Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
LNH Cosa occorre sapere Eziopatogenesi Fattori eziologici
Classificazione REAL con tipo di aggressività clinica per ogni forma Cellula d’origine B T Livello maturativo della cellula d’origine (se noto) Eziopatogenesi Fattori eziologici Fattori predisponenti Modello EBV e linfoma di B Burkitt, linfoma MALT Patogenesi citogenetico-molecolare Stadiazione Quadri di presentazione e concetti di terapia Principali danni genetici Ann Arbor Relazione coi principali istotipi
 Eziopatogenesi. Fattori eziologici. Fattori predisponenti. Modello EBV e linfoma di B. Burkitt, linfoma MALT. Patogenesi citogenetico-molecolare. Stadiazione. Quadri di presentazione. e concetti di terapia. Principali danni genetici. Ann Arbor. Relazione coi principali istotipi.")
2
Quadro di presentazione generale
Linfoadenopatie in 2/3 dei casi Adenopatia persistente (> 1 cm per >4 settimane) Non dolente Andamento del volume delle adenopatie fluttuante nelle forme indolenti Da differenziare Adenopatie infettive (Batteri, Mononucleosi CMV, HIV,Toxoplasmosi, Istoplasmosi) Sarcoidosi (mediastino) Adenopatie metastatiche Sintomi correlati a linfoadenopatie Mediastino Addome Extranodali Tosse persistente Senso di fastidio retrosternale Sindrome medistinica Senso di gonfiore, dolore, Splenomegalia Linfedema SNC, midollo spinale Gastrico Orbita ossa Testicolo cute Sintomi sistemici 20% circa dei casi Soprattautto negli alti gradi e negli stadi avanzati
 Non dolente. Andamento del volume delle adenopatie fluttuante nelle forme indolenti. Da differenziare. Adenopatie infettive. (Batteri, Mononucleosi CMV, HIV,Toxoplasmosi, Istoplasmosi) Sarcoidosi (mediastino) Adenopatie metastatiche. Sintomi correlati a linfoadenopatie. Mediastino. Addome. Extranodali. Tosse persistente. Senso di fastidio retrosternale. Sindrome medistinica. Senso di gonfiore, dolore, Splenomegalia. Linfedema. SNC, midollo spinale. Gastrico. Orbita. ossa. Testicolo. cute. Sintomi sistemici. 20% circa dei casi. Soprattautto negli alti gradi e negli stadi avanzati.")
3
Schematic representation of the lymph node structure
CELL ORIGIN AND HISTOLOGICAL TYPES OF NHL Schematic representation of the lymph node structure

4
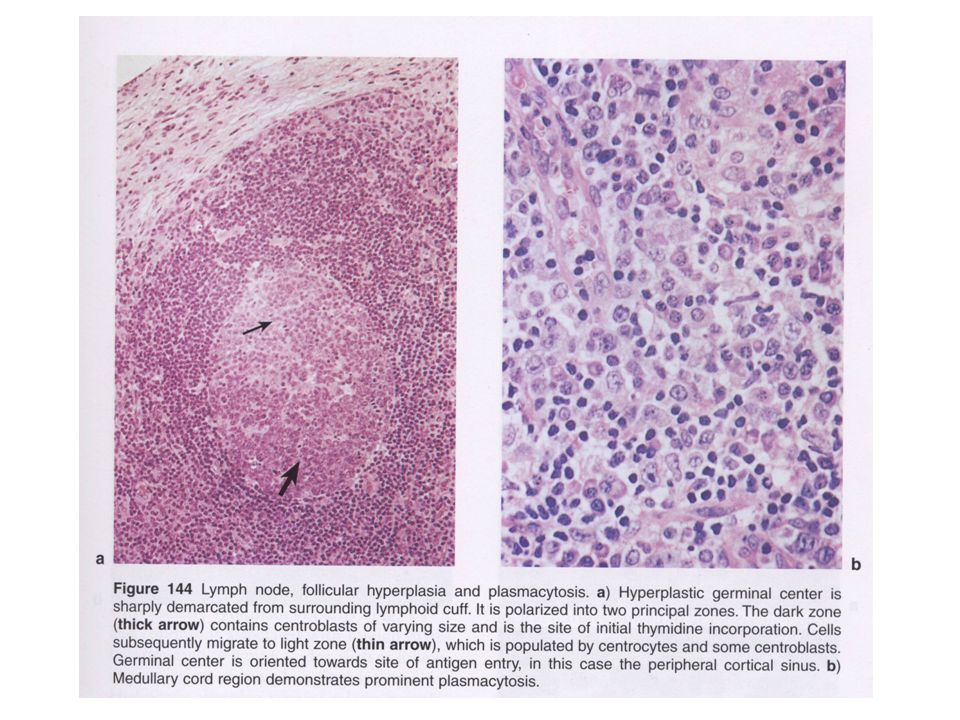
Section of a normal hyperplastic lymph node

5
Follicular lymphoma Cell of origin: centrobasts/centrocytes in the follicole centre which have encountered the Ag Immunophenotype: sIgM>IgG+ sIgD+; cyIg+/-; CD19+; CD5-; CD10+/-; CD43- Follicular lymphoma: neoplastic follicles of uniform shape efface the LN architecture Both centrocytes and centroblasts are present (right)
")
7
The t(14;18) which is the hallmark of FL leads to the overexpression of BCL2 within the
neoplastic follicle (left). Reactive germinal centres are BCL2 negative (right)
. Reactive germinal centres are BCL2 negative (right)")
8
Mantle cell lymphoma: Cell of origin: B-lymph in the follicle mantle which did not encounter the Ag Immunophenotype: CD19+; CD5+; sIgM>D+CD10-/+; CD23-; CD43+ Cyclin D1 overxpression by Neoplastic cells and not by GC cells The lymph node architecture is replaced by centrocyte-like cells Residual germinal centre cells (arrow)
")
9
Cell origin of B-lymphoid neoplasia
Pre-germinal centre (no IGVH mutation) (post)-germinal centre (IGVH mutation) Mantle cell Lymphoma Diffuse large B cell lymphoma Follicular lymphoma Multiple myeloma Burkitt’s lymphoma Lymphoblastic NHL Germinal centre Pre-plasma cell Plasma cell Naive B-cell (no Ag) B-precursor cell Mantle zone Lymphoplasmacytic lymphoma Marginal zone Marginal zone Lymphoma Small lymphocytic lymphoma Memory B-cell Bone marrow blood LYMPH NODE
 (post)-germinal centre (IGVH mutation) Mantle cell. Lymphoma. Diffuse large B cell lymphoma. Follicular lymphoma. Multiple. myeloma. Burkitt’s lymphoma. Lymphoblastic NHL. Germinal. centre. Pre-plasma cell. Plasma cell. Naive B-cell. (no Ag) B-precursor cell. Mantle zone. Lymphoplasmacytic. lymphoma. Marginal zone. Marginal zone Lymphoma. Small lymphocytic lymphoma. Memory. B-cell. Bone marrow. blood. LYMPH NODE.")
10
Cell origin of T-lymphoid neoplasia
Mycosis fungoides Sezary’s syndrome T-cell CLL/PLL skin Angiocentric NHL Intestinal NHL Mucosae Bowel CD4+ lymphocytes T-ALL THYMUS Hepato-splenic γδ NHL Spleen liver Peripheral blood BM T-precursor cell Lymph node ALCL PTCL CD8+ lymphocytes LGL expansion Germinal centre AITL Follicular helper T-cells

11
NHL Non lymphoid Hemopoietic tumors Myeloma Hodgkin’s lymphoma
Trends in incidence of hematopoietic neoplasms by broad subtype category, 9 SEER registries, to *All incidence rates are age adjusted to the 2000 United States population and presented for 12 fixed 2-year time periods ( to ). Lymphoid neoplasms excepting Hodgkin lymphoma and plasma-cell neoplasms. Predominantly myeloid leukemia. Predominantly multiple myeloma. Non lymphoid Hemopoietic tumors Myeloma Hodgkin’s lymphoma
. Lymphoid neoplasms excepting Hodgkin lymphoma and plasma-cell neoplasms. Predominantly myeloid leukemia. Predominantly multiple myeloma. Non lymphoid. Hemopoietic tumors. Myeloma. Hodgkin’s. lymphoma.")
12
Morton, L. M. et al. Blood 2006;107:265-276
Incidence of lymphoid neoplasms by subtype and race, 12 SEER registries, Morton, L. M. et al. Blood 2006;107: Copyright ©2006 American Society of Hematology. Copyright restrictions may apply.

13
Causative factors Virus Bacteria EBV Burkitt’s + others HTLV1
Adult T-cell leukemia/lymphoma HCV Indolent B-cell lymphoma HHV-6 Angioimmunoblastic lymphadenopathy (variety of T-cell NHL / Hodgkin’s disease (rare) HHV-8 Body cavity Lymphoma (rare B-NHL) Bacteria Helicobacter pylori Mucosa associated lymphoid tissue (MALT) lymphoma (variety of marginal zone B-cell lymphoma) Chlamydia psittaci Orbit lymphoma
 HHV-8. Body cavity Lymphoma (rare B-NHL) Bacteria. Helicobacter pylori. Mucosa associated lymphoid tissue (MALT) lymphoma (variety of marginal zone B-cell lymphoma) Chlamydia psittaci. Orbit lymphoma.")
14
Immunodeficiency (AIDS, organ transplant recipients)
Ionizing radiation Pesticides (?) Organic solvents (?)
 Organic solvents ( )")
15
Types of non Hodgkin’s lymphoma
Clinically Indolent / clinically aggressive (slow growth= low grade lymphoma (rapid growth and invasiveness = high grade lymphoma) B-cell / T-cell (immunophenotype) Histopathologic types Pattern of growth recalling primarily involved lymph node structure. (i.e. mantle zone, germinal centre, marginal zone) Morphology and immunophenotype of the neoplastic cells; pattern of growth in the lymph node
 B-cell / T-cell. (immunophenotype) Histopathologic types. Pattern of growth recalling primarily involved lymph node structure. (i.e. mantle zone, germinal centre, marginal zone) Morphology and immunophenotype of the neoplastic cells; pattern of growth in the lymph node.")
16
Most frequent types of non Hodgkin’s lymphoma
Clinically Indolent - B-cell type Follicular lymphoma Marginal zone B-cell lymphoma Small lymphocytic lymphoma/CLL Lymphoplasmacytic lymphoma (Waldenstrom macroglobulinemia) extranodal (gastric) Splenic nodal - T-cell type Peripheral T-cell lymphoma (some) Mycosis fungoides LGL expansion (T or NK)
 extranodal (gastric) Splenic. nodal. - T-cell type. Peripheral T-cell lymphoma (some) Mycosis fungoides. LGL expansion (T or NK)")
17
Most frequent types of non Hodgkin’s lymphoma
Clinically aggressive - T-cell type - B-cell type Anaplastic large cell lymphoma (ALK+) Peripheral T-cell lymphoma (some) Sezary’s syndrome T- Prolymphocytic leukemia Lymphoblastic lymphoma Angioimmunoblastic lymphoma Diffuse large B-cell lymphoma Mantle cell lymphoma Anaplastic large cell lymphoma Burkitt’s lymphoma Lymphoblastic lymphoma
 Peripheral T-cell lymphoma (some) Sezary’s syndrome. T- Prolymphocytic leukemia. Lymphoblastic lymphoma. Angioimmunoblastic lymphoma. Diffuse large B-cell lymphoma. Mantle cell lymphoma. Anaplastic large cell lymphoma. Burkitt’s lymphoma. Lymphoblastic lymphoma.")
18
Presentation picture and diagnosis
Sistemic symptoms B symptoms in Ann Arbor staging system: unexplained fever > 38°C; weight loss >10% body weight over 6 months, night sweats = pruritus other sistemic: pruritus Tumor-related symptoms Superficial adenopathy > 1cm for more than 4 weeks (wax and wane in low-grade lymphomas) Thorax (cough, discomfort, superior vena cava syndrome) Abdomen (chronic pain, early satiety, left quadrant discomfort, jaundice, intestinal symptoms) Lymphedema Extra-nodal (depending on tissue involved)
 Thorax (cough, discomfort, superior vena cava syndrome) Abdomen (chronic pain, early satiety, left quadrant discomfort, jaundice, intestinal symptoms) Lymphedema. Extra-nodal (depending on tissue involved)")
19
Diagnosis Biopsy of any lymph node enlargement > 1 cm for > 4 weeks without an obvious explanation Imaging techniques according to symptoms No blood test is specific for NHL

20
Essentials for Diagnosis and Staging
Histopathology: histologic type allows for the identification of distinct clinical behaviour: low grade lymphoma vs high grade or indolent vs aggressive lymphoma Each entity deserve different treatment Visit with documentation of systemic (B) symptoms CT scan (thorax and abdomen) CNS study in special subtype (i.e. Burkitt’s lymphoma) or in symptomatic patients Bone biopsy (BM involvement) + Complete blood count (possible leukemic involvement) Liver +renal function, uric acid, LDH, calcium beta-2-microglobulin, electrophoresis
 symptoms. CT scan (thorax and abdomen) CNS study in special subtype (i.e. Burkitt’s lymphoma) or in symptomatic patients. Bone biopsy (BM involvement) + Complete blood count (possible leukemic involvement) Liver +renal function, uric acid, LDH, calcium beta-2-microglobulin, electrophoresis.")
22
Entità clinicopatologica
Presentazione Evoluzione istologica e clinica Linfomi indolenti Linfoma linfocitico linfoma marginale c) linfoma centrofollicolare Frequentissimo coinvolgimento ematico (LLC) Variante extranodale (MALT) Linfomi gastrici, bronchiali, gh. salivari Variante linfonodale Variante splenica (linfoma marginale splenici con o senza linfocicti villosi circolanti) Malattia frequentemente disseminata Linfoma ad alto grado (s Richter) Linfoma malt con componente ad alto grado (grandi cellule) Linfoma marginale ad alto grado Linfoma alto grado a grandi cellule (p53, p16) (avviene nel 5-10% dei casi per anno) Linfomi aggressivi linfoma del mantello linfoma B diffuso a grandi cellule linfoma a grandi cellule con sclerosi del mediastino linfomi T periferici linfoma anaplastico CD30+ Frequente iniziale coinvolgimento BM e PB Malattia spesso disseminata (sedi linofonodali ed extranodali), con splenomegalia e leucemizzazione Crescita rapida ed invasiva (compressione vasi sanguigni, nervi, bronchi, ossa) Localmente invasivo (mediastino) Svariate entità di malattia primitivo interessamento cutaneo malattia disseminata Trasformazione in linfoma mantellare blastoide Tenere presente possibile estensione tardiva al SNC Se buona risposta alla terapia (CTx + RT) remissioni durature Buona risposta alla terapia
 linfoma centrofollicolare. Frequentissimo coinvolgimento ematico (LLC) Variante extranodale (MALT) Linfomi gastrici, bronchiali, gh. salivari. Variante linfonodale. Variante splenica (linfoma marginale splenici con o senza linfocicti villosi circolanti) Malattia frequentemente disseminata. Linfoma ad alto grado (s Richter) Linfoma malt con componente ad alto grado (grandi cellule) Linfoma marginale ad alto grado. Linfoma alto grado a grandi cellule (p53, p16) (avviene nel 5-10% dei casi per anno) Linfomi aggressivi. linfoma del mantello. linfoma B diffuso a grandi cellule. linfoma a grandi cellule con sclerosi del mediastino. linfomi T periferici. linfoma anaplastico CD30+ Frequente iniziale coinvolgimento BM e PB. Malattia spesso disseminata (sedi linofonodali ed extranodali), con splenomegalia e leucemizzazione. Crescita rapida ed invasiva (compressione vasi sanguigni, nervi, bronchi, ossa) Localmente invasivo (mediastino) Svariate entità di malattia. primitivo interessamento cutaneo. malattia disseminata. Trasformazione in linfoma mantellare blastoide. Tenere presente possibile estensione tardiva al SNC. Se buona risposta alla terapia (CTx + RT) remissioni durature. Buona risposta alla terapia.")
23
Survival Patterns are Different for Indolent and Aggressive NHL
Indolent NHL (e.g. Follicular lymphoma) Probability of survival (%) Aggressive NHL (e.g. Diffuse large B-cell lymphoma) Key Point: The clinical features of the various lymphoma types were remarkably different, as were the survivals.1 Although aggressive NHL can have a more rapid mortality outcome than indolent NHL, it can be cured with treatment. In contrast, indolent NHL is rarely cured with current treatments: Relapses are common The prognosis worsens after each relapse Often becomes refractory to treatment. Using overall survival the various lymphoma types could be divided into four broad groups for prognostic purposes:1 NHLs with a 5-year survival of >70% (including follicular lymphoma and marginal zone B-cell lymphoma of MALT type) NHLs with a 5-year survival of 50% to 70% (including small lymphocytic, lymphoplasmacytoid and nodal marginal zone B-cell lymphomas) NHLs with a 5-year survival of 30% to 49% (including diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, Burkitt lymphoma) NHLs with a 5-year survival of <30% (including peripheral T-cell lymphoma, precursor T-lymphoblastic lymphoma and mantle cell lymphoma). 1. The Non-Hodgkin’s Lymphoma Classification Project. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. Blood 1997;89(11):3909–3918. Years The Non-Hodgkin’s Lymphoma Classification Project. Blood 1997;89:3909–3918
 Probability of survival (%) Aggressive NHL (e.g. Diffuse large B-cell lymphoma) Key Point: The clinical features of the various lymphoma types were remarkably different, as were the survivals.1. Although aggressive NHL can have a more rapid mortality outcome than indolent NHL, it can be cured with treatment. In contrast, indolent NHL is rarely cured with current treatments: Relapses are common. The prognosis worsens after each relapse. Often becomes refractory to treatment. Using overall survival the various lymphoma types could be divided into four broad groups for prognostic purposes:1. NHLs with a 5-year survival of >70% (including follicular lymphoma and marginal zone B-cell lymphoma of MALT type) NHLs with a 5-year survival of 50% to 70% (including small lymphocytic, lymphoplasmacytoid and nodal marginal zone B-cell lymphomas) NHLs with a 5-year survival of 30% to 49% (including diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, Burkitt lymphoma) NHLs with a 5-year survival of <30% (including peripheral T-cell lymphoma, precursor T-lymphoblastic lymphoma and mantle cell lymphoma). 1. The Non-Hodgkin’s Lymphoma Classification Project. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. Blood 1997;89(11):3909–3918. Years. The Non-Hodgkin’s Lymphoma Classification Project. Blood 1997;89:3909–3918.")
25
Therapy Depends on Age and performance status
Histogic features low-grade vs high grade, specific types (B vs T, Burkitt’s) Tumor dissemination (Staging) Is compete remission a reasonable goal?
 Tumor dissemination (Staging) Is compete remission a reasonable goal")
26
Flow chart for treatment of follicular lymphoma (indolent lymphoma)
Disseminated Stage II bulky Stage 3,4 Localized (Stage 1) (Stage 2) Consider age Consider age <60 >60 Watchful waiting Involved field radiotherapy Chemotherapy CVP, chlorambucil CVP or CHOP +/- anti CD20 Anti CD20 monoclonal antibody (?) CHOP+/- anti CD20 high dose therapy in selected cases with autologous BMT Radiactive anti CD20 in relapsed or resistant
 (Stage 2) Consider age. Consider age. <60. >60. Watchful. waiting. Involved field. radiotherapy. Chemotherapy. CVP, chlorambucil. CVP or CHOP +/- anti CD20. Anti CD20 monoclonal antibody ( ) CHOP+/- anti CD20. high dose therapy. in selected cases with. autologous BMT. Radiactive. anti CD20. in relapsed. or resistant.")
27
Flow chart for treatment of large cell lymphoma (aggressive lymphoma)
Localized Disseminated Stage II bulky Stage 3,4 (Stage 1) (Stage 2) Consider age Consider age <60 >60 CHOP -/+ RT CVP if unfit Chemotherapy +/- RT CHOP + anti CD20 Anti CD20 monoclonal antibody Aggressive regimens + anti CD20 +/- autologous BMT Radiactive anti CD20 (?) in relapsed or resistant
 (Stage 2) Consider age. Consider age. <60. >60. CHOP -/+ RT. CVP if unfit. Chemotherapy. +/- RT. CHOP + anti CD20. Anti CD20 monoclonal antibody. Aggressive regimens + anti CD20 +/- autologous BMT. Radiactive. anti CD20 ( ) in relapsed. or resistant.")
28
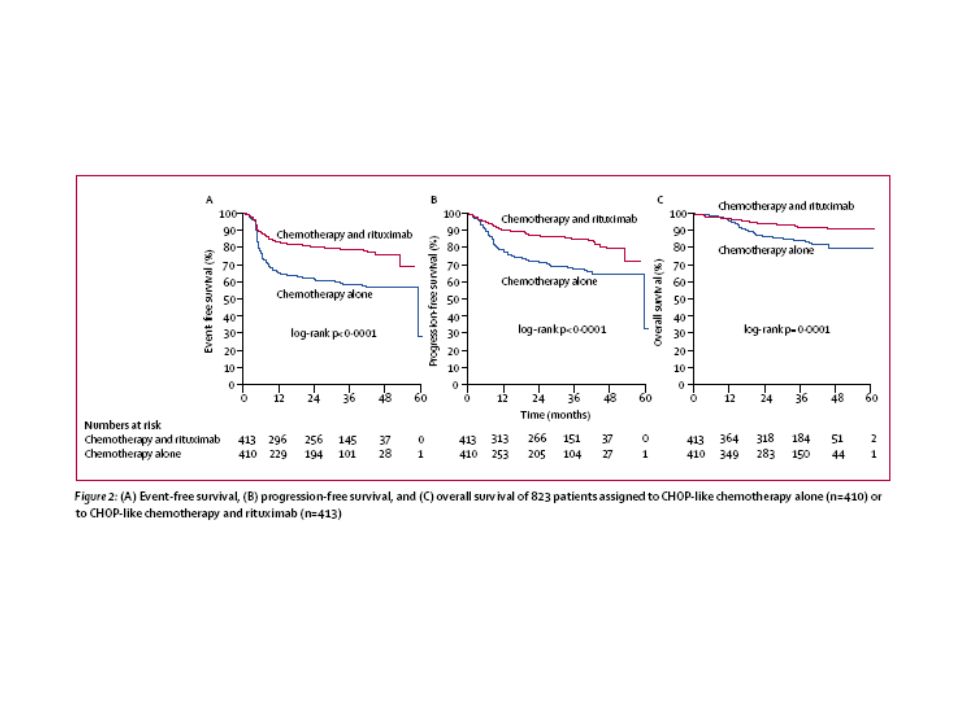
Outcome of advanced DLCL with various chemotherpy regimens

29
GELA Trial: Survival R-CHOP CHOP R-CHOP CHOP Event- Free Survival
0.5 1.0 1.5 2.0 2.5 3 Years 0.0 0.2 0.4 0.6 0.8 R-CHOP CHOP 0.5 1.0 1.5 2.0 2.5 3 Years 0.0 0.2 0.4 0.6 0.8 R-CHOP CHOP Event- Free Survival P < 0.001 Survival P = 0.007 Median follow-up of 2 years

30
Effetti tossici della chemio + radioterapia
Nausea e vomito Mucosite Tossicità ematologica Tossicità neurologica Tossicità polmonare Tossicità cardiologica Tossicità endocrina

Presentazioni simili





 is a disease state characterized by airflow limitation that is not fully reversible. The.>")



>")










