Scaricare la presentazione
1
CLASSIFICAZIONE DEI FARMACI ANTI-IPERTENSIVI
IN BASE AL LORO MECCANISMO D’AZIONE PRINCIPALE Farmaci attivi sul sistema RAA

5
(+)
")
6
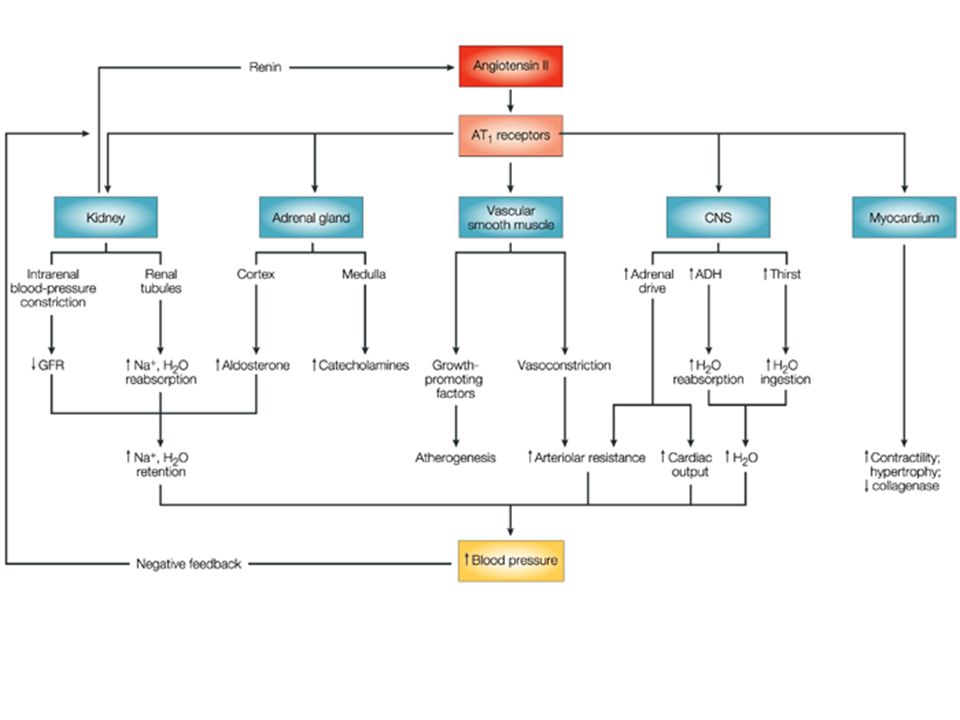
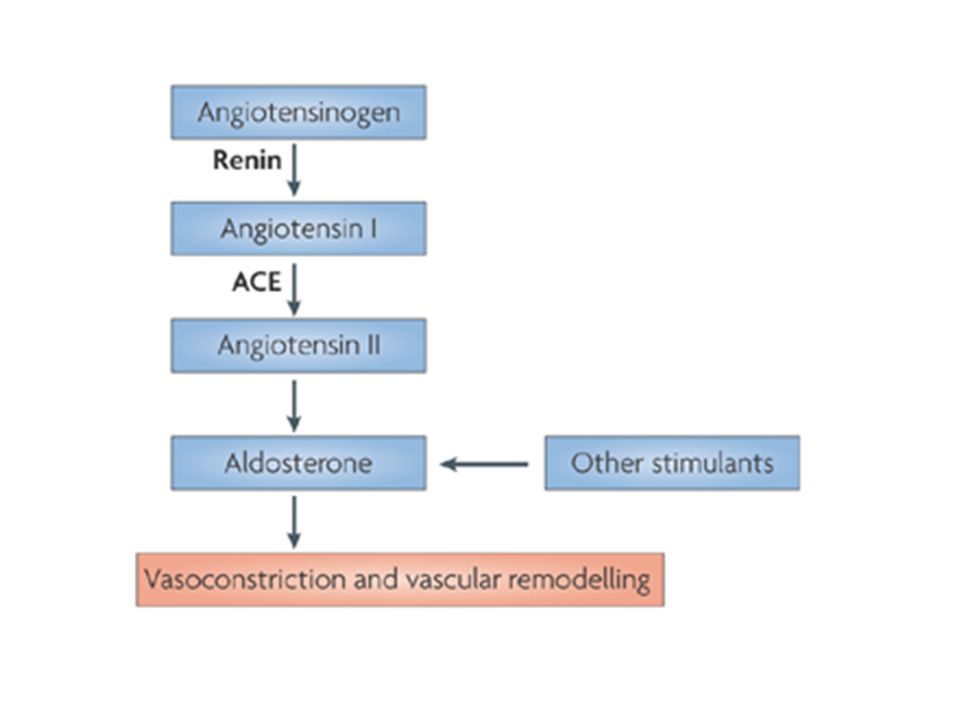
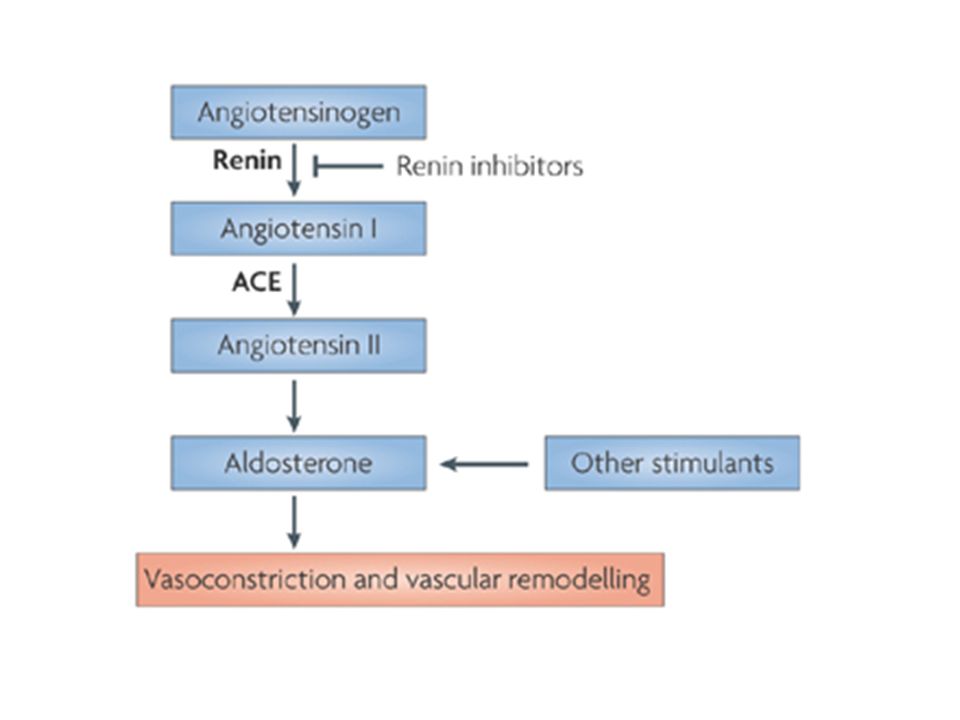
Renin — a protease that is secreted into the circulation in response to various physiological stimuli — cleaves the protein angiotensinogen to produce the inactive decapeptide angiotensin I. Cleavage of angiotensin I by angiotensin-converting enzyme (ACE) produces the active octapeptide angiotensin II (as shown, ACE also inactivates bradykinin, and there are alternative routes for the generation of angiotensin II). Angiotensin II activates the angiotensin II type 1 (AT1) receptor — a member of the G-protein-coupled-receptor superfamily — which has various effects (Box 1). Many of these effects, such as vasoconstriction and stimulation of aldosterone synthesis and release (which leads to sodium retention), tend to elevate blood pressure. Only the aldosterone-mediated effects are shown here; a comprehensive summary of the effects of AT1-receptor activation is given in Fig. 3. Angiotensin II also activates the AT2 receptor, the effects of which (Box 1) are less well understood, but which could antagonize many of the effects of activation of the AT1 receptor. Various points shown in the renin–angiotensin–aldosterone cascade have been the targets for pharmacological intervention, and inhibitors of ACE, angiotensin-receptor blockers and aldosterone-receptor antagonists are in clinical use at present. ACTH, adrenocorticotropic hormone; BK receptor, bradykinin receptor.
 produces the active octapeptide angiotensin II (as shown, ACE also inactivates bradykinin, and there are alternative routes for the generation of angiotensin II). Angiotensin II activates the angiotensin II type 1 (AT1) receptor — a member of the G-protein-coupled-receptor superfamily — which has various effects (Box 1). Many of these effects, such as vasoconstriction and stimulation of aldosterone synthesis and release (which leads to sodium retention), tend to elevate blood pressure. Only the aldosterone-mediated effects are shown here; a comprehensive summary of the effects of AT1-receptor activation is given in Fig. 3. Angiotensin II also activates the AT2 receptor, the effects of which (Box 1) are less well understood, but which could antagonize many of the effects of activation of the AT1 receptor. Various points shown in the renin–angiotensin–aldosterone cascade have been the targets for pharmacological intervention, and inhibitors of ACE, angiotensin-receptor blockers and aldosterone-receptor antagonists are in clinical use at present. ACTH, adrenocorticotropic hormone; BK receptor, bradykinin receptor..")
8
Effetti mediati dal recettore AT1
Vasocostrizione (preferenzialmente distretti coronarico, renale, cerebrale) ritenzione di sodio (angiotensina, produzione di aldosterone ) ritenzione idrica (liberazione di vasopressina) soppressione della liberazione di renina (feedback negativo) ipertrofia dei miociti e della muscolatura liscia induzione di fibrosi vascolare e miocardica effetto inotropo positivo (cardiomiociti) effetto cronotropo/aritmogenico (cardiomiociti) stimolazione dell’inibitore dell’attivatore del plasminogeno stimolazione della formazione di superossido attivazione del sistema nervoso simpatico aumento della secrezione di endotelina
 ritenzione di sodio (angiotensina, produzione di aldosterone ) ritenzione idrica (liberazione di vasopressina) soppressione della liberazione di renina (feedback negativo) ipertrofia dei miociti e della muscolatura liscia. induzione di fibrosi vascolare e miocardica. effetto inotropo positivo (cardiomiociti) effetto cronotropo/aritmogenico (cardiomiociti) stimolazione dell’inibitore dell’attivatore del plasminogeno. stimolazione della formazione di superossido. attivazione del sistema nervoso simpatico. aumento della secrezione di endotelina.")
9
Effetti mediati dal recettore AT2
effetto antiproliferativo,/inibizione della crescita cellulare differenziamento tessutale riparazione tessutale apoptosi vasodilatazione sviluppo del rene e del tratto urinario protezione nei confronti dell’ischemia

13
ACE INIBITORI

16
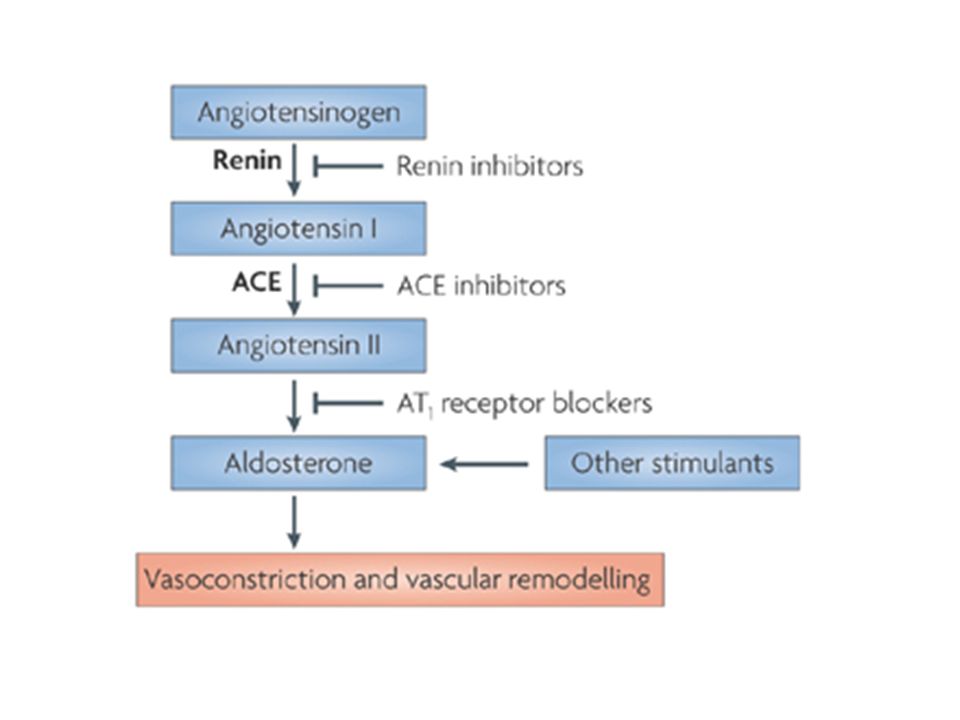
Renin — a protease that is secreted into the circulation in response to various physiological stimuli — cleaves the protein angiotensinogen to produce the inactive decapeptide angiotensin I. Cleavage of angiotensin I by angiotensin-converting enzyme (ACE) produces the active octapeptide angiotensin II (as shown, ACE also inactivates bradykinin, and there are alternative routes for the generation of angiotensin II). Angiotensin II activates the angiotensin II type 1 (AT1) receptor — a member of the G-protein-coupled-receptor superfamily — which has various effects (Box 1). Many of these effects, such as vasoconstriction and stimulation of aldosterone synthesis and release (which leads to sodium retention), tend to elevate blood pressure. Only the aldosterone-mediated effects are shown here; a comprehensive summary of the effects of AT1-receptor activation is given in Fig. 3. Angiotensin II also activates the AT2 receptor, the effects of which (Box 1) are less well understood, but which could antagonize many of the effects of activation of the AT1 receptor. Various points shown in the renin–angiotensin–aldosterone cascade have been the targets for pharmacological intervention, and inhibitors of ACE, angiotensin-receptor blockers and aldosterone-receptor antagonists are in clinical use at present. ACTH, adrenocorticotropic hormone; BK receptor, bradykinin receptor.
 produces the active octapeptide angiotensin II (as shown, ACE also inactivates bradykinin, and there are alternative routes for the generation of angiotensin II). Angiotensin II activates the angiotensin II type 1 (AT1) receptor — a member of the G-protein-coupled-receptor superfamily — which has various effects (Box 1). Many of these effects, such as vasoconstriction and stimulation of aldosterone synthesis and release (which leads to sodium retention), tend to elevate blood pressure. Only the aldosterone-mediated effects are shown here; a comprehensive summary of the effects of AT1-receptor activation is given in Fig. 3. Angiotensin II also activates the AT2 receptor, the effects of which (Box 1) are less well understood, but which could antagonize many of the effects of activation of the AT1 receptor. Various points shown in the renin–angiotensin–aldosterone cascade have been the targets for pharmacological intervention, and inhibitors of ACE, angiotensin-receptor blockers and aldosterone-receptor antagonists are in clinical use at present. ACTH, adrenocorticotropic hormone; BK receptor, bradykinin receptor..")
18
Signal transduction by angiotensin AT1 receptors
Signal transduction by angiotensin AT1 receptors. The AT1 receptor is a member of the G-protein-coupled-receptor superfamily. The amino terminus and other parts of the protein close to the surface (red) participate in binding angiotensin II, whereas deeper amino-acid residues (blue) contribute to the binding of the 'sartan' family of angiotensin-receptor blockers. The carboxyl terminus and the three intracellular loops interact with G proteins, which — when activated by binding of angiotensin II — stimulate phospholipase C (PLC) and open calcium channels. PLC cleaves phosphoinositide (PIP2) to inositol trisphosphate (IP3), which releases calcium from the endoplasmic reticulum, and to diacylglycerol (DAG). DAG and calcium activate enzymes, such as protein kinase C, which phosphorylate proteins and affect cellular functions
 participate in binding angiotensin II, whereas deeper amino-acid residues (blue) contribute to the binding of the sartan family of angiotensin-receptor blockers. The carboxyl terminus and the three intracellular loops interact with G proteins, which — when activated by binding of angiotensin II — stimulate phospholipase C (PLC) and open calcium channels. PLC cleaves phosphoinositide (PIP2) to inositol trisphosphate (IP3), which releases calcium from the endoplasmic reticulum, and to diacylglycerol (DAG). DAG and calcium activate enzymes, such as protein kinase C, which phosphorylate proteins and affect cellular functions.")
19
ANTAGONISTI DEL RECETTORE AT1

21
FARMACI ATTIVI SUL SISTEMA RENINA-ANGIOTENSINA-ALDOSTERONE
Inibitori della renina Inibitori dell’Angiotensin-converting enzyme (ACE) Antagonisti del recettore AT1 ACE/NEP inibitori Antagonisti dell’aldosterone Eplerenone
 Antagonisti del recettore AT1. ACE/NEP inibitori. Antagonisti dell’aldosterone. Eplerenone.")
22
FARMACI ATTIVI SUL SISTEMA RENINA-ANGIOTENSINA-ALDOSTERONE
Inibitori della renina Inibitori dell’Angiotensin-converting enzyme (ACE) Antagonisti del recettore AT1
 Antagonisti del recettore AT1.")
23
FARMACI ATTIVI SUL SISTEMA RENINA-ANGIOTENSINA-ALDOSTERONE
Inibitori dell’Angiotensin Converting Enzyme e delle Endopeptidasi Neutre (ACE/NEP inibitori)
")
24
Mechanism of action of vasopeptidase inhibitors
Mechanism of action of vasopeptidase inhibitors. Synergistic effects resulting from combined inhibition of angiotensin-converting enzyme (ACE) and neutral endopeptidase (NEP) are due to similar mechanisms — blockade of angiotensin (AT) synthesis and concomitant potentiation of natriuretic peptides and bradykinin (BK), leading to vasodilatation, natriuresis and improvement in myocardial function. L-Arg, L-arginine; ECE, endothelin-converting enzyme; eNOS, endothelial nitric-oxide synthase; ET, endothelin; pGC, particulate guanylyl cyclase; sGC, soluble guanylyl cyclase; Thr, thrombin.
 and neutral endopeptidase (NEP) are due to similar mechanisms — blockade of angiotensin (AT) synthesis and concomitant potentiation of natriuretic peptides and bradykinin (BK), leading to vasodilatation, natriuresis and improvement in myocardial function. L-Arg, L-arginine; ECE, endothelin-converting enzyme; eNOS, endothelial nitric-oxide synthase; ET, endothelin; pGC, particulate guanylyl cyclase; sGC, soluble guanylyl cyclase; Thr, thrombin.")
25
CLASSIFICAZIONE DEI FARMACI ANTI-IPERTENSIVI
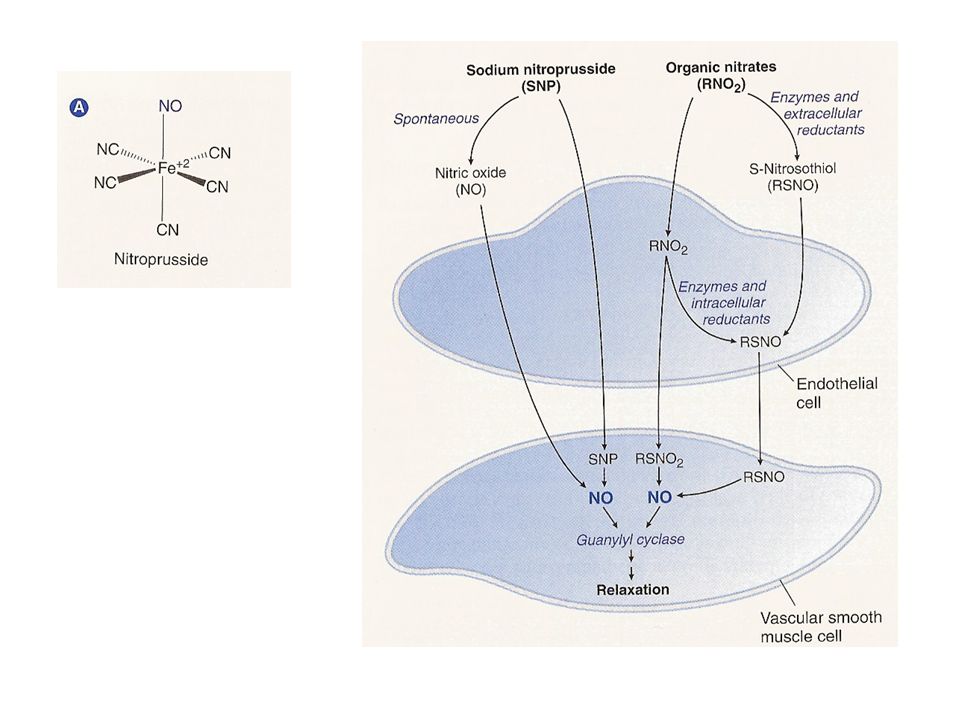
IN BASE AL LORO MECCANISMO D’AZIONE PRINCIPALE Farmaci attivi sul sistema RAA Vasodilatatori diretti nitroprussiato sodico (arterie e vene)
")
30
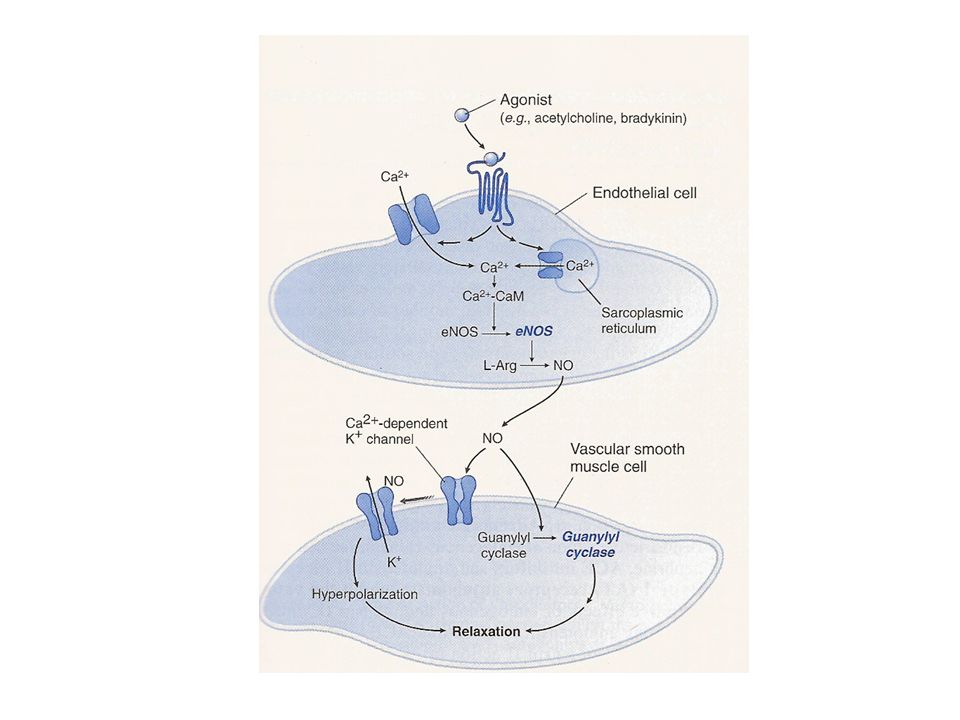
L-arginine is converted in the endothelium monolayer by the endothelial nitric oxide synthase (eNOS) to NO, which diffuses into both the vessel lumen and the vessel wall, thereby activating soluble guanylate cyclase (sGC). Haem-dependent sGC stimulators and haem-independent sGC activators increase the cellular cGMP concentration via the direct activation of sGC, which results in both vasorelaxation and inhibition of platelet aggregation. In contrast, organic nitrates require bioconversion to release NO, which is not implemented in platelets, leading to poor anti-aggregatory effect.

31
Rappresentazione schematica del metabolismo dell’arginina
Rappresentazione schematica del metabolismo dell’arginina. La sintesi di NO avviene per trasformazione enzimatica dell’arginina operata dalla NO sintasi con produzione finale di citrullina

32
RUOLO DEL NO ENDOGENO SISTEMA CARDIOVASCOLARE
Controllo della pressione sanguigna e del flusso ematico regionale endotelio/m. liscia vascolare Limitazione dell’adesione/aggregazione piastrine MECCANISMI DI DIFESA Difesa nei cfr. di virus, batteri, funghi, protozoi e parassiti macrofagi, neutrofili, leucociti SISTEMA NERVOSO Neurotrasmissione, potenziamento a lungo termine; plasticità (memoria appetito, nocicezione) centrale Neurotrasmissione (p.e. svuotamento gastrico; erezione del pene) periferico
 centrale. Neurotrasmissione (p.e. svuotamento gastrico; erezione del pene) periferico.")
33
MECCANISMO D’AZIONE DEL NO ENDOGENO
Interazione con il gruppo eme della guanilato ciclasi Interazione con il gruppo eme di altre proteine (citocromo c ossidasi) Interazione con l’anione superossido Nitrosazione di proteine, lipidi e acidi nucleici
 Interazione con l’anione superossido. Nitrosazione di proteine, lipidi e acidi nucleici.")
34
Nitric oxide (NO) is synthesized enzymatically from the amino acid L-arginine by three isoforms of NO synthase (NOS), including endothelial NOS (eNOS). Minute amounts of endogenously produced or exogenously administered NO activate soluble guanylate cyclase (sGC), which converts GTP to cyclic GMP, mediating various physiological and tissue protective effects. Degradation of cGMP to GMP is catalysed by several phosphodiesterase (PDE) families. Excessive amounts of NO produced under pathological conditions associated with increased inflammation and oxidative stress react avidly with superoxide anion ( O2-), to form peroxynitrite (ONOO-). Peroxynitrite, in concert with other oxidants, induces cell damage via lipid peroxidation, inactivation of enzymes and other proteins by oxidation and nitration, and activation of matrix metalloproteinases (MMP) and the nuclear enzyme poly(ADP-ribose) polymerase (PARP), which ultimately leads to cellular dysfunction and death. NO–sGC–cGMP signalling can be compromised either by reducing the bioavailability of NO (for example, via chemical interaction of NO with O2-) or by altering the redox state of sGC itself (for example, through oxidative stress or the action of peroxynitrite), thereby making it unresponsive to endogenous NO and NO-releasing drugs. Two novel drug classes seem to be able to overcome these obstacles: sGC stimulators (stimulate sGC directly and enhance sensitivity of the reduced enzyme to low levels of bioavailable NO) and sGC activators (activate the NO-unresponsive, haem-oxidized or haem-free enzyme). Other potential therapeutic approaches that modulate this pathway are also shown (dotted lines).
, which converts GTP to cyclic GMP, mediating various physiological and tissue protective effects. Degradation of cGMP to GMP is catalysed by several phosphodiesterase (PDE) families. Excessive amounts of NO produced under pathological conditions associated with increased inflammation and oxidative stress react avidly with superoxide anion ( O2-), to form peroxynitrite (ONOO-). Peroxynitrite, in concert with other oxidants, induces cell damage via lipid peroxidation, inactivation of enzymes and other proteins by oxidation and nitration, and activation of matrix metalloproteinases (MMP) and the nuclear enzyme poly(ADP-ribose) polymerase (PARP), which ultimately leads to cellular dysfunction and death. NO–sGC–cGMP signalling can be compromised either by reducing the bioavailability of NO (for example, via chemical interaction of NO with O2-) or by altering the redox state of sGC itself (for example, through oxidative stress or the action of peroxynitrite), thereby making it unresponsive to endogenous NO and NO-releasing drugs. Two novel drug classes seem to be able to overcome these obstacles: sGC stimulators (stimulate sGC directly and enhance sensitivity of the reduced enzyme to low levels of bioavailable NO) and sGC activators (activate the NO-unresponsive, haem-oxidized or haem-free enzyme). Other potential therapeutic approaches that modulate this pathway are also shown (dotted lines)..")
35
The figure illustrates the intracellular redox equilibrium of the two sGC redox states, nitric oxide (NO)-sensitive reduced (blue) and NO-insensitive oxidized sGC (pink). The equilibrium can be shifted by reactive oxygen species to the oxidized (ferric) state and by postulated but yet undiscovered reductases to the reduced (ferrous) form. Disequilibrium towards the oxidized NO-unresponsive enzyme exists under various pathophysiological conditions associated with oxidative stress. Haem-independent sGC activators such as BAY and HMR-1766 activate the oxidized or haem-deficient form. By contrast, haem-dependent stimulators YC-1, BAY , BAY , A and CFM-1571 can activate the reduced sGC and show a strong synergism when combined with NO.
 state and by postulated but yet undiscovered reductases to the reduced (ferrous) form. Disequilibrium towards the oxidized NO-unresponsive enzyme exists under various pathophysiological conditions associated with oxidative stress. Haem-independent sGC activators such as BAY and HMR-1766 activate the oxidized or haem-deficient form. By contrast, haem-dependent stimulators YC-1, BAY , BAY , A and CFM-1571 can activate the reduced sGC and show a strong synergism when combined with NO..")
36
CLASSIFICAZIONE DEI FARMACI ANTI-IPERTENSIVI
IN BASE AL LORO MECCANISMO D’AZIONE PRINCIPALE Farmaci attivi sul sistema RAA Vasodilatatori diretti nitroprussiato sodico (arterie e vene) Inibitori delle fosfodiesterasi
 Inibitori delle fosfodiesterasi.")
37
Sildenafil Sexual stimulation causes the release of nitric oxide (NO) from nerves and endothelial cells in the penis. NO activates guanylyl cyclase, which converts GTP into cyclic GMP. This second messenger mediates smooth-muscle relaxation in the penis, and the resulting increased blood flow into the penis leads to an erection. PDE5, which is the major PDE subtype in penile tissue, degrades cGMP, and so inhibiting PDE5 allows cGMP to remain active as a second messenger, thereby promoting erection
 from nerves and endothelial cells in the penis. NO activates guanylyl cyclase, which converts GTP into cyclic GMP. This second messenger mediates smooth-muscle relaxation in the penis, and the resulting increased blood flow into the penis leads to an erection. PDE5, which is the major PDE subtype in penile tissue, degrades cGMP, and so inhibiting PDE5 allows cGMP to remain active as a second messenger, thereby promoting erection.")
38
CLASSIFICAZIONE DEI FARMACI ANTI-IPERTENSIVI
IN BASE AL LORO MECCANISMO D’AZIONE PRINCIPALE Farmaci attivi sul sistema RAA Vasodilatatori diretti nitroprussiato sodico (arterie e vene) Inibitori delle fosfodiesterasi potassium channel openers (arterie)
 Inibitori delle fosfodiesterasi. potassium channel openers (arterie)")
39
SUR2 SUR2 SUR2 SUR2

41
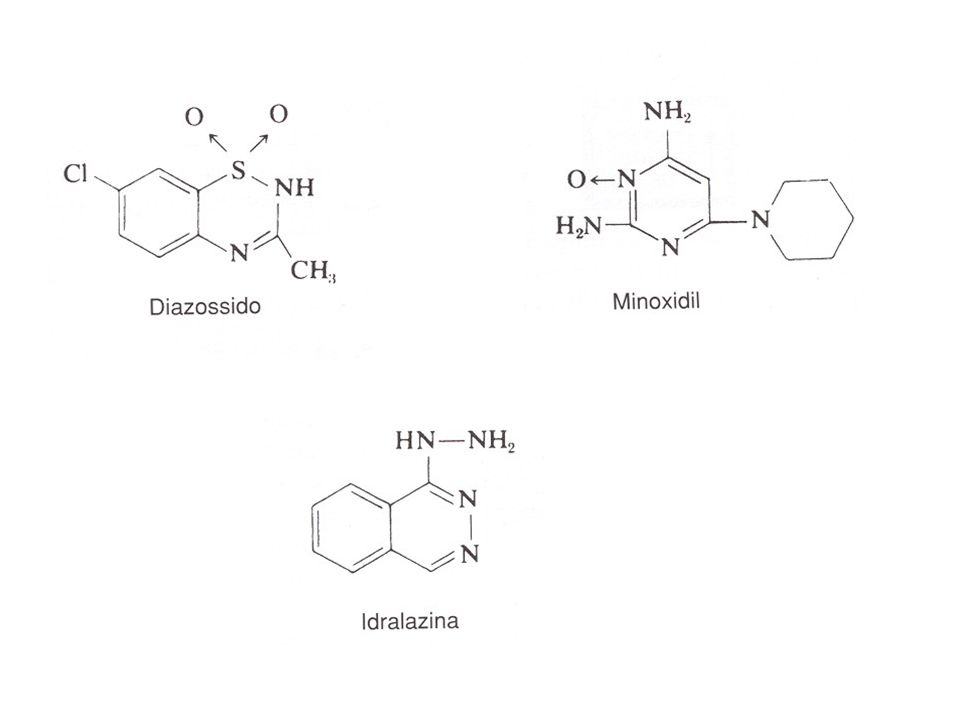
MINOXIDIL

43
CLASSIFICAZIONE DEI FARMACI ANTI-IPERTENSIVI
IN BASE AL LORO MECCANISMO D’AZIONE PRINCIPALE Farmaci attivi sul sistema RAA Vasodilatatori diretti nitroprussiato sodico (arterie e vene) Inibitori delle fosfodiesterasi potassium channel openers (arterie) bloccanti dei canali del calcio
 Inibitori delle fosfodiesterasi. potassium channel openers (arterie) bloccanti dei canali del calcio.")
44
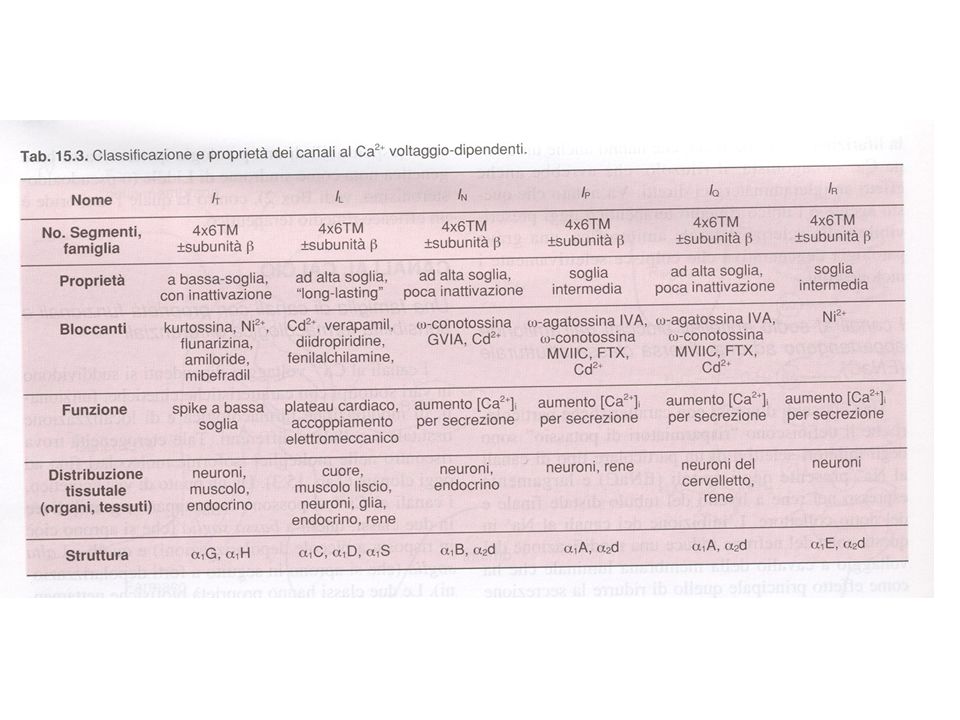
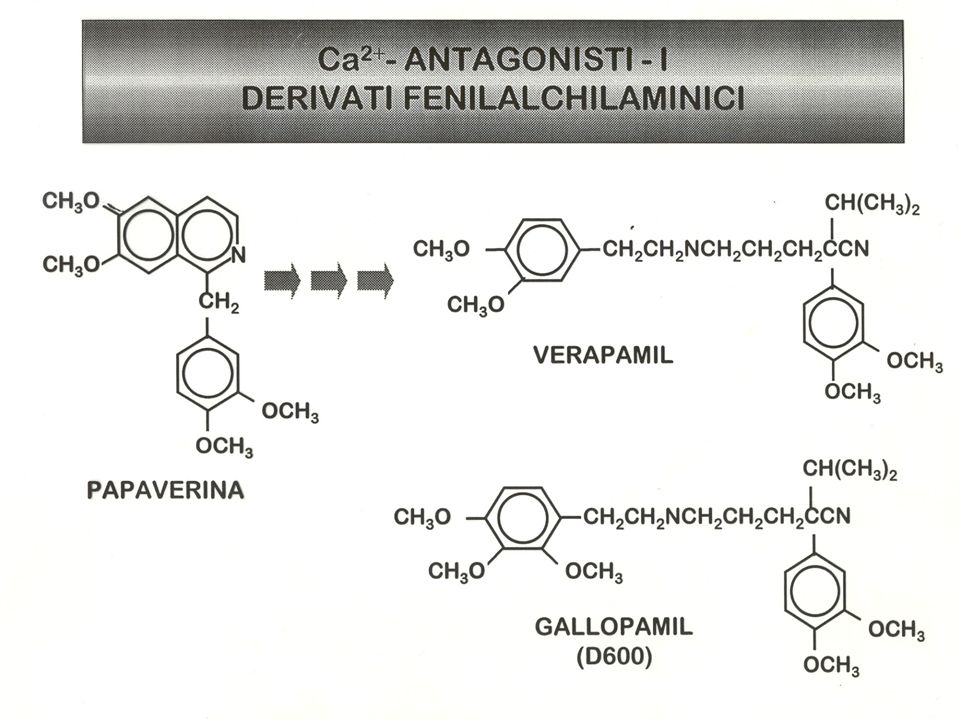
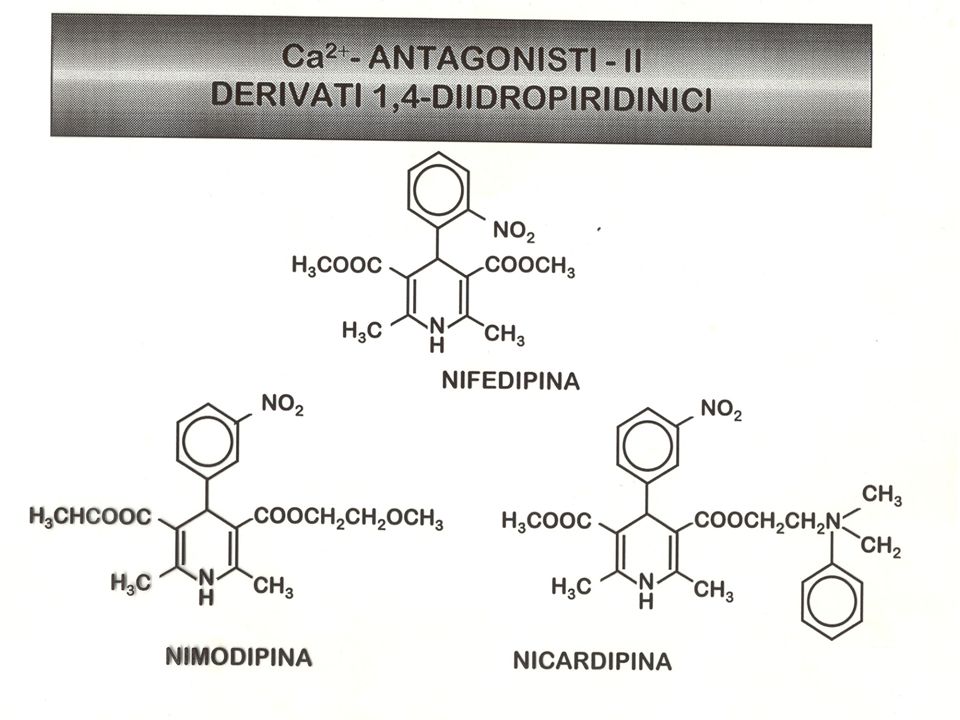
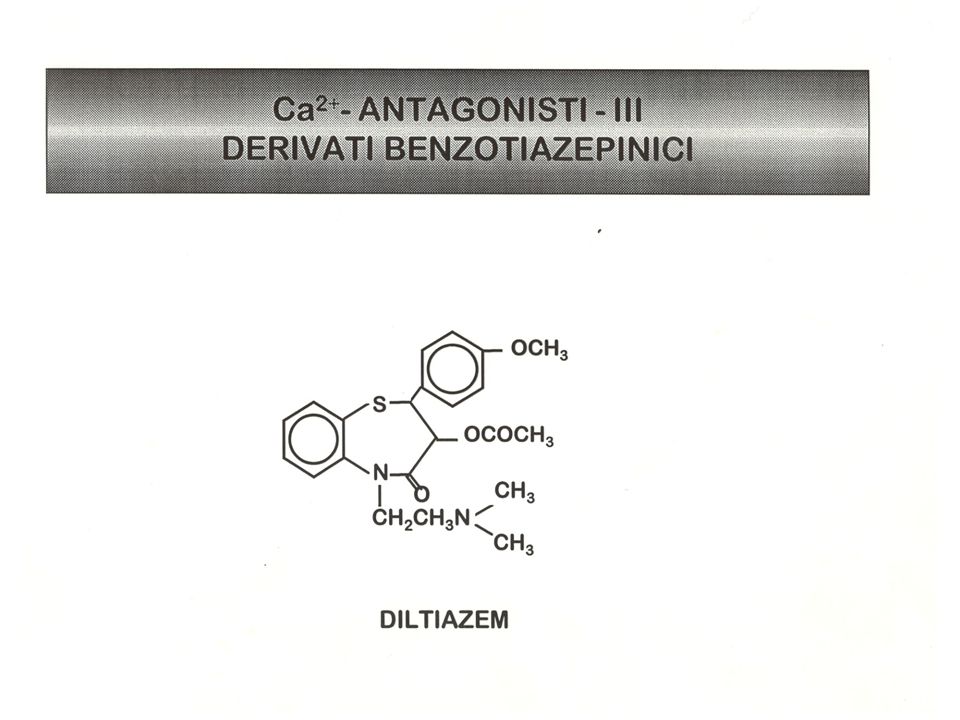
Calcio antagonisti

51
- - - + + 1,4-diidropiridine benzotiazepine fenilalchilamine poro per
il passaggio del Ca2+ -

56
CLASSIFICAZIONE DEI FARMACI ANTI-IPERTENSIVI
IN BASE AL LORO MECCANISMO D’AZIONE PRINCIPALE Farmaci attivi sul sistema RAA Vasodilatatori diretti nitroprussiato sodico (arterie e vene) Inibitori delle fosfodiesterasi potassium channel openers (arterie) bloccanti dei canali del calcio Simpaticolitici Ad azione centrale (-metildopa, clonidina) Bloccanti gangliari (trimetafano) Bloccanti del neurone adrenergico (reserpina, guanetidina) Antagonisti -adrenergici (propranololo, metoprololo) Antagonisti -adrenergici (fenossibenzamina, fentolamina, prazosina) Antagonisti adrenergici misti (labetalolo)
 Inibitori delle fosfodiesterasi. potassium channel openers (arterie) bloccanti dei canali del calcio. Simpaticolitici. Ad azione centrale (-metildopa, clonidina) Bloccanti gangliari (trimetafano) Bloccanti del neurone adrenergico (reserpina, guanetidina) Antagonisti -adrenergici (propranololo, metoprololo) Antagonisti -adrenergici (fenossibenzamina, fentolamina, prazosina) Antagonisti adrenergici misti (labetalolo)")
58
Pressione sistemica Pressione sistemica Attività del sistema nervoso
simpatico Stimolazione cardiaca Gittata cardiaca Rilassamento della muscolatura liscia vascolare Resistenze vascolari periferiche Pressione sistemica Resistenze vascolari periferiche Pressione sistemica Renina plasmatica Angiotensina circolante Meccanismi neuroendocrini attivati in seguito a una diminuzione della pressione sistemica causata da vasodilatatori. L’evento finale è n aumento della pressione sistemica che pertanto compromette l’efficacia della terapiacon vasodilatatori. Tale efficacia può essere preservata attraverso la co-somministrazione di beta bloccanti e di un diuretico. Aldosterone Escrezione di sodio Volume dei fluidi

59
β-BLOCCANTE β-BLOCCANTE DIURETICO Pressione sistemica Pressione
Attività del sistema nervoso simpatico Stimolazione cardiaca Gittata cardiaca Rilassamento della muscolatura liscia vascolare Resistenze vascolari periferiche β-BLOCCANTE Pressione sistemica Resistenze vascolari periferiche Pressione sistemica Renina plasmatica Angiotensina circolante Meccanismi neuroendocrini attivati in seguito a una diminuzione della pressione sistemica causata da vasodilatatori. L’evento finale è n aumento della pressione sistemica che pertanto compromette l’efficacia della terapiacon vasodilatatori. Tale efficacia può essere preservata attraverso la co-somministrazione di beta bloccanti e di un diuretico. DIURETICO Aldosterone Escrezione di sodio Volume dei fluidi

60
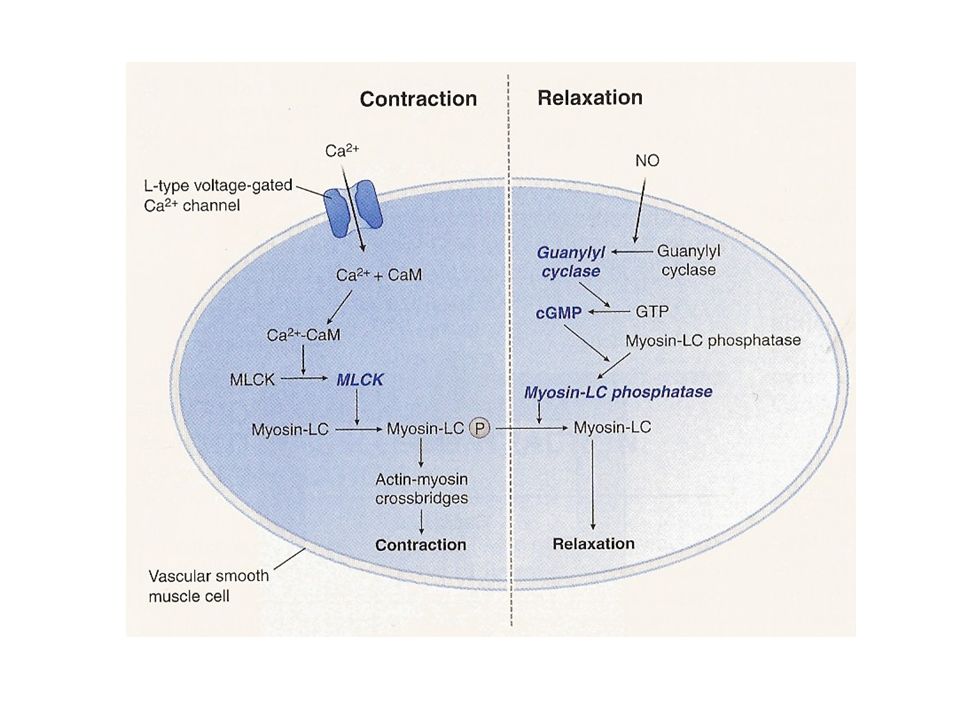
Sites of action of vasodilators
Sites of action of vasodilators. Vasodilators act at several sites in the vascular smooth muscle cell. Left panel: Ca2+ channel blockers and K+ channel openers inhibit the entry of Ca2+ into vascular smooth muscle by decreasing activation of L-type Ca2+ channels. ACE inhibitors, AT1 antagonists, alpha1 antagonists and endothelin receptor (ETa, ETb) antagonists all decrease intracellular Ca2+ signaling. The decreased cytosolic Ca2+ results in less vascular smooth muscle cell contraction and hence in relaxation. Right panel: ACE inhibitors inhibit Kininase II, leading to increased level of bradykinin. Nitrates release NO. Sildenafil inhibits phosphodiesterase (PDE). These agents all cause an increase in cGMP, an effect that promotes vascular smooth muscle relaxation.
 antagonists all decrease intracellular Ca2+ signaling. The decreased cytosolic Ca2+ results in less vascular smooth muscle cell contraction and hence in relaxation. Right panel: ACE inhibitors inhibit Kininase II, leading to increased level of bradykinin. Nitrates release NO. Sildenafil inhibits phosphodiesterase (PDE). These agents all cause an increase in cGMP, an effect that promotes vascular smooth muscle relaxation.")
61
Regulation of ET-1 synthesis, pathway of ET generation and ET-receptor-mediated actions on smooth muscle cells. Endothelin-1 (ET-1) synthesis is regulated by many factors; stimulators are highlighted in green, and inhibitors are highlighted in red. The product of ET1 transcription is prepro-ET-1, which is cleaved by a neutral endopeptidase to form the active precursor pro-ET-1 or big ET-1. Big ET-1 is converted to the mature peptide by the metalloproteinase endothelin-converting enzyme-1 (ECE-1). Two ET receptors have been identified in the vasculature: ET type-A receptors (ETA) reside in vascular smooth muscle cells and mediate vasoconstriction and cell proliferation, whereas ETB receptors reside on endothelial cells and are mainly vasodilatory through NO (which in turn can mediate the anti-apoptotic effects of ET-1), and regulate the synthesis of ET-1. ETB receptors on smooth muscle cells can elicit vessel contraction. CsA, cyclosporin A; EGF, epidermal growth factor; HGF, hepatocyte growth factor; IL-1, interleukin-1; LDL, low-density lipoprotein; VEGF, vascular endothelial growth factor.
 synthesis is regulated by many factors; stimulators are highlighted in green, and inhibitors are highlighted in red. The product of ET1 transcription is prepro-ET-1, which is cleaved by a neutral endopeptidase to form the active precursor pro-ET-1 or big ET-1. Big ET-1 is converted to the mature peptide by the metalloproteinase endothelin-converting enzyme-1 (ECE-1). Two ET receptors have been identified in the vasculature: ET type-A receptors (ETA) reside in vascular smooth muscle cells and mediate vasoconstriction and cell proliferation, whereas ETB receptors reside on endothelial cells and are mainly vasodilatory through NO (which in turn can mediate the anti-apoptotic effects of ET-1), and regulate the synthesis of ET-1. ETB receptors on smooth muscle cells can elicit vessel contraction. CsA, cyclosporin A; EGF, epidermal growth factor; HGF, hepatocyte growth factor; IL-1, interleukin-1; LDL, low-density lipoprotein; VEGF, vascular endothelial growth factor..")
62
RISPOSTA FARMACOLOGICA
Surrene Intestino Rene Cervello M. liscia Endotelio Vasi TESSUTI PEPTIDI RECETTORI ET3 ET2 ET1 ETB ETA +++ + ++ ++++ ++ + +++ RISPOSTA FARMACOLOGICA AFFINITÀ RECETTORE Vasocostrizione Broncocostrizione Stimolazione secrezione aldosterone ET1 = ET2 > ET3 ETA Vasodilatazione Inibizione aggregazione piastrinica ET1 = ET2 = ET3 ETB

63
ANTAGONISTI DEL RECETTORE ETA


















>")











