Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Prevenzione cardiovascolare dopo un evento coronarico
19 Gennaio 2008 Elisa Salvetti

2
Prevenzione primaria I fattori di rischio contribuiscono negli anni alla formazione della placca aterosclerotica a livello coronarico. Fattori di rischio Età Sesso Maschile Fumo Dislipidemia Ipertensione Diabete Prevenzione primaria

3
Sindrome coronarica acuta
L’infiammazione e la disfunzione endoteliale portano a destabilizzazione della placca con possibile rottura e formazione di trombosi Aterosclerosi Sindrome coronarica acuta Recidive Prevenzione secondaria Prevenzione terziaria

4
Cardiopatia ischemica: la piramide del rischio
Prev. secondaria Prev. primaria Post IMA/angina Prev. terziaria Altre manifestazioni aterosclerotiche Aterosclerosi subclinica Fattori di rischio multipli Basso rischio

5
Persistent Hyperreactive
ACS The Tip of the Atherothrombotic “Iceberg” Acute Plaque Rupture (UA/NSTEMI/STEMI) Clinical Subclinical Presence of Multiple Coronary Plaques Persistent Hyperreactive Platelets Vascular Inflammation ACS= acute coronary syndrome. Bhatt DL. J Invasive Cardiol. 2003;15:3B-9B.
 Clinical. Subclinical. Presence of Multiple. Coronary Plaques. Persistent Hyperreactive. Platelets. Vascular. Inflammation. ACS= acute coronary syndrome. Bhatt DL. J Invasive Cardiol. 2003;15:3B-9B.")
6
ESC Guidelines of CVD prevenction - 2007
EUROPEAN SOCIETY OF CARDIOLOGY OBIETTIVI DELLA PREVENZIONE CARDIOVASCOLARE Individuare le caratteristiche che deve avere la popolazione generale per mantenere uno adeguato stato di salute 2) Maggior rigoroso controllo dei fattori di rischio in soggetti ad alto rischio CV 3) Terapia farmacologica adeguata nei pazienti ad alto rischio
 Maggior rigoroso controllo dei fattori di rischio in soggetti. ad alto rischio CV. 3) Terapia farmacologica adeguata nei pazienti ad alto rischio.")
7
ESC Guidelines of CVD prevenction - 2007
EUROPEAN SOCIETY OF CARDIOLOGY Obiettivi della prevenzione cardiovascolare nella popolazione generale : 0 Non fumare 5 Porzioni di frutta e/o verdura al giorno 3 Camminare 3 km al giorno o 30 min attività fisica moderata 25 Kg/m2 limite max di indice di massa corporea 140 mmHg max valore di PA sistolica 190 mg/dl max valore di colesterolo totale 115 mg/dl max valore di LDL 110 mg/dl max valore di glicemia

8
ESC Guidelines of CVD prevenction - 2007
EUROPEAN SOCIETY OF CARDIOLOGY Obiettivi della prevenzione cardiovascolare nei pazienti ad alto rischio e quindi dopo sindrome coronarica acuta: Valori pressori < 130/80 mmHg se possibile Colesterolo totale < 175 mg/dl, se possibile circa 155 LDL colesterolo < 100 mg/dl, se possibile circa 80 Glicemia a digiuno < 110 mg/dl ed emoglobina glicosilata < 6,5 % se possibile

9
Prevenzione cardiovascolare dopo SCA:
A) fase precoce (a domicilio, ospedale): FARMACI B) follow-up : - FARMACI (adesione al trattamento, ottimizzazione terapia) - STILE DI VITA
 fase precoce (a domicilio, ospedale): FARMACI. B) follow-up : - FARMACI (adesione al trattamento, ottimizzazione terapia) - STILE DI VITA.")
10
FARMACI CHE HANNO DIMOSTRATO RIDUZIONE DI NUOVI EVENTI
ASPIRINA CLOPIDOGREL BETA BLOCCANTI STATINE ACE- INIBITORI SARTANI OMEGA 3

11
Pathogenesis of Acute Coronary Syndromes: The integral role of platelets
Plaque Fissure or Rupture Platelet Adhesion Platelet Activation Thrombotic Occlusion Platelet Aggregation Platelets are recognized to play an integral role in acute coronary syndromes and arterial thrombosis. After plaque fissure or rupture, there is platelet adhesion and activation. This leads to platelet aggregation within the coronary artery, and ultimately partial or complete occlusion of the coronary artery. Few SMCs Activated Macrophages Inflammatory Cells

12
Acute Coronary Syndromes
ACC/AHA Guidelines JACC 2000 No ST Segment Elevation ST Segment Elevation STEMI Q-wave MI (old terminology) Unstable Angina NSTEMI Non Q-wave MI (old terminology) New Terminology on ACS Non-ST-Segment Elevation ACS ST-Segment Elevation ACS
 Unstable. Angina. NSTEMI. Non Q-wave MI. (old terminology) New Terminology on ACS. Non-ST-Segment Elevation ACS. ST-Segment Elevation ACS.")
13
GP IIb/IIIa inhibitors
Arachidonic Acid ADP cicloossigenasi Aspirin Ticlopidine Clopidogrel Thrombin Heparin LMW Heparin Direct Thrombin Inhibitors Tx A2 ATP The Platelet IIb/IIIa receptors There are multiple mediators which can result in platelet activation, including ADP, epinephrine, collagen, arachidonic acid, and thrombin. Aspirin blocks activation of platelets by arachidonic acid. The thienopyridines (ticlopidine and clopidogrel) block ADP-mediated platelet activation. Antithrombin therapy (heparin, low-molecular-weight heparin, or direct thrombin inhibitors) block thrombin-mediated platelet activation. The glycoprotein IIb/IIIa inhibitors block platelet aggregation by inhibiting fibrin from binding to the GP IIb/IIIa receptor fibrin GP IIb/IIIa inhibitors
 block ADP-mediated platelet activation. Antithrombin therapy (heparin, low-molecular-weight heparin, or direct thrombin inhibitors) block thrombin-mediated platelet activation. The glycoprotein IIb/IIIa inhibitors block platelet aggregation by inhibiting fibrin from binding to the GP IIb/IIIa receptor. fibrin. GP IIb/IIIa inhibitors.")
14
Meta-analysis of IIb/IIIa Inhibition in PCI for 30-Day Mortality
IIb/IIIa Inhibitor Better Placebo Better N 2099 2792 483 1265 150 4010 2141 2399 2064 401 300 2082 20186 Ctrl 1.7 0.7 2.1 1.3 2.0 1.1 0.6 4.5 6.6 2.3 Trt 1.5 0.4 2.5 1.0 0.7 0.8 0.5 2.0 3.4 1.9 0.9 EPIC EPILOG RAPPORT CAPTURE Impact I Impact II Restore Epistent Espirit ISAR 2 Admiral Cadillac Combined 0.73 (0.55,0.96) P=.024 0.1 1 10 OR Kong DF, et al. Am J Cardiol. 2003;92:
 P= OR. Kong DF, et al. Am J Cardiol. 2003;92:")
16
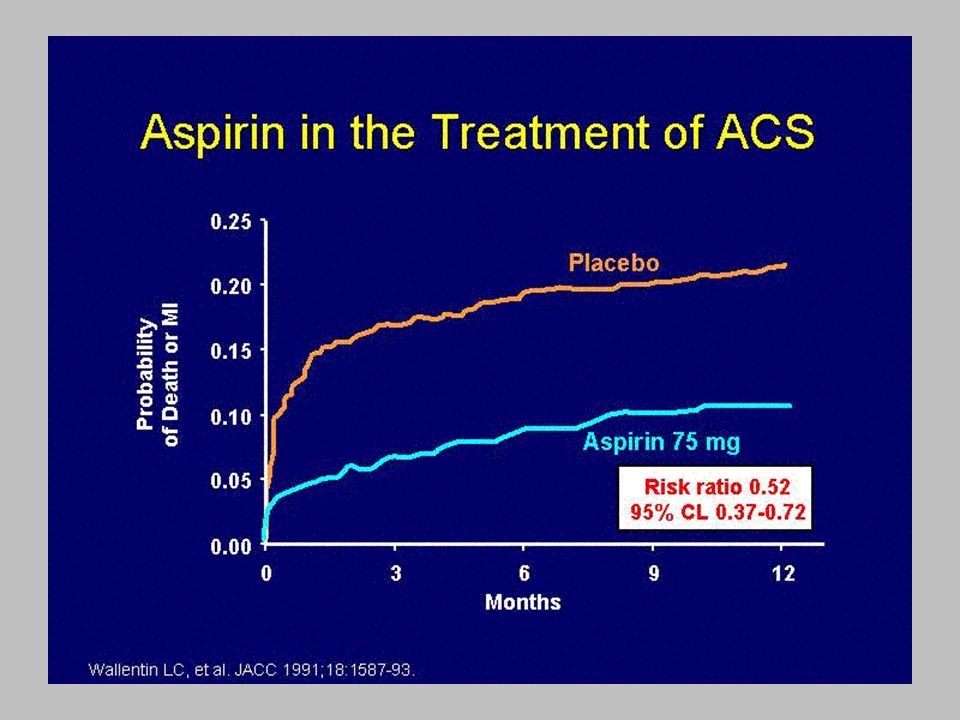
Asa nelle Sindromi Coronariche Acute
Cairns JA, NEJM; 1985

17
75 mg of aspirin per day results in almost complete inhibition of cyclooxygenase activity in platelets. This slide demonstrates that high doses of aspirin are no more effective than medium or low doses in reducing the odds of vascular events. Trials using doses of <75mg are less conclusive and, therefore, the available evidence supports daily doses of aspirin in the mg range.

18
Riduzione % occlusioni
Antiplatelet Trialists’ Collaboration: Riduzione di occlusione vascolare con ASA N° TRIALS ASA Controllo Riduzione % occlusioni CABG 20 560/2652 810/2671 - 41% PTCA 3 17/418 33/415 - 50% Tutte le procedure 23 577/3070 843/3086

19
Aspirin Recommendations
AHA/ACC Secondary Prevention for Patients with Coronary Artery and Other Atherosclerotic Vascular Disease Aspirin Recommendations Start and continue indefinitely aspirin 75 to 162 mg/d in all patients unless contraindicated For patients undergoing CABG, aspirin (100 to 325 mg/d) should be started within 48 hours after surgery to reduce saphenous vein graft closure Post-PCI-stented patients should receive 325 mg per day of aspirin for 1 month for bare metal stent, 3 months for sirolimus-eluting stent and 6 months for paclitaxel-eluting stent Circulation 2006;113: and J Am Coll Cardiol 2006;47:
 should be started within 48 hours after surgery to reduce saphenous vein graft closure. Post-PCI-stented patients should receive 325 mg per day of aspirin for 1 month for bare metal stent, 3 months for sirolimus-eluting stent and 6 months for paclitaxel-eluting stent. Circulation 2006;113: and. J Am Coll Cardiol 2006;47:")
21
Clopidogrel Evidence – Secondary Prevenction
CURE : clopidogrel in unstable angina to prevent recurrent events End Point Primario IMA/Stroke/Decesso 11.4% Placebo + ASA* 9.3% Clopidogrel + ASA* Sono stati arruolati oltre pz e i dati conclusivi hanno dimostrato che l’ associazione di clopidogrel e acido acetilsalicilico permette una significativa riduzione delle complicanze ischemiche. Si è osservata una riduzione del 20% del rischio relativo di IMA ,morte o stroke (P < 0.001), che è evidente fin dalle prime ore di trattamento , con una separazione che persiste ed aumenta progressivamente nel successivo periodo di controllo. Clopidogrel provided a 20% relative risk reduction in the composite outcome of MI, stroke or CV death (95% CI , P < 0.001). Overall there were 719 (11.4%) first events in the placebo group and 582 (9.3%) in the clopidogrel group. The hazard rate curves began to separate within the first few hours after therapy initiation and continued to diverge over the remainder of the trial. 20% RRR P < 0.001 N = 12,562 Da 12 h a 12 mesi 3 6 9 12 Mesi di Follow up * In aggiunta alla terapia standard The CURE Trial Investigators. N Engl J Med. 2001;345:
, che è evidente fin dalle prime ore di trattamento , con una separazione che persiste ed aumenta progressivamente nel successivo periodo di controllo. Clopidogrel provided a 20% relative risk reduction in the composite outcome of MI, stroke or CV death (95% CI , P < 0.001). Overall there were 719 (11.4%) first events in the placebo group and 582 (9.3%) in the clopidogrel group. The hazard rate curves began to separate within the first few hours after therapy initiation and continued to diverge over the remainder of the trial. 20% RRR. P < N = 12,562. Da 12 h a 12 mesi Mesi di Follow up. * In aggiunta alla terapia standard. The CURE Trial Investigators. N Engl J Med. 2001;345:")
22
PCI-CURE Decessi/IMA in 2658 pazienti sottoposti
a PTCA nello studio CURE 0.15 12.6% Placebo + ASA* 0.10 8.8% Percentuale Clopidogrel + ASA* 0.05 31% RRR P = N = 2658 Prospectively designed study of patients undergoing PCI who were randomized to double-blind therapy with clopidogrel or placebo, both in addition to aspirin and other standard therapy in the CURE trial. Objectives: to test the hypothesis that pre-treatment with clopidogrel in addition to aspirin and other standard therapy would be more effective than aspirin and standard therapy alone in preventing major ischemic events within the first 30 days after PCI to determine if long-term treatment (up to 1 year) with clopidogrel after PCI would provide additional clinical benefit. For the end point of MI or cardiovascular death from time of randomization to end of follow-up, treatment with clopidogrel in addition to aspirin and other standard therapy resulted in a 31% RRR (8.8% clopidogrel vs. 12.6% placebo, P = 0.002). The curves diverged early and continued to separate over the course of 12 months. This end point included events that were prevented prior to PCI, in addition to those following the procedure. There were consistent reductions in MI or cardiovascular death in almost every subgroup examined 0.0 100 200 300 400 Giorni di follow up * In combination with standard therapy Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001.
 with clopidogrel after PCI would provide additional clinical benefit. For the end point of MI or cardiovascular death from time of randomization to end of follow-up, treatment with clopidogrel in addition to aspirin and other standard therapy resulted in a 31% RRR (8.8% clopidogrel vs. 12.6% placebo, P = 0.002). The curves diverged early and continued to separate over the course of 12 months. This end point included events that were prevented prior to PCI, in addition to those following the procedure. There were consistent reductions in MI or cardiovascular death in almost every subgroup examined Giorni di follow up. * In combination with standard therapy Mehta, SR. et al for the CURE Trial Investigators. Lancet. August")
23
The CHARISMA trial randomized 15,603 patients with multiple CV risk factors or known CVD to aspirin ( mg) or aspirin ( mg) + clopidogrel (75 mg) for a mean of 30 months. The primary endpoint was stroke, myocardial infarction, or death from cardiovascular causes. The primary end point occurred in 6.8% of the clopidogrel + aspirin group and 7.3% of the placebo + aspirin group (RR 0.93; 95% CI, 0.83 to 1.05; P=0.22). There was a trend for increased total events in the primary prevention group (RR 1.2; 95% CI, 0.91 to 1.59; P=0.20) and a modest trend for benefit in those subjects with a history of prior atherothrombotic event (RR 0.88; 95% CI, 0.77 to 0.99; P=0.046).
. There was a trend for increased total events in the primary prevention group (RR 1.2; 95% CI, 0.91 to 1.59; P=0.20) and a modest trend for benefit in those subjects with a history of prior atherothrombotic event (RR 0.88; 95% CI, 0.77 to 0.99; P=0.046)..")
24
Clopidogrel Recommendations
AHA/ACC Secondary Prevention for Patients with Coronary Artery and Other Atherosclerotic Vascular Disease Clopidogrel Recommendations Start and continue clopidogrel 75 mg/d in combination with aspirin for post ACS or post PCI with stent placement patients for up to 12 months for post PCI-stented patients >1 month for bare metal stent, >3 months for sirolimus-eluting stent >6 months for paclitaxel-eluting stent *Clopidogrel is generally given preference over Ticlopidine because of a superior safety profile Circulation 2006;113: and J Am Coll Cardiol 2006;47:

25
FARMACI CHE HANNO DIMOSTRATO RIDUZIONE DI NUOVI EVENTI
ASPIRINA CLOPIDOGREL BETA BLOCCANTI STATINE ACE- INIBITORI SARTANI OMEGA 3

26
Beta bloccanti nella Prevenzione Secondaria
Metanalisi di 17 Trials Riduzione di circa il 20% del rischio di morte dopo IMA in p. in terapia cronica con b-bloccanti vs. placebo

27
Beta blockers are standard therapy for the secondary prevention of cardiovascular disease.

28
Numerous trials have shown significant decreases in all cause mortality with beta blocker therapy in patients with varying degrees of left ventricular dysfunction.

29
b-blocker Recommendations
AHA/ACC Secondary Prevention for Patients with Coronary Artery and Other Atherosclerotic Vascular Disease b-blocker Recommendations Start and continue indefinitely in all post MI, ACS, LV dysfunction with or without HF symptoms, unless contraindicated. Consider chronic therapy for all other patients with coronary or other vascular disease or diabetes unless contraindicated. I IIa IIb III *Precautions but still indicated include mild to moderate asthma or chronic obstructive pulmonary disease, insulin dependent diabetes mellitus, severe peripheral arterial disease, and a PR interval >0.24 seconds. MI=Myocardial infarction, HF=Heart Failure Circulation 2006;113: and J Am Coll Cardiol 2006;47:

30
FARMACI CHE HANNO DIMOSTRATO RIDUZIONE DI NUOVI EVENTI
ANTIPIASTRINICI BETA BLOCCANTI STATINE ACEINIBITORI PUFA

32
Pleiotropic effects ascribed to statins
Reduce platelet aggregability Reduce thrombus formation PAI-1 tF Improve endothelial function & vasomotion NO bioavailability circ. endothelial progenitor cells Decrease matrix degradation macrophage metalloproteinase collagen content Reduce inflammation within plaque CRP monocyte adhesion Promote plaque remodeling HDL-Chol LDL-Chol TGL adapted from Rosensonet al. JAMA1998;279:1643–1650

33
Statine e variazione % della PCR (proteina C-reattiva)
Atorvastatina (10 mg) Simvastatina (20 mg) Pravastatina (40 mg) * P < 0.025 vs. basale -5 -10 % riduzione -15 -20 * * -25 (n=22, LDL-C>130 mg%, 6 settimane di trattamento) * -30 Jalal I et al. Effect of Hydroxymethyl Gllutaryl Coenzyme A Reductase Inhibitor Therapy on High Sensitive C-Reactive Protein Levels. Circulation, 103: ; 2001
 Simvastatina. (20 mg) Pravastatina. (40 mg) * P < vs. basale % riduzione * * -25. (n=22, LDL-C>130 mg%, 6 settimane di trattamento) * -30. Jalal I et al. Effect of Hydroxymethyl Gllutaryl Coenzyme A Reductase Inhibitor Therapy on High Sensitive C-Reactive Protein Levels. Circulation, 103: ;")
34
Statins administration in primary and secondary prevention
Pre-clinical CHD Chronic CHD ACS Secondary prevention 4S /HPS (sim mg) CARE /LIPID (pra 40 mg) LIPS (flu 80 mg) TNT/IDEAL (ato > mg) Primary prevention AFCAPS (lov mg) WOSCOPS (pra 40 mg) ASCOT/ CARDS (ato 10 mg) Statins, or HMG-CoA reductase inhibitors, have been shown to reduce cardiovascular events in subjects with or at risk for coronary artery disease. Clinical benefit in trials with progressively lower baseline and achieved cholesterol levels has led to expanded indications for these medications. Despite robust and consistent results, questions remained about early initiation of statin therapy after acute coronary syndrome (ACS) and whether intensive therapy would result in a greater benefit. Until recently, few data were available on the optimal timing and intensity of initiation of statin therapy after ACS. MIRACL Intensive treatment (atorvastatin mg) Early statins Miracl A to Z Prove IT NRMI
 CARE /LIPID (pra 40 mg) LIPS (flu 80 mg) TNT/IDEAL (ato > mg) Primary prevention. AFCAPS (lov mg) WOSCOPS (pra 40 mg) ASCOT/ CARDS (ato 10 mg) Statins, or HMG-CoA reductase inhibitors, have been shown to reduce cardiovascular events in subjects with or at risk for coronary artery disease. Clinical benefit in trials. with progressively lower baseline and achieved cholesterol levels has led to expanded indications for these medications. Despite robust and consistent results, questions remained about early initiation of statin therapy after acute coronary syndrome (ACS) and whether intensive therapy. would result in a greater benefit. Until recently, few data were available on the optimal timing and intensity of initiation of statin therapy after ACS. MIRACL. Intensive treatment. (atorvastatin mg) Early statins. Miracl. A to Z. Prove IT. NRMI.")
35
Colesterolemia (212-309 mg/dL)
The 4S trial was a landmark study that sought to evaluate the effect of statin therapy in secondary prevention. A total of 4,444 men and women with angina or prior MI and serum cholesterol levels of mmol/L ( mg/dL) were randomized to simvastatin (20-40 mg) or placebo for greater than 5 years. Treatment with simvastatin resulted in a 30% relative risk reduction in all-cause mortality (11.5 vs. 8.2%, p<0.001). Colesterolemia ( mg/dL)
 were randomized to simvastatin (20-40 mg) or placebo for greater than 5 years. Treatment with simvastatin resulted in a 30% relative risk reduction in all-cause mortality (11.5 vs. 8.2%, p<0.001). Colesterolemia ( mg/dL)")
36
cholesterol level was <240 mg/dL
The CARE trial sought to evaluate the effect of statins in secondary prevention, particularly among those with average cholesterol levels. The mean total cholesterol level was <240 mg/dL and the LDL-C levels ranged between mg/dL. A total of 4,159 patients with a history of myocardial infarction were randomized to pravastatin (40 mg) or placebo for 5 years. Treatment with pravastatin resulted in a 24% relative risk reduction in the primary end point (myocardial infarction or coronary heart disease death). cholesterol level was <240 mg/dL
 or placebo for 5 years. Treatment with pravastatin resulted in a 24% relative risk reduction in the primary end point (myocardial infarction or coronary heart disease death). cholesterol level was <240 mg/dL.")
37
The LIPID study sought to evaluate the effect of statins in secondary prevention among those with a broad range of cholesterol levels. Patients with a history of known coronary artery disease were randomized to pravastatin (40 mg) or placebo over a mean of 6.1 years. Patients receiving pravastatin experienced a significant 24% relative risk reduction in coronary heart disease mortality, with no clinically significant adverse effects.
 or placebo over a mean of 6.1 years. Patients receiving pravastatin experienced a significant 24% relative risk reduction in coronary heart disease mortality, with no clinically significant adverse effects..")
38
The Heart Protection Study sought to evaluate the effect of simvastatin on all cause mortality in high risk patients regardless of LDL-C levels. Treatment with simvastatin resulted in a 12% relative risk reduction in all-cause mortality and a 24% relative risk reduction in the first occurrence of any major vascular event. The benefit of simvastatin even extended to individuals with a baseline LDL-C level <100 mg/dL.

39
Early statins in ACS: What Evidence ?
Observational studies Stenestrand et al , 2001 (RIKS-HIA database) Aronow et al, 2001 (GUSTO-IIB+PURSUIT) Newby et al, 2002 (SYMPHONY) Fonarow et al, 2005 (NRMI-4) Lenderink et al, 2006 (Euro Heart Survey ACS) Large RCTs MIRACL (2001) A to Z (2004) PROVE-IT TIMI 22 (2004) Meta-analysis
 Aronow et al, 2001 (GUSTO-IIB+PURSUIT) Newby et al, 2002 (SYMPHONY) Fonarow et al, 2005 (NRMI-4) Lenderink et al, 2006 (Euro Heart Survey ACS) Large RCTs. MIRACL (2001) A to Z (2004) PROVE-IT TIMI 22 (2004) Meta-analysis.")
40
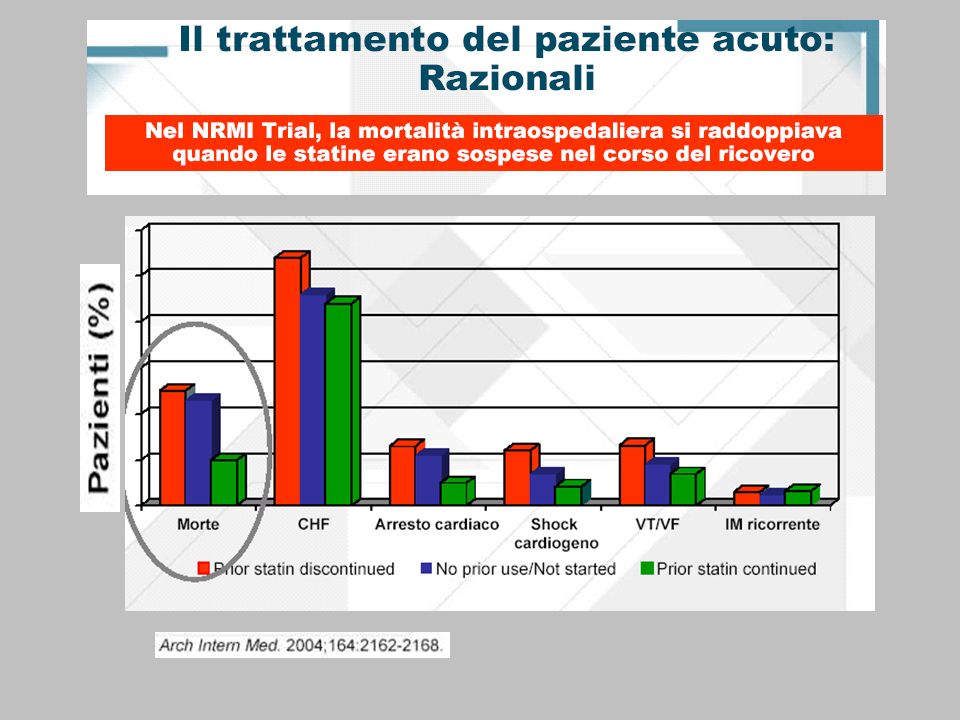
Clinical events % Rispetto al non uso, somministrare statina nelle prime 24 ore di ospedalizzazione porta a una riduzione della mortalità pari al 77% Yes/yes= pazienti che continuano la terapia con statina; no/yes= pazienti appena inseriti nella terapia con statine; no/no=pazienti che non hanno ricevuto statina né prima né durante le prime 24 ore di ospedalizzazione; yes/no=pazienti in cui la terapia con statina è stata interrotta.

42
Lenderink et al, Eur Heart J 2006;27:1799-1804
Very early (<24 hrs) statin therapy in patients with ACS associated with reduced mortality Euro Heart Survey (10,484 patiens) HR 0.44 (95% CI ) 7 HR 0.16 (95% CI ) (n=1426) (n=6771) Lenderink et Al. Eur Heart J 2006 Lenderink et al, Eur Heart J 2006;27:
 statin therapy in patients with ACS associated with reduced mortality. Euro Heart Survey (10,484 patiens) HR 0.44 (95% CI ) 7. HR 0.16 (95% CI ) (n=1426) (n=6771) Lenderink et Al. Eur Heart J Lenderink et al, Eur Heart J 2006;27:")
43
Terapia standard + atorvastatina 80 mg
MIRACL (Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering) Disegno dello studio Popolazione Infarto Non-Q Angina instabile randomizzazione ore dal ricovero esclusione: prevista CABG/ PTCA comparsa di onda Q < 28 giorni, CABG < 3 mesi, PTCA < 6 mesi, NYHA IIIb/IV, TC > 7 mmol Terapia standard + Placebo 3.086 Pazienti Terapia standard + atorvastatina 80 mg 4 mesi Endpoint primario tempo al 1° evento ischemico (morte per CHD, IMA non-fatale, arresto cardiaco)
 Disegno dello studio. Popolazione. Infarto Non-Q. Angina instabile. randomizzazione ore dal ricovero. esclusione: prevista CABG/ PTCA. comparsa di onda Q < 28 giorni, CABG < 3 mesi, PTCA < 6 mesi, NYHA IIIb/IV, TC > 7 mmol. Terapia standard + Placebo Pazienti. Terapia standard + atorvastatina 80 mg. 4 mesi. Endpoint primario. tempo al 1° evento ischemico. (morte per CHD, IMA non-fatale, arresto cardiaco)")
44
The MIRACL trial was the first large scale study to evaluate the effects of acute intensive statin therapy in the secondary prevention setting. Compared to placebo, treatment with atorvastatin (80 mg) within 96 hours of an acute coronary syndrome resulted in a 16% relative risk reduction in the primary end point (death, nonfatal acute myocardial infarction, cardiac arrest with resuscitation, or objective evidence of recurrent symptomatic myocardial ischemia requiring emergency rehospitalization). There were no significant differences in the risk of death, nonfatal myocardial infarction, or cardiac arrest in the two arms of the study. The difference in the primary endpoint was driven by a lower risk of symptomatic ischemia requiring emergency rehospitalization (6.2% vs. 8.4%; RR, 0.74; 95% CI, ; P =0.02). Treatment with atorvastatin resulted in a mean decrease in LDL-C from 124 mg/dL to 72 mg/dL. There was a significant increase in hepatic transaminases >3x the upper limit of normal with atorvastatin as compared to placebo (2.5% vs 0.6%; P<.001).
. Treatment with atorvastatin resulted in a mean decrease in LDL-C from 124 mg/dL to 72 mg/dL. There was a significant increase in hepatic transaminases >3x the upper limit of normal with atorvastatin as compared to placebo (2.5% vs 0.6%; P<.001).")
45
The A to Z trial sought to determine whether treatment with a low dose statin regimen would provide similar risk reduction in patients with an ACS as a high dose statin regimen (similar to that used in the PROVE IT-TIMI 22 and MIRACL trials). The high dose statin regimen consisted of treatment with simvastatin at 40 mg/day for one month, followed by an increase to 80 mg/day thereafter. The low dose statin regimen consisted of treatment with placebo for 4 months, followed by simvastatin at 20 mg/day thereafter. There was no statistical difference in the primary end point between the two treatment strategies; however, there was a trend towards a reduced event rate in the high dose statin regimen at the end of the 24 month follow-up. Unfortunately, the high dose statin regimen was associated with nine cases of statin-induced myopathy.

46
mod. from Schwartz G et al, Am J Cardiol 2005;96:45F–53F
Intensive, but not moderate, statin treatment reduces early ischemic events after ACS Months of randomized treatment MIRACL A to Z RR=0.84 P=0.048 RR=1.01 P=NS mod. from Schwartz G et al, Am J Cardiol 2005;96:45F–53F Schwartz et Al. Am J Cardiol 2005

47
PROVE IT-TIMI 22 was designed to assess the effects of early statin therapy in individuals with an acute coronary syndrome. In a head-to-head comparison of statin regimens, patients were randomized to a high dose potent statin (atorvastatin 80 mg) or a moderate dose less potent statin (pravastatin 40 mg) over a mean follow-up of 24 months to determine if intensive statin therapy was associated with a lower event rate. Use of atorvastatin and pravastatin resulted in on-treatment mean LDL-C levels of 62 mg/dL and 95 mg/dL, respectively. The primary end point (a composite of death from any cause, myocardial infarction, documented unstable angina requiring rehospitalization, recurrent revascularization, or stroke) occurred in 22.4% of individuals on atorvastatin vs. 26.3% of individuals on pravastatin, p= This effect of intensive statin therapy set a new benchmark for aggressive early LDL-C lowering in acute coronary syndromes.
 occurred in 22.4% of individuals on atorvastatin vs. 26.3% of individuals on pravastatin, p= This effect of intensive statin therapy set a new benchmark for aggressive early LDL-C lowering in acute coronary syndromes.")
48
Intensive, but not moderate, statin treatment reduces early ischemic events after ACS Kaplan-Meier event curves for the primary end point MIRACL A to Z PROVE IT HR=0.8 P =0.03 Death, AMI, stroke, USA, revascularization >30 days RR=0.84 p=0.048 RR=1.01 p=NS Months of randomized treatment

49
Following the Heart Protection Study, the TNT study sought to determine whether high dose statin therapy provided additional cardiovascular benefit among individuals with chronic coronary heart disease. All patients entered an open-label eight week period with low dose atorvastatin (10 mg) to achieve an LDL-C level <130 mg/dL prior to randomization. Among enrolled patients, high dose atorvastatin (80 mg) resulted in a significant 22% relative risk reduction in the primary composite endpoint (death from coronary heart disease, nonfatal MI, resuscitation after cardiac arrest, and fatal or nonfatal stroke) as compared to low dose atorvastatin (10 mg). Paralleling the reduction in the composite primary endpoint was a decrease in the LDL-C levels to 77 mg/dL and 101 mg/dl in the high and low dose atorvastatin arms, respectively. There were no differences in overall mortality. These results add to the body of data obtained in the PROVE IT-TIMI 22 and HPS trials, demonstrating a benefit with lower LDL-C levels in individuals with coronary heart disease.
 resulted in a significant 22% relative risk reduction in the primary composite endpoint (death from coronary heart disease, nonfatal MI, resuscitation after cardiac arrest, and fatal or nonfatal stroke) as compared to low dose atorvastatin (10 mg). Paralleling the reduction in the composite primary endpoint was a decrease in the LDL-C levels to 77 mg/dL and 101 mg/dl in the high and low dose atorvastatin arms, respectively. There were no differences in overall mortality. These results add to the body of data obtained in the PROVE IT-TIMI 22 and HPS trials, demonstrating a benefit with lower LDL-C levels in individuals with coronary heart disease.")
50
Frequenza delle mialgie in rapporto al dosaggio utilizzato

51
Cannon et al, J Am Coll Cardiol 2006;48:438-45
Severe adverse event rates for intensive vs moderate statin therapy (n. 27,548 pts) Rhabdomyolysis CPK >10 xULN AST/ALT >3 xULN Standard dose High dose PROVE IT (n=4162) 0% 0.1% 1.1% 3.3% A to Z (n=4497) 0.13% 0.04% 0.4% 0.36% 0.84% TNT (n=10001) 0.06% 0.18% 1.2% IDEAL (n=8888) 0.07% 0.05% 0.16% 1.37% Cannon et al, J Am Coll Cardiol 2006;48:438-45
 Rhabdomyolysis CPK >10 xULN AST/ALT >3 xULN. Standard dose. High dose. PROVE IT (n=4162) 0% 0.1% 1.1% 3.3% A to Z (n=4497) 0.13% 0.04% 0.4% 0.36% 0.84% TNT (n=10001) 0.06% 0.18% 1.2% IDEAL (n=8888) 0.07% 0.05% 0.16% 1.37% Cannon et al, J Am Coll Cardiol 2006;48:")
52
Lipid Management Goal LDL-C should be less than 100 mg/dL
AHA/ACC Secondary Prevention for Patients with Coronary Artery and Other Atherosclerotic Vascular Disease Lipid Management Goal LDL-C should be less than 100 mg/dL Further reduction to LDL-C to < 70 mg/dL is reasonable I IIa IIb III If TG >200 mg/dL, non-HDL-C should be < 130 mg/dL Circulation 2006;113: and J Am Coll Cardiol 2006;47:

53
FARMACI CHE HANNO DIMOSTRATO RIDUZIONE DI NUOVI EVENTI
ASPIRINA CLOPIDOGREL BETA BLOCCANTI STATINE ACE-INIBITORI SARTANI OMEGA 3

54
The HOPE trial sought to evaluate the role of ramipril in patients that were at high risk for cardiovascular events without left ventricular dysfunction or heart failure. The primary outcome was a composite of MI, stroke, or death from cardiovascular causes. A total of 14% of patients taking ramipril reached the primary end point, as compared with 18% of patients assigned to receive placebo (RR 0.78; ; P<0.001). Treatment with ramipril reduced the rates of death from cardiovascular causes (6%, vs. 8%; RR 0.74; P<0.001), MI (10% vs. 12%; RR 0.80; P<0.001), stroke (3.4% vs. 5%; RR 0.68; P<0.001), death from any cause (10% vs. 12%; RR 0.84; P=0.005), revascularization procedures (16% vs. 18%;RR 0.85; P=0.002), cardiac arrest (0.8% vs. 1.3%; RR 0.63; P=0.03), heart failure (9% vs. 11.5%; RR 0.77; P<0.001), and complications related to diabetes (6% vs. 8%; RR 0.84; P=0.03). Treatment with ramipril was associated with a significant reduction in the rates of death, MI, and stroke in a broad range of high-risk patients that were not known to have left ventricular systolic dysfunction or heart failure. Studio interrotto anticipatamente per chiara e significativa riduzione di mortalità nel gruppo ramipril. Nei diabetici il beneficio è stato ancora più evidente.
, MI (10% vs. 12%; RR 0.80; P<0.001), stroke (3.4% vs. 5%; RR 0.68; P<0.001), death from any cause (10% vs. 12%; RR 0.84; P=0.005), revascularization procedures (16% vs. 18%;RR 0.85; P=0.002), cardiac arrest (0.8% vs. 1.3%; RR 0.63; P=0.03), heart failure (9% vs. 11.5%; RR 0.77; P<0.001), and complications related to diabetes (6% vs. 8%; RR 0.84; P=0.03). Treatment with ramipril was associated with a significant reduction in the rates of death, MI, and stroke in a broad range of high-risk patients that were not known to have left ventricular systolic dysfunction or heart failure. Studio interrotto anticipatamente per chiara e significativa riduzione di mortalità nel gruppo ramipril. Nei diabetici il beneficio è stato ancora più evidente.")
55
This trial assessed whether perindopril reduced cardiovascular risk in an intermediate-risk population with stable coronary heart disease and no apparent heart failure. After a run-in period of 4 weeks in which all patients received perindopril, 12,218 patients were randomly assigned perindopril 8 mg once daily (n=6110) or matching placebo (n=6108). The mean follow-up was 4.2 years and the primary end point by an intention to treat analysis was cardiovascular death, myocardial infarction, or cardiac arrest. A majority of patients were already on antiplatelet agents, a beta-blocker, and lipid lowering therapy. Perindopril resulted in a 20% relative risk reduction in the primary endpoint compared to placebo (95% Cl 9–29, p=0.0003). These benefits were consistent in all prespecified subgroups and secondary end points. This led the investigators to conclude that among patients with stable coronary heart disease without apparent heart failure, perindopril resulted in significantly improved outcomes and a reduction of one major cardiovascular event for every 50 patients treated over 4 years.
. These benefits were consistent in all prespecified subgroups and secondary end points. This led the investigators to conclude that among patients with stable coronary heart disease without apparent heart failure, perindopril resulted in significantly improved outcomes and a reduction of one major cardiovascular event for every 50 patients treated over 4 years.")
56
The PEACE Trial was designed to test the hypothesis that patients with stable coronary artery disease and normal or slightly reduced left ventricular function derive therapeutic benefit from the addition of ACE inhibitors to modern conventional therapy. The incidence of the primary end point (death from cardiovascular causes, myocardial infarction, or coronary revascularization) was 21.9% in the trandolapril group, as compared with 22.5% in the placebo group (hazard ratio in the trandolapril group, 0.96; 95 percent CI, 0.88 to 1.06; P=0.43) over a median follow-up period of 5 years. This led the authors to conclude that in patients with stable coronary artery disease and preserved left ventricular systolic function that are receiving "current standard" therapy and in whom the rate of cardiovascular events is lower than in previous trials of ACE inhibitors in patients with vascular disease, there is no evidence that the addition of an ACE inhibitor is associated with further benefit in terms of death from cardiovascular causes, myocardial infarction, or coronary revascularization. Trandolapril at this dose, however, did slow progression from the metabolic syndrome to diabetes.
 was 21.9% in the trandolapril group, as compared with 22.5% in the placebo group (hazard ratio in the trandolapril group, 0.96; 95 percent CI, 0.88 to 1.06; P=0.43) over a median follow-up period of 5 years. This led the authors to conclude that in patients with stable coronary artery disease and preserved left ventricular systolic function that are receiving current standard therapy and in whom the rate of cardiovascular events is lower than in previous trials of ACE inhibitors in patients with vascular disease, there is no evidence that the addition of an ACE inhibitor is associated with further benefit in terms of death from cardiovascular causes, myocardial infarction, or coronary revascularization. Trandolapril at this dose, however, did slow progression from the metabolic syndrome to diabetes.")
57
A meta-analysis of 7 trials demonstrated that ACE inhibitors decrease overall mortality (OR, 0.86; 95% confidence interval, ), myocardial infarction (OR, 0.82; 95% confidence interval, ), cardiovascular mortality (OR, 0.81; 95% confidence interval, ), and stroke (OR, 0.77; 95% confidence interval, ) in patients with coronary artery disease and preserved left ventricular systolic function.
, myocardial infarction (OR, 0.82; 95% confidence interval, ), cardiovascular mortality (OR, 0.81; 95% confidence interval, ), and stroke (OR, 0.77; 95% confidence interval, ) in patients with coronary artery disease and preserved left ventricular systolic function.")
58
In these three post-infarction trials (n=5966), mortality was lower with ACE inhibitors than with placebo (odds ratio 0.74 [95% Cl 0.66–0.83]), as were the rates of readmission for heart failure (OR 0.73 [0.63–0.85]), re-infarction (OR 0.80 [ ]) or the composite of these events (OR 0.75 [0.67–0.83]; all p<0.001). The benefits were observed early after the start of therapy and persisted long term. The benefits were independent of age, sex, and baseline use of diuretics, aspirin, and β-blockers. Although there was a trend towards greater reduction in risk of death or readmission for heart failure in patients with lower ejection fractions, the benefit extended over the range of ejection fractions examined. This led the authors to conclude that ACE inhibitors lower rates of mortality, myocardial infarction, and hospital admission for heart failure in patients with left-ventricular systolic dysfunction or heart failure following a MI.
![In these three post-infarction trials (n=5966), mortality was lower with ACE inhibitors than with placebo (odds ratio 0.74 [95% Cl 0.66–0.83]), as were the rates of readmission for heart failure (OR 0.73 [0.63–0.85]), re-infarction (OR 0.80 [ ]) or the composite of these events (OR 0.75 [0.67–0.83]; all p<0.001).](http://slideplayer.it/slide/553717/1/images/58/In+these+three+post-infarction+trials+%28n%3D5966%29%2C+mortality+was+lower+with+ACE+inhibitors+than+with+placebo+%28odds+ratio+0.74+%5B95%25+Cl+0.66%E2%80%930.83%5D%29%2C+as+were+the+rates+of+readmission+for+heart+failure+%28OR+0.73+%5B0.63%E2%80%930.85%5D%29%2C+re-infarction+%28OR+0.80+%5B+%5D%29+or+the+composite+of+these+events+%28OR+0.75+%5B0.67%E2%80%930.83%5D%3B+all+p%3C0.001%29..jpg "The benefits were observed early after the start of therapy and persisted long term. The benefits were independent of age, sex, and baseline use of diuretics, aspirin, and β-blockers. Although there was a trend towards greater reduction in risk of death or readmission for heart failure in patients with lower ejection fractions, the benefit extended over the range of ejection fractions examined. This led the authors to conclude that ACE inhibitors lower rates of mortality, myocardial infarction, and hospital admission for heart failure in patients with left-ventricular systolic dysfunction or heart failure following a MI.")
59
Effects of ACE-inhibitors on mortality in AMI
(Long Term Clinical Trials) 2 1 0,5 AIRE TRACE SAVE ACE inhibitors better Placebo Relative Risk of mortality: - 26% Paz con EF<40%; Segni e/o sintomi da CHF; IMA anteriore
 ,5. AIRE. TRACE. SAVE. ACE inhibitors. better. Placebo. Relative Risk of mortality: - 26% Paz con EF<40%; Segni e/o sintomi da CHF; IMA anteriore.")
60
Effects of ACE-inhibitors on mortality in AMI
(Short Term Clinical Trials) 2 1 0,5 SMILE ISIS-4 GISSI-3 ACE inhibitors better Placebo Relative Risk of mortality: - 6,7% Arruolati tutti i paz. Con IMA FWP breve 1-2 mesi
 ,5. SMILE. ISIS-4. GISSI-3. ACE inhibitors. better. Placebo. Relative Risk of mortality: - 6,7% Arruolati tutti i paz. Con IMA. FWP breve 1-2 mesi.")
61
B ACE Inhibitor Recommendations
AHA/ACC Secondary Prevention for Patients with Coronary Artery and Other Atherosclerotic Vascular Disease ACE Inhibitor Recommendations Use in all patients with LVEF < 40%, and those with diabetes or chronic kidney disease indefinitely, unless contraindicated Consider for all other patients Among lower risk patients with normal LVEF where cardiovascular risk factors are well controlled and where revascularization has been performed, their use may be considered optional I IIa IIb III B ACE=Angiotensin converting enzyme, LVEF= left ventricular ejection fraction Circulation 2006;113: and J Am Coll Cardiol 2006;47:

62
FARMACI CHE HANNO DIMOSTRATO RIDUZIONE DI NUOVI EVENTI
ASPIRINA BETA BLOCCANTI STATINE ACE- INIBITORI SARTANI PUFA

63
This double-blind trial compared the effect of an angiotensin-receptor blocker (valsartan), to an ACE inhibitor (captopril), and the combination of the two on mortality in patients with post-infarction heart failure or left ventricular systolic dysfunction. During a median follow-up of 24.7 months, there was no difference in all cause mortality between the three groups. The upper limit of the one-sided 97.5% confidence interval for the comparison of the valsartan group with the captopril group was within the prespecified margin for noninferiority with regard to mortality (P=0.004) and with regard to the composite end point of fatal and nonfatal cardiovascular events (P<0.001). The valsartan-and-captopril group had the most drug-related adverse events. With monotherapy, hypotension and renal dysfunction were more common in the valsartan group, and cough, rash, and taste disturbance were more common in the captopril group. These findings led the authors to conclude that valsartan was as effective as captopril in patients that are at high risk for cardiovascular events after myocardial infarction and that combining valsartan with captopril increased the rate of adverse events without improving survival.
 and with regard to the composite end point of fatal and nonfatal cardiovascular events (P<0.001). The valsartan-and-captopril group had the most drug-related adverse events. With monotherapy, hypotension and renal dysfunction were more common in the valsartan group, and cough, rash, and taste disturbance were more common in the captopril group. These findings led the authors to conclude that valsartan was as effective as captopril in patients that are at high risk for cardiovascular events after myocardial infarction and that combining valsartan with captopril increased the rate of adverse events without improving survival.")
64
Angiotensin Receptor Blocker Recommendations
AHA/ACC Secondary Prevention for Patients with Coronary Artery and Other Atherosclerotic Vascular Disease Angiotensin Receptor Blocker Recommendations Use in patients who are intolerant of ACE inhibitors with HF or post MI with LVEF less than or equal to 40%. Consider in other patients who are ACE inhibitor intolerant. Consider use in combination with ACE inhibitors in systolic dysfunction HF. I IIa IIb III ACE=Angiotensin converting enzyme inhibitor, LVEF=Left Ventricular Ejection fraction, HF=Heart failure, MI=Myocardial infarction Circulation 2006;113: and J Am Coll Cardiol 2006;47:

65
FARMACI CHE HANNO DIMOSTRATO RIDUZIONE DI NUOVI EVENTI
ASPIRINA BETA BLOCCANTI STATINE ACE- INIBITORI SARTANI Omega 3

66
Omega 3 fatty acid supplementation appears to lower CV events in several large clinical trials.
In the Diet and Reinfarction Trial (DART), 2033 men with a history of MI received one of three dietary recommendations: (a) reduced fat and increased ratio of polyunsaturated to saturated fat, (b) increased fatty fish intake, or (c) increased fiber intake. The fish group was advised to eat at least 2 portions of fatty fish (300 grams total), corresponding to a weekly intake of about 2.5 grams of eicosapentaenoic acid (EPA). Those who could not tolerate this fish intake were advised to supplement it with fish oil capsules. Those advised to eat fatty fish had a 29% relative decrease in two year all-cause mortality compared with the other two groups. The GISSI trial randomized 11,324 patients with a history of MI to n-3 polyunsaturated fatty acids (PUFA) (1 gram daily), vitamin E (300 mg daily), both, or none for 3.5 years. n-3 PUFA, but not vitamin E, significantly lowered the risk of the primary end point (a composite of death, nonfatal MI, and stroke). n-3 PUFA decreased the relative risk of the primary end point by 15% in four-way analysis (p=0.023). Of note, the dose of n-3 PUFA used in this study (1 gram daily) is the dose recommended for patients with coronary heart disease, but is lower than the dose approved for triglyceride lowering (2-4 gram daily).
, 2033 men with a history of MI received one of three dietary recommendations: (a) reduced fat and increased ratio of polyunsaturated to saturated fat, (b) increased fatty fish intake, or (c) increased fiber intake. The fish group was advised to eat at least 2 portions of fatty fish (300 grams total), corresponding to a weekly intake of about 2.5 grams of eicosapentaenoic acid (EPA). Those who could not tolerate this fish intake were advised to supplement it with fish oil capsules. Those advised to eat fatty fish had a 29% relative decrease in two year all-cause mortality compared with the other two groups. The GISSI trial randomized 11,324 patients with a history of MI to n-3 polyunsaturated fatty acids (PUFA) (1 gram daily), vitamin E (300 mg daily), both, or none for 3.5 years. n-3 PUFA, but not vitamin E, significantly lowered the risk of the primary end point (a composite of death, nonfatal MI, and stroke). n-3 PUFA decreased the relative risk of the primary end point by 15% in four-way analysis (p=0.023). Of note, the dose of n-3 PUFA used in this study (1 gram daily) is the dose recommended for patients with coronary heart disease, but is lower than the dose approved for triglyceride lowering (2-4 gram daily).")
67
PUFA (GISSI-Prevenzione)
11324 pz con recente IMA sono stati randomizzati a ricevere un trattamento a base di acidi grassi polinsaturi n-3 (PUFA) (1 g/die), vitamina E (300 mg/die), la loro combinazione oppure niente. Follow-up di 3.5 anni. End point primario: misura combinata di mortalità totale, ictus cerebrale e reinfarto non fatale. RISULTATI : N-3 PUFA: - 20 % mortalità totale, - 30 % mortalità cardiovascolare, - 45 % morte improvvisa. - Non variazione significativa di eventi non fatali come reinfarto ed ictus. Vitamina E: lieve riduzione non significativa dell’end point combinato. PUFA + Vitamina E: stessi risultati del gruppo PUFA.
 (1 g/die), vitamina E (300 mg/die), la loro combinazione oppure niente. Follow-up di 3.5 anni. End point primario: misura combinata di mortalità totale, ictus cerebrale e reinfarto non fatale. RISULTATI : N-3 PUFA: - 20 % mortalità totale, - 30 % mortalità cardiovascolare, - 45 % morte improvvisa. - Non variazione significativa di eventi non fatali come reinfarto ed ictus. Vitamina E: lieve riduzione non significativa dell’end point combinato. PUFA + Vitamina E: stessi risultati del gruppo PUFA.")
68
Terapia farmacologica prevenzione terziaria
Statine Beta bloccanti ASA Clopidogrel ACE inibitori Omega3 Effetti sulla mortalità a 6 mesi a seconda del livello di appropriatezza Da Mukherjee et al., Heart Modificata

69
Conclusioni Il trattamento aggressivo dei fattori di rischio dopo un a sindrome coronarica acuta è dimostrato che: - migliora la sopravvivenza , - riduce la probabilità di eventi. A tal scopo ogni sforzo dovrebbe essere fatto per far sì che tutti i pazienti ricevano l’ adeguato trattamento ( evidence-based) raccomandato dalle linee guida e continuarlo per tutta la vita a meno che non esistano controindicazioni o intolleranza. E’ chiaro che il trattamento farmacologico deve essere associato ad un cambiamento dello stile di vita del paziente . In questo caso potremo ottenere un vero miglioramento della qualità di vita. Questo è possibile : aumentando l’aderenza alle linee guida ( registro) ambulatorio di follow-up dedicato collaborazione e integrazione ospedale-territorio
 raccomandato dalle. linee guida e continuarlo per tutta la vita a meno che non esistano. controindicazioni o intolleranza. E’ chiaro che il trattamento farmacologico deve essere associato. ad un cambiamento dello stile di vita del paziente . In questo caso potremo ottenere un vero miglioramento della qualità di vita. Questo è possibile : aumentando l’aderenza alle linee guida ( registro) ambulatorio di follow-up dedicato. collaborazione e integrazione ospedale-territorio.")
Presentazioni simili












>")

 N. Pazienti in Dialisi (2002: 308.910)>")




 sottoposto a CABG.>")
