Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
L’ ANEURISMA AORTICO ADDOMINALE PATRIZIO CASTELLI CHIRURGIA VASCOLARE
DIPARTIMENTO DI SCIENZE CHIRURGICHE E MORFOLOGICHE UNIVERSITA’ DEGLI STUDI DELL’INSUBRIA A.O.U. OSPEDALE DI CIRCOLO E “FONDAZIONE MACCHI” - VARESE

3
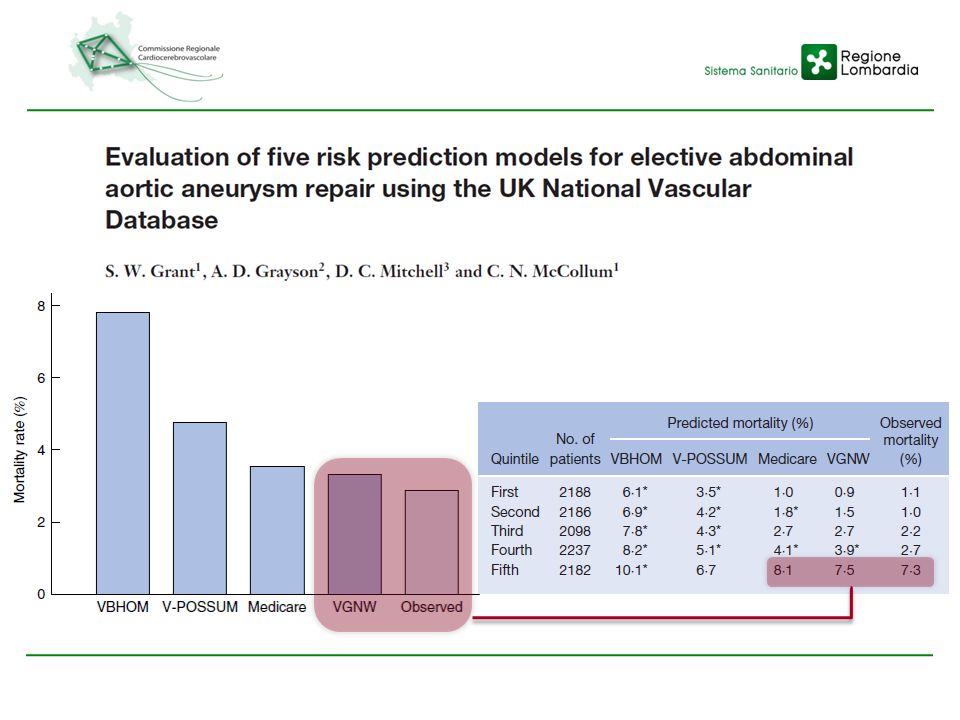
Holt PJE, et al. Provider volume and long-term outcome after elective abdominal aortic aneurysm repair. Br J Surg 2012;99: Barshes NR, et al. Increasing complexity in the open surgical repair of abdominal aortic aneurysms. Ann Vasc Surg 2012;26:10-17 Chadi SA, et al. Trend in management of abdominal aortic aneurysms J Vasc Surg 2012;55: Grant SW, et al. Evaluation of five risk prediction models for elective abdominal aortic aneurysm repair using the UK National Vascular database Br J Surg 2012;99: McPhee JT, et al. Surgeon case volume, not institution case volume, is the primary determinant of in-hospital mortality after elective open abdominal aortic aneurysm repair. J Vasc Surg 2011;53: Brown LC, et al. Use of baseline factors to predict complications and reinterventions after endovascular repair of abdominal aortic aneurysm. Br J Surg 2010;97: Landon BE, et al. Volume-outcome relationship and abdominal aortic aneurysm repair. Circulation 2010;122: Schanzer A, et al. Vascular surgery training trends rfom : a substantial increase in total procedure volume is driven by escalating endovascular procedure volume and stable open procedure volume. J Vasc Surg 2009;49: Hill JS, et al. Regionalization of abdominal aortic aneurysm repair: evidence of a shift to high-volume centers in the endovascular era. J Vasc Surg 2008;48:29-36 Dimick JB, et al. Surgeon specialty and provider volumes are related to outcome of intact aabdominal aortic aneurysm repair in the United States. J Vasc Surg 2003;38:

4
SOTTORENALE IUXTARENALE PSEUDO P.A.U. DISSECANTE

5
ROTTI INTATTI PREVALENZA DIAGNOSI di A.A.A. TRATTAMENTO di A.A.A.

6
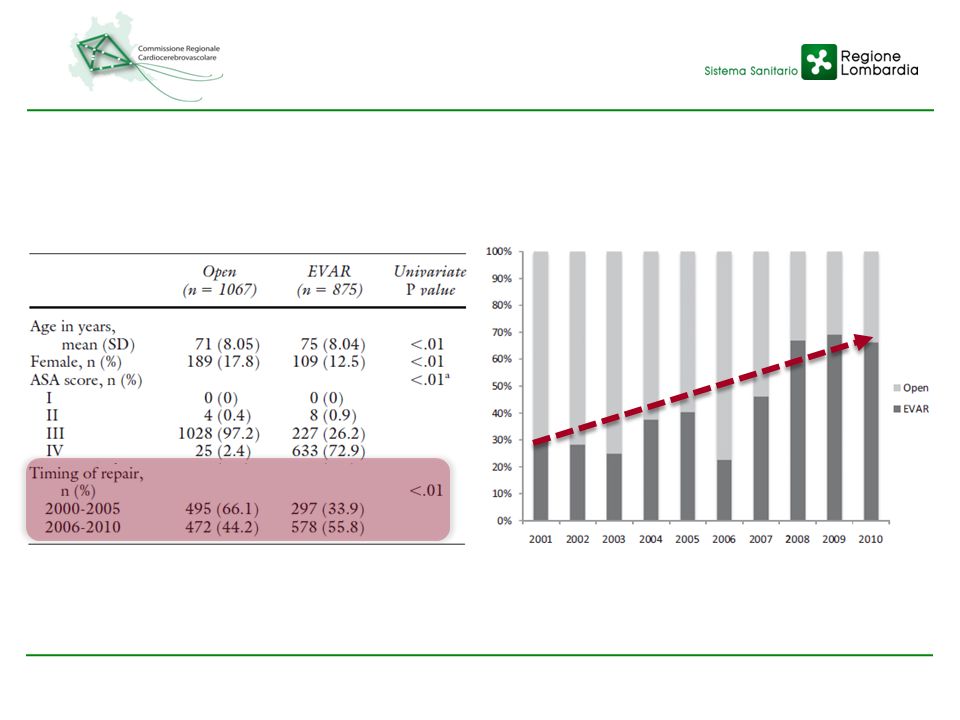
“SHIFT OF THE PARADIGM”

8
CASI EVAR CASI ASA IV CASI 80enni

9
SOPRAVVIVENZA SOVRAPPONIBILE > 2y COMPLICANZE: TASSO PIU’ 30g-6m

11
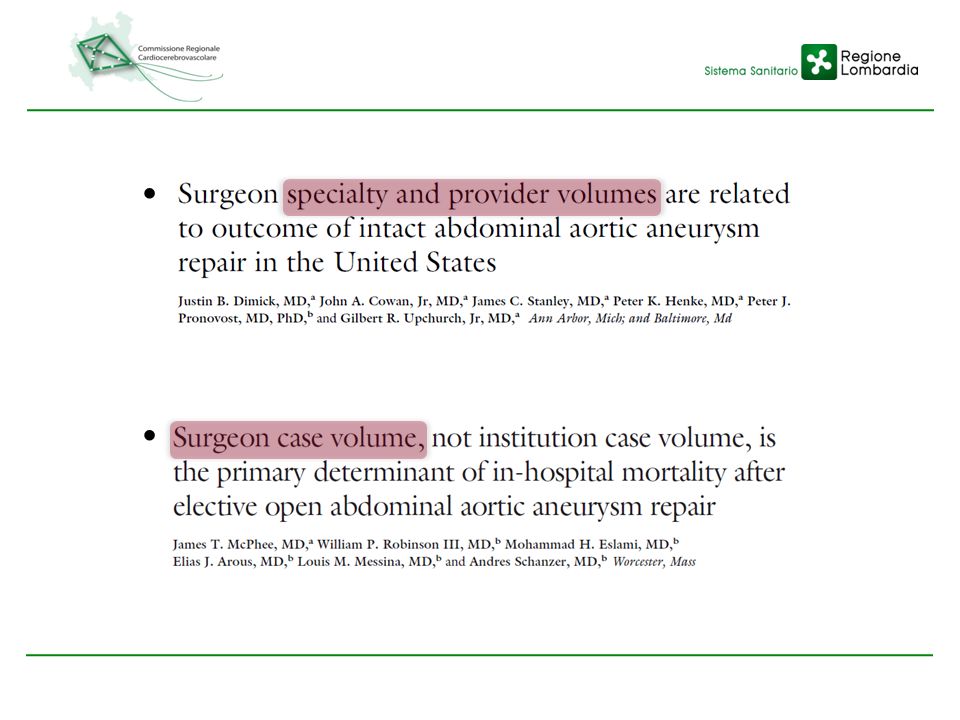
DEFINIZIONE VOLUME DELL’OSPEDALE (“PROVIDER”) DEL CHIRURGO
RIFERIMENTO CONDIVISO: > 30 CASI/y

12
59.7% 40.3%

14
MORTALITA’ HVH SUPERIORITA’ ESTESA AD OLTRE 2 ANNI NONOSTANTE
“HIGH RISK” STRETTAMENTE CORRELATA A 30d “SECONDARY MANAGEMENT”

15
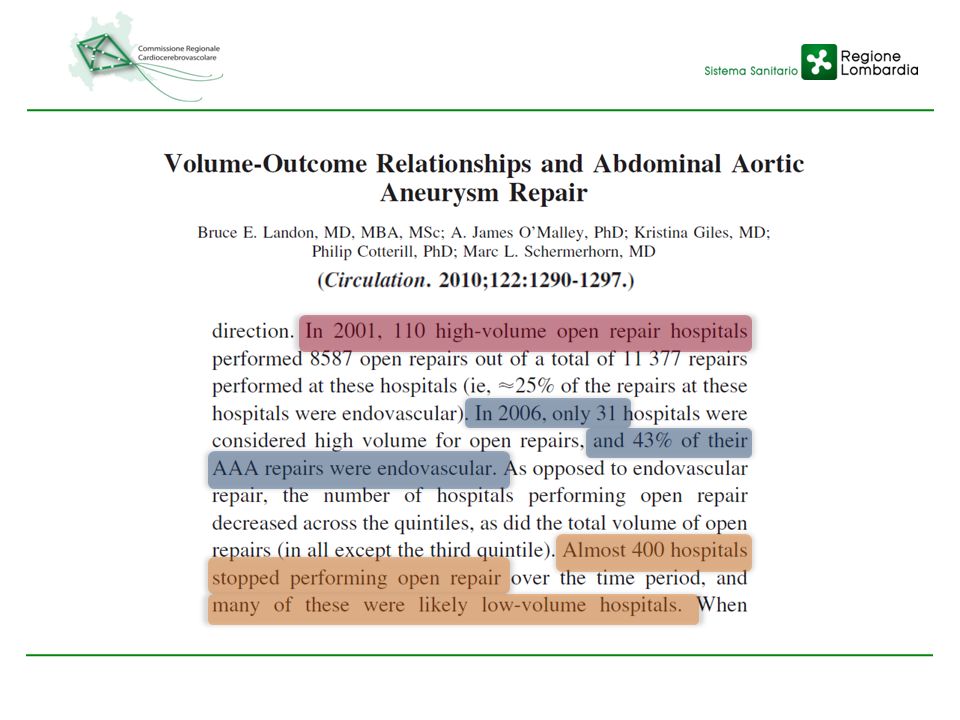
HVH HANNO ADOTTATO EVAR
RAPIDAMENTE E CON MAGGIOR ESTENSIVITA’ DI CASI

16
PIU’ FREQUENTEMENTE NEL CONTESTO DI HVH MA SOLO 27% DEGLI A.A.A. TRATTATI DA CH VASCOLARI PIU’ FREQUENTEMENTE SONO HVS rA.A.A. PIU’ FREQUENTEMENTE OPERATI DA GENERALI

17
MORTALITA’ A.A.A. DETERMINATA DA “EFFETTO ADDITIVO”: VOLUME ANNUALE
DI CHIRURGO E HOSP DISCIPLINA DI SPECIALIZZAZIONE

18
HIGH VOLUME HOSPITAL (A.A.A.) TEACH 44.6% N-TEACH 12.6% URBAN 29.2%
RURAL 3.4% EVAR 62.9% 34.2%

19
NUM DEI CLAMP SOVRARENALE (14.1% vs 30.3%) COMPLICANZE PER CLAMP SOVRARENALE (25.8% vs 31.9%) CLAMP SOVRARENALE (P = .04)
")
Presentazioni simili