Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Verificare qualè il migliore trattamento dellasma acuta nei bambini in età prescolare (1,5-6 anni), tenendo conto dellanamnesi specifica del paziente (possibilità: primo episodio o problema ricorrente). E necessario formulare anche una prognosi e valutare quali esami far eseguire. P P bambini in età prescolare con asma (1°episodio/ricorrente) M e F. Non patologie associate I I terapia farmacologica dellattacco acuto C C comparazione efficacia dei diversi farmaci impiegabili O O efficacia (ospedalizzazione); esami diagnostici
 M e F. Non patologie associate I I terapia farmacologica dellattacco acuto C C comparazione efficacia dei diversi farmaci impiegabili O O efficacia (ospedalizzazione); esami diagnostici.")
2
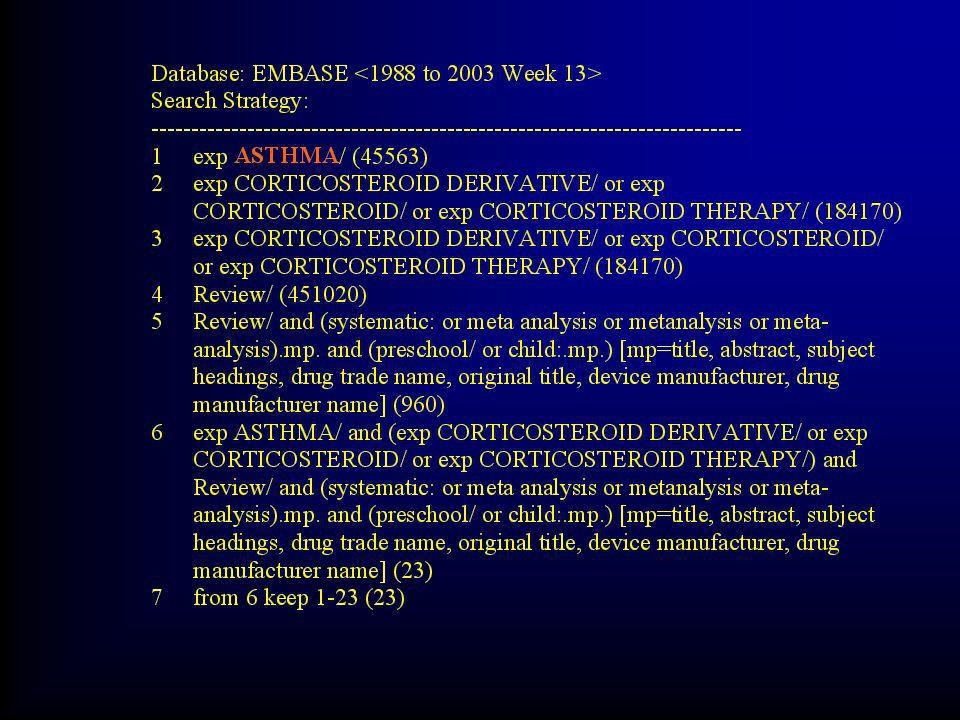
EBM Reviews - Cochrane Database of Systematic Reviews Database: EBM Reviews - Cochrane Database of Systematic Reviews Search Strategy: ----------------------------------------------------------------------------- 1 (acut: asthm: and child:).mp. [mp=title, short title, abstract, full text, keywords, caption text] (42) 2 limit 1 to systematic reviews (30) 3 from 2 keep 5-8,16-18,20-22,24-25,28-29 (14) 4 from 2 keep 21-22,24-25,28-29 (6) 5 from 3 keep 1-14 (14) 1
 2 limit 1 to systematic reviews (30) 3 from 2 keep 5-8,16-18,20-22,24-25,28-29 (14) 4 from 2 keep 21-22,24-25,28-29 (6) 5 from 3 keep 1-14 (14) 1.")
3
Early emergency department treatment of acute asthma with systemic corticosteroids. Objectives: To determine the benefit of treating patients with acute asthma with systemic corticosteroids within an hour of presenting to the emergency department (ED). Main results: Twelve studies involving 863 patients (435 corticosteroids; 428 placebo). Early use of CS for acute asthma in the ED significantly reduced admission rates (N = 11; pooled OR: 0.40, 95% CI: 0.21 to 0.78). This would correspond with a number needed to treat of 8 (95% CI: 5 to 21). This benefit was more pronounced for those not receiving systemic CS prior to ED presentation (N = 7; OR: 0.37, 95% CI: 0.19 to 0.70) and those with more severe asthma (N = 7; OR: 0.35, 95% CI: 0.21 to 0.59). Oral CS therapy in children was particularly effective (N = 3; OR: 0.24, 95% CI: 0.11 to 0.53); no trials in adults used the oral route. Side effects were not significantly different between corticosteroid treatments and placebo. Conclusions: Use of corticosteroids within 1 hour of presentation to an ED significantly reduces the need for hospital admission in patients with acute asthma. Benefits appear greatest in patients with more severe asthma, and those not currently receiving steroids. Children appear to respond well to oral steroids.
. Main results: Twelve studies involving 863 patients (435 corticosteroids; 428 placebo). Early use of CS for acute asthma in the ED significantly reduced admission rates (N = 11; pooled OR: 0.40, 95% CI: 0.21 to 0.78). This would correspond with a number needed to treat of 8 (95% CI: 5 to 21). This benefit was more pronounced for those not receiving systemic CS prior to ED presentation (N = 7; OR: 0.37, 95% CI: 0.19 to 0.70) and those with more severe asthma (N = 7; OR: 0.35, 95% CI: 0.21 to 0.59). Oral CS therapy in children was particularly effective (N = 3; OR: 0.24, 95% CI: 0.11 to 0.53); no trials in adults used the oral route. Side effects were not significantly different between corticosteroid treatments and placebo. Conclusions: Use of corticosteroids within 1 hour of presentation to an ED significantly reduces the need for hospital admission in patients with acute asthma. Benefits appear greatest in patients with more severe asthma, and those not currently receiving steroids. Children appear to respond well to oral steroids..")
4
EBM Reviews - Cochrane Central Register of Controlled Trials Database: EBM Reviews - Cochrane Central Register of Controlled Trials Search Strategy: -------------------------------------------------------------------------------- 1 (acut: asthm: and child: and corticost:).mp. [mp=title, original title, abstract, mesh headings, heading words, keyword] (29) 2 limit 1 to (clinical trial or comparative study or controlled clinical trial or meta analysis or multicenter study or randomized controlled trial or review) (23) 3from 2 keep 2-6,8,11-13,15-16,18,21-23 (15) 4 lettura /selezione 5
 2 limit 1 to (clinical trial or comparative study or controlled clinical trial or meta analysis or multicenter study or randomized controlled trial or review) (23) 3from 2 keep 2-6,8,11-13,15-16,18,21-23 (15) 4 lettura /selezione 5.")
5
Stesso P (preschool age) Stessa I (corticosteroidi) Stessa C (vs placebo) Stesso O (ospedalizzazione) Trattamento corticosteroideo, associato a beta2 agonisti Utile Efficace nel ridurre il tasso di ospedalizzazione Non gravato da eccesso di tossicità
 Stessa I (corticosteroidi) Stessa C (vs placebo) Stesso O (ospedalizzazione) Trattamento corticosteroideo, associato a beta2 agonisti Utile Efficace nel ridurre il tasso di ospedalizzazione Non gravato da eccesso di tossicità")
6
Database: EBM Reviews - ACP Journal Club Search Strategy: ------------------------------------------------------------------------------- 1 (acut: asthm: and child: and corticost:).mp. [mp=title, abstract, full text, keywords, caption text] (6) 2 limit 1 to (clinical trial or comparative study or controlled clinical trial or meta analysis or multicenter study or randomized controlled trial or review) [Limit not valid; records were retained] (6) 3 from 1 keep 1,5-6 (3) 4 lettura /selezione 3
 2 limit 1 to (clinical trial or comparative study or controlled clinical trial or meta analysis or multicenter study or randomized controlled trial or review) [Limit not valid; records were retained] (6) 3 from 1 keep 1,5-6 (3) 4 lettura /selezione 3.")
7
Stesso P (preschool age) Stessa I (corticosteroidi) Stessa C (vs placebo) Stesso O (ospedalizzazione) Art. 1 I CSS per via inalatoria sono efficaci nel ridurre il tasso di ospedalizzazione Art. 2 Conferma lutilità dellassociazione di beta2 ag/corticosteroidi Art. 3 Fonte di discussione: uso Mg ev utile per PICO ma discordante con Systematic Review

8
Database: EBM Reviews - Database of Abstracts of Reviews of Effectiveness Search Strategy: ----------------------------------------------------------------------------- 1(acut: asthm: and child:).mp. [mp=title, full text, keywords] (5) 2 from 1 keep 1,4 (2) 3 Lettura: Pertinenti per PICO Risultati non applicabili per tossicità (teofillina) o per inefficacia del farmaco testato (ipratropio bromuro)
 2 from 1 keep 1,4 (2) 3 Lettura: Pertinenti per PICO Risultati non applicabili per tossicità (teofillina) o per inefficacia del farmaco testato (ipratropio bromuro).")
9
Passando a PubMed il PICO è cambiato!!!! P P bambini in età prescolare con asma (1°episodio/ricorrente) M e F. Non patologie associate I terapia cortisonica dellattacco acuto C C comparazione efficacia p.o/e.v./placebo O O efficacia (ospedalizzazione); esami diagnostici
 M e F. Non patologie associate I terapia cortisonica dellattacco acuto C C comparazione efficacia p.o/e.v./placebo O O efficacia (ospedalizzazione); esami diagnostici.")
10
Strategia PubMed 1/2

11
Strategia PubMed 2/2

14
Authors Van Asperen PP. Mellis CM. Sly PD. Institution Prof. P.P. Van Asperen, Department of Respiratory Medicine, Children's Hospital at Westmead, Locked Bag 4001, Westmead, NSW 2145; Australia. E-Mail: peterv@chw.edu.au. Title The role of corticosteroids in the management of childhood asthma. Source Medical Journal of Australia. Vol 176(4) (pp 168-173), 2002. Date of Publication: 18 FEB 2002.
 (pp ), Date of Publication: 18 FEB")
15
National Guideline Clearinghouse 4 2 1 Children age 0-18 years treatment for an exacerbation of asthma These guidelines are not intended for use in children likely to be admitted to the intensive care unit (ICU), to require intubation, to require ventilator support or who are in severe respiratory distress; nor are they intended for management of bronchiolitis or conditions characterized by non-bronchodilator-responsive wheezing. Caution should be exercised in managing children with comorbid conditions such as: congenital or acquired cardiovascular disease, cystic fibrosis, chronic lung disease, bronchopulmonary dysplasia, or immunodeficiency syndromes. 2 Adults and children over 5 years old Children less than or equal to 5

16
(Oxygen (O 2 ) saturation (pulse oximetry) Arterial blood gases (ABGs) Chest x-ray (CXR) Complete blood count (CBC) Electrocardiogram (EKG) Electrolytes Test di diagnosi
 saturation (pulse oximetry) Arterial blood gases (ABGs) Chest x-ray (CXR) Complete blood count (CBC) Electrocardiogram (EKG) Electrolytes Test di diagnosi")
17
Authors Sullivan TJ. Institution Department of Internal Medicine, Texas University SW Medical Center,Dallas, TX 75235-8859; United States. Title Is asthma curable? Source Pediatric Clinics of North America. Vol 39(6) (pp 1363-1382), 1992. Conclusioni 1/2
 (pp ), Conclusioni 1/2.")
18
Authors Martin J. Donaldson ANA. Villarroel R. Parmar MKB. Ernst E. Higginson IJ. Institution A.N.A. Donaldson, GKT School of Medicine, Weston Education Centre, Denmark Hill, London SE5 9RJ; United Kingdom. E-Mail: nora.donaldson@kcl.ac.uk. Efficacy of acupuncture in asthma: Systematic review and meta- analysis of published data from 11 randomised controlled trials. Source European Respiratory Journal. Vol 20(4) (pp 846-852), 2002. Date of Publication: 01 OCT 2002. Conclusioni 2/2
 (pp ), Date of Publication: 01 OCT Conclusioni 2/2.")
Presentazioni simili


 Brussels, 26 settembre 2013.>")
 Università degli Studi, Pavia (founder) IRCCS Fondazione.>")






>")




>")




