Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Corso di “Farmacologia”
Facoltà di Scienze Motorie Università degli Studi di Verona Corso di “Farmacologia” Lezione 19: Amfetamine e altri stimolanti Docenti: Guido Fumagalli e Roberto Leone

2
Gli stimolanti del SNC

4
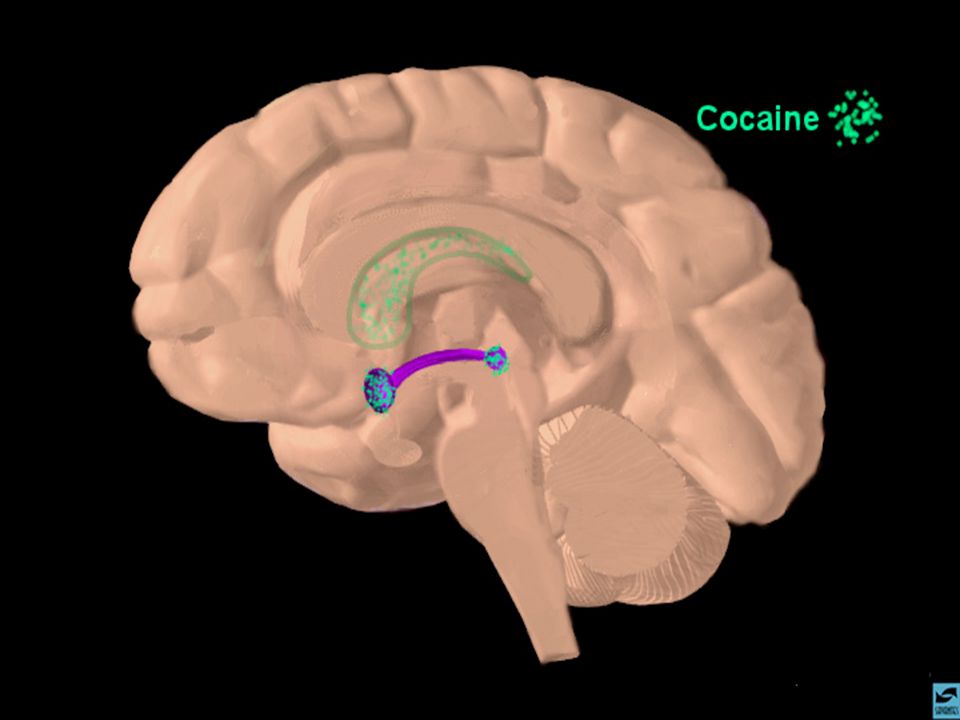
Slide 2: Brain regions and neuronal pathways
Certain parts of the brain govern specific functions. Point to sensory, motor, association and visual cortex to highlight specific functions. Point to the cerebellum for coordination and to the hippocampus for memory. Indicate that nerve cells or neurons travel from one area to another via pathways to send and integrate information. Show, for example, the reward pathway. Start at the ventral tegmental area (VTA) (in magenta), follow the neuron to the nucleus accumbens, and then on to prefrontal cortex. Explain that this pathway gets activated when a person receives positive reinforcement for certain behaviors ("reward"). Indicate that you will explain how this happens when a person takes an addictive drug.
 (in magenta), follow the neuron to the nucleus accumbens, and then on to prefrontal cortex. Explain that this pathway gets activated when a person receives positive reinforcement for certain behaviors ( reward ). Indicate that you will explain how this happens when a person takes an addictive drug.")
5
La via del “piacere” Gli stimolanti (es. cocaina, oppioidi, amfetamine,cannabinoidi) alterano le aree cerebrali che mediano le sensazioni di motivazione e di piacere
 alterano le aree cerebrali che mediano le sensazioni di motivazione e di piacere.")
7
Eroina

8
Marijuana

10
I neurotrasmettitori I neurotrasmettitori sono sostanze chimiche rilasciate dalle cellule nervose per “comunicare” tra loro

11
Slide 6: Dopamine and the production of cyclic AMP
Using the close-up view, explain what happens when dopamine binds to its receptor. When dopamine binds to its receptor, another protein called a G-protein (in pink) moves up close to the dopamine receptor. The G-protein signals an enzyme to produce cyclic adenosine monophosphate (cAMP) molecules (in green) inside the cell. [Sometimes the signal can decrease production of cAMP, depending on the kind of dopamine receptor and G-protein present.] Point to the dopamine receptor-G-protein/adenylate cyclase complex, and show how cAMP is generated when dopamine binds to its receptor. Indicate that cAMP (point to the cyclic-looking structures) controls many important functions in the cell including the ability of the cell to generate electrical impulses.
 moves up close to the dopamine receptor. The G-protein signals an enzyme to produce cyclic adenosine monophosphate (cAMP) molecules (in green) inside the cell. [Sometimes the signal can decrease production of cAMP, depending on the kind of dopamine receptor and G-protein present.] Point to the dopamine receptor-G-protein/adenylate cyclase complex, and show how cAMP is generated when dopamine binds to its receptor. Indicate that cAMP (point to the cyclic-looking structures) controls many important functions in the cell including the ability of the cell to generate electrical impulses.")
12
La dopamina Alcool, amfetamine, cocaina, eroina, marijuana e nicotina (così come il sesso e la cioccolata), direttamente o indirettamente, aumentano i livelli di dopamina nelle sinapsi della “via del piacere”
, direttamente o indirettamente, aumentano i livelli di dopamina nelle sinapsi della via del piacere")
13
Meccanismo comune agli stimolanti: liberazione di dopamina

14
Meccanismo comune agli stimolanti: liberazione di dopamina

15
Meccanismo comune agli stimolanti: liberazione di dopamina

16
Meccanismo comune agli stimolanti: liberazione di dopamina

17
Sostanze la cui assunzione è proibita in occasione delle competizioni
S6. Stimolanti Adrenalina^, amfetamina, catina*, cocaina, efedrina**, metilefedrina**, metilfenidato, modafinil, pemolina, selegilina, sibutramina, stricnina, ecc., e altre sostanze con struttura chimica o effetto farmacologico similare ^associata ad agenti anestetici o per via topica non è proibita *concentrazioni urinarie >5mcg/ml **concentrazioni urinarie >10mcg/ml) S7. Narcotici Buprenorfina, destromoramide, eroina, fentanile e derivati, idromorfone, metadone, morfina, ossicodone, ossimorfone, pentazocina, petidina S8. Cannabinoidi (es. hashish e marijuana) S9. Glucocorticosteroidi Proibiti per via orale, rettale, e.v. o i.m. a meno di esenzione terapeutica. Per altre vie (es. inalatoria, intra-articolare, ecc.) esenzione terapeutica abbreviata. Preparazioni topiche (dermatologiche, oftalmiche, ecc.) non proibite
 S7. Narcotici Buprenorfina, destromoramide, eroina, fentanile e derivati, idromorfone, metadone, morfina, ossicodone, ossimorfone, pentazocina, petidina. S8. Cannabinoidi (es. hashish e marijuana) S9. Glucocorticosteroidi Proibiti per via orale, rettale, e.v. o i.m. a meno di esenzione terapeutica. Per altre vie (es. inalatoria, intra-articolare, ecc.) esenzione terapeutica abbreviata. Preparazioni topiche (dermatologiche, oftalmiche, ecc.) non proibite.")
18
Stimolanti del SNC Cocaina
Derivata dalla pianta Erythroxylon coca è un potente stimolante del SNC, agisce inibendo il reuptake della dopamina a livello delle sinapsi. Provoca euforia, fiducia in se stessi, potenza sessuale, non fa sentire la fatica, mantiene sveglie aumenta l’attenzione. Provoca aritmie cardiache, infarto del miocardio, ipertensione o ipotensione, ansia, depressione, attacchi di panico, aggressività, irritabilità, psicosi tossiche, tremori, convulsioni, alterazione dei riflessi, mancata coordinazione motoria, paralisi muscolare, respirazione irregolare dipendenza, morte

19
LA DIPENDENZA DA COCAINA
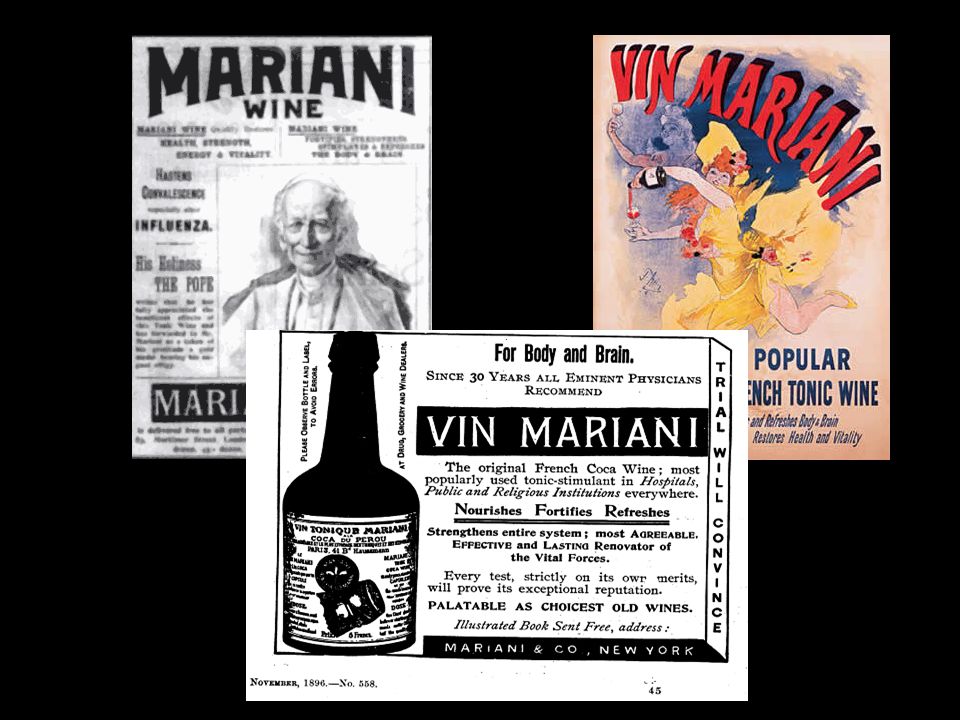
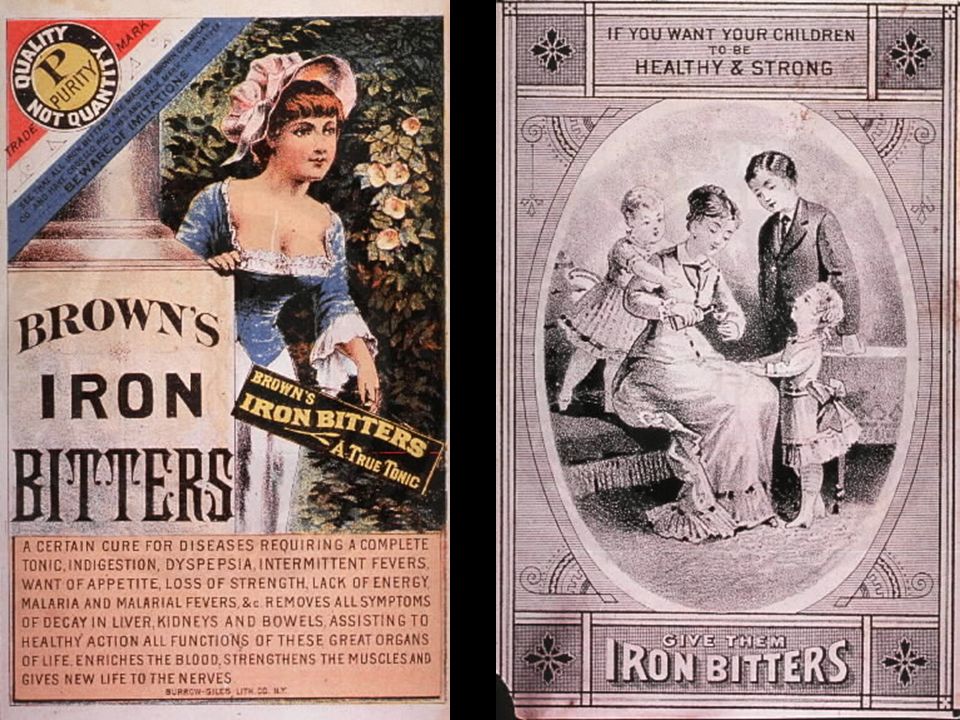
Come l’oppio anche la cocaina ha un’origine antichissima. E’ stata riscontrata, insieme alla nicotina, in mummie egiziane risalenti a più di 3000 anni fa. Quantità misurabili di cocaina sono state altresì rinvenute in antiche tombe peruviane e mummie cilene del 2000 a.C. Inoltre, la scoperta di un incisione raffigurante una testa umana nel tipico atteggiamento dei masticatori del bolo di coca e di vasi e statue riproducenti soggetti nell’atto di preparare le “dosi”, fanno risalire a prima del 3000 a.C. la tossicodipendenza da cocaina. Ricordiamo il Vin Mariani utilizzato da Edison, Stevenson, Dumas, Verne, Sarah Bernhardt, Eleonora Duse e perfino il papa Leone XIII. Altra bevanda del tempo era la French Wine Cola prodotta da Pemberton da cui derivò la Coca-Cola.. Ma l’anno decisivo per la diffusione della cocaina fu il 1884 quando Freud pubblicò il libro “Uber Coca”.. Uno dei più noti consumatori di cocaina fu Conan Doyle, l’autore di Sherlock Holmes (anche lui descritto da Doyle come consumatore di cocaina). In Europa si diffuse ampiamente nel XIX secolo e vi erano in commercio numerose bevande a base di cocaina, quali il Vin Mariani o la French Coca Wine. Anno decisivo per la diffusione della cocaina fu il 1884 quando Freud pubblicò il libro “Uber Coca”.
. In Europa si diffuse ampiamente nel XIX secolo e vi erano in commercio numerose bevande a base di cocaina, quali il Vin Mariani o la French Coca Wine. Anno decisivo per la diffusione della cocaina fu il 1884 quando Freud pubblicò il libro Uber Coca .")
22
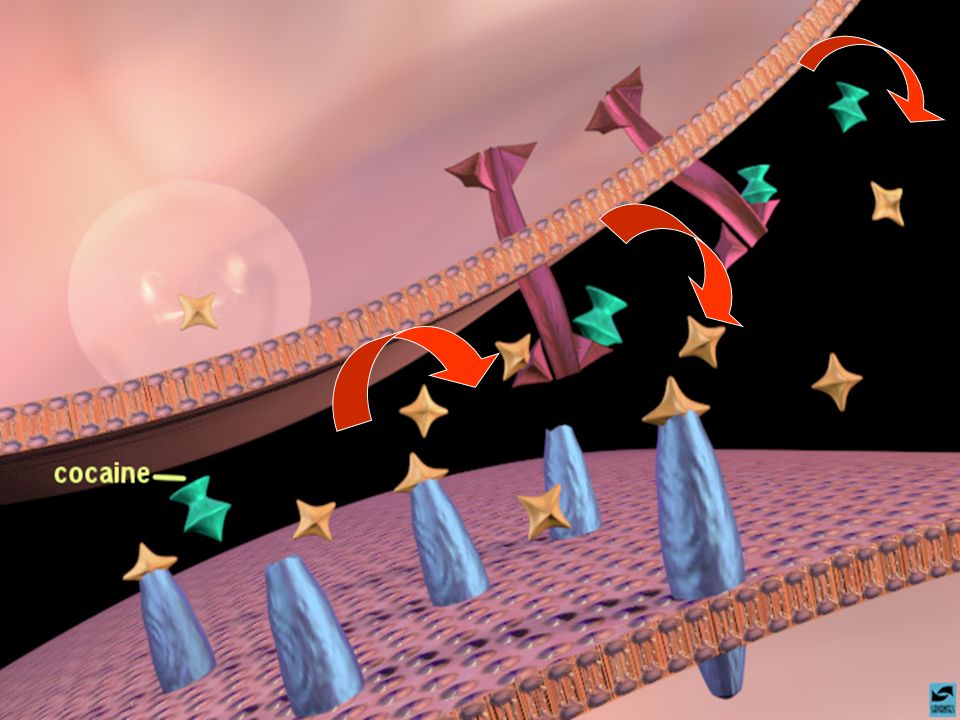
Slide 12: Dopamine binding to receptors and uptake pumps in the nucleus accumbens
Explain that cocaine concentrates in areas of the brain that are rich in dopamine synapses. Review dopamine transmission in the nucleus accumbens. Point to dopamine in the synapse and to dopamine bound to dopamine receptors and to uptake pumps on the terminal.

24
Durante la droga: cocaina
1-2 Min 3-4 5-6 6-7 7-8 8-9 9-10 10-20 20-30 Slide 7: This is literally the brain on drugs. When someone gets “high” on cocaine, where does the cocaine go in the brain? With the help of a radioactive tracer, this PET scan shows us a person’s brain on cocaine and the area of the brain, highlighted in yellow, where cocaine is “binding” or attaching itself. This PET scan shows us minute by minute, in a time-lapsed sequence, just how quickly cocaine begins affecting a particular area of the brain. We start in the upper left hand corner. You can see that 1 minute after cocaine is administered to this subject nothing much happens. All areas of the brain seem to be functioning normally. But after 3 to 4 minutes [the next scan to the rightl, we see areas highlighted in yellow where cocaine is starting to bind to the striatum [stry-a-tum] of the brain and activate it. At the 5- to 8-minute interval, we see that cocaine is affecting a large area of the brain. After that, the drug’s effects begin to wear off. At the 9- to 10-minute point, the high feeling is almost gone. Unless the abuser takes more cocaine, the experience is over in about 20 to 30 minutes. Scientists are doing research to find out if the striatum produces the “high feeling”and controls our feelings of pleasure and motivation. One of the reasons scientists are curious about specific areas of the brain affected by drugs such as cocaine is to develop treatments for people who become addicted to these drugs. Scientists hope to find the most effective way to change an addicted brain back to normal functioning. Photo courtesy of Nora Volkow, Ph.D. Mapping cocaine binding sites in human and baboon brain in vivo. Fowler JS, Volkow ND, Wolf AP, Dewey SL, Schlyer DJ, Macgregor RIR, Hitzemann R, Logan J, Bendreim B, Gatley ST. et al. Synapse 1989;4(4):
:")
25
Modificazioni nell’attività cerebrale dopo cocaina
Slide 8: Long-term effects of drug abuse. This PET scan shows us that once addicted to a drug like cocaine, the brain is affected for a long, long time. In other words, once addicted, the brain is literally changed. Let’s see how... In this slide, the level of brain function is indicated in yellow. The top row shows a normal-functioning brain without drugs. You can see a lot of brain activity. In other words, there is a lot of yellow color. The middle row shows a cocaine addict’s brain after 10 days without any cocaine use at all. What is happening here? [Pause for response.] Less yellow means less normal activity occurring in the brain—even after the cocaine abuser has abstained from the drug for 10 days. The third row shows the same addict’s brain after 100 days without any cocaine. We can see a little more yellow, so there is some improvement— more brain activity—at this point. But the addict’s brain is still not back to a normal level of functioning. . . more than 3 months later. Scientists are concerned that there may be areas in the brain that never fully recover from drug abuse and addiction. Photo courtesy of Nora Volkow, Ph.D. Volkow ND, Hitzemann R, Wang C-I, Fowler IS, Wolf AP, Dewey SL. Long-term frontal brain metabolic changes in cocaine abusers. Synapse 11: , 1992; Volkow ND, Fowler JS, Wang G-J, Hitzemann R, Logan J, Schlyer D, Dewey 5, Wolf AP. Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse 14: , 1993.

26
Mortalità da cocaina: meccanismi

27
Stimolanti del SNC Amfetamine
La prima amfetamina è stata sintetizzata nel Consentono un rendimento più elevato e allontanano la soglia della stanchezza. Aumentano la temperatura corporea, il battito cardiaco e la pressione sanguigna. Danno euforia, stimolando alcune aree del cervello, aumentano l’aggressività, la concentrazione e l’attenzione. Diminuiscono l’appetito. Vengono utilizzate dagli atleti poco prima della competizione (gli effetti ricercati si evidenziano a breve termine e non con uso cronico) Sono probabilmente le sostanze che hanno provocato più morti nella storia del doping a causa delle gravi reazioni avverse (vedi oltre) Efedrina, pseudoefredina, fenilpropanolamina Farmaci utilizzati nel raffreddore (ma anche illegalmente come anoressizanti) hanno effetti simili alle amfetamine (anche come reazioni avverse) quando impiegati a dosaggi elevati
 Sono probabilmente le sostanze che hanno provocato più morti nella storia del doping a causa delle gravi reazioni avverse (vedi oltre) Efedrina, pseudoefredina, fenilpropanolamina. Farmaci utilizzati nel raffreddore (ma anche illegalmente come anoressizanti) hanno effetti simili alle amfetamine (anche come reazioni avverse) quando impiegati a dosaggi elevati.")
28
Reazioni avverse da amfetamine
Anoressia Cefalea Impazienza Insonnia Irritabilità Movimenti inc. Nausea Palpitazioni Tremori Vertigini Vomito Allucinazioni Aggressività Angina pectoris Collasso circolatorio Confusione Convulsioni Delirio Emorragia cerebrale Infarto del miocardio Ipertensione arteriosa Paranoia Dipendenza Disturbi comportamentali Delirio paranoide Discinesia Neuropatie Perdita di peso Psicosi Effetti acuti o a rapida insorgenza Effetti da uso cronico Moder. gravi Gravi

29
EFEDRINA AMFETAMINA Struttura chimica dell’efedrina (principale principio attivo dell’efedra) a confronto con quella dell’amfetamina
 a confronto con quella dell’amfetamina.")
30
Ma Huang (Efedra) Effetti vantati che spingono all’uso
Aumenta l’energia Stimola la perdita di peso Stimola la libido Aiuta il respiro nell’influenza e l’asma Migliora la concentrazione

31
Efedra 17 Febbraio 2003: morte del pitcher Steve Bechler dei Baltimore Orioles L’esame autoptico determino che l’efedra ebbe un ruolo nella sua morte Efedra Contiene sostanze stimolanti quali Efedrina e Pseudoefedrina Provocano vaso costrizione dei vasi sanguigni Benefici Studi non conclusivi: sopprime appettito e forse aiutare nella perdita di peso nel breve periodo Rischi Aumento pressione arteriosa Morti in genere a causa degli eventi cardiaci In particolare nei soggetti con fattori predisponenti Vietata dalla WADA Steve Bechler

32
Reazioni avverse dell’efedra
Dal 1993 al 1997 oltre 800 report di reazioni avverse, incluse 36 morti Cardiovascolari aritmie arresto cardiaco tachicardia GI nausea e vomito stipsi Altre reazioni cutanee alterazioni test epatici Sistema Nervoso psicosi pensieri suicidari convulsioni e tremori disturbi vestibolari insonnia nervosismo

33
Alcuni soggetti sono a maggior rischio
Soggetti con diabete, ipertensione, malattie tiroidee e cardiovascolari devono assolutamente evitare sostanze contenenti efedrina FDA ha riportato diverse morti di persone che hanno abusato di efedra Assumere efedra insieme a specialità medicinali contenenti pseudoefedrina (preparazioni per il raffreddore), efedrina, caffeina o altri stimolanti il SNC aumenta ulteriormente i rischi per la salute
, efedrina, caffeina o altri stimolanti il SNC aumenta ulteriormente i rischi per la salute.")
34
Modificazioni nell’attività cerebrale dopo amfetamine
Slide 9: Drugs have long-term consequences. Here is another example of what science has shown us about the long-term effects of drugs. What this PET scan shows us is how just 10 days of drug use can produce very dramatic and long-term changes in the brain of a monkey. The drug in these images is amphetamine, or what some people call “speed.” Remember the previous slide showed us what the brain of a chronic cocaine abuser looks like. This slide shows us what using a drug like amphetamine can do in only 10 days to the brain of a monkey. This slide also gives us a better idea of what methamphetamine, a drug similar in structure, can do to the brain. Methamphetamine use is becoming increasingly popular in certain areas of the country. The top row shows us, in white and red, normal brain activity. The second row shows us that same brain 4 weeks after being given amphetamine for 10 days. There is a dramatic decrease in brain activity. This decreased brain activity continues for up to 1 year after amphetamine use. These continuous brain changes often trigger other changes in social and emotional behavior, too, including a possible increase in aggressiveness, feelings of isolation, and depression. Photo courtesy of NIDA from research conducted by Melega WP, Raleigh MJ, Stout DB, Lacan C, Huang SC, Phelps ME. Recovery of striatal dopamine function after acute amphetamine- and methamphetamineinduced neurotoxicity in the vervet monkey. Brain Res 1997 Aug 22;766(1-2);
;")
35
Ecstasy È il nome dato ad una sostanza amfetaminica allucinogena chiamata MDMA (3,4 metilendiossime-tamfetamina) Scoperta nel 1912 in Germania dai ricercatori della Merck, è stata brevettata nel 1914 come anoressizzante. La sua sintesi richiede minime conoscenze di chimica, pertanto può essere facilmente prodotta in laboratori clandestini (basso prezzo) Nel nostro paese, l'MDMA ha fatto la sua comparsa agli inizi degli anni novanta, diffondendosi molto rapidamente presso i rave party e le discoteche. Si possono trovare tipi diversi di pasticche, con diversi colori e disegni stampati in rilievo da cui prendono il nome. Si chiamano Fish, Californiane, Offman, Colombelle, Bianchine, Playboy, Butterfly
 Nel nostro paese, l MDMA ha fatto la sua comparsa agli inizi degli anni novanta, diffondendosi molto rapidamente presso i rave party e le discoteche. Si possono trovare tipi diversi di pasticche, con diversi colori e disegni stampati in rilievo da cui prendono il nome. Si chiamano Fish, Californiane, Offman, Colombelle, Bianchine, Playboy, Butterfly.")
36
Ecstasy In Europa dopo la cannabis è la droga più popolare tra i giovani dai 14 ai 25 anni Ne esistono più di 200 “tipi” diversi mischiati ad altri farmaci o ad altre sostanze (eroina, steroidi, cocaina, amfetamina, veleno per topi, fibra di vetro, vermifughi, anestetici, insetticidi, pesticidi ecc.). Molte di queste sostanze sono pericolose per l’uomo! L’Olanda è uno dei principali produttori. Gia nel 1994 fu sequestrato un laboratorio che produceva oltre dodici milioni di pastiglie ogni giorno. Esistono laboratori mobili su container o camper. E’ normale trovare laboratori in grado di produrre più di centomila pastiglie ogni ora
. Molte di queste sostanze sono pericolose per l’uomo! L’Olanda è uno dei principali produttori. Gia nel 1994 fu sequestrato un laboratorio che produceva oltre dodici milioni di pastiglie ogni giorno. Esistono laboratori mobili su container o camper. E’ normale trovare laboratori in grado di produrre più di centomila pastiglie ogni ora.")
37
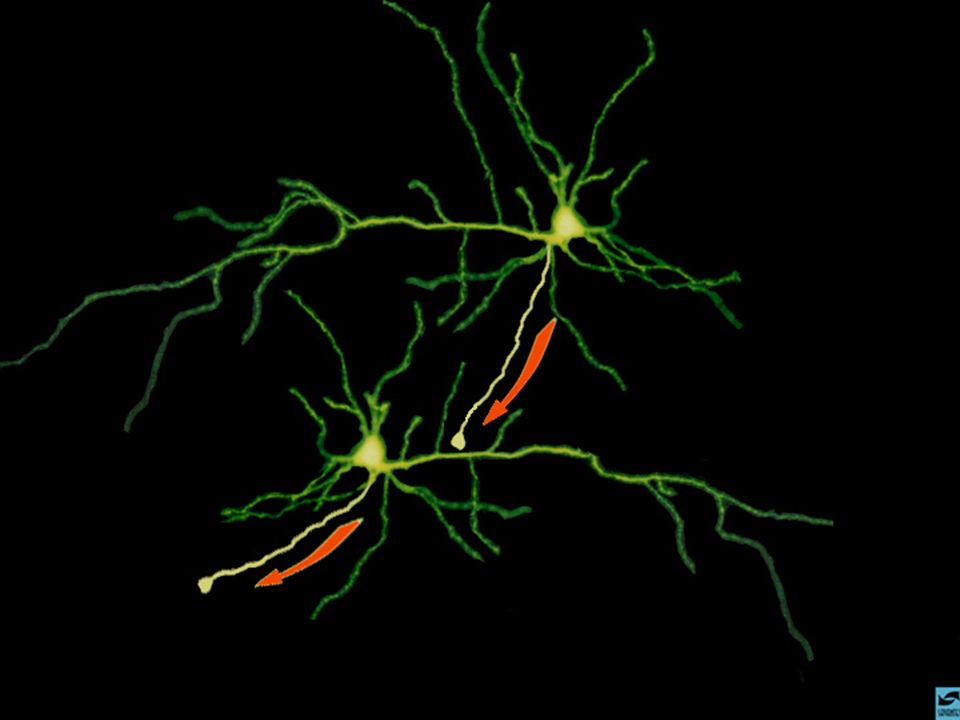
Slide 9: The Serotonin Neuron; The Major Target of Ecstasy
In order to help students understand how Ecstasy affects the function of serotonin neurons, it will be useful to review how neurotransmission takes place in a little more detail. You can explain serotonin neurotransmission as an example (serotonin is one of many neurotransmitters). This slide shows the connection between two neurons (the “synapse”). Serotonin is stored in small vesicles within the nerve terminal of a neuron. Electrical impulses (arising in the Raphe nucleus, for example) traveling down the axon toward the terminal cause the release of serotonin from small vesicles into the synaptic space. Point to the space between the terminal and the neighboring neuron. Once in the synaptic space, the serotonin binds to special proteins, called receptors, on the membrane of a neighboring neuron (this is usually at a dendrite or cell body). When serotonin binds to serotonin receptors (there are actually at least 14 types of serotonin receptors), it causes a change in the electrical properties of the receiving neuron that generally results in a decrease in its firing rate. Go to the next slide to explain how the action of serotonin is terminated.
. This slide shows the connection between two neurons (the synapse ). Serotonin is stored in small vesicles within the nerve terminal of a neuron. Electrical impulses (arising in the Raphe nucleus, for example) traveling down the axon toward the terminal cause the release of serotonin from small vesicles into the synaptic space. Point to the space between the terminal and the neighboring neuron. Once in the synaptic space, the serotonin binds to special proteins, called receptors, on the membrane of a neighboring neuron (this is usually at a dendrite or cell body). When serotonin binds to serotonin receptors (there are actually at least 14 types of serotonin receptors), it causes a change in the electrical properties of the receiving neuron that generally results in a decrease in its firing rate. Go to the next slide to explain how the action of serotonin is terminated.")
38
Slide 10: Serotonin Transporters
Serotonin (in pink) is present in the synaptic space only for a limited amount of time. If it is not bound to the serotonin receptor, serotonin is removed from the synaptic space via special proteins called transporters (in green). The serotonin transporters are proteins located on the serotonin neuron terminals and they are in a unique position to transport serotonin from the synaptic space back into the neuron where it can be metabolized by enzymes. Explain to your students that the serotonin transporters are the primary targets for Ecstasy.
 is present in the synaptic space only for a limited amount of time. If it is not bound to the serotonin receptor, serotonin is removed from the synaptic space via special proteins called transporters (in green). The serotonin transporters are proteins located on the serotonin neuron terminals and they are in a unique position to transport serotonin from the synaptic space back into the neuron where it can be metabolized by enzymes. Explain to your students that the serotonin transporters are the primary targets for Ecstasy.")
39
Slide 11: Ecstasy and Serotonin Transporters
When Ecstasy binds to the serotonin transporters, more serotonin ends up in the synaptic space. This occurs for two reasons. First, Ecstasy can prevent the transporters from carrying serotonin back into the terminal. Second, Ecstasy can cause the transporters to work in reverse mode-- they actually bring serotonin from the terminal into the synaptic space. So, more serotonin is present in the synaptic space and more serotonin receptors become activated. This is the major short-term effect of Ecstasy that alters brain chemistry. While the serotonin system is the primary target for Ecstasy, Ecstasy has similar effects on the dopamine (another neurotranmsitter) system as well. Ecstasy can inhibit dopamine transporters and cause an increase in dopamine levels in the synaptic space (not shown here). To help students understand how the alteration in brain chemistry results in psychological changes, go to the next slide.
 system as well. Ecstasy can inhibit dopamine transporters and cause an increase in dopamine levels in the synaptic space (not shown here). To help students understand how the alteration in brain chemistry results in psychological changes, go to the next slide.")
40
Effetti acuti ecstasy percezioni più vive stimolazione
miglioramento umore percezioni più vive stimolazione appetito ridotto Slide 12: Short-term (acute) Effects of Ecstasy Explain that when a person uses Ecstasy, the increase in serotonin in different brain regions (i.e. the areas where serotonin neurons traveling from the raphe nucleus terminate) causes psychological effects. These include, elevated mood and feelings of empathy. The Ecstasy is also reinforcing; this means that its pleasurable properties increase the likelihood that the person will take it again. Tell the students that drugs that are reinforcing are usually addictive. Students might ask you if Ecstasy is addictive. Scientists and health professionals don't have a definative answer yet, because Ecstasy use has not reached the level of cocaine abuse (although, if Ecstasy use continues to rise at the current rate, it will be only a matter of time until we see that Ecstasy, like other amphetamines, is addictive.) For now, there are several pieces of evidence that suggest that Ecstasy has the potential to be addictive. For example, in a research setting, monkeys will administer Ecstasy to themselves (they actually press a lever to obtain an injection), just as they do for other addictive drugs. Monkeys will not self-administer drugs that are not addictive. In addition, there is emerging research to show that Ecstasy has actions in a specific pathway within the limbic system called the the 'reward pathway'--which can explain it's reinforcing effects. In fact, all addictive drugs act in some way within the 'reward pathway'. For more information on this, see the NIDA Teaching Packet referenced at the end. Many of the psychological effects of Ecstasy are due to its actions within the limbic system (the amygdala, in red, and hippocampus, in blue, especially). The ability of Ecstasy to produce mild stimulation is due to its actions in another part of the limbic system -- the basal ganglia (in purple). It is here where Ecstasy's effects on the dopamine system may be important. The heightened perceptions involve the actions of ecstasy in the neocotex (in yellow). Ecstasy can also reduce the appetite, because it acts in the hypothalamus (in green), which controls feeding behavior.
 Effects of Ecstasy. Explain that when a person uses Ecstasy, the increase in serotonin in different brain regions (i.e. the areas where serotonin neurons traveling from the raphe nucleus terminate) causes psychological effects. These include, elevated mood and feelings of empathy. The Ecstasy is also reinforcing; this means that its pleasurable properties increase the likelihood that the person will take it again. Tell the students that drugs that are reinforcing are usually addictive. Students might ask you if Ecstasy is addictive. Scientists and health professionals don t have a definative answer yet, because Ecstasy use has not reached the level of cocaine abuse (although, if Ecstasy use continues to rise at the current rate, it will be only a matter of time until we see that Ecstasy, like other amphetamines, is addictive.) For now, there are several pieces of evidence that suggest that Ecstasy has the potential to be addictive. For example, in a research setting, monkeys will administer Ecstasy to themselves (they actually press a lever to obtain an injection), just as they do for other addictive drugs. Monkeys will not self-administer drugs that are not addictive. In addition, there is emerging research to show that Ecstasy has actions in a specific pathway within the limbic system called the the reward pathway --which can explain it s reinforcing effects. In fact, all addictive drugs act in some way within the reward pathway . For more information on this, see the NIDA Teaching Packet referenced at the end. Many of the psychological effects of Ecstasy are due to its actions within the limbic system (the amygdala, in red, and hippocampus, in blue, especially). The ability of Ecstasy to produce mild stimulation is due to its actions in another part of the limbic system -- the basal ganglia (in purple). It is here where Ecstasy s effects on the dopamine system may be important. The heightened perceptions involve the actions of ecstasy in the neocotex (in yellow). Ecstasy can also reduce the appetite, because it acts in the hypothalamus (in green), which controls feeding behavior.")
41
Effetti avversi ecstasy
pensieri nebulosi ipertermia comportamento alterato Slide 13: Short-Term Adverse Effects People who take Ecstasy desire its pleasurable or reinforcing effects (just described above). However, few drugs are able to produce desirable effects without also producing side effects. Ecstasy is no exception, and there are several side effects or adverse effects that can occur, especially if the dose increases. Some people who take only one Ecstasy pill may have negative psychological effects such as clouded thinking, agitation and disturbed behavior. Point to areas of the brain where Ecstasy may produce these adverse effects (the neocortex, in yellow and limbic structures, in red and blue). Other adverse effects can occur as well. These include sweating, dry mouth (thirsty), increased heart rate, fatigue, muscle spasms (especially jaw-clenching) and hyperthermia. In the latter case, Ecstasy can disrupt the ability of the brain to regulate body temperature. This usually results in hyperthermia, especially when the user is in a hot environment and/or engaging in intense physical activity such as fast dancing at rave parties. You can provide some examples to show where Ecstasy produces these side effects. For example, the development of thirst and the hyperthermia are due to actions of Ecstasy in the hypothalamus (green), which controls drinking behavior and body temperature. You might point out that the effect of Ecstasy on the hypothalamus causes multiple effects in the body, and in some cases they are very dangerous (see the next slide). The muscle spasms and jaw-clenching are due to Ecstasy’s action at the motor neurons in the spinal cord (in yellow) (remind the students that a major serotonin pathway descends down the spinal cord). The motor neurons send signals to the muscles to contract. disturbi mascellari
. However, few drugs are able to produce desirable effects without also producing side effects. Ecstasy is no exception, and there are several side effects or adverse effects that can occur, especially if the dose increases. Some people who take only one Ecstasy pill may have negative psychological effects such as clouded thinking, agitation and disturbed behavior. Point to areas of the brain where Ecstasy may produce these adverse effects (the neocortex, in yellow and limbic structures, in red and blue). Other adverse effects can occur as well. These include sweating, dry mouth (thirsty), increased heart rate, fatigue, muscle spasms (especially jaw-clenching) and hyperthermia. In the latter case, Ecstasy can disrupt the ability of the brain to regulate body temperature. This usually results in hyperthermia, especially when the user is in a hot environment and/or engaging in intense physical activity such as fast dancing at rave parties. You can provide some examples to show where Ecstasy produces these side effects. For example, the development of thirst and the hyperthermia are due to actions of Ecstasy in the hypothalamus (green), which controls drinking behavior and body temperature. You might point out that the effect of Ecstasy on the hypothalamus causes multiple effects in the body, and in some cases they are very dangerous (see the next slide). The muscle spasms and jaw-clenching are due to Ecstasy’s action at the motor neurons in the spinal cord (in yellow) (remind the students that a major serotonin pathway descends down the spinal cord). The motor neurons send signals to the muscles to contract. disturbi mascellari.")
42
Effetti mortali ecstasy
ipertermia aritmia Slide 14: Life-Threatening Effects After Multiple Doses or “Stacking” Some people take multiple doses of Ecstasy in one night (“stacking”) This might be due to the reinforcing effect of the drug. Often, if something feels good, one wants to do it again! Unfortunately, the increased dose also increases the adverse effects, and some of these can become life-threatening. For example, repeated doses or a high dose of Ecstasy can cause heat injury due to hyperthermia, hypertension (high blood pressure), cardiac arrhythmias (irregular heart beat), muscle breakdown and renal failure due to salt and fluid depletion. Indicate that these dangerous effects can be produced by Ecstasy acting in the brain. Again, the hypothalamus is very important, because it regulates heart rate and blood pressure, fluid retention and kidney function and, of course, body temperature. If the body temperature gets too high, it can cause brain damage or even kill a person. blocco renale
 This might be due to the reinforcing effect of the drug. Often, if something feels good, one wants to do it again! Unfortunately, the increased dose also increases the adverse effects, and some of these can become life-threatening. For example, repeated doses or a high dose of Ecstasy can cause heat injury due to hyperthermia, hypertension (high blood pressure), cardiac arrhythmias (irregular heart beat), muscle breakdown and renal failure due to salt and fluid depletion. Indicate that these dangerous effects can be produced by Ecstasy acting in the brain. Again, the hypothalamus is very important, because it regulates heart rate and blood pressure, fluid retention and kidney function and, of course, body temperature. If the body temperature gets too high, it can cause brain damage or even kill a person. blocco renale.")
43
Caffeina Stimolante del SNC Controversi gli effetti sulla performance
L’ultima lista WADA non l’inserisce più tra le sostanze vietate (prima lo era per valori urinari superiori a 12 mcg/ml). Uno studio effettuato per verificare se dopo l’eliminazione dalla lista ci fosse un aumento del ricorso alla caffeina da parte degli atleti dimostrerebbe che ciò non si è verificato (Int J Sports Med 2006; 27:745) Migliora l’attenzione, accorcia i tempi di reazione provoca diuresi, fa sentire meno o ritarda l’affaticamento Provoca dispepsia, danni cardiaci, disidratazione, la combinazione con altri stimolanti SNC può anche essere fatale
. Uno studio effettuato per verificare se dopo l’eliminazione dalla lista ci fosse un aumento del ricorso alla caffeina da parte degli atleti dimostrerebbe che ciò non si è verificato (Int J Sports Med 2006; 27:745) Migliora l’attenzione, accorcia i tempi di reazione provoca diuresi, fa sentire meno o ritarda l’affaticamento. Provoca dispepsia, danni cardiaci, disidratazione, la combinazione con altri stimolanti SNC può anche essere fatale.")
44
Influenze della caffeina che possono portare a migliorare la performance, ma anche a danni
Sistema Nervoso Centrale Cuore Muscoli scheletrici Mobilizzazione glucosio e grassi

45
Meccanismo attraverso cui la caffeina può incrementare la mobilizzazione dei grassi

46
Cannabinoidi Marijuana, hashish Presenti nella lista WADA
Il principale principio attivo è il tetraidrocannabinolo (THC) Uso di tipo voluttuario. Molti atleti usano i THC come miorilassanti e ipnoinducenti Alcuni studi mostrano un maggior uso negli atleti maschi rispetto ai non atleti, l’inverso per le femmine Più che migliorare possono peggiorare la prestazione sportiva Possono provocare percezione distorta, sindromi amotivazionali, paranoia, disturbi psicomotori, tachicardia, cefalea, diminuire il testosterone quando usati a lungo, tipici problemi respiratori da fumo
 Uso di tipo voluttuario. Molti atleti usano i THC come miorilassanti e ipnoinducenti. Alcuni studi mostrano un maggior uso negli atleti maschi rispetto ai non atleti, l’inverso per le femmine. Più che migliorare possono peggiorare la prestazione sportiva. Possono provocare percezione distorta, sindromi amotivazionali, paranoia, disturbi psicomotori, tachicardia, cefalea, diminuire il testosterone quando usati a lungo, tipici problemi respiratori da fumo.")
47
Slide 22: THC binding to THC receptors in the nucleus accumbens: increased dopamine release
[Note to scientists - the interaction of THC with the reward system is not fully understood at this point. The following discussion is based on recent data, but additional theories may emerge as we obtain more data.] State that scientists know the least about THC. Over the last few years, there has been intense study to discover where and how THC works. One theory is that it acts in a similar way to opiates. Again use the nucleus accumbens as an example. The same 3 neurons are probably involved; the dopamine terminal, another terminal (on the right) containing a different neurotransmitter (probably GABA), and the post-synaptic cell containing dopamine receptors. Ask the students if they can tell you how THC might work. THC binds to THC receptors (magenta) on the neighboring terminal and this sends a signal to the dopamine terminal to release more dopamine. [Again, it is probably a presynaptic receptor on GABA interneurons that controls dopamine release.]
 containing a different neurotransmitter (probably GABA), and the post-synaptic cell containing dopamine receptors. Ask the students if they can tell you how THC might work. THC binds to THC receptors (magenta) on the neighboring terminal and this sends a signal to the dopamine terminal to release more dopamine. [Again, it is probably a presynaptic receptor on GABA interneurons that controls dopamine release.]")
48
La cannabis indica La canapa indiana (cannabis indica) è una pianta originaria dell’Asia Centrale, delle zone tropicali e temperate, ma ormai è coltivata in tutto il pianeta. Dalla canapa indiana si estraggono la marijuana e l’hashish. Si ipotizza che l’uso della canapa indiana è iniziato in età neolitica nei territori dell’attuale Afghanistan. Da qui si sarebbe diffuso verso la Cina, dove il suo uso come sedativo è documentato in un trattato cinese di botanica del 1500 a.C. In India la canapa era ritenuta di origine divina, poiché si pensava provenisse dalla trasformazione dei peli della schiena di Visnù. In tutto il mondo islamico la canapa era tenuta in grandissima considerazione, poiché favoriva l’unione con la divinità.
 è una pianta originaria dell’Asia Centrale, delle zone tropicali e temperate, ma ormai è coltivata in tutto il pianeta. Dalla canapa indiana si estraggono la marijuana e l’hashish. Si ipotizza che l’uso della canapa indiana è iniziato in età neolitica nei territori dell’attuale Afghanistan. Da qui si sarebbe diffuso verso la Cina, dove il suo uso come sedativo è documentato in un trattato cinese di botanica del 1500 a.C. In India la canapa era ritenuta di origine divina, poiché si pensava provenisse dalla trasformazione dei peli della schiena di Visnù. In tutto il mondo islamico la canapa era tenuta in grandissima considerazione, poiché favoriva l’unione con la divinità.")
49
I Cannabinoidi: (contenuto in THC)
Marijuana (0,5 – 1,5%) Ganja (2 - 4%) Hashish (3 - 7%) (nero, afgano, pakistano…) Olio di hashish ( %) Sintetici: nabilone, dronabinolo, con potenza superiore ai naturali
 Ganja (2 - 4%) Hashish (3 - 7%) (nero, afgano, pakistano…) Olio di hashish ( %) Sintetici: nabilone, dronabinolo, con potenza superiore ai naturali.")
50
Effetti del THC Effetti sedativi ed euforici
Effetti allucinogeni (a dosi alte) Sensazione di benessere Rilassamento, calore Aumento dell’appetito Arrossamento tipico degli occhi Percezione alterata del tempo Sollievo dall’ansia Ansia e panico (timore di perdere il controllo) Incoordinazione motoria Difficoltà alla concentrazione Stato confusionale Nausea ….paranoia….compromissione delle capacità mnemoniche…SLATENTIZZAZIONE DI PSICOSI… …SINDROME AMOTIVAZIONALE (apatia, il soggetto appare inerte, perdita di interessi, abulia…)
 Sensazione di benessere. Rilassamento, calore. Aumento dell’appetito. Arrossamento tipico degli occhi. Percezione alterata del tempo. Sollievo dall’ansia. Ansia e panico (timore di perdere il controllo) Incoordinazione motoria. Difficoltà alla concentrazione. Stato confusionale. Nausea. ….paranoia….compromissione delle capacità mnemoniche…SLATENTIZZAZIONE DI PSICOSI… …SINDROME AMOTIVAZIONALE (apatia, il soggetto appare inerte, perdita di interessi, abulia…)")
51
Alcune caratteristiche del THC
Distribuzione ai vari organi, soprattutto in quelli ad elevata concentrazione di adipe Eliminazione lenta: rimane nell’organismo per svariati giorni L’eliminazione lenta tende a prolungare ed intensificare gli effetti dei cannabinoidi successivamente fumati No sindrome astinenziale: tuttavia l’interruzione può determinare nervosismo, irrequitezza, diminuizione dell’appetito con perdita di peso, insonnia, aumento del sonno REM, tremore… Dipendenza psicologica soprattutto dovuta al piacere indotto dalla sostanza e al condizionamento del gruppo Forte tolleranza

52
Discipline sportive in cui l’alcool è vietato in competizione (> 0,1 g/L)
P1 Alcool: aeronautica, automobilismo, arco, bocce, bowling, karate, pentatlon moderno per discipline tiro, motociclismo, motonautica La presenza dell’alcool viene determinata mediante analisi dell’espirato e/o del sangue. Come paragone si ricorda che in Italia il limite legale per la guida è di 0.5 g/L.

53
L’alcol vietato in alcuni sport ma l’abuso dannoso per tutti
Uso frequente In passato l’uso di liquori (es. brandy) come doping era una pratica diffusa Tradizionalmente uno degli sport dove è più frequente l’uso di alcol è il rugby
 come doping era una pratica diffusa. Tradizionalmente uno degli sport dove è più frequente l’uso di alcol è il rugby.")
54
L’alcol vietato in alcuni sport ma l’abuso dannoso per tutti
EFFETTI DOSE DIPENDENTI EFFETTI INDESIDERATI Depressione Attività riflesse già a piccole dosi Riduzione ansia e tensione nervosa Assunto a piccole dosi riduce l’ansia e la tensione nervosa Aumento della sicurezza di sé Alte dosi e ripetute Depressione dell’attività del sistema nervoso Alterazione della coordinazione Danni epatici

55
Alcool L’ingrediente tossico è l’alcool etilico (incolore e insapore quando è puro). Si misura in grammi. 10 grammi di alcool (1 unità) corrispondono a: Una birra piccola (circa 300 ml) (alc. vol. 4-6%) Un bicchiere (piccolo) di vino (100 ml) (alc. vol %) Un bicchierino di superalcolici (30 ml) (vodka, rum, whisky, grappa, amari ecc.) (alc. vol %) Un consumo medio prevede non più di 4-5 unità al giorno (in media) comunque non più di 6-7 nello stesso giorno (due-tre in meno per le donne)
 corrispondono a: Una birra piccola (circa 300 ml) (alc. vol. 4-6%) Un bicchiere (piccolo) di vino (100 ml) (alc. vol %) Un bicchierino di superalcolici (30 ml) (vodka, rum, whisky, grappa, amari ecc.) (alc. vol %) Un consumo medio prevede non più di 4-5 unità al giorno (in media) comunque non più di 6-7 nello stesso giorno (due-tre in meno per le donne)")
56
Alcool Le donne sono più esposte (hanno minore quantità di un enzima, l’alcol deidrogenasi) Intossicazione acuta: la sintomatologia compare con dosi di 1 grammo per kg di peso corporeo. La morte può avvenire per dosi di circa 5-6 grammi per kg di peso corporeo L’alcool interagisce con molte sostanze. L’alcool aumenta l’effetto di tutte le droghe

57
Consumatori di alcol in Italia (Fonte: Osservatorio permanente su giovani e alcol. Indagine Doxa 2001) Uso: 88% maschi, 73% femmine

58
Consumatori eccessivi di alcol in Italia (Fonte: Osservatorio permanente su giovani e alcol. Indagine Doxa 2001) % sul totale consumatori Eccedenza 9,6% maschi; 2,4% femmine; Abuso: 2,1% machi, 0,6% femmine

59
L’alcol vietato in alcuni sport ma l’abuso dannoso per tutti
Impatto negativo sui tempi di reazione, sulla cordinazione occhio-mano e occhio-piede, sull’equilibrio, sulla contrazione muscolare per diminuita produzione di ATP (l'alcol etilico influenza il metabolismo epatico dei glucidi inibendo il processo di sintesi del glucosio, il suo deposito sotto forma di glicogeno e attivando il processo di demolizione del glicogeno, in questo modo tende a esaurire le scorte glicidiche e ostacola la loro reintegrazione) Squilibri ormonali (es. inibizione ipotalamica della produzione di GH) Eccessiva produzione di calore e disidratazione Reazioni avverse: effetti cardiovascolari e GI, deficit nutrizionali, patologie epatiche (cirrosi) e pancreatiche, osteoporosi (uso cronico), alterazioni SNC (atrofia cerebellare), dipendenza
 Squilibri ormonali (es. inibizione ipotalamica della produzione di GH) Eccessiva produzione di calore e disidratazione. Reazioni avverse: effetti cardiovascolari e GI, deficit nutrizionali, patologie epatiche (cirrosi) e pancreatiche, osteoporosi (uso cronico), alterazioni SNC (atrofia cerebellare), dipendenza.")
60
Dopo la droga: alcool

61
Altri farmaci (non vietati) anti-tremore: gli ansiolitici
Barbiturici Benzodiazepine (BDZ) I barbiturici nella pratica clinica sono stati sostituiti , per la loro minore tossicità, dalla benzodiazepine (Valium®, Halcion®, En®, Xanax®, ecc. ecc.) E’ difficile stimare il ricorso agli ansiolitici da parte di atleti Gli effetti farmacologici delle BDZ sono: Ansiolitico Ipnotico Anticonvulsivante Miorilassante
 I barbiturici nella pratica clinica sono stati sostituiti , per la loro minore tossicità, dalla benzodiazepine (Valium®, Halcion®, En®, Xanax®, ecc. ecc.) E’ difficile stimare il ricorso agli ansiolitici da parte di atleti. Gli effetti farmacologici delle BDZ sono: Ansiolitico. Ipnotico. Anticonvulsivante. Miorilassante.")
62
BENZODIAZEPINE potenziamento GABA inibizione NA DA Ach 5-HT GLICINA
Possibile meccanismo d’azione delle benzodiazepine. NA = noradrenalina; DA = dopamina; Ach = acetilcolina; 5-HT = serotonina

63
BENZODIAZEPINE: reazioni avverse
Comuni Meno comuni Rare Eccessiva sedazione Effetti residui dopo l’assunzione serale (hangover) Diminuzione della performance psicomotoria e cognitiva Stanchezza muscolare Disturbi della memoria (amnesia anterograda) Confusione mentale (soprattutto negli anziani) Atassia, vertigini Effetti paradossi (stati di irrequietezza, irritabilità depressione Reazioni cutanee Il problema più serio è la possibilità d’insorgenza della dipendenza
 Diminuzione della performance psicomotoria e cognitiva. Stanchezza muscolare. Disturbi della memoria (amnesia anterograda) Confusione mentale (soprattutto negli anziani) Atassia, vertigini. Effetti paradossi (stati di irrequietezza, irritabilità depressione. Reazioni cutanee. Il problema più serio è la possibilità d’insorgenza della dipendenza.")
Presentazioni simili








, che è originario dei paesi del Medio Oriente.>")











