Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
I nuovi obiettivi terapeutici allo studio con statine. Difendiamo il cuore ANMCO – Toscana 9 febbraio 2008 Hotel Le Dune Lido di Camaiore A. Del Carlo

2
05 ottobre 2004 - BMJ 2004; 329: 645 Statine: troppe o troppo poche

3
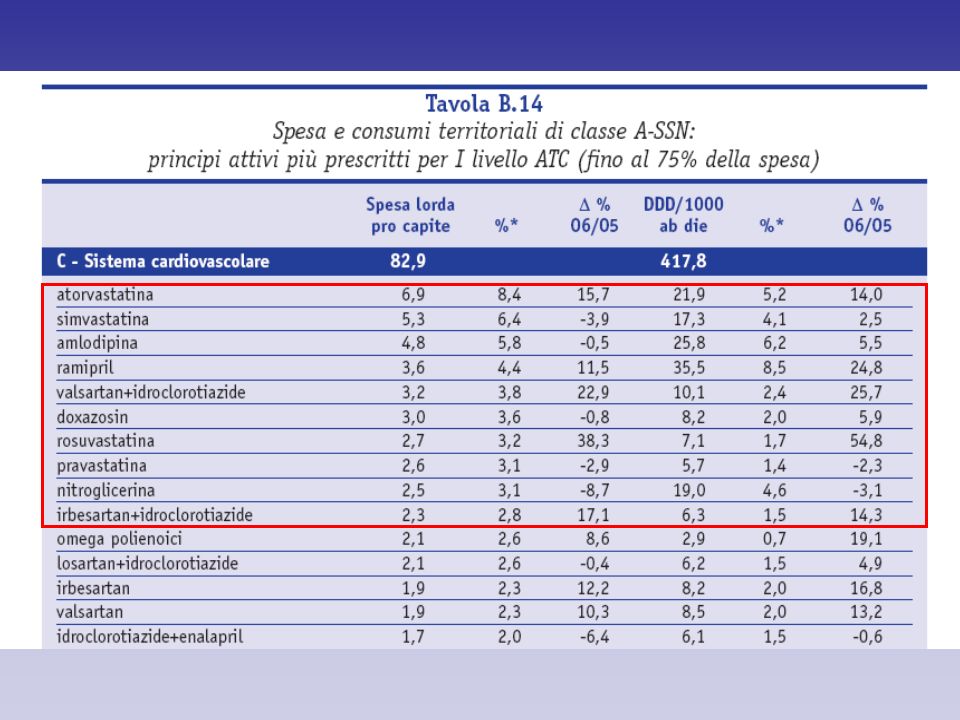
Rapporto OsMed 2006 Costo territoriale per farmaci più elevato: Atorvastatina: da 19,4 a 21,9 DDD Simvastatina stabile su 17 DDD Rosuvastatina da 4,6 a 7,1 DDD Pravastatina da 5,9 a 5,7 DDD

5
Nuove indicazioni allo studio per le signore inibitrici del 3-idrossi-3-metiglutaril Coenzima A reduttasi 1.Nuovi dosaggi (alti!) 2.Nuove indicazioni (oltre CHD) 3.Nuove suggestioni
 2.Nuove indicazioni (oltre CHD) 3.Nuove suggestioni")
6
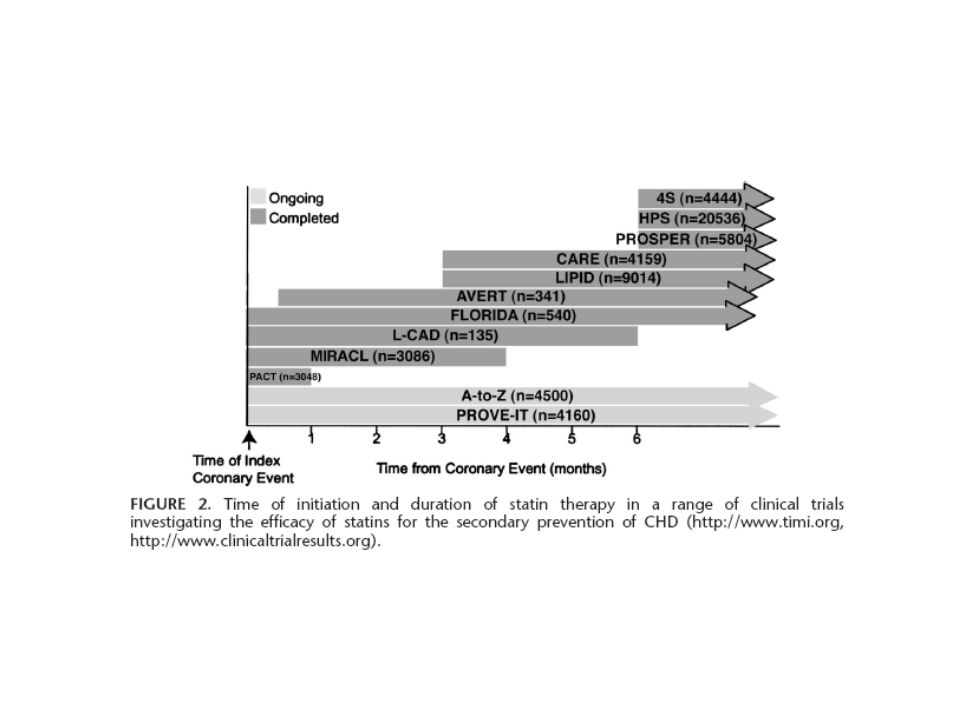
TRIALS con STATINE Acute coronary event MIRACL, PROVE IT 4S, HPS, TNT AFCAPS/TexCAPS, WOSCOPS, ASCOT, CARDS CARE 1, LIPID 2, SEARCH, IDEAL 4 mo No history of CADUnstable CAD Randomization: 24–96 h 3 mo t=0 6 mo Randomization: CARE - 3–20 mo LIPID - 3–36 mo Randomization: >6 mo Stable CAD Primary prevention Secondary prevention Schwartz GG et al. Am J Cardiol 1998;81:578–581. Duration of follow-up: 1 5.0 years; 2 6.1 years; 3 5.4 years. Cooyright 2000 – 2004 QUBIsoft

8
Figure 1. Median Low-Density Lipoprotein (LDL) Cholesterol Levels during the Study. PROVE IT – TIMI 22

9
Figure 2. Kaplan–Meier Estimates of the Incidence of the Primary End Point of Death from Any Cause or a Major Cardiovascular Event. Intensive lipid lowering with the 80-mg dose of atorvastatin, as compared with moderate lipid lowering with the 40-mg dose of pravastatin, reduced the hazard ratio for death or a major cardiovascular event by 16 percent. PROVE IT – TIMI 22

10
Figure 3. Hazard Ratio for the the Primary End Point of Death from Any Cause or a Major Cardiovascular Event at 30, 90, and 180 Days and at the End of Follow-up in the High-Dose Atorvastatin Group, as Compared with the Standard-Dose Pravastatin Group. Event rates are Kaplan–Meier estimates censored at the time points indicated with the use of the average duration of follow-up (two years). CI denotes confidence interval. PROVE IT – TIMI 22
. CI denotes confidence interval. PROVE IT – TIMI 22.")
11
Figure 4. Estimates of the Hazard Ratio for the Secondary End Points and the Individual Components of the Primary End Point in the High-Dose Atorvastatin Group, as Compared with the Standard-Dose Pravastatin Group. CI denotes confidence interval, CHD coronary heart disease, and MI myocardial infarction. Revascularization was performed at least 30 days after randomization.

12
Ideal study Prev. sec. Atorva 80 vs Simva 20 o 40 Table 1. Lipid Levels During Treatment Atorvastatin mg/dL (mmol/L) Simvastatin mg/dL (mmol/L) LDL- cholesterol81 (2.1)104 (2.7) HDL- cholesterol47 (1.22)46 (1.19) HDL = high-density lipoprotein; LDL = low-density lipoprotein
 Simvastatin mg/dL (mmol/L) LDL- cholesterol81 (2.1)104 (2.7) HDL- cholesterol47 (1.22)46 (1.19) HDL = high-density lipoprotein; LDL = low-density lipoprotein.")
13
Ideal study Table 2. Primary Composite Endpoint Simvastatin (%)Atorvastatin (%)HR95% CIP Value Major coronary event10.49.30.890.78-1.01.07 CHD death4.03.90.990.80-1.22.90 Nonfatal MI7.26.00.830.71-0.98).02 Cardiac arrest with resuscitation0.2 CHD = coronary heart disease; CI = confidence interval; HR = hazard ratio; MI = myocardial infarction
Atorvastatin (%)HR95% CIP Value Major coronary event CHD death Nonfatal MI ).02 Cardiac arrest with resuscitation0.2 CHD = coronary heart disease; CI = confidence interval; HR = hazard ratio; MI = myocardial infarction.")
14
Atorvastatin 80 mg n=4,995 Atorvastatin 80 mg n=4,995 Primary Endpoint: Major cardiovascular event defined as coronary heart death (CHD), nonfatal MI, resuscitated cardiac arrest, and fatal or nonfatal stroke at a mean follow-up of 4.9 years. Secondary Endpoint: Major coronary events, cerebrovascular events, hospitalization for congestive heart failure (CHF), all-cause mortality, peripheral artery disease, any cardiovascular event, any coronary event Primary Endpoint: Major cardiovascular event defined as coronary heart death (CHD), nonfatal MI, resuscitated cardiac arrest, and fatal or nonfatal stroke at a mean follow-up of 4.9 years. Secondary Endpoint: Major coronary events, cerebrovascular events, hospitalization for congestive heart failure (CHF), all-cause mortality, peripheral artery disease, any cardiovascular event, any coronary event TNT Trial Presented at ACC 2005 Atorvastatin 10 mg n=5,006 Atorvastatin 10 mg n=5,006 10,003 patients with stable coronary heart disease Age 35-75 years, LDL between 130 and 250 mg/dL, triglyceride 600 mg/dL 19% female, mean age 60.3 years All received atorvastatin 10 mg during 8 week open-label run-in period 10,003 patients with stable coronary heart disease Age 35-75 years, LDL between 130 and 250 mg/dL, triglyceride 600 mg/dL 19% female, mean age 60.3 years All received atorvastatin 10 mg during 8 week open-label run-in period
, all-cause mortality, peripheral artery disease, any cardiovascular event, any coronary event Primary Endpoint: Major cardiovascular event defined as coronary heart death (CHD), nonfatal MI, resuscitated cardiac arrest, and fatal or nonfatal stroke at a mean follow-up of 4.9 years. Secondary Endpoint: Major coronary events, cerebrovascular events, hospitalization for congestive heart failure (CHF), all-cause mortality, peripheral artery disease, any cardiovascular event, any coronary event TNT Trial Presented at ACC 2005 Atorvastatin 10 mg n=5,006 Atorvastatin 10 mg n=5,006 10,003 patients with stable coronary heart disease Age years, LDL between 130 and 250 mg/dL, triglyceride 600 mg/dL 19% female, mean age 60.3 years All received atorvastatin 10 mg during 8 week open-label run-in period 10,003 patients with stable coronary heart disease Age years, LDL between 130 and 250 mg/dL, triglyceride 600 mg/dL 19% female, mean age 60.3 years All received atorvastatin 10 mg during 8 week open-label run-in period.")
15
TNT Trial: Primary endpoint The primary composite endpoint of CHD death, nonfatal MI, resuscitated cardiac arrest, and fatal or nonfatal stroke was lower in the high-dose atorvastatin 80 mg group at a mean follow-up of 4.9 years. Hazard Ratio [HR]=0.78 p<0.001 Presented at ACC 2005

16
TNT Trial: Primary Endpoint p=0.09 p=0.004 p=0.89 p=0.02 The individual components of the primary endpoint were also lower or tended to be lower in the high-dose group compared to the low-dose group with the exception of resuscitation after cardiac arrest, which was the equal in both groups. Presented at ACC 2005

17
MIRACL: study design Hospitalization for unstable angina or non-Q MI n=3086 Randomized 24–96 hours after admission Placebo + diet Atorvastatin 80 mg + diet 16 weeks Assessments conducted at weeks 0, 2, 6 and 16 Schwartz GG et al. Am J Cardiol 1998;81:578–581.

18
MIRACL: plasma LDL-C values at baseline, 6 and 16 weeks *p<0.0001 vs placebo at 6 and 16 weeks. Schwartz GG et al. Jama 2001; 285: 1711-1718 0 60 120 180 240 Baseline6 WeeksEnd of study LDL-C (mg/dL) * * Atorvastatin 80 (- 40%) Placebo Cooyright 2000 – 2004 QUBIsoft
 * * Atorvastatin 80 (- 40%) Placebo Cooyright 2000 – 2004 QUBIsoft.")
19
MIRACL: primary efficacy measure Relative risk = 0.84 p=0.048 Atorvastatin Placebo 0 5 10 15 0481216 Time since randomization (weeks) Cumulative Incidence (%) Time to first occurrence of: Death (any cause) Nonfatal MI Resuscitated cardiac arrest Worsening angina with new objective evidence requiring urgent rehospitalization 17.4% 14.8% Schwartz GG et al. Jama 2001; 285: 1711-1718 Cooyright 2000 – 2004 QUBIsoft

20
MIRACL: worsening angina with new objective evidence of ischemia requiring urgent rehospitalization 0 3 6 9 0481216 Time since randomization (weeks) Cumulative Incidence (%) Relative risk = 0.74 p=0.02 Atorvastatin Placebo 8.4% 6.2% Schwartz GG et al. Jama 2001; 285: 1711-1718

21
MIRACL: fatal or nonfatal stroke 0 0.5 1 1.5 2 0481216 Time since randomization (weeks) Cumulative Incidence (%) Relative risk = 0.50 p=0.045 Atorvastatin Placebo 1.6% 0.8% Schwartz GG et al. Jama 2001; 285: 1711-1718

23
Is lower better?

24
SAGE Trial: Background The purpose of the SAGE study was to compare the effects of intensive versus moderate statin therapy on the reduction of myocardial ischemia, as assessed by ambulatory ECG, in older men and women with stable CAD. Deedwania et al. Circulation. 2007 Feb 13; 115: 700 - 707.

25
SAGE Trial: Study Design Primary Efficacy Parameter: Absolute change from baseline in total duration of myocardial ischemia on 48-hour Holter Monitor Primary Efficacy Parameter: Absolute change from baseline in total duration of myocardial ischemia on 48-hour Holter Monitor Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Primary Efficacy Parameter: Absolute change from baseline in total duration of myocardial ischemia on 48-hour Holter Monitor Primary Efficacy Parameter: Absolute change from baseline in total duration of myocardial ischemia on 48-hour Holter Monitor Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Atorvastatin 80 mg/d n=377 Atorvastatin 80 mg/d n=377 Pravastatin 40 mg/d n=374 Pravastatin 40 mg/d n=374 893 ambulatory CAD patients 65-85 years with 1 MI that lasted 3 minutes during 48- hour ambulatory ECG at screening Prospective. Randomized. Double-blind. Double-dummy. Multi-Center. International. Mean follow-up 12 months 893 ambulatory CAD patients 65-85 years with 1 MI that lasted 3 minutes during 48- hour ambulatory ECG at screening Prospective. Randomized. Double-blind. Double-dummy. Multi-Center. International. Mean follow-up 12 months R 3 and 12 mos. follow-up Deedwania et al. Circulation. 2007 Feb 13; 115: 700 - 707.
 the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Primary Efficacy Parameter: Absolute change from baseline in total duration of myocardial ischemia on 48-hour Holter Monitor Primary Efficacy Parameter: Absolute change from baseline in total duration of myocardial ischemia on 48-hour Holter Monitor Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Secondary Efficacy Parameters: (1) absolute change in total duration of ischemia from baseline to month 3; from baseline to month 3 and to month 12: (2) the % change in total duration of ischemia, (3) the absolute and % change in no. of ischemic episodes, (4) the % change in ischemic burden, (5) the proportion of patients who were totally free of ischemia, and (6) the % change in the levels of total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides, and apolipoprotein B. Atorvastatin 80 mg/d n=377 Atorvastatin 80 mg/d n=377 Pravastatin 40 mg/d n=374 Pravastatin 40 mg/d n= ambulatory CAD patients years with 1 MI that lasted 3 minutes during 48- hour ambulatory ECG at screening Prospective. Randomized. Double-blind. Double-dummy. Multi-Center. International. Mean follow-up 12 months 893 ambulatory CAD patients years with 1 MI that lasted 3 minutes during 48- hour ambulatory ECG at screening Prospective. Randomized. Double-blind. Double-dummy. Multi-Center. International. Mean follow-up 12 months R 3 and 12 mos. follow-up Deedwania et al. Circulation Feb 13; 115:")
26
SAGE Trial: Primary Efficacy Endpoint Atorvastatin (n=408) Atorvastatin (n=408) Pravastatin (n=396) Pravastatin (n=396) Baseline Month 3 Month 12 The total duration of myocardial ischemia at month 12 was significantly reduced from baseline in both atorvastatin- and pravastatin-treated patients. There was no significant difference between atorvastatin and pravastatin. Total duration of Myocardial Ischemia (min) Mean total duration of myocardial ischemia over 48 hours P<0.001 Deedwania et al. Circulation. 2007 Feb 13; 115: 700 - 707.
 Mean total duration of myocardial ischemia over 48 hours P<0.001 Deedwania et al. Circulation Feb 13; 115:")
27
SAGE Trial: Lipid Parameters TotalLDLHDL Least Squares Mean Percent Changes in Lipid Parameters from Baseline p=0.009 p<0.001 p<0.001 AtorvastatinAtorvastatin Atorvastatin PravastatinPravastatin Pravastatin Month 3 Month 12 Deedwania et al. Circulation. 2007 Feb 13; 115: 700 - 707. LS mean percent change

28
Statine e stroke

29
Efficacia delle statine nella prevenzione dellictus Zhou et al. Am H J. 2006; 151:273-81. Studi su simvastatina 4S0,74(0,52 – 1,94) HPS0,76(0,67 – 0,86) Unificati (IC 95%)0,76(0,69 – 0,85) Studi su pravastatina CARE0,60(0,40 – 0,57) LIPID0,03(0,60 – 1,61) PROSPER1,04(0,02 – 1,31) WOSCOPS0,90(0,61 – 1,34) Unificati (IC 95%)0,87(0,76 – 1,02) Con ALLHAT-LLT ALLHAT-LLT0,91(0,76 – 1,09) CARE0,60(0,40 – 0,97) LIPID0,01(0,60 – 1,01) PROSPER1,04(0,02 – 1,31) WOSCOPS0,90(0,61 – 1,34) Unificati (IC 95%)0,66(0,73 – 0,55) Studi su atorvastatina ASCOT-LLA0,75(0,56 – 0,95) CARDS0,53(0,51 – 0,90) Unificati (IC 95%)0,68(0,55 – 0,88) Con GREACE ASCOT-ILA0,73(0,56 – 0,96) CARDS0,53(0,31 – 0,90) GREACE0,53(0,34 – 1,16) Unificati (IC 95%)0,68(0,59 – 0,06) 0,20,51,02,05,0 RR e IC 95% sulla base di un modello per effetti random Eventi cerebrovascolari maggiori (ictus fatali e non fatali) A favore del controllo A favore della statina RR 0,76 0,87 0,68 0,88 0,68
 HPS0,76(0,67 – 0,86) Unificati (IC 95%)0,76(0,69 – 0,85) Studi su pravastatina CARE0,60(0,40 – 0,57) LIPID0,03(0,60 – 1,61) PROSPER1,04(0,02 – 1,31) WOSCOPS0,90(0,61 – 1,34) Unificati (IC 95%)0,87(0,76 – 1,02) Con ALLHAT-LLT ALLHAT-LLT0,91(0,76 – 1,09) CARE0,60(0,40 – 0,97) LIPID0,01(0,60 – 1,01) PROSPER1,04(0,02 – 1,31) WOSCOPS0,90(0,61 – 1,34) Unificati (IC 95%)0,66(0,73 – 0,55) Studi su atorvastatina ASCOT-LLA0,75(0,56 – 0,95) CARDS0,53(0,51 – 0,90) Unificati (IC 95%)0,68(0,55 – 0,88) Con GREACE ASCOT-ILA0,73(0,56 – 0,96) CARDS0,53(0,31 – 0,90) GREACE0,53(0,34 – 1,16) Unificati (IC 95%)0,68(0,59 – 0,06) 0,20,51,02,05,0 RR e IC 95% sulla base di un modello per effetti random Eventi cerebrovascolari maggiori (ictus fatali e non fatali) A favore del controllo A favore della statina RR 0,76 0,87 0,68 0,88 0,68.")
30
Riduzione % Del rischio di ictus (n=444)(n=585) 4.3 5.7 -25%(p=0,0001) Heart Protection Study con simvastatina 40mg Riduzione del rischio di ictus TUTTI I PAZIENTI
(n=585) %(p=0,0001) Heart Protection Study con simvastatina 40mg Riduzione del rischio di ictus TUTTI I PAZIENTI")
31
CARDS: atorvastatina 10 e ictus in pazienti diabetici senza CHD Modificato da Colhoun HM et al. Lancet. 2004; 364:685-696; Newman C et al. Accettato per presentazione allAmerican Heart Association Scientific Sessions 2005; Dallas, TX. 13-16 novembre 2005. Endpoint primario127 (9,0)83 (5,8)–37% (–52, –17) Eventi coronarici acuti77 (5,5) 51 (3,6)–36% (–55, –9) Rivascolarizzazione coronarica34 (2,4)24 (1,7)–1% (–59, +16) Ictus39 (2,8)21 (1,5)–48% (–69, –11) * Numero di pazienti con evento (%). 0,40,60,81,01,2 EventoPlacebo*Atorva*Rapporto di rischioRischio relativo (IC) A favore placeboA favore atorvastatina 0,2 (n=2.841) p=0,001
83 (5,8)–37% (–52, –17) Eventi coronarici acuti77 (5,5) 51 (3,6)–36% (–55, –9) Rivascolarizzazione coronarica34 (2,4)24 (1,7)–1% (–59, +16) Ictus39 (2,8)21 (1,5)–48% (–69, –11) * Numero di pazienti con evento (%). 0,40,60,81,01,2 EventoPlacebo*Atorva*Rapporto di rischioRischio relativo (IC) A favore placeboA favore atorvastatina 0,2 (n=2.841) p=0,001.")
32
PROSPER è il primo studio disegnato specificatamente per valutare il trattamento con una statina nei pazienti molto anziani a rischio vascolare Razionale PROSPER Study Group. Lancet. 2002 Prospective Study of Pravastatin in the Elderly at Risk (PROSPER)
.")
33
PROSPER Study Group Obiettivo dello studio PROSPER Study Group Obiettivo dello studio Determinare se pravastatina al dosaggio di 40 mg/die riduca gli eventi cardio e cerebro vascolari (morte, IMA, ictus) nei pazienti anziani ad alto rischio o affetti da patologia vascolare. Follow up medio 3,2 a. PROSPER Study Group. Lancet. 2002

34
5804 pazienti (70–82 anni) ad alto rischio Terapia: pravastatina 40 mg vs. placebo 19% di riduzione di eventi coronarici maggiori 24% riduzione di mortalità cardiovascolare 25% riduzione in TIA (non stroke riduzione) Shepherd J et al. Lancet 2002;360:1623–1630. Risultati
 Shepherd J et al. Lancet 2002;360:1623–1630. Risultati.")
35
Statine e ictus cerebrale * p<0,001 Le statine riducono apparentemente tutti gli ictus del 20%, ma tale riduzione è dovuta a una riduzione del 28% dellictus tromboembolico. Ciò spiega perché la riduzione degli ictus per effetto delle statine sia stata osservata soprattutto negli studi condotti in pazienti con pregresse malattie cardiovascolari, nei quali è più frequente lictus ischemico. Trials randomizzati CategoriaNo. trialsNo. eventi Variazione % del rischio (IC 95%) Tutti gli ictus 413.319-20* (-14/-26) Tutti gli ictus nei pazienti con pregresse malattie cardiovascolari 322.311-22* (-28/-16) Tutti gli ictus nei pazienti senza pregresse malattie cardiovascolari 7752-6 (-22/14) Ictus tromboembolico 81.204-28* (-35/-20) Ictus emorragico 8149-3 (-35/47) Ictus fatale 56678-2 (-17/16) Ictus non fatale 402.519-23* (-29/-16) Law MR et al. Br Med J. 2003; 326:1423-9.
 Tutti gli ictus * (-14/-26) Tutti gli ictus nei pazienti con pregresse malattie cardiovascolari * (-28/-16) Tutti gli ictus nei pazienti senza pregresse malattie cardiovascolari (-22/14) Ictus tromboembolico * (-35/-20) Ictus emorragico (-35/47) Ictus fatale (-17/16) Ictus non fatale * (-29/-16) Law MR et al. Br Med J. 2003; 326:")
36
Stroke reduction results from large secondary prevention studies and meta-analyses of statins 4S, CARE, LIPID Clin Med Card –FI adapted from Cucchiara et al, Stroke 2001 -35% Relative Risk Reduction -20% -25% -15% -10% -5% 0% -30% Secondary Prevention Studies Meta-Analyses 4S CARE LIPID Blauw et alCrouse III et al -30% -32% -19% -31% -27%

37
La terapia con statine non è associata ad aumento del rischio di ictus emorragico * Simvastatina vs placebo. Atorvastatina vs cure abituali. Atorvastatina vs placebo. § Pravastatina vs trattamento convenzionale. II Pravastatina vs placebo. ¶ Lovastatina vs placebo. Amarenco P et al. Stroke. 2004; 35:2902-2909; Yano K et al. Stroke. 1989; 20:1460-1465; Iso H et al. N Engl J Med. 1989; 320:904-910. HPS* GREACE MIRACL KLIS § LIPID ıı CARE ıı SSSS* AFCAPS ¶ Complessivo (IC 95%) Eterogeneità Trial 0,050,20,51,010,0 Odds ratio (IC 95%) A favore del controllo A favore della statina 3,0 0,90 (0,65–1,22) p=0,15
 Eterogeneità Trial 0,050,20,51,010,0 Odds ratio (IC 95%) A favore del controllo A favore della statina 3,0 0,90 (0,65–1,22) p=0,15.")
38
Randomly assigned 4,731 patients who had had a stroke or TIA within 1 to 6 months before the study entry, had low LDL levels (100-190 mg/dL) and had no knonw CHD 2,365 atorvastatin 80 mg 2,366 placebo Median follow-up time: 4.9 years SPARCL investigators, N Engl J Med 2006
 and had no knonw CHD 2,365 atorvastatin 80 mg 2,366 placebo Median follow-up time: 4.9 years SPARCL investigators, N Engl J Med 2006")
39
3 5 0 Years Fatal or non-fatal stroke (%) 8 12 16 20 4 0 Placebo (n=2,366) Atorvastatin (n=2,365) HR 0.84 (0.71-0.99) p<0.0001 Kaplan-Meier for fatal or non-fatal stroke in the SPARCL study (n=4,731); follow-up 4.9 years SPARCL investigators, N Engl J Med 2006
 Placebo (n=2,366) Atorvastatin (n=2,365) HR 0.84 ( ) p< Kaplan-Meier for fatal or non-fatal stroke in the SPARCL study (n=4,731); follow-up 4.9 years SPARCL investigators, N Engl J Med 2006")
40
3 5 0 Years Stroke or TIA event (%) 10 15 20 25 5 0 Placebo (n=2,366) Atorvastatin (n=2,365) HR 0.77 (0.67-0.88) p<0.0001 Kaplan-Meier for stroke or TIA in the SPARCL study (n=4,731); follow-up 4.9 years SPARCL investigators, N Engl J Med 2006
 Placebo (n=2,366) Atorvastatin (n=2,365) HR 0.77 ( ) p< Kaplan-Meier for stroke or TIA in the SPARCL study (n=4,731); follow-up 4.9 years SPARCL investigators, N Engl J Med 2006")
41
SPARCL: Main results Welch M et al. 15th European Stroke Conference; May 16-19, 2006; Brussels, Belgium. Type of stroke Hazard ratio with atorvastatin Any 0.84 Fatal 0.57 Nonfatal0.87 Ischemic0.78 Hemorrhagic Nessuna riduzione della morte globale 1.66

42
SPARCL LIncremento di stroke emorragico è dovuto alleffetto pleiotropico antiaggregante? I dati in letteratura sono ancora controversi (HPS +; Prosper -) Il Pharmacovigilance Working Party dellEMEA probabilmente inserirà una modifica sul riassunto delle caratteristiche del prodotto.
 Il Pharmacovigilance Working Party dellEMEA probabilmente inserirà una modifica sul riassunto delle caratteristiche del prodotto..")
43
Statine e scompenso cardiaco Small prospective clinical studies of atorvastatin and simvastatin in systolic HF are promising, documenting improved ventricular systolic function and decreased inflammatory biomarkers with statin therapy. Expert Opin Pharmacother. 2007 Dec;8(17):3061-8. Links Atorvastatin and statins in the treatment of heart failure. Horwich TBHorwich TB, MacLellan WR.MacLellan WR
: Links Atorvastatin and statins in the treatment of heart failure. Horwich TBHorwich TB, MacLellan WR.MacLellan WR.")
44
Rosuvastatina e rimodellamento ventricolare Despite being safe and effective at decreasing plasma cholesterol, high-dose ROS did not beneficially alter parameters of LV remodeling. J Card Fail. 2007 Feb;13(1):1-7. Double-blind, randomized, placebo-controlled study of high-dose HMG CoA reductase inhibitor therapy on ventricular remodeling, pro-inflammatory cytokines and neurohormonal parameters in patients with chronic systolic heart failure. Krum HKrum H, Ashton E, Reid C, Kalff V, Rogers J, Amarena J, Singh B, Tonkin A.Ashton EReid CKalff VRogers JAmarena JSingh BTonkin A
:1-7. Double-blind, randomized, placebo-controlled study of high-dose HMG CoA reductase inhibitor therapy on ventricular remodeling, pro-inflammatory cytokines and neurohormonal parameters in patients with chronic systolic heart failure. Krum HKrum H, Ashton E, Reid C, Kalff V, Rogers J, Amarena J, Singh B, Tonkin A.Ashton EReid CKalff VRogers JAmarena JSingh BTonkin A.")
45
Studio CORONA Rosu 10 vs plb – paz. > 60 aa scompenso ischemico Rosuvastatin did not reduce the primary outcome or the number of deaths from any cause in older patients with systolic heart failure, although the drug did reduce the number of cardiovascular hospitalizations. N Engl J Med. 2007 Nov 29;357(22):2301-4. Rosuvastatin in older patients with systolic heart failure. Kjekshus JKjekshus J, Apetrei E, Barrios V, Böhm M, Cleland JG, Cornel JH, Dunselman P, Fonseca C, Goudev A, Grande P, Gullestad L, Hjalmarson A, Hradec J, Jánosi A, Kamenský G, Komajda M, Korewicki J, Kuusi T, Mach F, Mareev V, McMurray JJ, Ranjith N, Schaufelberger M, Vanhaecke J, van Veldhuisen DJ, Waagstein F, Wedel H, Wikstrand J; CORONA Group.Apetrei EBarrios VBöhm MCleland JGCornel JHDunselman PFonseca CGoudev A Grande PGullestad LHjalmarson AHradec JJánosi AKamenský GKomajda MKorewicki JKuusi TMach FMareev VMcMurray JJRanjith NSchaufelberger MVanhaecke Jvan Veldhuisen DJ Waagstein FWedel HWikstrand JCORONA Group
: Rosuvastatin in older patients with systolic heart failure. Kjekshus JKjekshus J, Apetrei E, Barrios V, Böhm M, Cleland JG, Cornel JH, Dunselman P, Fonseca C, Goudev A, Grande P, Gullestad L, Hjalmarson A, Hradec J, Jánosi A, Kamenský G, Komajda M, Korewicki J, Kuusi T, Mach F, Mareev V, McMurray JJ, Ranjith N, Schaufelberger M, Vanhaecke J, van Veldhuisen DJ, Waagstein F, Wedel H, Wikstrand J; CORONA Group.Apetrei EBarrios VBöhm MCleland JGCornel JHDunselman PFonseca CGoudev A Grande PGullestad LHjalmarson AHradec JJánosi AKamenský GKomajda MKorewicki JKuusi TMach FMareev VMcMurray JJRanjith NSchaufelberger MVanhaecke Jvan Veldhuisen DJ Waagstein FWedel HWikstrand JCORONA Group.")
46
Rimaniamo in attesa …. …dei risultati del GISSI – HF Paz. con diagnosi di SC randomizzati a n3 PUFA, Rosuvastatina e Placebo. Follow up di 3 aa.

47
Statine e glaucoma Arch Ophthalmol. 2004 Jun;122(6):822-6. Links Statins and other cholesterol-lowering medications and the presence of glaucoma. McGwin G JrMcGwin G Jr, McNeal S, Owsley C, Girkin C, Epstein D, Lee PP.McNeal SOwsley CGirkin CEpstein DLee PP Studio caso-controllo: Sia luso di Statine che altri ipolipemizzanti indicherebbero la riduzione del rischio di glaucoma ad angolo aperto.

48
Statine e maculopatia Br J Ophthalmol. 2003 Sep;87(9):1121-5. Links The association between statin use and age related maculopathy. McGwin G JrMcGwin G Jr, Owsley C, Curcio CA, Crain RJ.Owsley CCurcio CACrain RJ Studio caso – controllo Possibile correlazione tra uso di statine e maculopatia.

49
Statine e rischio di frattura Calcif Tissue Int. 2006 Jul;79(1):27-36. Epub 2006 Jul 24. Links Statin but not non-statin lipid-lowering drugs decrease fracture risk: a nation-wide case-control study. Rejnmark LRejnmark L, Vestergaard P, Mosekilde L.Vestergaard PMosekilde L La correlazione è presente per tutte le statine eccetto la Prava e le non-statine.

50
Statine e cancro pancreatico Pancreas. 2007 Mar;34(2):260-5. Links Statins reduce the risk of pancreatic cancer in humans: a case- control study of half a million veterans. Khurana VKhurana V, Sheth A, Caldito G, Barkin JS.Sheth ACaldito GBarkin JS Effetto protettivo con riduzione statistica del 67% per > 6 mesi e fino all80% > 4 anni !!!

51
Statine e cancro prostatico Am J Epidemiol. 2005 Aug 15;162(4):318-25. Epub 2005 Jul 13. Links Statins and prostate cancer risk: a case-control study. Shannon JShannon J, Tewoderos S, Garzotto M, Beer TM, Derenick R, Palma A, Farris PE.Tewoderos SGarzotto MBeer TMDerenick RPalma A Farris PE Correlazione favorevole in particolare per cancri aggressivi. J Natl Cancer Inst. 2006 Dec 20;98(24):1819-25. Links Statin drugs and risk of advanced prostate cancer. Platz EAPlatz EA, Leitzmann MF, Visvanathan K, Rimm EB, Stampfer MJ, Willett WC, Giovannucci E.Leitzmann MFVisvanathan KRimm EBStampfer MJ Willett WCGiovannucci E Studio di coorte: correlazione favorevole solo per cancri invasivi e metastatici.
: Links Statin drugs and risk of advanced prostate cancer. Platz EAPlatz EA, Leitzmann MF, Visvanathan K, Rimm EB, Stampfer MJ, Willett WC, Giovannucci E.Leitzmann MFVisvanathan KRimm EBStampfer MJ Willett WCGiovannucci E Studio di coorte: correlazione favorevole solo per cancri invasivi e metastatici..")
52
Statine e cancro colorettale Gastroenterology. 2007 Aug;133(2):393-402. Epub 2007 May 21. Links Risk of colorectal cancer in patients prescribed statins, nonsteroidal anti- inflammatory drugs, and cyclooxygenase-2 inhibitors: nested case-control study. Vinogradova Y, Hippisley-Cox J, Coupland C, Logan RF.Vinogradova YHippisley-Cox JCoupland CLogan RF Correlazione positiva con FANS, non con statine. J Natl Cancer Inst. 2007 Jan 3;99(1):32-40. Links Statin use and risk of colorectal cancer. Coogan PFCoogan PF, Smith J, Rosenberg L.Smith JRosenberg L Nessuna correlazione con statine N Engl J Med. 2005 May 26;352(21):2184-92. Links Statins and the risk of colorectal cancer. Poynter JNPoynter JN, Gruber SB, Higgins PD, Almog R, Bonner JD, Rennert HS, Low M, Greenson JK, Rennert G.Gruber SBHiggins PDAlmog RBonner JDRennert HSLow M Greenson JKRennert G Riduzione RR 47%.
: Links Statin use and risk of colorectal cancer. Coogan PFCoogan PF, Smith J, Rosenberg L.Smith JRosenberg L Nessuna correlazione con statine N Engl J Med May 26;352(21): Links Statins and the risk of colorectal cancer. Poynter JNPoynter JN, Gruber SB, Higgins PD, Almog R, Bonner JD, Rennert HS, Low M, Greenson JK, Rennert G.Gruber SBHiggins PDAlmog RBonner JDRennert HSLow M Greenson JKRennert G Riduzione RR 47%..")
53
Statine e cancro mammario J Natl Cancer Inst. 2006 May 17;98(10):700-7. Links Statin use and breast cancer: prospective results from the Women's Health Initiative. Cauley JACauley JA, McTiernan A, Rodabough RJ, LaCroix A, Bauer DC, Margolis KL, Paskett ED, Vitolins MZ, Furberg CD, Chlebowski RT; Women's Health Initiative Research Group.McTiernan ARodabough RJLaCroix ABauer DC Margolis KLPaskett EDVitolins MZFurberg CDChlebowski RT Women's Health Initiative Research Group Nessuna associazione di classe. Possibile lieve correlazione con statine idrofobiche. Cancer Epidemiol Biomarkers Prev. 2007 Mar;16(3):416-21. Links Statin use and breast cancer risk in a large population-based setting. Boudreau DMBoudreau DM, Yu O, Miglioretti DL, Buist DS, Heckbert SR, Daling JR.Yu OMiglioretti DLBuist DSHeckbert SRDaling JR Nessuna associazione
: Links Statin use and breast cancer risk in a large population-based setting. Boudreau DMBoudreau DM, Yu O, Miglioretti DL, Buist DS, Heckbert SR, Daling JR.Yu OMiglioretti DLBuist DSHeckbert SRDaling JR Nessuna associazione.")
54
Statine e cancro in generale J Natl Cancer Inst. 2008 Jan 16;100(2):134-9. Epub 2008 Jan 8. Links The association between statins and cancer incidence in a veterans population. Farwell WRFarwell WR, Scranton RE, Lawler EV, Lew RA, Brophy MT, Fiore LD, Gaziano JM.Scranton RELawler EVLew RABrophy MTFiore LDGaziano JM Rischio ridotto. Circulation. 2007 Jan 2;115(1):27-33. Epub 2006 Dec 18. Links Statins and the risk of lung, breast, and colorectal cancer in the elderly. Setoguchi SSetoguchi S, Glynn RJ, Avorn J, Mogun H, Schneeweiss S.Glynn RJAvorn JMogun HSchneeweiss S Nessuna correlazione.
: Epub 2006 Dec 18. Links Statins and the risk of lung, breast, and colorectal cancer in the elderly. Setoguchi SSetoguchi S, Glynn RJ, Avorn J, Mogun H, Schneeweiss S.Glynn RJAvorn JMogun HSchneeweiss S Nessuna correlazione..")
55
Statine e demenza Dement Geriatr Cogn Disord. 2007;23(3):194-201. Epub 2007 Jan 25. Links Prevention and treatment of dementia or Alzheimer's disease by statins: a meta-analysis. Zhou BZhou B, Teramukai S, Fukushima M.Teramukai SFukushima M Nessun beneficio su rischio di demenza. Arch Gen Psychiatry. 2005 Feb;62(2):217-24. Links Do statins reduce risk of incident dementia and Alzheimer disease? The Cache County Study. Zandi PPZandi PP, Sparks DL, Khachaturian AS, Tschanz J, Norton M, Steinberg M, Welsh-Bohmer KA, Breitner JC; Cache County Study investigators.Sparks DLKhachaturian ASTschanz JNorton MSteinberg MWelsh-Bohmer KABreitner JCCache County Study investigators Nessuna associazione
: Links Do statins reduce risk of incident dementia and Alzheimer disease. The Cache County Study. Zandi PPZandi PP, Sparks DL, Khachaturian AS, Tschanz J, Norton M, Steinberg M, Welsh-Bohmer KA, Breitner JC; Cache County Study investigators.Sparks DLKhachaturian ASTschanz JNorton MSteinberg MWelsh-Bohmer KABreitner JCCache County Study investigators Nessuna associazione.")
56
Statine e AR Lancet. 2004 Jun 19;363(9426):2015-21. Links Trial of Atorvastatin in Rheumatoid Arthritis (TARA): double-blind, randomised placebo-controlled trial. McCarey DWMcCarey DW, McInnes IB, Madhok R, Hampson R, Scherbakov O, Ford I, Capell HA, Sattar N.McInnes IBMadhok RHampson RScherbakov OFord ICapell HASattar N Piccolo trial (n=116) con breve F.U. (6 mesi). Modesto effetto antiinfiammatorio
: double-blind, randomised placebo-controlled trial. McCarey DWMcCarey DW, McInnes IB, Madhok R, Hampson R, Scherbakov O, Ford I, Capell HA, Sattar N.McInnes IBMadhok RHampson RScherbakov OFord ICapell HASattar N Piccolo trial (n=116) con breve F.U. (6 mesi). Modesto effetto antiinfiammatorio.")
57
Statine e rischio di rabmiolisi Pharmacoepidemiol Drug Saf. 2007 Mar;16(3):352-8. Links Risk factors for statin-associated rhabdomyolysis. Schech SSchech S, Graham D, Staffa J, Andrade SE, La Grenade L, Burgess M, Blough D, Stergachis A, Chan KA, Platt R, Shatin D.Graham DStaffa JAndrade SELa Grenade LBurgess M Blough DStergachis AChan KAPlatt RShatin D Studio caso controllo Soprattutto nelletà avanzata e con fattori aggiunti come alti dosaggi, malattia renale e genere femminile.
: Links Risk factors for statin-associated rhabdomyolysis. Schech SSchech S, Graham D, Staffa J, Andrade SE, La Grenade L, Burgess M, Blough D, Stergachis A, Chan KA, Platt R, Shatin D.Graham DStaffa JAndrade SELa Grenade LBurgess M Blough DStergachis AChan KAPlatt RShatin D Studio caso controllo Soprattutto nelletà avanzata e con fattori aggiunti come alti dosaggi, malattia renale e genere femminile..")
58
FINE Grazie

Presentazioni simili













>")

 N. Pazienti in Dialisi (2002: 308.910)>")



