Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

2
PROFILO DELL’ANESTETICO PER INALAZIONE IDEALE
Induzione rapida e gradevole Rapida variazione della profondità dell’anestesia Soddisfacente rilasciamento muscolare Ampio margine di sicurezza Assenza di tossicità e di altri effetti collaterali alle usuali dosi terapeutiche

3
GAS ANESTETICI DI INTERESSE STORICO Non alogenati Dietiletere Etilene Ciclopropano Alogenati Cloroformio Tricloroetilene Fluoroxene GAS ANESTETICI ATTUALMENTE UTILIZZATI Non alogenati Protossido di azoto Alogenati Alotano Metossiflurano Enflurano Isoflurano Sevoflurano Desflurano

4
STRUTTURA DI ALCUNI ANESTETICI INALATORI
“vecchi” “nuovi” Protossido di azoto

6
Effects of general anaesthetics on ligand-gated ion channels
Ligand-gated ion channels are thought to be among the most relevant targets for general anesthetics, and the modulatory activity of general anaesthetics on these channels has been studied in vitro. In the figure, a dark green or pink spot indicates significant potentiation or inhibition, respectively, of agonist actions at the receptor by the anaesthetic with an EC50 or IC50 that is no greater than three times higher than the EC50 for producing immobility; a light green or light pink spot indicates little potentiation or inhibition, respectively, at concentrations that were less than three times the EC50 for immobility; an empty spot indicates no effect at any concentration tested. The data are from Refs 107,110. It should be noted that for many ligand-gated ion channels, there are multiple subtypes that might differ in their functional properties, so this presentation represents a vast oversimplification. Furthermore, equipotent anaesthetic doses were not necessarily used in the various studies summarized in this figure, making comparisons difficult and the rating within the classification scheme arbitrary. The results might depend on specific experimental conditions, and there might be conflicting reports. For example, in the case of nitrous oxide, some reports indicate a potentiation of GABAA ( -aminobutyric acid, type A) receptors111, 112, whereas other papers report no effect or only a mild effect113, 114. The figure shows that all general anaesthetics interact with multiple targets, and with the potential exceptions of isoflurane and sevoflurane, each drug has a unique pattern. At present, it is largely unknown which behavioural action of which anaesthetic is caused by which ligand-gated ion channel. AMPA, -amino-3-hydroxy-5-methyl-4-isoxazole propionic acid; 5-HT3, 5-hydroxytryptamine, type 3; nACh, acetylcholine receptor (nicotinic subtype); NMDA, N-methyl-D-aspartate receptors.
 receptors111, 112, whereas other papers report no effect or only a mild effect113, 114. The figure shows that all general anaesthetics interact with multiple targets, and with the potential exceptions of isoflurane and sevoflurane, each drug has a unique pattern. At present, it is largely unknown which behavioural action of which anaesthetic is caused by which ligand-gated ion channel. AMPA, -amino-3-hydroxy-5-methyl-4-isoxazole propionic acid; 5-HT3, 5-hydroxytryptamine, type 3; nACh, acetylcholine receptor (nicotinic subtype); NMDA, N-methyl-D-aspartate receptors.")
7
Synaptic and extrasynaptic locations of GABAA receptors
Synaptic and extrasynaptic locations of GABAA receptors. a | On binding of GABA ( -aminobutyric acid; yellow dots) to the pentameric GABAA receptor complexes, chloride flows into the postsynaptic neuron, leading to hyperpolarization. Synaptic GABAA receptors (pink) have a low potency and a high efficacy, whereas extrasynaptic GABAA receptors (blue) have a high potency and a low efficacy. GABAA receptors that contain the - and the 3 subunit, which are located extrasynaptically, have an increased sensitivity to ethanol in vitro, and it has been suggested that they might be important targets for general anaesthetics70. b | General anaesthetics prolong channel opening and increase postsynaptic inhibition. c | A pentameric GABAA receptor complex in the lipid bilayer membrane. Nature Reviews Neuroscience 5; (2004); doi: /nrn1496 MOLECULAR AND NEURONAL SUBSTRATES FOR GENERAL ANAESTHETICS
 to the pentameric GABAA receptor complexes, chloride flows into the postsynaptic neuron, leading to hyperpolarization. Synaptic GABAA receptors (pink) have a low potency and a high efficacy, whereas extrasynaptic GABAA receptors (blue) have a high potency and a low efficacy. GABAA receptors that contain the - and the 3 subunit, which are located extrasynaptically, have an increased sensitivity to ethanol in vitro, and it has been suggested that they might be important targets for general anaesthetics70. b | General anaesthetics prolong channel opening and increase postsynaptic inhibition. c | A pentameric GABAA receptor complex in the lipid bilayer membrane. Nature Reviews Neuroscience 5; (2004); doi: /nrn1496 MOLECULAR AND NEURONAL SUBSTRATES FOR GENERAL ANAESTHETICS.")
8
CARATTERISTICHE DELLA MAC
(minima concentrazione alveolare in grado di determinare assenza di reazione a uno stimolo nocicettivo nel 50% dei pazienti o degli animali) Scarsa variabilità interindividuale nell’ambito di una stessa specie Non viene modificata da sesso, altezza, peso corporeo del paziente o durata dell’anestesia Non è modificata da stimoli nocicettivi diversi Le MAC dei diversi anestetici sono additive
 Scarsa variabilità interindividuale nell’ambito di una stessa specie. Non viene modificata da sesso, altezza, peso corporeo del paziente o durata dell’anestesia. Non è modificata da stimoli nocicettivi diversi. Le MAC dei diversi anestetici sono additive.")
9
Distribuzione della gittata cardiaca e della capacità di volume per gli anestetici generali tra i principali compartimenti tessutali. I tessuti dell’organismo si possono suddividere in 4 gruppi, sulla base del loro grado di perfusione e della loro capacità di incorporare gli anestetici. Questi comprendono il gruppo dei tessuti altamente vascolarizzati (VRG), la muscolatura (MG),il tessuto adiposo (FG) e il gruppo dei tessuti scarsmente vascolarizzati (VPG). (Il contributo del VPG viene generalmente ignorato nella maggior parte dei modelli farmacocinetici di anestesia). IlVRG che comprende gli organi interni, tra cui l’encefalo, rappresenta una piccola percentuale (9%) del peso corporeo totale, ha la più bassa capacità di immagazzinare anestetici e riceve la maggior parte della gittata cardiaca (75%). L’elevata perfusione e la bassa capacità consente una rapida equilibrazione tra PVRG e Part. Inoltre il VRG fornisce il contributo più importante alla pressione parziale nel sangue misto venoso di ritorno PMVR, che è pari a (0.75 PVRG PMG PFG PVPG)
, la muscolatura (MG),il tessuto adiposo (FG) e il gruppo dei tessuti scarsmente vascolarizzati (VPG). (Il contributo del VPG viene generalmente ignorato nella maggior parte dei modelli farmacocinetici di anestesia). IlVRG che comprende gli organi interni, tra cui l’encefalo, rappresenta una piccola percentuale (9%) del peso corporeo totale, ha la più bassa capacità di immagazzinare anestetici e riceve la maggior parte della gittata cardiaca (75%). L’elevata perfusione e la bassa capacità consente una rapida equilibrazione tra PVRG e Part. Inoltre il VRG fornisce il contributo più importante alla pressione parziale nel sangue misto venoso di ritorno PMVR, che è pari a (0.75 PVRG PMG PFG PVPG).")
10
FATTORI CHE INFLUENZANO LA FARMACOCINETICA DEGLI ANESTETICI INALATORI
Concentrazione dell’anestetico nell’aria inspirata

11
FATTORI CHE INFLUENZANO LA FARMACOCINETICA DEGLI ANESTETICI INALATORI
Concentrazione dell’anestetico nell’aria inspirata Ventilazione polmonare

12
Determinanti della pressione parziale alveolare di un anestetico volatile. La pressione parziale alveolare, rappresentata dalla profondità del liquido nel recipiente, risulta dall’equilibrio tra l’apporto dovuto alla ventilazione e la rimozione per assorbimento in circolo. Un aumento dell’apporto di anestetico, dovuto a un aumento della ventilazione o a un aumento della pressione parziale dell’anestetico nell’aria inspirata, determina un aumento di PALV. Al contrario, un aumento dell’assorbimento nel circolo sanguigno, causato da un elevato valore di (sangue/gas) o da un aumento della gittata cardiaca, diminuisce PALV
 o da un aumento della gittata cardiaca, diminuisce PALV.")
13
FATTORI CHE INFLUENZANO LA FARMACOCINETICA DEGLI ANESTETICI INALATORI
Concentrazione dell’anestetico nell’aria inspirata Ventilazione polmonare Flusso ematico polmonare

14
FATTORI CHE INFLUENZANO LA FARMACOCINETICA DEGLI ANESTETICI INALATORI
Concentrazione dell’anestetico nell’aria inspirata Ventilazione polmonare Flusso ematico polmonare Solubilità dell’anestetico

16
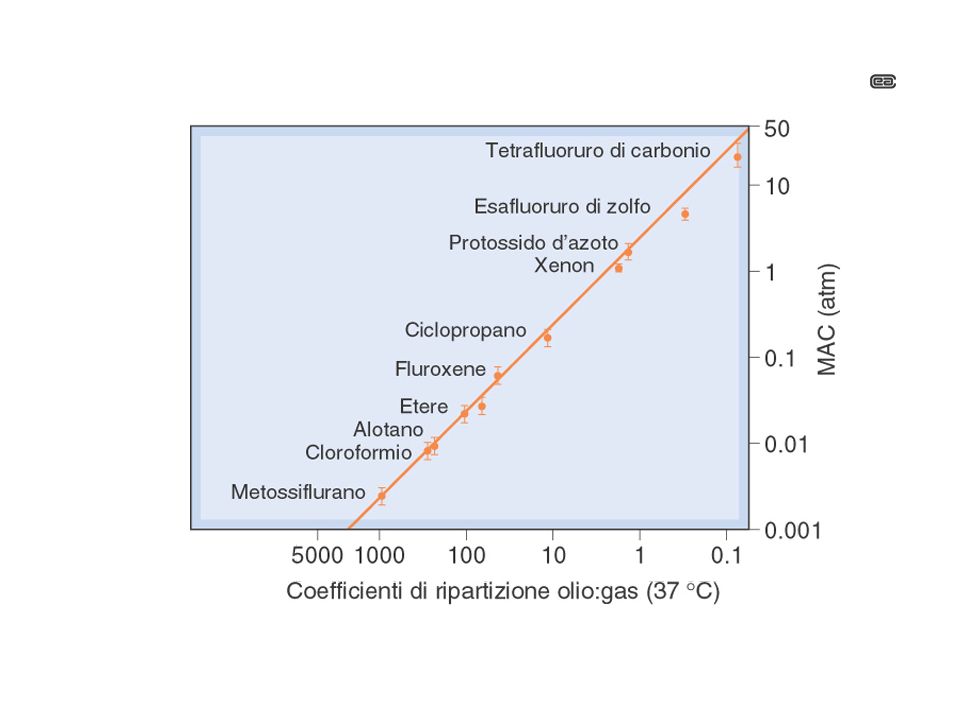
Velocità di equilibrazione degli anestetici inalatori nell’uomo

18
FATTORI CHE INFLUENZANO LA FARMACOCINETICA DEGLI ANESTETICI INALATORI
Concentrazione dell’anestetico nell’aria inspirata Ventilazione polmonare Flusso ematico polmonare Solubilità dell’anestetico Rilascio dell’anestetico dal sangue ai tessuti corporei

21
IPERTERMIA MALIGNA At a neuromuscular junction in malignant hyperthermia, a molecular gate deep inside the muscle cell stays open, releasing a dangerously large amount of calcium into the cell.

22
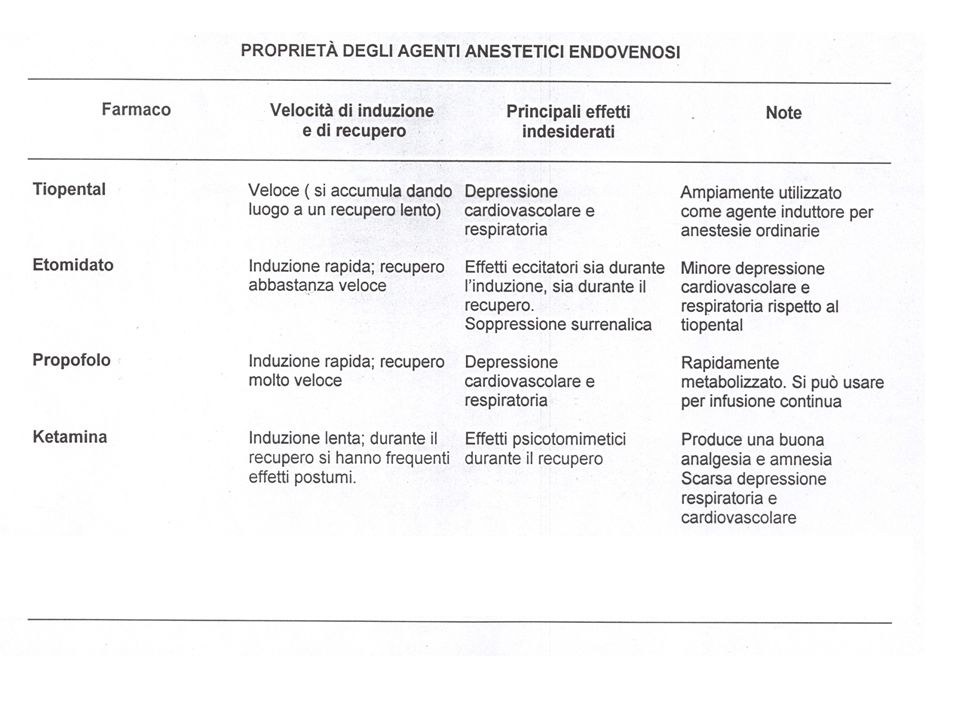
ANESTETICI ENDOVENOSI

Presentazioni simili


















>")

