Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
QUALE LATTE PER IL TUO BAMBINO Carlo Agostoni Dipartimento di Scienze Cliniche e di Comunità IRCCS Policlinico Cà Granda Università degli Studi di Milano

2
Il latte nel divezzamento (e oltre) Quale latte? Latte materno Formule Latte vaccino
 Quale latte Latte materno Formule Latte vaccino")
3
LATTE MATERNO 24 mesi e anche oltre se la mamma o il bambino lo desiderano WHO

4
IGF-I at 9 Months and Number of Breastfeedings SKOT Cohort P=0.0006 n=115 n=88n=46n=3 Madsen AL, et al. Growth Hormone IGF Res. 2011;21:199-204. 4 In all infants recorded different daily intakes of cow’s milk, infant formula and meat

5
Fasting Insulin at 9 Months and Number of Breastfeedings SKOT Cohort P=0.0015 n=115 n=88n=46n=3 Madsen AL, et al. Diabet Med. 2010;27:1350-1357. 5

6
Allattamento al seno e prevalenza di sovrappeso e obesità in 9357 bambini di età compresa tra 5 e 6 anni (Von Kries R et al, BMJ 1999; 319:147) sovrappeso : BMI> 90 o percentile per età e sesso obesità: BMI>97 o percentile per età e sesso
 sovrappeso : BMI> 90 o percentile per età e sesso obesità: BMI>97 o percentile per età e sesso")
7
Breastfeeding and prevalence of overweight° in over 15000 adolescents aged 9-14 years. (adapted from Gillmann et al, JAMA 2001:285:2461-67) °Overweight was BMI>95th percentile for age and sex
 °Overweight was BMI>95th percentile for age and sex.")
8
Taveras EM et al 2004; 114: e577

9
Life expectancy at birth in EU member states has increased by over 6 years between 1980 and 2010. On average across the European Union, life expectancy at birth for the three-year period 2008-10 was 75.3 years for men and 81.7 years for women. Most European countries have reduced tobacco consumption via public awareness campaigns, advertising bans and increased taxation Alcohol consumption has also fallen in many European countries. In the European Union, 52% of the adult population is now overweight and 17% is obese. The obesity rate has doubled since 1990 in many European countries. Obesity tends to be more common among disadvantaged social groups, and especially women

10
Il latte materno 1. Basso apporto proteico (< 1 g / 100 ml; latte vaccino 3.5 g/100 ml, formule non meno di 1.2- 1.4 g/100 ml) 2. Ottimale rapporto energia/proteine 3. Presenza di numerosi fattori anti-infettivi 3. Grassi e carboidrati con valore funzionale (LCPUFA, oligosaccaridi)
 2. Ottimale rapporto energia/proteine 3. Presenza di numerosi fattori anti-infettivi 3. Grassi e carboidrati con valore funzionale (LCPUFA, oligosaccaridi).")
11
Ljung K et al

12
Formule : quali Formule standard fino a 6 o 12 mesi Formule di seguito tra 6 e 12 mesi Formule di crescita 2 e 3 anni

13
Elementi chiave delle formule 1.Proteine (quantità e qualità) 2.Grassi (quantità e qualità acido linolenico, acido docosaesaenoico) 3.Qualità carboidrati (digeribili/non digeribili) 4.Minerali e micronutrienti (ferro, zinco, calcio, Vitamina D), altri composti “funzionali”
 2.Grassi (quantità e qualità acido linolenico, acido docosaesaenoico) 3.Qualità carboidrati (digeribili/non digeribili) 4.Minerali e micronutrienti (ferro, zinco, calcio, Vitamina D), altri composti funzionali")
14
Is Cows' Milk Harmful for a Child's Health ? Key-note lecture - NUTRITION Carlo Agostoni Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico University of Milan, Italy CHAIR PERSON: Dominique Turck, Lille, France

15
Conclusions: Cow’s Milk harmful? Negative effects on iron status up to 9-12 months, then no negative effects if adequately complemented with iron enriched foods Lactose intolerance easily managed Allergy to WCM proteins may be transient. Atopics may independently be at risk of poor growth A cause-effect relationship with T1D is not established, and the same for ASDs Cow’s milk stimulates IGF-1 and may affect linear growth, but associations with non-communicable diseases is still not convincing

16
Conclusions: Cow’s Milk Safety From 12 months of life onwards Up to around 500 mL per day 250 mL in lactose intolerants Fat-reduced milks after 24-36 months on individual basis

19
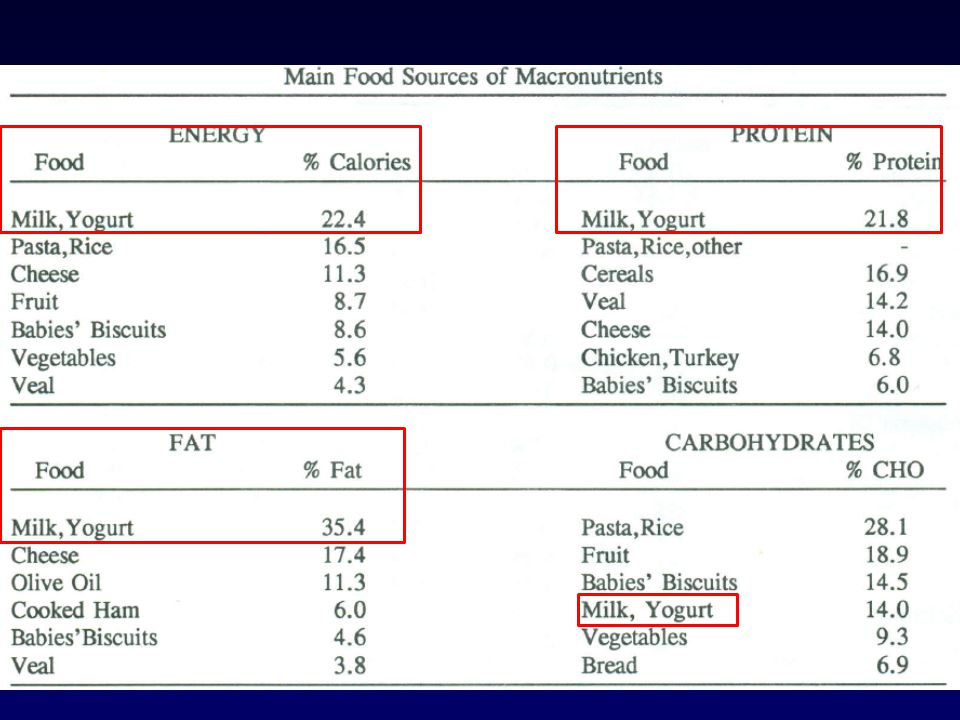
Reports of nutrient intakes in European Countries in the 8-24 mos period Country age(mos) Pg/kg P % Lip% Cho% Spain 9 4.4 15.7 26.4 58 France 10 4.3 15.6 27.1 57 Italy 12 5.1 19.5 30.5 50 Denmark 12-36 3.3 15 28 57 Rolland-Cachera et al. Acta Paed 1999; 88:365

20
Protein/obesity association Author Prot% Age Observation: P (obesity, BMI) Rolland-Cachera 1995 >14.8 2 yrs 8 yrs <0.05 Int J Obes Rel Dis 19:573 Scaglioni 2000 22 1yr 5 yrs <0.05 Int J Obes Rel Dis 24:777 Dorosty 2000 14 18ms Adiposity Rebound NS Pediatrics 105: 1115 Hoppe 2004 13,F, 14,M 9ms 10yrs NS Am J Clin Nutr 79:494 Scaglioni 2004 14 1y 8yrs NS Acta Paediatrica 93:1596
 Rolland-Cachera 1995 > yrs 8 yrs <0.05 Int J Obes Rel Dis 19:573 Scaglioni yr 5 yrs <0.05 Int J Obes Rel Dis 24:777 Dorosty ms Adiposity Rebound NS Pediatrics 105: 1115 Hoppe ,F, 14,M 9ms 10yrs NS Am J Clin Nutr 79:494 Scaglioni y 8yrs NS Acta Paediatrica 93:1596")
21
LARN 2012- PROTEINE AR e PRI Anni kg AR g/d PRI g/d En%* 0.5-0.99 8.6 9 11 -- 1-3 13.7 11 14 4M, 3.7F 4-6 20.6 16 19 4.1M, 4.3F 7-10 31.4 25 31 5M, 5.4F 11-14M 49.7 39 48 5.7M 11-14F 50.7 39 48 6.5F 15-17M 66.6 50 62 6.25M 15-17F 55.7 40 50 6.3F *En% calcolata come AR (fabbisogno medio) proteine vs mediana (kcal/die) fabbisogno energetico per LAF
 proteine vs mediana (kcal/die) fabbisogno energetico per LAF")
22
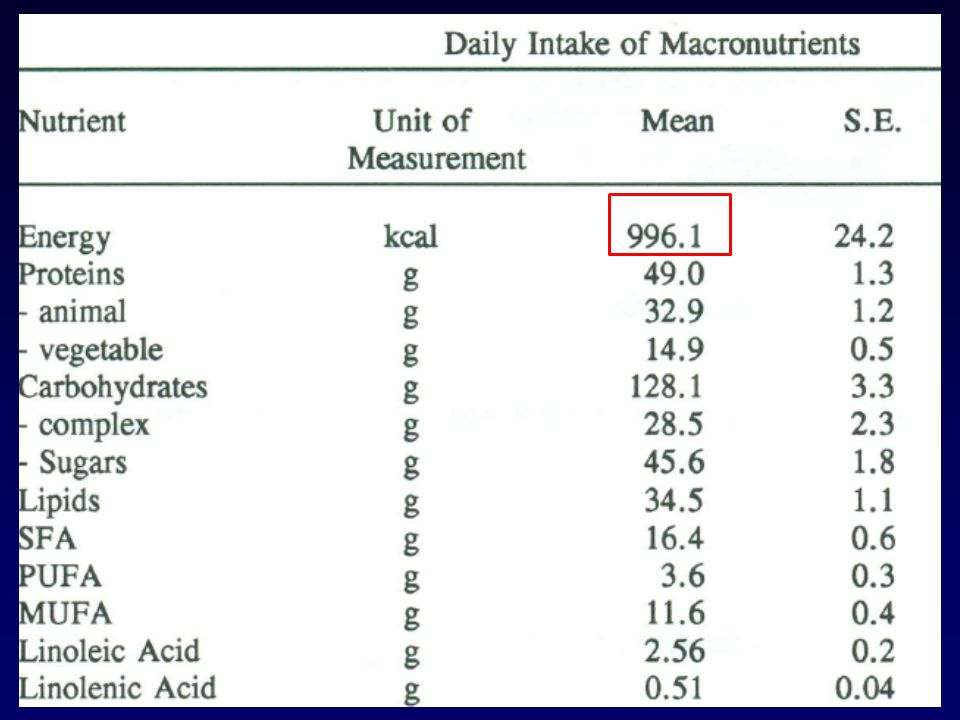
Come ridurre le proteine ? Latte vaccino 500 mL (o equivalente) circa 3.5 g/dL 18 g proteine 72 kcal Latte “formula” 1.5 g dL circa 7.5 g proteine 30 kcal In una dieta giornaliera intorno a 1000 kcal il bambino (con 500 mL di prodotto) passerebbe da circa 45 g proteine (180 kcal, 18% energia) a circa 35 grammi proteine (140 kcal, 14% energia)
 circa 3.5 g/dL 18 g proteine 72 kcal Latte formula 1.5 g dL circa 7.5 g proteine 30 kcal In una dieta giornaliera intorno a 1000 kcal il bambino (con 500 mL di prodotto) passerebbe da circa 45 g proteine (180 kcal, 18% energia) a circa 35 grammi proteine (140 kcal, 14% energia).")
25
Influence of Protein Intake on Metabolic-endocrine Response in Infants Socha P, et al. Am J Clin Nutr. 2011.

26
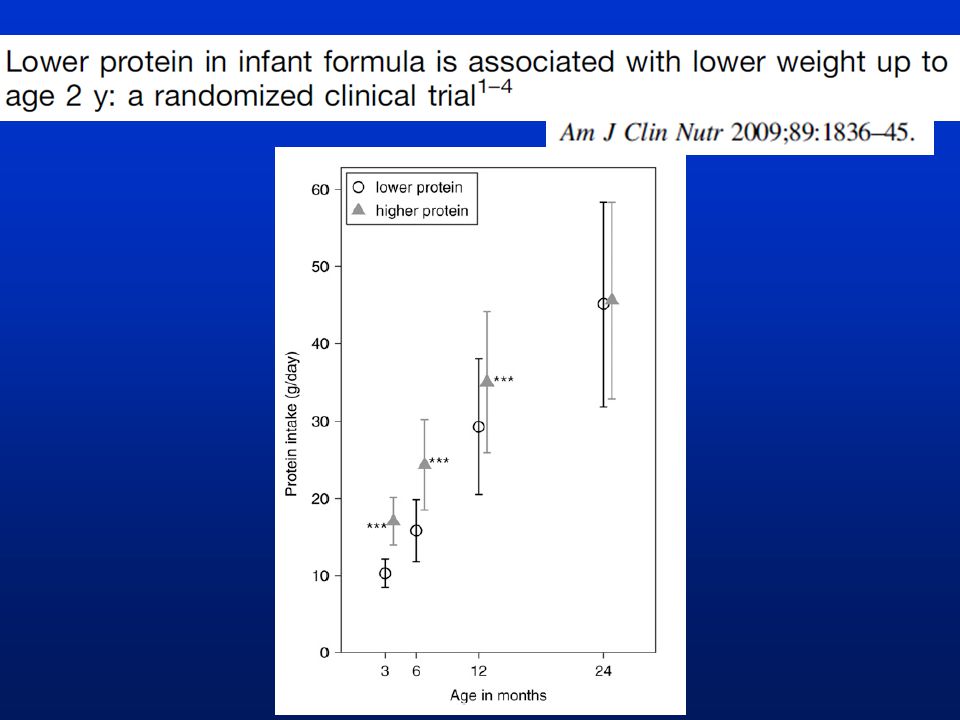
FORMULA TYPE AND PROTEIN INTAKE g/d (SD)En% TimeHPLPP EFSA 2012 PRI g/d T1 14 (3) 119 (1) 70.001 m f T6 10 9 T12 12 11 T18 12 11 T24 12 12 T2 16 (2) 119 (1) 70.001 T3 17 (3) 1110 (1) 70.001 T4 18 (3) 1111 (2) 70.001 T5 21 (5) 1313 (2) 70.001 T6 24 (5) 1415 (4) 80.001 T7 28 (6) 1520 (5) 100.001 T8 30 (7) 1522 (6) 110.001 T9 30 (7) 1524 (7)110.001 T12 35 (9) 1529 (8)130.00131 (9) 14 0.001 0.028 T18 42(12) 16 0.62639 (10) 15 0.004 0.013 T24 45(12) 1645 (13) 160.67943 (11) 16 0.025 0.073 BF P vs HP P vs LP
En% TimeHPLPP EFSA 2012 PRI g/d T1 14 (3) 119 (1) m f T6 10 9 T12 T18 T24 T2 16 (2) 119 (1) T3 17 (3) 1110 (1) T4 18 (3) 1111 (2) T5 21 (5) 1313 (2) T6 24 (5) 1415 (4) T7 28 (6) 1520 (5) T8 30 (7) 1522 (6) T9 30 (7) 1524 (7) T12 35 (9) 1529 (8) (9) T18 42(12) (10) T24 45(12) 1645 (13) (11) BF P vs HP P vs LP")
27
Energy and nutrient content per 100 ml of different milk based products for young children (modified from Nutrition Committee, Germany, 2011)
")
28
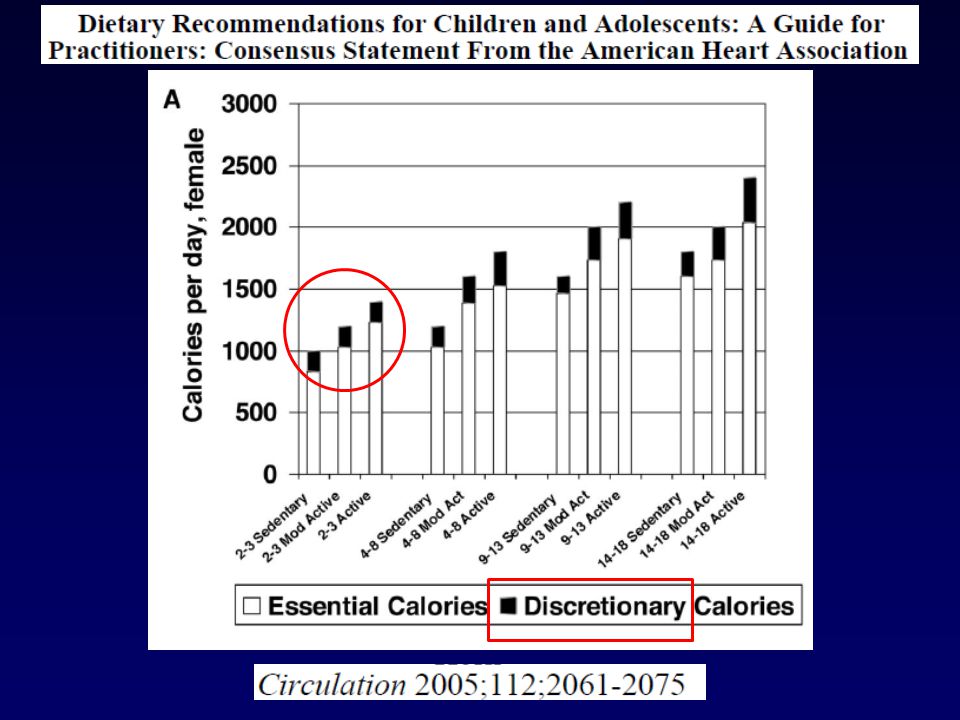
2.9% 6.9% 5.3% Changing protein requirements in relation to different energy intakes: example in young adults Nutrient:energy ratio requirement depends upon the activity level of the individuals in a population

29
29

31
REE, resting energy expenditure predicted with the equations of Henry (2005) using body mass and height. LARN 1120 1382 LARN 1040 1346 mediana

33
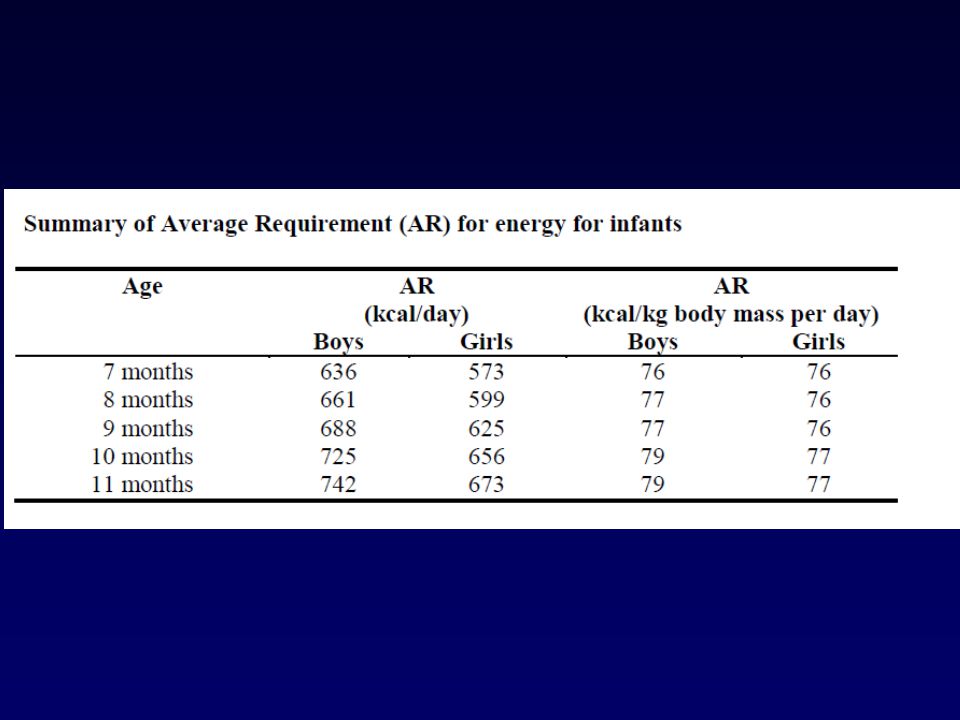
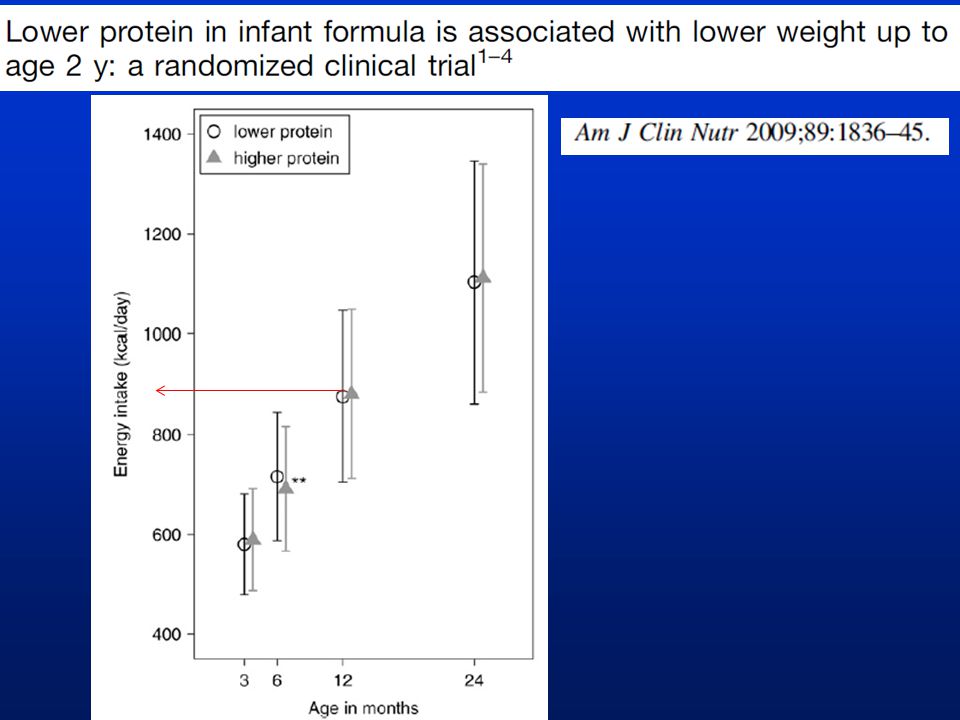
TimeHPLP EFSA 2013 AR M F BF T1509.9 (118)512.46 (110) T2563. (117)559.2 (113) T3595.7 (116)588.9 (118) T4631.1 (113)632.3 (116) T5667.0 (115)678.8 (131) T6 * 700.9 (140)* * 726.6 (147)* T7754.4 (143)765.7 (153)636 573 T8791.4 (155)810.2 (162)661 599 T9814.8 (155)837.8 (188)688 625 T12891.5 (184) a 881.9 (176) a 777 712 792.5(224) b T181043.3 (223)1045.1 (223)988.8 (195) T241119.7 (240)1112.6 (253)1028 9461079.4 (222) FORMULA TYPE AND ENERGY INTAKE k cal/day
559.2 (113) T (116)588.9 (118) T (113)632.3 (116) T (115)678.8 (131) T6 * (140)* * (147)* T (143)765.7 (153) T (155)810.2 (162) T (155)837.8 (188) T (184) a (176) a (224) b T (223) (223)988.8 (195) T (240) (253) (222) FORMULA TYPE AND ENERGY INTAKE k cal/day.")
35
TimeHPLP EFSA 2013 AR M F BF T1509.9 (118)512.46 (110) T2563. (117)559.2 (113) T3595.7 (116)588.9 (118) T4631.1 (113)632.3 (116) T5667.0 (115)678.8 (131) T6 * 700.9 (140)* * 726.6 (147)* T7754.4 (143)765.7 (153)636 573 T8791.4 (155)810.2 (162)661 599 T9814.8 (155)837.8 (188)688 625 T12891.5 (184) a 881.9 (176) a 777 712 792.5(224) b T181043.3 (223)1045.1 (223)988.8 (195) T241119.7 (240)1112.6 (253)1028 9461079.4 (222) FORMULA TYPE AND ENERGY INTAKE k cal/day Circa 20% energia in più dell’AR raccomandato
559.2 (113) T (116)588.9 (118) T (113)632.3 (116) T (115)678.8 (131) T6 * (140)* * (147)* T (143)765.7 (153) T (155)810.2 (162) T (155)837.8 (188) T (184) a (176) a (224) b T (223) (223)988.8 (195) T (240) (253) (222) FORMULA TYPE AND ENERGY INTAKE k cal/day Circa 20% energia in più dell’AR raccomandato.")
36
T1 T2 T3 T4 T5 T6 T7 T8 T9 T12 T24

37
Energy costs of fat and protein deposition in the human infant Am J Clin Nutr 1988; 48:951 Total energy requirement for deposition 1.17 kJ/kJ (kcal/kcal) deposited for fat (ie, 1 kJ deposited and 0.17 kJ expended for deposition, and 2.38 kJ/kJ (kcal/kcal) for protein. The metabolizable-energy requirement for weight gain during infancy was calculated (range, 12.2-25.1 kJ/g, or 2.9-6.0 kcal/g; means, 18.7 kJ/g, or 4.5 kcal/g) from the energy costs of fat and protein deposition and published information on changes in body composition during the first year of life.
 from the energy costs of fat and protein deposition and published information on changes in body composition during the first year of life..")
38
Energy expended by low birth weight infants in the deposition of protein and fat. Pediatr Res 1997 ;41:584 Using multiple regression analysis of energy expenditure against protein stored, and metabolizable energy, the energy expended in the deposition of protein was calculated to be 5.5 kcal/g +/- 1.1 kcal/g (SE) and the energy cost of fat deposited was 1.6 kcal/g +/- 0.3 kcal/g (SE).
 and the energy cost of fat deposited was 1.6 kcal/g +/- 0.3 kcal/g (SE)..")
42
Ghisolfi et al, Public Health Nutr, 2013; 16:524

44
AGE 17 (GUM) – 19 (CM) months 961 + 33 967 + 18
 – 19 (CM) months")
46
46

47
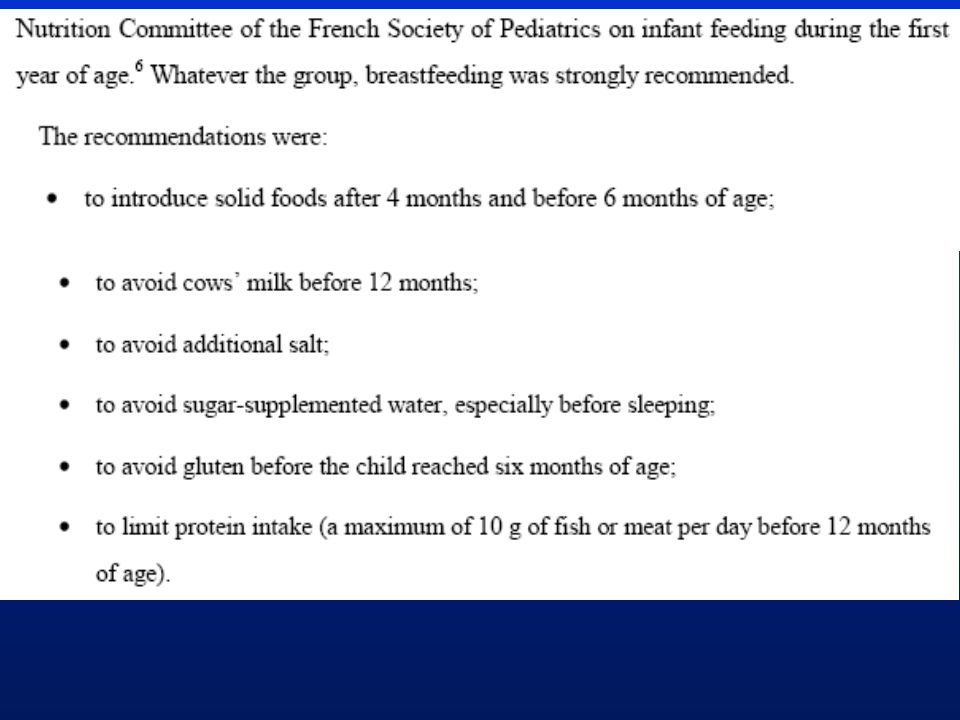
Quando introdurre il latte vaccino ? Non prima del dodicesimo mese latte materno fino ad un anno, anche più a lungo Dopo il 12° mese può essere introdotto il latte vaccino (limitare la quantità?) Tra il 12° ed il 36° mese una formula di crescita - GUM- può migliorare il bilancio dei nutrienti effetti funzionali non noti, mancano dati “diretti” su parametri ematici ATTENZIONE al bilancio energetico nel suo complesso puo’ vanificare ogni altro tentativo di riequilibrio qualitativo e quantitativo
 Tra il 12° ed il 36° mese una formula di crescita - GUM- può migliorare il bilancio dei nutrienti effetti funzionali non noti, mancano dati diretti su parametri ematici ATTENZIONE al bilancio energetico nel suo complesso puo’ vanificare ogni altro tentativo di riequilibrio qualitativo e quantitativo.")
Presentazioni simili


 Brussels, 26 settembre 2013.>")
 Università degli Studi, Pavia (founder) IRCCS Fondazione.>")















>")
