapes the loop of Henle is reabsorbed at more distal sites, decreasing overall diuresis; this may be overcome with sequential diuretic blockade.1 Diuretic insensitivity and resistance are conferred largely by activation of various neurohormonal systems. Ang II and renal nerve stimulation activate receptors on the proximal tubule epithelium,2,3 causing proximal tubular reabsorption of water and sodium, which decreases availability of substrates for loop and thiazide diuretics. Catecholamines (eg, norepinephrine) and endothelin, which mediate some of the renal actions of Ang II, also may decrease renal blood flow and consequently can decrease delivery of diuretics to tubules. Nearly all diuretics must be filtered by the glomeruli to reach their (intraluminal) transport mechanism.4 References: 1. Brater DC. N Engl J Med. 1998:339:387. 2. Riggleman A et al. Hypertension. 2001;38:105. 3. Bell-Reuss E et al. Effect of renal sympathetic nerve stimulation on proximal water and sodium reabsorption. J Clin Invest. 1976;57: 4. Myers BD et al. Effects of norepinephrine and angiotensin II on the determinants of glomerular ultrafiltration and proximal tubule fluid reabsorption in the rat. Circ Res. 1983;37: Dotto Collettore Aldosterone aumenta il riassorbimento di sodio Krämer et al. Am J Med. 1999;106:90.
 diminuiscono il flusso renale e GRF. Tubulo prossimale. Ang II aumenta il riassorbimento di sodio. There are 2 types of diuretic resistance—short-term tolerance ( braking ), which may be mediated by activation of angiotensin II (Ang II) or the sympathetic nervous system (SNS), or long-term tolerance, in which sodium that escapes the loop of Henle is reabsorbed at more distal sites, decreasing overall diuresis; this may be overcome with sequential diuretic blockade.1. Diuretic insensitivity and resistance are conferred largely by activation of various neurohormonal systems. Ang II and renal nerve stimulation activate receptors on the proximal tubule epithelium,2,3 causing proximal tubular reabsorption of water and sodium, which decreases availability of substrates for loop and thiazide diuretics. Catecholamines (eg, norepinephrine) and endothelin, which mediate some of the renal actions of Ang II, also may decrease renal blood flow and consequently can decrease delivery of diuretics to tubules. Nearly all diuretics must be filtered by the glomeruli to reach their (intraluminal) transport mechanism.4. References: 1. Brater DC. N Engl J Med. 1998:339: Riggleman A et al. Hypertension. 2001;38: Bell-Reuss E et al. Effect of renal sympathetic nerve stimulation on proximal water and sodium reabsorption. J Clin Invest. 1976;57: Myers BD et al. Effects of norepinephrine and angiotensin II on the determinants of glomerular ultrafiltration and proximal tubule fluid reabsorption in the rat. Circ Res. 1983;37: Dotto Collettore. Aldosterone aumenta il riassorbimento di sodio. Krämer et al. Am J Med. 1999;106:90.")
23
Diuretico-resistenza
Section 3: Diuretic Therapy in Acute Decompensated Heart Failure Diuretico-resistenza Riduzione o perdita della diuresi prima del raggiungimento del goal terapeurico di risoluzione dell’edema1 20%–30% dei pazienti con SC2 1. Kramer et al. Nephrol Dial Transplant. 1999;14(suppl 4):39-42. 2. Ellison. Cardiology. 2001;96: . CAUSE: Fenomeno del “Braking” Riduzione della risposta diuretica dopo la prima dose Tolleranza nel lungo termine Ipertrofia tubulare compensatoria alla perdita di sali There is no consensus definition of diuretic resistance; however, it has been described as a clinical state in which the diuretic response is diminished or lost before the therapeutic goal of relief from edema has been reached. This may be mediated by the “braking” phenomenon.1 20% to 30% of all patients with HF develop diuretic resistance.2 References: Kramer et al. Nephrol Dial Transplant. 1999;14(suppl 4):39-42. Ellison. Cardiology. 2001;96: Brater. N Engl J Med. 1998;339:387.
: Ellison. Cardiology. 2001;96: CAUSE: Fenomeno del Braking Riduzione della risposta diuretica dopo la prima dose. Tolleranza nel lungo termine. Ipertrofia tubulare compensatoria alla perdita di sali. There is no consensus definition of diuretic resistance; however, it has been described as a clinical state in which the diuretic response is diminished or lost before the therapeutic goal of relief from edema has been reached. This may be mediated by the braking phenomenon.1. 20% to 30% of all patients with HF develop diuretic resistance.2. References: Kramer et al. Nephrol Dial Transplant. 1999;14(suppl 4): Ellison. Cardiology. 2001;96: Brater. N Engl J Med. 1998;339:387.")
24
5

25
METODICHE DIALITICHE CONTINUE (CRRT)
Le CRRT sono tutti i trattamenti extracorporei intesi a sostituire la funzione renale insufficiente per un periodo di almeno 24 ore. “DIALISI”: movimenti di soluti in concentrazioni diverse, per depurare ed eliminare fluidi in eccesso utilizzando una membrana semipermeabile. I principi chimico – fisici in gioco nelle CRRT sono: Differenza di concentrazione delle sostanze ai due lati della membrana (DIFFUSIONE) Pressione idrostatica del liquido da filtrare (ULTRAFILTRAZIONE/CONVEZIONE)
 Pressione idrostatica del liquido da filtrare (ULTRAFILTRAZIONE/CONVEZIONE)")
26
DIFFUSIONE

27
Storia dell’Ultrafiltrazione
Section 4: Ultrafiltration History and Physiology Storia dell’Ultrafiltrazione 1974: Silverstein described solitary ultrafiltration on 5 ESRD patients via a modified dialysis circuit3 1949: Schneierson proposed intermittent peritoneal dialysis for refractive ADHF1 1940 1950 1960 1970 1980 1954: Kolff noted that ultrafiltration could be used for a “reduction of intractable edema”2 1979: Paganini and others reported the practical application of ultrafiltration in a volume-overloaded patient4 Ultrafiltration in its many forms (ie, peritoneal, isolated ultrafiltration via a dialysis model) as a therapeutic option for refractory ADHF has been historically evident for over 50 years. A literature review1 counted 115 published case reports that gathered patients with or without concurrent renal failure who were treated with peritoneal dialysis for refractory ADHF. Several other examples exist, as described in this slide, of isolated ultrafiltration administered in the edematous patient. Ensuing slides list various references of over 50 studies where ultrafiltration has been used in patients with refractory edema. In 1949, Schneierson proposed that peritoneal dialysis be used in a patient with refractory congestive HF. Regression of congestive HF was noted, followed by the observation of enhanced response to diuretics.2 2. “The concept of the extracorporeal removal of fluid with UF has been reported for over 50 years” and can be used for the “reduction of otherwise intractable edema by dialysis or filtration.” This was opined by Willem Kolff—who to some is considered the father of dialysis—who developed the first artificial kidney in Dr Kolff went on to design the heart–lung machine that made open-heart surgery possible. He has pioneered artificial eyes, ears, and arms, and for 25 years led the effort to develop the artificial heart. In 1982, a heart designed under his supervision was successfully implanted in Barney Clark, an event that captured the imagination of the world. 3,4 3. Silverstein described, for the first time, the use of solitary ultrafiltration in 5 current patients with end-stage renal disease (ESRD). He noted that a certain subset of patients would continue to have persistent edema despite being treated with fluid and dietary salt restriction. Ultrafiltration was completed utilizing a modified circuit with applied transmembrane pressure of 200 mmHG, with ultrafiltration rates of between 200 to 800 mL. He further observed that this was a safe procedure and that the ultrafiltrate components were identical to plasma; thus electrolyte imbalances from diuretic therapy such as hypokalemia, hypocalcemia, hyperuricemia, or contraction metabolic alkalosis would be avoided.5 Continued on next page 1. Schneierson SJ. Am J Med Soc. 1949;298. 2. Kolff et al. Cleve Clin Q. 1954;21. 3. Silverstein et al. N Engl J Med. 1974;291: 4. Paganini et al. Adv Ren Replace Ther. 1996;3:
 as a therapeutic option for refractory ADHF has been historically evident for over 50 years. A literature review1 counted 115 published case reports that gathered patients with or without concurrent renal failure who were treated with peritoneal dialysis for refractory ADHF. Several other examples exist, as described in this slide, of isolated ultrafiltration administered in the edematous patient. Ensuing slides list various references of over 50 studies where ultrafiltration has been used in patients with refractory edema. In 1949, Schneierson proposed that peritoneal dialysis be used in a patient with refractory congestive HF. Regression of congestive HF was noted, followed by the observation of enhanced response to diuretics The concept of the extracorporeal removal of fluid with UF has been reported for over 50 years and can be used for the reduction of otherwise intractable edema by dialysis or filtration. This was opined by Willem Kolff—who to some is considered the father of dialysis—who developed the first artificial kidney in Dr Kolff went on to design the heart–lung machine that made open-heart surgery possible. He has pioneered artificial eyes, ears, and arms, and for 25 years led the effort to develop the artificial heart. In 1982, a heart designed under his supervision was successfully implanted in Barney Clark, an event that captured the imagination of the world. 3,4. 3. Silverstein described, for the first time, the use of solitary ultrafiltration in 5 current patients with end-stage renal disease (ESRD). He noted that a certain subset of patients would continue to have persistent edema despite being treated with fluid and dietary salt restriction. Ultrafiltration was completed utilizing a modified circuit with applied transmembrane pressure of 200 mmHG, with ultrafiltration rates of between 200 to 800 mL. He further observed that this was a safe procedure and that the ultrafiltrate components were identical to plasma; thus electrolyte imbalances from diuretic therapy such as hypokalemia, hypocalcemia, hyperuricemia, or contraction metabolic alkalosis would be avoided.5. Continued on next page. 1. Schneierson SJ. Am J Med Soc. 1949; Kolff et al. Cleve Clin Q. 1954; Silverstein et al. N Engl J Med. 1974;291: Paganini et al. Adv Ren Replace Ther. 1996;3:")
28
Utilizzo in Cardiologia
SCUF: Ultrafiltrazione lenta continua Rimozione di quantità elevate di liquidi dove non siano richieste necessità di depurazione. Rimuove liquido ISOTONICO rispetto al plasma (Es: SE RIMUOVO 2 LITRI DI ACQUA IN UN PAZIENTE CON NA+ DI 130 MEQ/L RIMUOVERÒ 130X2 MEQ DI SODIO) CVVHDF: Emodiafiltrazione veno-venosa continua Utilizza DIFFUSIONE E CONVEZIONE. Rimuove piccole e medie molecole dal sangue. E’ la tecnica più utilizzata. Rimozione indipendente di sodio e acqua (Esempio: POSSO RIMUOVERE 10 LITRI DI ACQUA SENZA DOVER RIMUOVERE 130X10 MEQ DI NA+)
 CVVHDF: Emodiafiltrazione veno-venosa continua. Utilizza DIFFUSIONE E CONVEZIONE. Rimuove piccole e medie molecole dal sangue. E’ la tecnica più utilizzata. Rimozione indipendente di sodio e acqua. (Esempio: POSSO RIMUOVERE 10 LITRI DI ACQUA SENZA DOVER RIMUOVERE 130X10 MEQ DI NA+)")
29
Effetti Emodinamici dell’UF nello SC
Section 4: Ultrafiltration History and Physiology Effetti Emodinamici dell’UF nello SC CO (L/m) SV (mL) 5.0 – 4.0 – 3.0 – 2.0 – 70 – 60 – 50 – 40 – 30 – Before UF 1 liter 2 liter 3 liter 4 liter After UF 24h after UF Before UF 1 liter 2 liter 3 liter 4 liter After UF 24h after UF RAP (mmHg) PWP (mmHg) This study by Marenzi et al (brief description below) demonstrates that ultrafiltration of more than 4 L of plasma water over approximately 9 h reduced mean arterial pressures and pulmonary wedge pressure (PWP).1 Cardiac output increased at the end of the session and was shown to decrease further 24 h after ultrafiltration was completed. Moreover during treatment, heart rate, systemic arterial pressure, cardiac output, and systemic vascular resistances did not change. Further details: The goal of the study was to investigate the hemodynamic and circulatory adjustments to extracorporeal ultrafiltration in refractory congestive HF. Twenty-four patients (18 men and 6 women)—Class IV ADHF, with signs and symptoms of volume overload, >5 kg weight gain within 1 month—were allowed to continue on digoxin, diuretics (24 of 24 patients), and angiotensin-converting enzyme inhibitors (15 of 24 patients). A continuous renal replacement therapy (CRRT) device was utilized to remove fluid, and hemodynamic measurements were taken after 1 L, 2 L, 3 L, and 4 L ultrafiltration, and then 24 h after ultrafiltration had ceased. The mean duration of ultrafiltration was 9 ± 3 h, and total volume removed was 4880 L ± 896 mL. Urine output and NYHA association class improved. Response to diuretics improved from 380 ± 157 mg/day to 112 ± 70 mg/day beginning the day after ultrafiltration started. Reference: 1. Marenzi et al. Circulatory response to fluid overload by extracoporeal ultrafiltration in refractory congestive heart failure. J Am Coll Cardiol. 2001;38: 25 – 20 – 15 – 10 – 5 – 0 - 30 – 25 – 20 – 15 – 10 - Before UF 1 liter 2 liter 3 liter 4 liter After UF 24h after UF Before UF 1 liter 2 liter 3 liter 4 liter After UF 24h after UF Marenzi et al. J Am Coll Cardiol. 2001;38:
 SV (mL) 5.0 – 4.0 – 3.0 – 2.0 – 70 – 60 – 50 – 40 – 30 – Before. UF. 1. liter. 2. liter. 3. liter. 4. liter. After. UF. 24h after. UF. Before. UF. 1. liter. 2. liter. 3. liter. 4. liter. After. UF. 24h after. UF. RAP (mmHg) PWP (mmHg) This study by Marenzi et al (brief description below) demonstrates that ultrafiltration of more than 4 L of plasma water over approximately 9 h reduced mean arterial pressures and pulmonary wedge pressure (PWP).1 Cardiac output increased at the end of the session and was shown to decrease further 24 h after ultrafiltration was completed. Moreover during treatment, heart rate, systemic arterial pressure, cardiac output, and systemic vascular resistances did not change. Further details: The goal of the study was to investigate the hemodynamic and circulatory adjustments to extracorporeal ultrafiltration in refractory congestive HF. Twenty-four patients (18 men and 6 women)—Class IV ADHF, with signs and symptoms of volume overload, >5 kg weight gain within 1 month—were allowed to continue on digoxin, diuretics (24 of 24 patients), and angiotensin-converting enzyme inhibitors (15 of 24 patients). A continuous renal replacement therapy (CRRT) device was utilized to remove fluid, and hemodynamic measurements were taken after 1 L, 2 L, 3 L, and 4 L ultrafiltration, and then 24 h after ultrafiltration had ceased. The mean duration of ultrafiltration was 9 ± 3 h, and total volume removed was 4880 L ± 896 mL. Urine output and NYHA association class improved. Response to diuretics improved from 380 ± 157 mg/day to 112 ± 70 mg/day beginning the day after ultrafiltration started. Reference: 1. Marenzi et al. Circulatory response to fluid overload by extracoporeal ultrafiltration in refractory congestive heart failure. J Am Coll Cardiol. 2001;38: – 20 – 15 – 10 – 5 – – 25 – 20 – 15 – 10 - Before. UF. 1. liter. 2. liter. 3. liter. 4. liter. After. UF. 24h after. UF. Before. UF. 1. liter. 2. liter. 3. liter. 4. liter. After. UF. 24h after. UF. Marenzi et al. J Am Coll Cardiol. 2001;38:")
30
Costanzo et al. J Am Coll Cardiol. 2005;46:2047-2051.
The EUPHORIA Trial: Early Ultrafiltration in Patients With Decompensated HF and Observed Resistance to Intervention With Diuretic Agents Section 5: Ultrafiltration Clinical Trials Studio di EFFICACIA e SICUREZZA Media dei cicli di 8: 2.6 ± 1.2 Volume rimosso dall’UF: 8653 ± 4314 mL Costanzo et al. J Am Coll Cardiol. 2005;46:

31
Costanzo MR et al. J Am Coll Cardiol. 2007;49:675-683.
Section 5: Ultrafiltration Clinical Trials Costanzo MR et al. J Am Coll Cardiol. 2007;49:

32
Adverse Events Ultrafiltration Standard Care P Value Catheter/Needle 3
Section 5: Ultrafiltration Clinical Trials Ultrafiltration Standard Care P Value Catheter/Needle 3 .156 Filter 5 NA .154 Infection Catheter related 1 .315 Other 4 9 .202 Bleeding 7 .032 Hypotension 22 10 .113 Anemia .080 Dialysis Worsening HF 39 63 .094 Myocardial infarction 2 .988 Arrhythmias .968 Cardiac arrest 6 .987 Neurological 15 .070 Costanzo MR et al. J Am Coll Cardiol. 2007;49:

33
Section 5: Ultrafiltration Clinical Trials
Conclusioni La precoce UF produce una perdita di peso > dei diuretici EV, senza peggioramento della funzione renale La strategia di UF, nel follow up a 90 giorni, RIDUCE: % di paz. reospedalizzati Numero di ospedalizzazioni per SC Giorni di reospedalizzazione per SC Visite Emergenza o non programmate Costanzo MR et al. J Am Coll Cardiol. 2007;49:

34
Ultrafiltrazione vs Terapia Diuretica
Section 4: Ultrafiltration History and Physiology Ultrafiltrazione vs Terapia Diuretica Ultrafiltrato ISOTONICO Maggior rimozione di Sodio Non ci sono turbe elettrolitiche Maggior riduzione del volume extracellulare rispetto ad equivalente perdita di peso da diuretici Point 2: Ultrafiltration removes more sodium than diuretics for a similar given volume. Approximately 3 g of sodium per liter of ultrafiltrate.1 Point 4: Since sodium and its anion are the major determinants of extracelllular fluid (ECF) volume, ultrafiltration decreases ECF volume more than a comparable volume induced by diuretics. Therefore, it follows that ultrafiltration decreases more ECF volume than diuretics.1 Reference: 1. Schrier R. Role of diminished renal function in cardiovascular mortality. J Am Coll Cardiol ;47:1-8. Schrier. J Am Coll Cardiol. 2006;47:1-8. 1
 volume, ultrafiltration decreases ECF volume more than a comparable volume induced by diuretics. Therefore, it follows that ultrafiltration decreases more ECF volume than diuretics.1. Reference: 1. Schrier R. Role of diminished renal function in cardiovascular mortality. J Am Coll Cardiol. 2006;47:1-8. Schrier. J Am Coll Cardiol. 2006;47:")
35
ACC/AHA Guidelines 4.4.1. Management of Fluid Status
Section 6: Current Therapies and Guidelines in ADHF ACC/AHA Guidelines Management of Fluid Status In general, patients should not be discharged from the hospital until a stable and effective diuretic regimen is established, and ideally, not until euvolemia is achieved Patients who are sent home before these goals are reached are at high risk of recurrence of fluid retention and early readmission because unresolved edema may itself attenuate the response to diuretics Hunt et al. ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult. American College of Cardiology and the American Heart Association, Inc

36
Section 6: Current Therapies and Guidelines in ADHF
HFSA 2006 Guidelines 12.11 When congestion fails to improve in response to diuretic therapy, the following options should be considered: Sodium fluid restriction Increasing doses of loop diuretic Continuous infusion of loop diuretic Addition of a second type of diuretic orally (metolazone or spironolactone) or intravenously (chlorothiazide) A fifth option, ultrafiltration, may be considered (strength of evidence:c)
 or intravenously (chlorothiazide) A fifth option, ultrafiltration, may be considered (strength of evidence:c)")
37
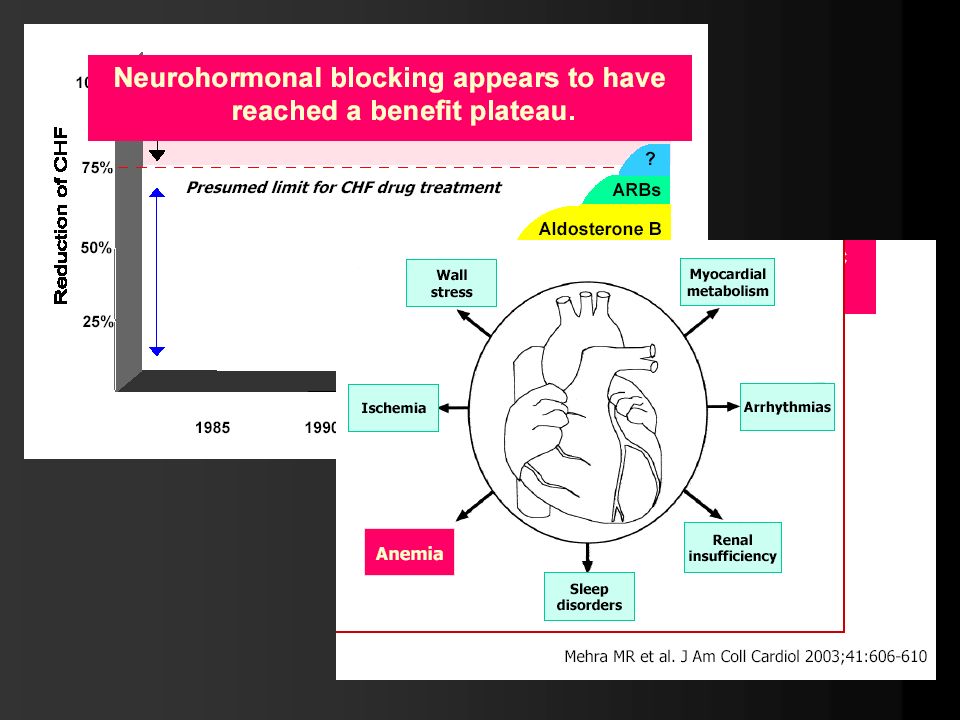
Scompenso Cardiaco ed Anemia
Lo studio Framingham ha dimostrato che la presenza di anemia costituisce un fattore di rischio indipendente per lo sviluppo di Scompenso Cardiaco. Lo studio SOLVD ne ha evidenziato l’importanza come fattore prognostico negativo in pazienti già affetti da Scompenso Cardiaco.

38
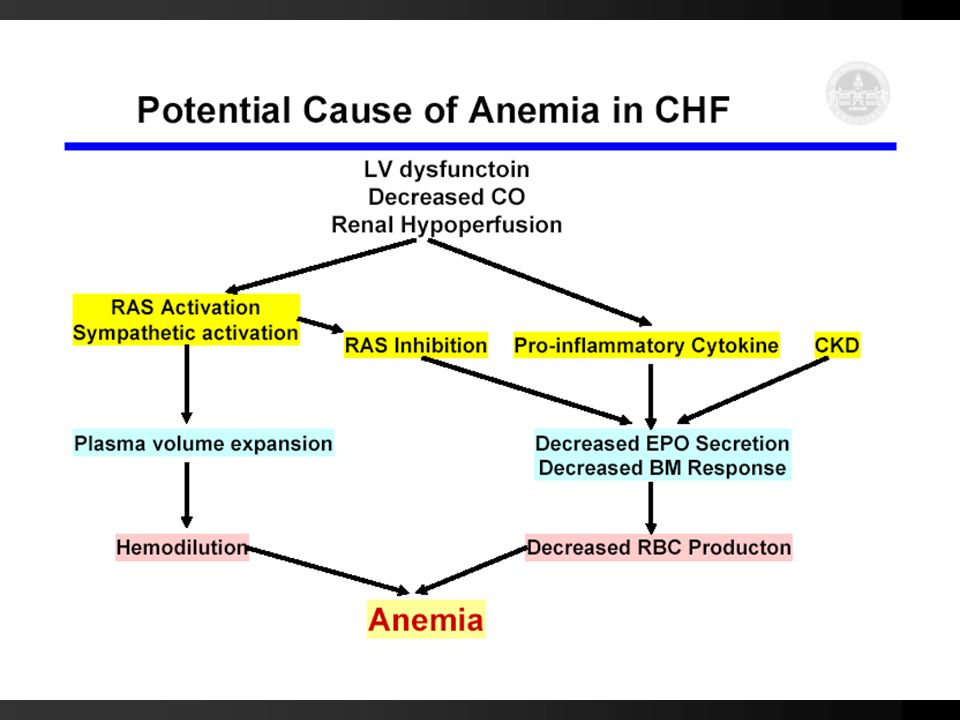
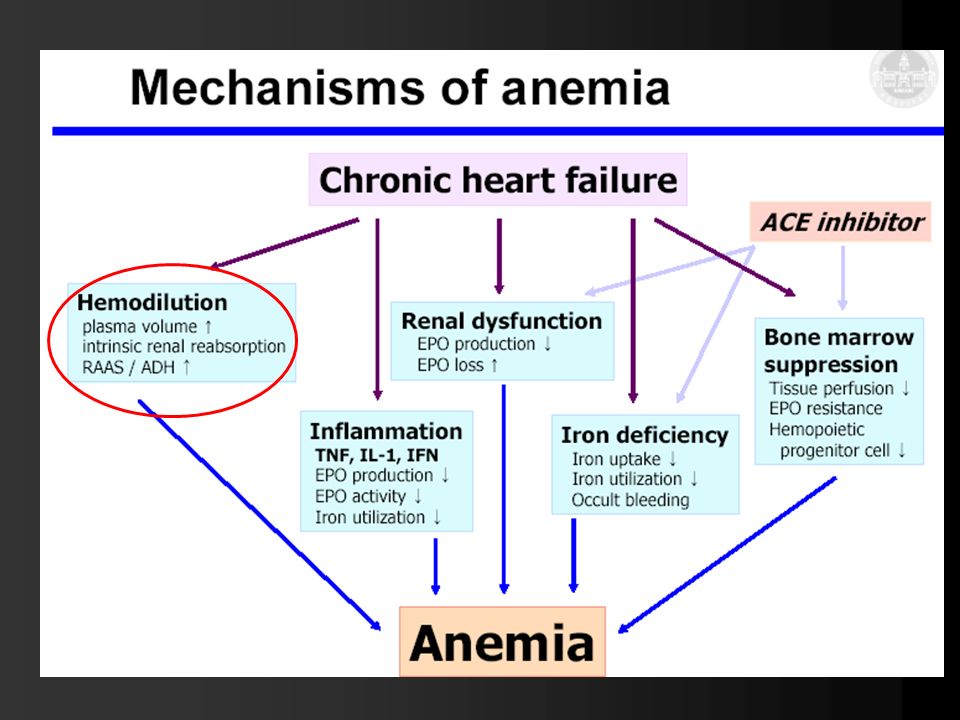
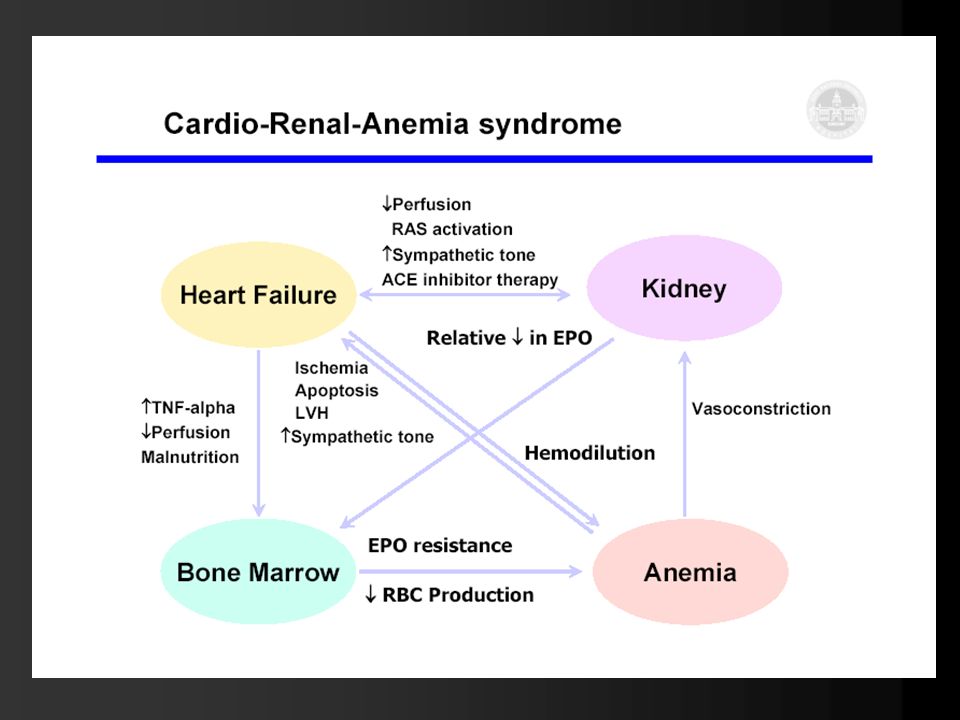
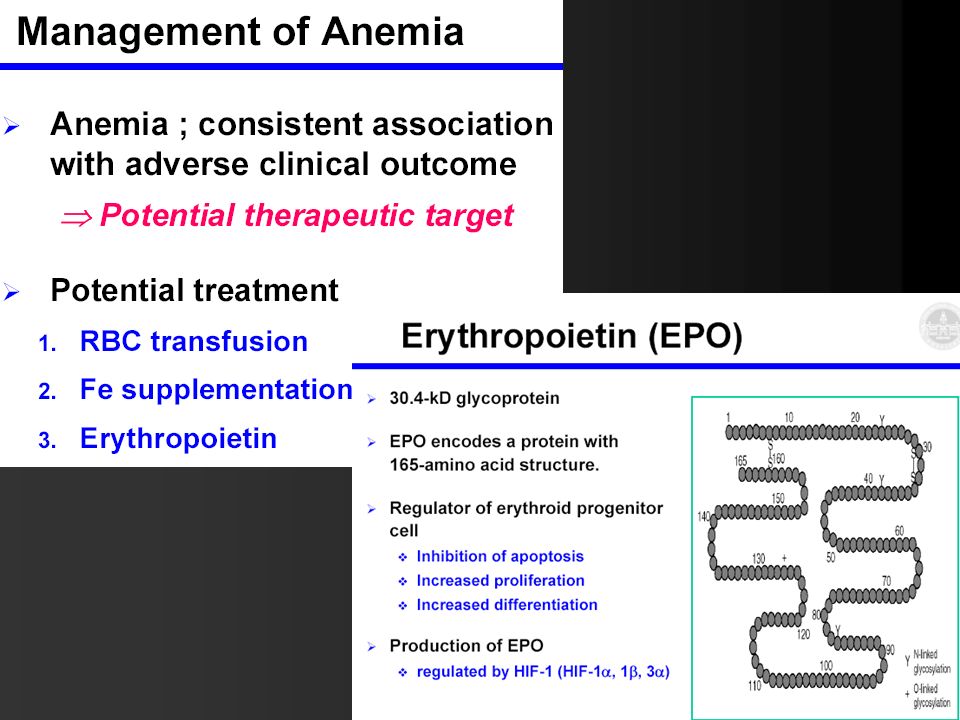
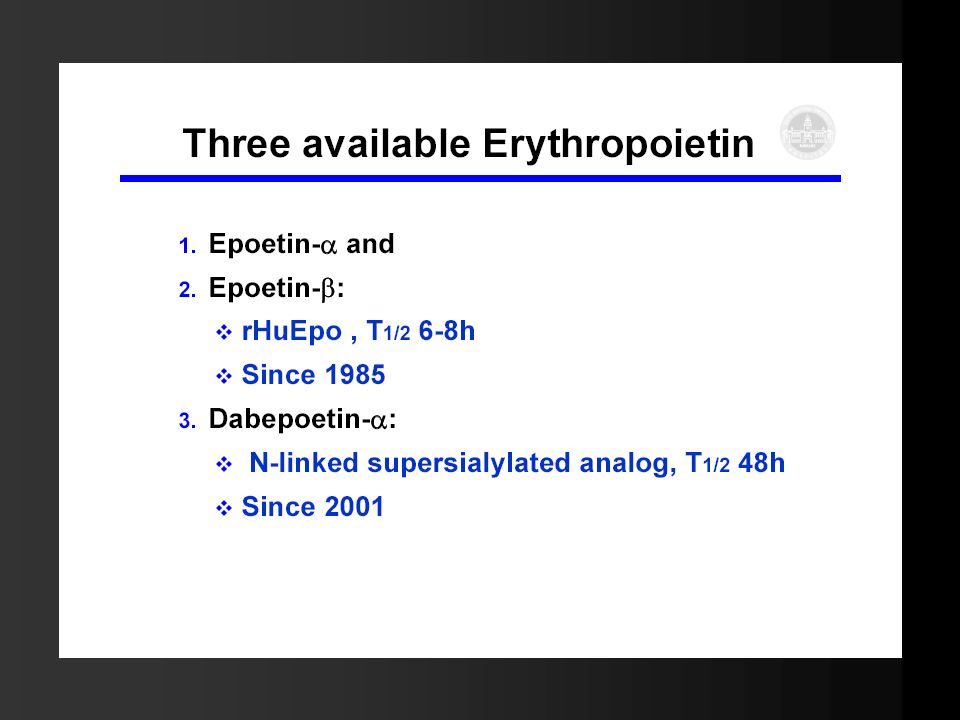
ANEMIA CAUSA DI SCOMPENSO CARDIACO
Ipossia tessutale Vasodilatazione periferica Pressione arteriosa Attività simpatica Flusso ematico renale Renina angiotensina aldosterone ADH Ritenzione liquidi Volume plasmatico Diametro ventricolare IVS e infine morte cellulare Scompenso cardiaco L’anemia nell’IRC attraverso vari meccanismi può essere causa di scompenso cardiaco.

43
Carvedilolo Sartani

58
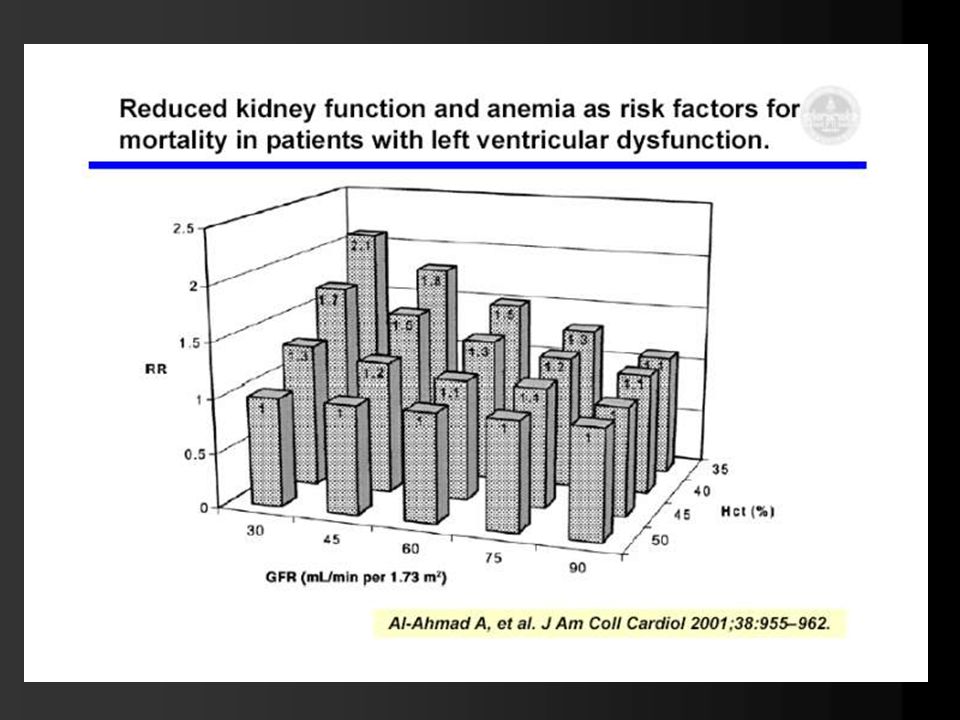
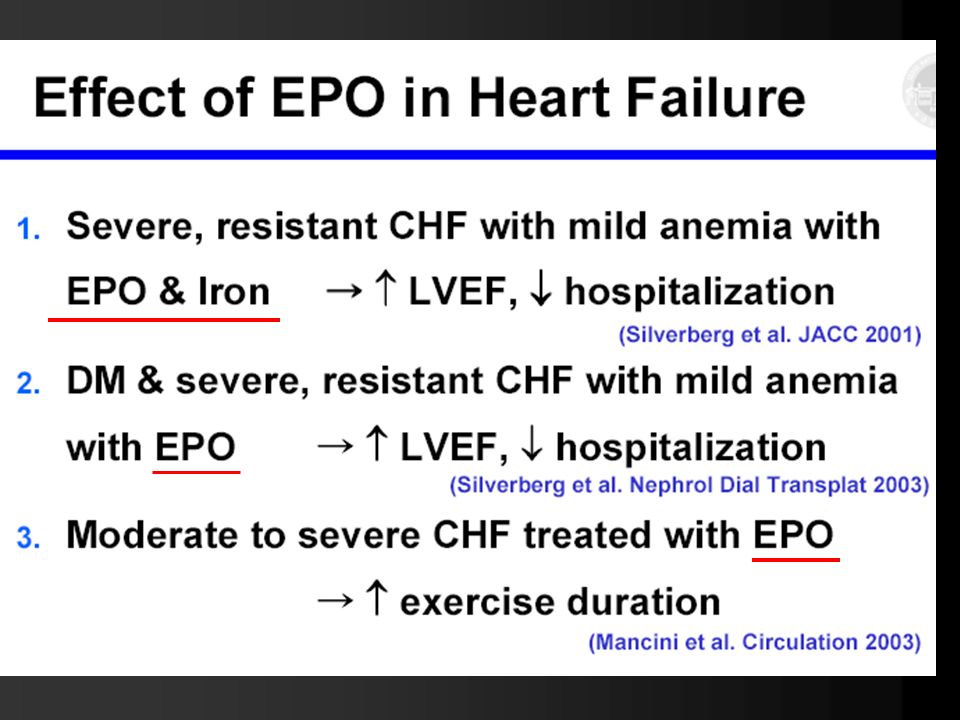
Intravenous Iron Reduces NT-Pro-Brain Natriuretic Peptide in Anemic Patients With Chronic Heart Failure and Renal Insufficiency Jorge Eduardo Toblli, MD et al, J Am Coll Cardiol, 2007; 50: Am Heart J Dec;152(6):1096.e9-15 Erythropoietin improves anemia exercise tolerance and renal function and reduces B-type natriuretic peptide and hospitalization in patients with heart failure and anemia. Palazzuoli A, Silverberg D Am Heart J Oct;154(4):645.e Links Effects of beta-erythropoietin treatment on left ventricular remodeling, systolic function, and B-type natriuretic peptide levels in patients with the cardiorenal anemia syndrome. Palazzuoli A, Silverberg DS, et al Siena J Cardiovasc Med (Hagerstown) Nov;8(11): Prognostic value of reduced kidney function and anemia in patients with chronic heart failure. Petretta M et al Napoli (NO ANEMIA!!!) IRON - HF
:1096.e9-15. Erythropoietin improves anemia exercise tolerance and renal function and reduces B-type natriuretic peptide and hospitalization in patients with heart failure and anemia. Palazzuoli A, Silverberg D. Am Heart J Oct;154(4):645.e9-15. Links. Effects of beta-erythropoietin treatment on left ventricular remodeling, systolic function, and B-type natriuretic peptide levels in patients with the cardiorenal anemia syndrome. Palazzuoli A, Silverberg DS, et al Siena. J Cardiovasc Med (Hagerstown) Nov;8(11): Prognostic value of reduced kidney function and anemia in patients with chronic heart failure. Petretta M et al Napoli (NO ANEMIA!!!) IRON - HF.")
62
Grazie per l’attenzione

Presentazioni simili














 N. Pazienti in Dialisi (2002: 308.910)>")


e mostra un ritmo irregolare che varia continuamente nella forma. La frequenza ventricolare media.>")






