Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Dott. Antonio Butera Lamezia Terme
U. O. CARDIOLOGIA con UTIC Preparazione farmacologica alla PTCA: STEMI Negli ospedali senza emodinamica Dott. Antonio Butera Lamezia Terme Roma, 20 marzo 2010

2
1 2

4
2009 Facilitaded and Rescue PCI…non longer used…potentially misleading labels

5
Scopi del trattamento farmacologico pre PTCA
Limitazione di eventi e riduzione del danno ischemico pre-PCI “Facilitazione” dell’angioplastica Riduzione delle complicanze peri e post-procedurali (trombosi dello stent, ischemia) (Il tutto con minori effetti pro- emorragici) -I sanguinamenti maggiori moltiplicano MACE: “GRACE” EHJ 2003; Eikelboom JW et al: Circulation 2006; Nikolski E et al: EHJ 2007; “CRUSADE “ Circulation 2009-
 (Il tutto con minori effetti pro- emorragici) -I sanguinamenti maggiori moltiplicano MACE: GRACE EHJ 2003; Eikelboom JW et al: Circulation 2006; Nikolski E et al: EHJ 2007; CRUSADE Circulation")
6
Facilitata

7
Razionale dell’Angioplastica facilitata
La maggiore pervietà dell’IRA prima dell’angioplastica migliora l’outcome 6 months mortality TIMI 3 (n=375) 100% 98% 96% 94% 92% 90% 0.5% TIMI 2 (n=295) 2.8% Survival (%) TIMI 0/1 (n=1,657) 4.4% QUALCHE CONSIDERAZIONE PERò VA FATTA log-rank p for trend = 0.009 Months Stone GW Circulation 2001;104:636
 100% 98% 96% 94% 92% 90% 0.5% TIMI 2 (n=295) 2.8% Survival (%) TIMI 0/1 (n=1,657) 4.4% QUALCHE CONSIDERAZIONE PERò VA FATTA. log-rank p for trend. = Months. Stone GW Circulation 2001;104:636.")
8
ASSENT- 4 PCI: study design
IMA ST (< 6h) n = 2000 n = 2000 ASA + UFH (bolus 40U/kg) + TNK-tPA ASA + UFH (bolus 70u/Kg) Immediate PTCA Immediate PTCA Stent or clopidogrel at researcher’s discretion No anti-GP IIb/IIIa Stent, clopidogrel or anti-GP IIb/IIIa at researcher’s discretion Sospeso in anticipo per eccesso di mortalità intraospedaliera nei pazienti pre trombolisati Primary endpoints: death, heart failure or cardiogenic shock at 90 days Lancet 2006
 n = n = ASA + UFH (bolus 40U/kg) + TNK-tPA. ASA + UFH (bolus 70u/Kg) Immediate PTCA. Immediate PTCA. Stent or clopidogrel. at researcher’s discretion. No anti-GP IIb/IIIa. Stent, clopidogrel or. anti-GP IIb/IIIa. at researcher’s discretion. Sospeso in anticipo per eccesso di mortalità intraospedaliera nei pazienti pre trombolisati. Primary endpoints: death, heart failure. or cardiogenic shock at 90 days. Lancet")
9
TIMI grade 3 flow prior to PCI and TIMI grade 2/3 flow post-PCI (%)
ASSENT- 4 PCI Trial: TIMI Flow Grade TIMI grade 3 flow prior to PCI and TIMI grade 2/3 flow post-PCI (%) p=0.03 TIMI grade 3 flow prior to PCI was present more frequently in the TNK + PCI arm (43.6% vs 15.0%) TIMI grade 2/3 post-PCI was slightly higher in the PCI alone group (95.3% vs 97.6%) p<0.001 Lancet 2006
 p=0.03. TIMI grade 3 flow prior to PCI was present more frequently in the TNK + PCI arm (43.6% vs 15.0%) TIMI grade 2/3 post-PCI was slightly higher in the PCI alone group (95.3% vs 97.6%) p< Lancet")
10
ASSENT-4: Primary Endpoint mortality, CHF, Shock at 90 days
Lancet 2006

11
ASSENT-4 PCI : in-hospital cardiac events
TNK+PCI (%) PCI alone (%) p Re-MI 4.1 1.9 0.01 Abrupt vessel closure 0.1 <0.001 Repeat TVR 4.4 1.0 Pericarditis 0.7 0.07 Tamponade 0.6 0.4 0.50 Cardiac rupture 0.9 0.2 0.11 EM dissociation 1.7 0.20 Pulmonary edema 3.4 3.1 0.78 Ventricular fibrillation 5.6 3.7 0.08 Lancet 2006
 PCI alone (%) p. Re-MI Abrupt vessel closure < Repeat TVR Pericarditis Tamponade Cardiac rupture EM dissociation Pulmonary edema Ventricular fibrillation Lancet")
12
ASSENT-4 PCI: in-hospital stroke rates
Outcome TNK+PCI (%) PCI alone (%) p Total stroke 1.81 <0.001 Intracranial hemorrhage 0.97 0.004 Ischemic stroke 0.60 0.03 Hemorrhagic conversion 0.12 0.50 Unclassified 0.24 0.25 van de Werf F. European Society of Cardiology Congress 2005; September 4-7, 2005; Stockholm, Sweden. Lancet 2006
 PCI alone (%) p. Total stroke < Intracranial hemorrhage Ischemic stroke Hemorrhagic conversion Unclassified van de Werf F. European Society of Cardiology Congress 2005; September 4-7, 2005; Stockholm, Sweden. Lancet")
13
Conclusioni ASSENT - 4

14
Major Objectives 1° - To test if Reteplase/Abciximab Facilitated PCI is superior to Primary PCI with in lab Abciximab Primary end-point:mortality, CHF, VF, Shock at 90 days Primary PCI with in lab Abciximab Abciximab Facilitated Primary PCI To test if Reteplase/Abciximab is superior to facilitation with Abciximab alone To test if Abciximab facilitation is superior to Primary PCI with in lab Abciximab 2°: ? R ? Reteplase ½ dose Reteplase/Abciximab Facilitated Primary PCI NEJM 2008

15
TIMI Flow in IRA Pre-PCI % Subjects with TIMI 2/3 (Patency) Pre-PCI
61 % Percentage 25 % TIMI 2 TIMI 3 25 % 26 % 11 % 36 % 12 % 15 % 13 % Primary PCI (in lab Abciximab) (n=790) Abciximab Facilitated PCI (n=809) Reteplase/Abciximab Facilitated PCI (n=815)
 (n=790) Abciximab Facilitated PCI (n=809) Reteplase/Abciximab Facilitated PCI (n=815)")
16
Primary Endpoint: mortality, CHF, VF, Shock at 90 days

17
TIMI Major or Minor Bleeding (nonintracranial) through Discharge/Day7
p<0.001 p<0.001 p=0.025 p=0.008 p=0.006 p=0.547 p=0.141 p=0.025 p=0.127

18
CONCLUSIONI …il rapporto rischio/beneficio della pPCI con Abciximab somministrato direttamente in emodinamica è migliore delle due strategie di facilitazione…

20
(19 studi)
")
21
Ma se la pPCI non si potesse proprio fare…
Ma se la pPCI non si potesse proprio fare….specialmente nei pazienti ad alto rischio…

22
CARESS Study design Urgent transfer after lysis to nearest PCI centre
STEMI patients <12 hrs from symptom onset Admitted to centres without PCI facilities and at least one high risk feature: >15 mm ST Elevation new onset LBBB, previous MI, Killip Class >2, < 35% LVEF ASA mg iv; Reteplase half dose; UFH (40 U/kg -max 3000-; 7 U/kg/h); Abciximab 0.25 mg/kg bolus mg/kg/min x 12 h Urgent transfer after lysis to nearest PCI centre for PCI plus stenting Admit to CCU and only transfer for PCI if persistent ST elevation at 90 min (>50% basal ECG), chest pain or haemodynamic compromise 600 pazienti Primary outcome: Death, Reinfarction, Refractory Ischemia at 30 Days Lancet 2008
; Abciximab 0.25 mg/kg bolus mg/kg/min x 12 h. Urgent transfer after. lysis to nearest PCI centre. for PCI plus stenting. Admit to CCU and only. transfer for PCI if persistent. ST elevation at 90 min (>50% basal ECG), chest pain or haemodynamic compromise. 600 pazienti. Primary outcome: Death, Reinfarction, Refractory Ischemia at 30 Days. Lancet")
23
Primary outcome: Death, Reinfarction, Refractory Ischemia at 30 Days

24
Il beneficio del trasferimento immediato si è ottenuto
malgrado 1/3 dei pazienti del braccio di controllo sia stato trattato con la Rescue. Il rischio di sanguinamento non è stato differente nei due Gruppi (e comunque basso: solo 5 ICH nei 598 pz )
")
25
Community Hospital Emergency Department PCI Centre Cath Lab
‘High Risk’ ST Elevation MI within 12 hours of symptom onset Community Hospital Emergency Department TNK + ASA + Heparin / Enoxaparin + Clopidogrel “Pharmacoinvasive Strategy” Urgent Transfer to PCI Centre “Standard Treatment” Assess chest pain, ST resolution at minutes after randomization Failed Reperfusion* Successful Reperfusion PCI Centre Cath Lab Cath / PCI within 6 hrs regardless of reperfusion status Cath and Rescue PCI GP IIb/IIIa Inhibitor Elective Cath PCI > 24 hrs later Repatriation of stable patients within 24 hrs of PCI * ST segment resolution < 50% & persistent chest pain, or hemodynamic instability Randomization stratified by age (≤75 vs. > 75) and by enrolling site NEJM 2009
 and by enrolling site. NEJM")
26
Primary end-point: 30-day composite Death, Reinfarction, recurrent ischemia, CHF, Shock
Tecneplase a dose piena; pazienti a rischio più elevato II-III classe Killip ecc. (però se si va a controllare la casistica si vede che la classe Killip 1 rappresenta il 90%) Risultati buoni anche per l’insorgenza di scompenso: 3% vs 5.6% p=0.04
 Risultati buoni anche per l’insorgenza di scompenso: 3% vs 5.6% p=0.04.")
27
Conclusioni In paz con STEMI ad alto rischio sottoposti alla fibrinolisi in centri periferici, il trasferimento entro 6 ore al centro hub per eseguire la PCI si associa ad una riduzione significativa di eventi ischemici, (malgrado il ricorso in circa il 40% dei pazienti alla PCI rescue) senza incrementare gli eventi emorragici, La PCI precoce dopo trombolisi, si è dimostrata più “safe” che nei precedenti trials (progressi con gli stent ed altra terapia concomitante –Clopidogrel-?)
 senza incrementare gli eventi emorragici, La PCI precoce dopo trombolisi, si è dimostrata più safe che nei precedenti trials (progressi con gli stent ed altra terapia concomitante –Clopidogrel- )")
28
1.Se possibile pPCI 2.Se non possibile pPCI

29
2009

30
Anti IIB/IIIA pre-cathlab
Molti studi eseguiti prima della doppia antiaggregazione non più attuali. BRAVE-3 (Abciximab): clinicamente neutro; ON-TIME 2 (Tirofiban): clinicamente neutro. MULTISTRATEGY: Abciximab vs Tirofiban e BMS vs DES (Sirolimus) – vantaggio del DES. FINESSE: Braccio abciximab clinicamente neutro (con + emorragie rispetto alla somministrazione in emodinamica) Brave 3 (Abciximab) 600 mg di Plavix Photon computed Tomography: neutro e neutro anche per gli eventi clinici; On TIME 2 (Tirofiban) 600 mg di Plavix: positivo solo per la risoluzione di ST, neutro per gli end point clinici; Multistrategy Abciximab vs Tirofiban e BMS vs Sirolimus
: clinicamente neutro; ON-TIME 2 (Tirofiban): clinicamente neutro. MULTISTRATEGY: Abciximab vs Tirofiban e BMS vs DES (Sirolimus) – vantaggio del DES. FINESSE: Braccio abciximab clinicamente neutro (con + emorragie rispetto alla somministrazione in emodinamica) Brave 3 (Abciximab) 600 mg di Plavix Photon computed Tomography: neutro e neutro anche per gli eventi clinici; On TIME 2 (Tirofiban) 600 mg di Plavix: positivo solo per la risoluzione di ST, neutro per gli end point clinici; Multistrategy Abciximab vs Tirofiban e BMS vs Sirolimus.")
31
2009

32
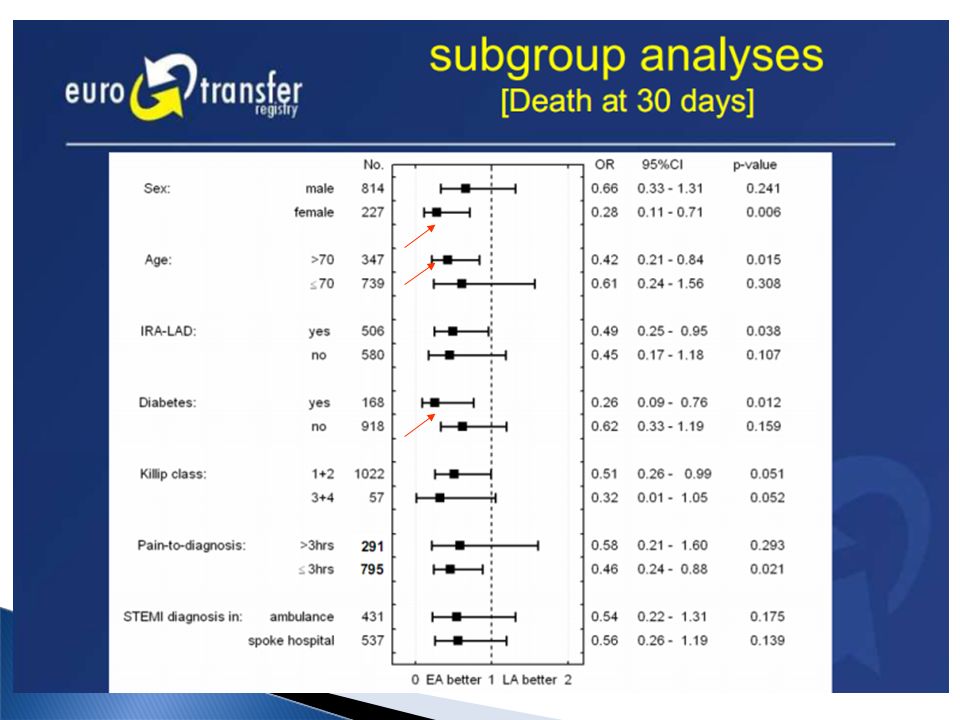
Come identificare, eventualmente, i pazienti della Classe 2B?
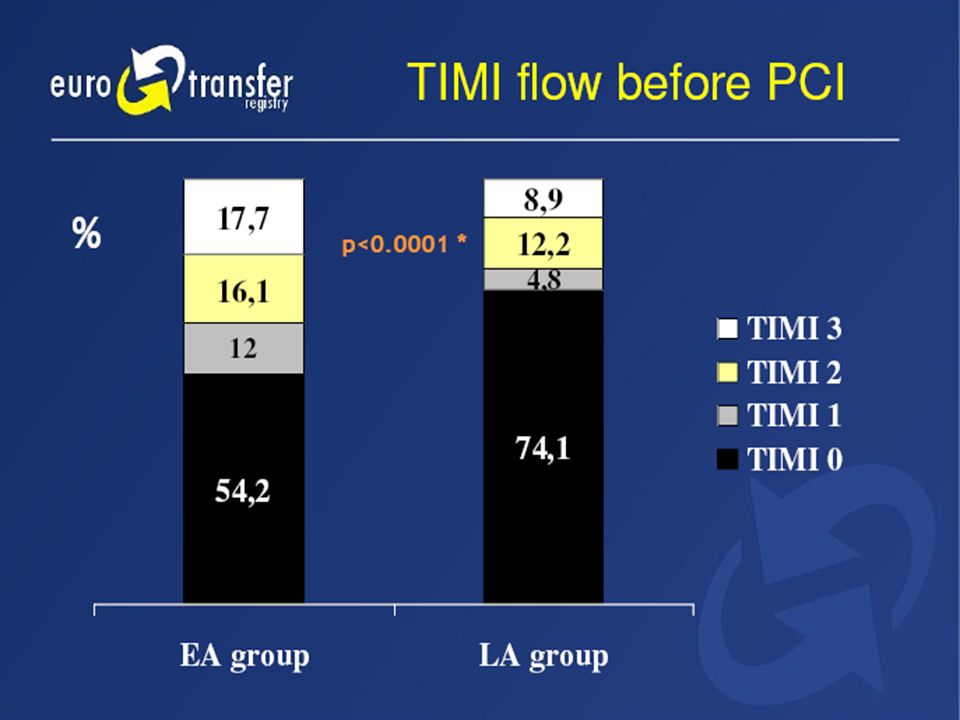
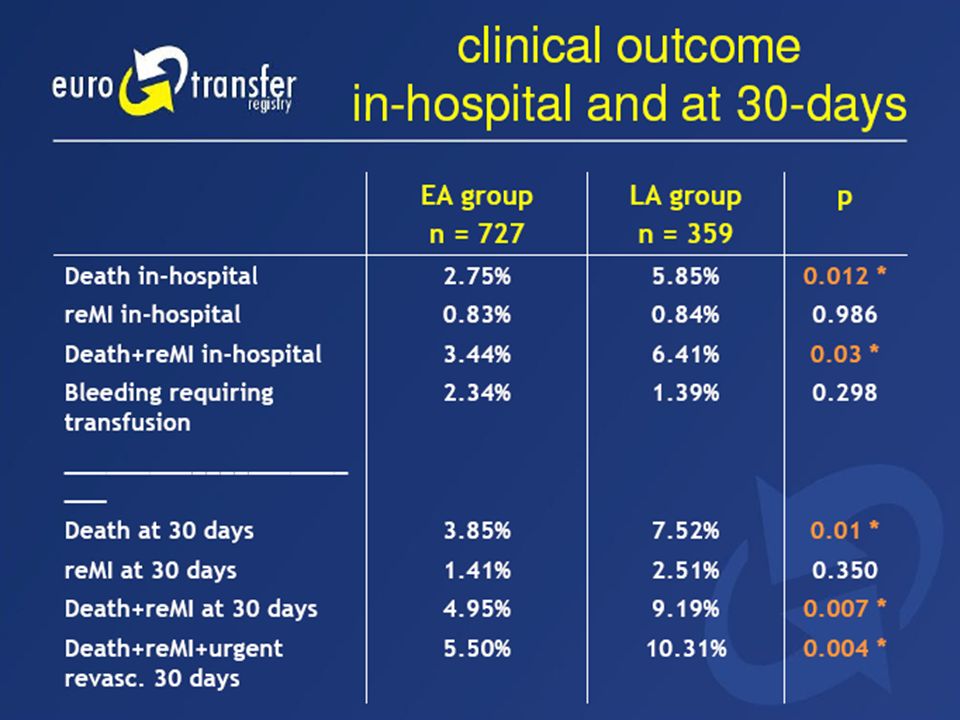
Probabilmente ad identificare quali pazienti in questo II B possono entrare. Attenzione: poco uso di Clopidogrel (20 e 25%) BACKGROUND: Abciximab is established as adjunct to primary percutaneous coronary intervention (PCI). Based on some smaller studies, ST-segment elevation myocardial infarction (STEMI) networks in various European countries have adopted the start of abciximab before transfer to the catheterization laboratory (cathlab) hospital as part of their routine treatment options. Although a recently published study did not reveal improved clinical outcome when starting abciximab before the cathlab, a potential benefit from such early administration, in particular in the setting of transfer networks, remains unclear and has been the subject of debate. METHODS: Data of consecutive patients with STEMI transferred for primary PCI in hospital/ambulance-feeded STEMI networks treated between November 2005 and January 2007 at 15 PCI centers from 7 European countries were collected in the web-based EUROTRANSFER Registry. RESULTS: Data from a total of 1,650 patients were collected. Abciximab was administered to 1086 patients (66%), of whom 727 received early abciximab (EA group: abciximab started before admission to cathlab, at least 30 minutes before balloon). Another 359 patients received late abciximab (LA group: periprocedural administration of abciximab in the cathlab). Preprocedural TIMI 3 flow was observed in 17.7% of patients with EA and in 8.9% in the LA group (P < .0001). Thirty-day mortality was 3.9% in the EA group versus 7.5% with LA (OR 0.49, 95% CI , P = .011), and composite 30-day outcome including death, repeated myocardial infarction, and urgent revascularization was present in 5.5% and 10.3%, respectively (OR 0.51, 95% CI , P = .004). These differences remain statistically significant in favor of early abciximab after accounting and adjustment for differences between the groups by means of a multivariate regression model and propensity score. CONCLUSIONS: Patients in STEMI networks transferred for primary PCI who have received abciximab before transfer rather than in the cathlab had more patent arteries before PCI and showed lower rates for death and the composite clinical outcome at 30-day follow-up. Am Heart J 2008
 BACKGROUND: Abciximab is established as adjunct to primary percutaneous coronary intervention (PCI). Based on some smaller studies, ST-segment elevation myocardial infarction (STEMI) networks in various European countries have adopted the start of abciximab before transfer to the catheterization laboratory (cathlab) hospital as part of their routine treatment options. Although a recently published study did not reveal improved clinical outcome when starting abciximab before the cathlab, a potential benefit from such early administration, in particular in the setting of transfer networks, remains unclear and has been the subject of debate. METHODS: Data of consecutive patients with STEMI transferred for primary PCI in hospital/ambulance-feeded STEMI networks treated between November 2005 and January 2007 at 15 PCI centers from 7 European countries were collected in the web-based EUROTRANSFER Registry. RESULTS: Data from a total of 1,650 patients were collected. Abciximab was administered to 1086 patients (66%), of whom 727 received early abciximab (EA group: abciximab started before admission to cathlab, at least 30 minutes before balloon). Another 359 patients received late abciximab (LA group: periprocedural administration of abciximab in the cathlab). Preprocedural TIMI 3 flow was observed in 17.7% of patients with EA and in 8.9% in the LA group (P < .0001). Thirty-day mortality was 3.9% in the EA group versus 7.5% with LA (OR 0.49, 95% CI , P = .011), and composite 30-day outcome including death, repeated myocardial infarction, and urgent revascularization was present in 5.5% and 10.3%, respectively (OR 0.51, 95% CI , P = .004). These differences remain statistically significant in favor of early abciximab after accounting and adjustment for differences between the groups by means of a multivariate regression model and propensity score. CONCLUSIONS: Patients in STEMI networks transferred for primary PCI who have received abciximab before transfer rather than in the cathlab had more patent arteries before PCI and showed lower rates for death and the composite clinical outcome at 30-day follow-up. Am Heart J")
36
Early abciximab administration before primary percutaneous coronary
intervention improves clinical outcome in elderly patients transferred with ST-elevation myocardial infarction: Data from the EUROTRANSFER registry 30-day death 30-day death + Reinfarction % % P = 0.001 P = 0.001 Nessuna differenza per emorragie nel gruppo >/= 65 aa Dziewiers et al: Int J Cardiol 2009

37
2009

38
ISIS-2 ISIS-2 (Second International Study of Infarct Survival) Collaborative Group, Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarctions: ISIS-2. Lancet ii -20%

39
Collaborative metaanalysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002; 324:71-86 NNT = 26

40
ACC/AHA Guidelines 2004 (invariate per l’ASA)
ESC Guidelines 2008

41
Biotransformation and Mode of Action
of Clopidogrel, Prasugrel, and Ticagrelor Schomig A. N Engl J Med 2009

42
CURE Primary end-point: CVD+MI+Stroke)
Il beneficio del Clopidogrel (300>75) è maggiore nei pazienti sottoposti a PCI CURE Primary end-point: CVD+MI+Stroke) Medical Rx Group Placebo Clopidogrel RR: 0.80 ( ) 0.20 4 0.15 0.10 0.05 0.0 100 200 300 0.20 4 0.15 0.10 0.05 0.0 100 200 300 PCI Group Placebo RR: 0.72 ( ) CVD/MI/Stroke CVD/MI/Stroke Clopidogrel -19% -30% NEJM 2001
 è maggiore nei pazienti sottoposti a PCI. CURE Primary end-point: CVD+MI+Stroke) Medical Rx Group. Placebo. Clopidogrel. RR: 0.80 ( ) PCI Group. Placebo. RR: 0.72 ( ) CVD/MI/Stroke. CVD/MI/Stroke. Clopidogrel. -19% -30% NEJM")
43
PCI- The CURE Investigators: Lancet 2001

44
Clarity TIMI 28 (Fibrinolisi) PCI- Clarity TIMI 28
-36% -46% NEJM 2005 JAMA 2005

45
Meta-Analysis of Clopidogrel Pretreatment
MI before PCI (%) Clopidogrel No Trial Pretreatment Pretreatment PCI-CURE CREDO n/a n/a PCI-CLARITY Overall Clopidogrel No PCI-CURE CREDO PCI-CLARITY Overall Favors Pretreatment Favors No Pretreatment OR 0.67 P=0.005 CVD or MI after PCI (%) 0.25 0.5 1.0 2.0 OR (95% CI) OR 0.71 P=0.004 0.25 0.5 1.0 2.0 Sabatine MS et al. JAMA 2005 OR (95% CI)
 Clopidogrel No. Trial Pretreatment Pretreatment. PCI-CURE CREDO n/a n/a. PCI-CLARITY Overall Clopidogrel No. PCI-CURE CREDO PCI-CLARITY Overall Favors. Pretreatment. Favors. No Pretreatment. OR P= CVD or MI after PCI (%) OR (95% CI) OR P= Sabatine MS et al. JAMA OR (95% CI)")
46
Angio 24,769 (99%) PCI 17,232 (70%) No PCI 7,855 (30%)
CURRENT OASIS: Study Design, Flow and Compliance 25,087 ACS Patients (UA/NSTEMI 70.8%, STEMI 29.2%) Planned Early (<24 h) Invasive Management with intended PCI Ischemic ECG Δ (80.8%) or ↑cardiac biomarker (42%) Randomized to receive (2 X 2 factorial): CLOPIDOGREL: Double-dose (600 mg then150 mg/d x 7d then 75 mg/d) vs Standard dose (300 mg then 75 mg/d) ASA: High Dose ( mg/d) vs Low dose ( mg/d) Angio 24,769 (99%) PCI 17,232 (70%) No PCI 7,855 (30%) No Sig. CAD 3,616 CABG 1,809 CAD 2,430 Efficacy Outcomes: CV Death, MI or stroke at day 30 Stent Thrombosis at day 30 Safety Outcomes: Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup: PCI v No PCI Complete Followup 99.8%
 Planned Early (<24 h) Invasive Management with intended PCI. Ischemic ECG Δ (80.8%) or ↑cardiac biomarker (42%) Randomized to receive (2 X 2 factorial): CLOPIDOGREL: Double-dose (600 mg then150 mg/d x 7d then 75 mg/d) vs Standard dose (300 mg then 75 mg/d) ASA: High Dose ( mg/d) vs Low dose ( mg/d) Angio 24,769. (99%) PCI 17,232. (70%) No PCI 7,855 (30%) No Sig. CAD 3,616. CABG 1,809. CAD 2,430. Efficacy Outcomes: CV Death, MI or stroke at day 30. Stent Thrombosis at day 30. Safety Outcomes: Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup: PCI v No PCI. Complete Followup 99.8%")
47
CURRENT OASIS: Double vs Standard Dose Primary Outcome (CV Death, MI or Stroke): PCI Patients
Clopidogrel Standard 15% RRR 0.04 Clopidogrel Double 0.03 Cumulative Hazard 0.02 HR 0.85 95% CI P=0.036 Sostanzialmente fallito l’End point principale 0.01 0.0 3 6 9 12 15 18 21 24 27 30 Days ESC 2009

48
CURRENT OASIS 7: Double vs Standard Dose Definite Stent Thrombosis (Angio confirmed)
Clopidogrel Standard Dose 0.012 42% RRR 0.008 Cumulative Hazard Clopidogrel Double Dose 0.004 Vantaggio per la restenosi HR 0.58 95% CI P=0.001 0.0 3 6 9 12 15 18 21 24 27 30 Days ESC 2009

49
Clopidogrel: Double v Standard Dose PCI Cohort Subgroups
CV Death, MI or Stroke MI or Stent Thrombosis 2N Std % Double % Intxn P Std % Double % Intxn P Overall 17232 4.5 3.9 3.7 3.0 NSTEMI/UA 10886 4.2 3.6 3.6 3.1 0.805 0.248 STEMI 6346 5.0 4.2 4.0 2.8 Male 13009 4.1 3.6 3.5 3.0 0.419 0.148 Female 4223 5.8 4.6 4.6 3.0 Age <= 65 yrs 10975 3.0 2.7 2.9 2.2 0.702 0.418 Age > 65 yrs 6257 7.1 6.0 5.2 4.4 Non-Diabetic 13400 4.2 3.6 3.6 2.8 0.836 0.567 Prev Diabetic 3831 5.6 4.9 4.1 3.6 No Inhosp GPIIb/IIIa 12288 3.9 3.5 3.1 2.5 0.465 0.894 GPIIb in hosp 4936 6.0 4.7 5.2 4.1 No Prot Pump Inhib 7675 3.8 3.2 3.1 2.3 0.408 0.613 Prot Pump Inhib 5557 5.7 4.2 4.8 3.3 Non-smoker 10845 4.9 4.6 3.9 3.5 0.045 0.050 Current Smoker 6380 3.8 2.6 3.4 2.1 ASA Low 8620 4.2 4.3 3.6 3.2 0.024 0.191 ASA High 8612 4.8 3.5 3.8 2.7 Double Dose Better Double Dose Better 0.50 1.50 0.50 1.50

50
Clopidogrel Double vs Standard Dose Bleeding Overall Population
Hazard Ratio 95% CI P TIMI Major 0.95 1.04 1.09 0.50 CURRENT Major 2.0 2.5 1.25 0.01 CURRENT Severe 1.5 1.9 1.23 0.03 Fatal 0.11 0.13 1.15 0.71 ICH 0.05 0.67 0.53 RBC transfusion ≥ 2U 1.76 2.21 1.26 CABG-related Major 0.9 1.0 1.10 0.48

51
TRITON TIMI 38: Study Design
ACS: STEMI (35%) or UA/NSTEMI) & Planned PCI ASA N= 13,608 Double-blind CLOPIDOGREL 300 mg LD/ 75 mg MD PRASUGREL 60 mg LD/ 10 mg MD Median duration of therapy - 12 months 1o endpoint: CV death, MI, Stroke 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleeds Key Substudies: Pharmacokinetic, Genomic NEJM 2007 NEJM: 2009
 or UA/NSTEMI) & Planned PCI. ASA. N= 13,608. Double-blind. CLOPIDOGREL. 300 mg LD/ 75 mg MD. PRASUGREL. 60 mg LD/ 10 mg MD. Median duration of therapy - 12 months. 1o endpoint: CV death, MI, Stroke. 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleeds Key Substudies: Pharmacokinetic, Genomic. NEJM NEJM:")
52
TRITON TIMI 38 Primary Endpoint: CV Death, MI, Stroke
15 Clopidogrel 12.1 (781) 9.9 (643) 10 Primary Endpoint (%) Prasugrel HR 0.81 ( ) P=0.0004 HR 0.80 P=0.0003 HR 0.77 P=0.0001 5 NNT= 46 Days 30 60 90 180 270 360 450 NEJM 2007 Days NEJM: 2009
 9.9 (643) 10. Primary Endpoint (%) Prasugrel. HR 0.81 ( ) P= HR 0.80 P= HR 0.77 P= NNT= 46. Days NEJM Days. NEJM:")
53
TRITON TIMI 38: Stent Thrombosis (Definite + Probable)
Any Stent at Index PCI N= 12,844 2.4 (142) Clopidogrel 2 Endpoint (%) 1.1 (68) 1 Prasugrel HR 0.48 P <0.0001 NNT= 77 30 60 90 180 270 360 450 Days NEJM 2007
 Clopidogrel. 2. Endpoint (%) 1.1 (68) 1. Prasugrel. HR 0.48 P < NNT= Days. NEJM")
54
TRITON TIMI 38: CV Death, MI, Stroke Major Subgroups
Reduction in risk (%) 18 UA/NSTEMI B 21 STEMI Male 21 Female 12 <65 25 Age 65-74 14 >75 6 No DM 14 DM 30 BMS 20 DES 18 GPI 21 No GPI 16 14 CrCl < 60 20 CrCl > 60 19 Pinter = NS OVERALL 0.5 1 2 Prasugrel Better Clopidogrel Better HR NEJM 2007
 18. UA/NSTEMI. B. 21. STEMI. Male. 21. Female. 12. < Age > No DM. 14. DM. 30. BMS. 20. DES. 18. GPI. 21. No GPI CrCl < CrCl > Pinter = NS. OVERALL Prasugrel Better. Clopidogrel Better. HR. NEJM")
55
TRITON TIMI 38 (STEMI: 3534 pt)
CVD + nf MI + nf Stroke CVD +nf MI + Urg target v revas. Stent thrombosis TIMI Major bleeding Lancet 2009

56
TRITON TIMI 38: Bleeding Events ICH in Pts w Prior Stroke/TIA (N=518)
Clopidogrel Prasugrel Clop 0 (0) % Pras 6 (2.3)% (P=0.02) % Events P=0.01 P=0.002 P=0.74 P=0.03 P=0.23 NEJM 2007 NEJM: 2007
 % Pras 6 (2.3)% (P=0.02) % Events. P=0.01. P= P=0.74. P=0.03. P=0.23. NEJM NEJM:")
57
PLATO study design NSTE-ACS (mod-to-high risk) STEMI 37% (if primary PCI) Clopidogrel-treated or -naive; randomised within 24 hours of index event (N=18,624) Clopidogrel If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor 180 mg loading dose, then 90 mg bid maintenance; (additional 90 mg pre-PCI) 6–12-month exposure Primary endpoint: CV death + MI + Stroke Primary safety endpint: Total major bleeding NEJM: 2009 NEJM: 2009
 Clopidogrel. If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor. 180 mg loading dose, then. 90 mg bid maintenance; (additional 90 mg pre-PCI) 6–12-month exposure. Primary endpoint: CV death + MI + Stroke. Primary safety endpint: Total major bleeding. NEJM: NEJM:")
58
PLATO: Risultati end-point primario (CVD+MI+Stroke)
8 8 6.60 Clopidogrel 6 6 Clopidogrel 5.43 5.28 4.77 Cumulative incidence (%) 4 Cumulative incidence (%) 4 Ticagrelor Ticagrelor 2 2 HR 0.88 (95% CI 0.77–1.00), p=0.045 HR 0.80 (95% CI 0.70–0.91), p<0.001 10 20 30 31 90 150 210 270 330 Days after randomisation Days after randomisation* No. at risk Ticagrelor 9,333 8,942 8,827 8,763 8,673 8,543 8,397 7,028 6,480 4,822 Clopidogrel 9,291 8,875 8,763 8,688 8,688 8,437 8,286 6,945 6,379 4,751 *Excludes patients with any primary event during the first 30 days NEJM: 2009 Wallentin L et al. N Engl J Med 2009;
 4. Cumulative incidence (%) 4. Ticagrelor. Ticagrelor HR 0.88 (95% CI 0.77–1.00), p= HR 0.80 (95% CI 0.70–0.91), p< Days after randomisation. Days after randomisation* No. at risk. Ticagrelor. 9,333. 8,942. 8,827. 8,763. 8,673. 8,543. 8,397. 7,028. 6,480. 4,822. Clopidogrel. 9,291. 8,875. 8,763. 8,688. 8,688. 8,437. 8,286. 6,945. 6,379. 4,751. *Excludes patients with any primary event during the first 30 days. NEJM: Wallentin L et al. N Engl J Med 2009;")
59
K-M estimated rate (% per year)
PLATO: Time to major bleeding – primary safety event 15 Ticagrelor 11.58 11.20 10 Clopidogrel K-M estimated rate (% per year) 5 HR 1.04 (95% CI 0.95–1.13), p=0.434 60 120 180 240 300 360 Ticagrelor 9,235 7,246 6,826 6,545 5,129 3,783 3,433 Clopidogrel 9,186 7,305 6,930 6,670 5,209 3,841 3,479 NEJM: 2009
 5. HR 1.04 (95% CI 0.95–1.13), p= Ticagrelor. 9,235. 7,246. 6,826. 6,545. 5,129. 3,783. 3,433. Clopidogrel. 9,186. 7,305. 6,930. 6,670. 5,209. 3,841. 3,479. NEJM:")
60
18,758 patients enrolled in PLATO
PLATO-STEMI 18,758 patients enrolled in PLATO 134 patients not randomized 18,624 patients randomized NSTEMI/UA/other: 10,194 patients STEMI: 8,430 patients Randomized to ticagrelor: efficacy population N= 4,201 Randomized to clopidogrel: efficacy population N= 4,229 No intake of study medication: 36 patients No intake of study medication: 48 patients Safety population N=4,165 Safety population N=4,181

61
PLATO-STEMI Primary endpoint: CV death, MI or stroke
12 11 10 9 8 7 6 5 4 3 2 1 Clopidogrel 11.0 9.3 Ticagrelor K-M estimated rate (% per year) HR: 0.85 (95% CI = 0.74–0.97), p=0.02 Months Steg PG: ESC 2009
 HR: 0.85 (95% CI = 0.74–0.97), p= Months. Steg PG: ESC")
62
PLATO: Stent thrombosis
PLATO-STEMI : Stent thrombosis NEJM: 2009 Steg PG: ESC 2009

63
K-M estimated rate (% per year)
PLATO-STEMI Primary safety event: major bleeding 10 8 6 4 2 Clopidogrel 9.3 9.0 Ticagrelor K-M estimated rate (% per year) HR 0.96 (95% CI = 0.83–1.12), p=0.63 Months Steg PG: ESC 2009
 HR 0.96 (95% CI = 0.83–1.12), p= Months. Steg PG: ESC")
64
PCI Recommendations – Class I
(Classe I – Evidenza C) 2008
")
65
Ancillary Therapy to Reperfusion (2004)
Unfractionated heparin (UFH) should be given intravenously in: Patients undergoing PCI or surgical revascularization After alteplase, reteplase, tenecteplase After streptokinase, anistreplase, urokinase in patients at high risk for systemic emboli.
 should be given. intravenously in: Patients undergoing PCI or surgical revascularization. After alteplase, reteplase, tenecteplase. After streptokinase, anistreplase, urokinase in patients at high risk for systemic emboli.")
67
Considerazioni finali (1)
La PTCA va considerata sempre e comunque un trattamento “Farmaco-invasivo” Forse è meglio abbandonare i termini “Facilitata” e “Rescue” perché “potentially misleading labels”: “as-soon-as-possible” o “timely” dovrebbero diventare il nuovo parametro di riferimento. La trombolisi rimane una buona scelta nei pazienti che si presentano presto con un tempo D2B lungo, con valutazione angiografica “as-soon-as-possible” Il calcolo del rischio emorragico deve assumere la stessa rilevanza del calcolo del rischio ischemico

68
Considerazioni finali (2)
Le Linee Guida forniscono elementi utilissimi per la preparazione corretta e l’invio alla PTCA, ma… …l’implementazione delle stesse va coniugata sempre con… Condizioni logistiche Fruibilità di risorse adeguate (SUEM 118, Emodinamica H24 ecc) Condizioni del paziente (classe Killip), insorgenza e durata dei sintomi, sede dell’infarto, età, rischio emorragico, comorbilità.
 Condizioni del paziente (classe Killip), insorgenza e durata dei sintomi, sede dell’infarto, età, rischio emorragico, comorbilità.")
69
Ospedale Giovanni Paolo II – Lamezia Terme
U. O. CARDIOLOGIA con UTIC Ospedale Giovanni Paolo II – Lamezia Terme GRAZIE

Presentazioni simili












 17 Ottobre 2009 DOPPIA ANTIAGGREGAZIONE PIASTRINICA.>")







