Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Salute e sistemi sanitari orientati al territorio
Gavino Maciocco Dipartimento di Sanità Pubblica Università di Firenze XXIII Congresso Nazionale CSeRMEG Costermano del Garda 29 ottobre 2011

2
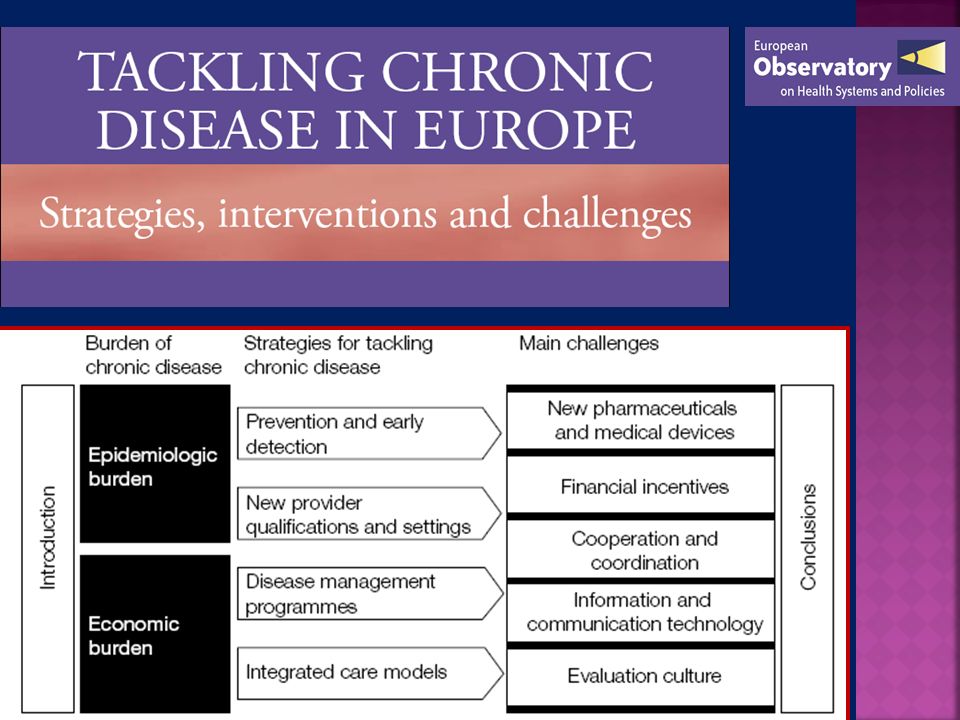
While the global disease burden has been shifting towards chronic conditions, health systems have not evolved to meet this changing demand. Care is fragmented, focused on acute and emergent symptoms, and often provided without the benefit of complete medical information. (WHO, 2003)
.")
4
Distribuzione % delle cause di morte in Paesi con differenti livelli di reddito

5
Distribuzione % delle cause di morte in Paesi con differenti livelli di reddito

7
LA STORIA NATURALE DELLE MALATTIE CRONICHE

9
LA STORIA NATURALE DELLE MALATTIE CRONICHE
SECONDO DUE DIFFERENTI SCENARI

10
SCENARIO DI MERCATO

12
BIG MAC ALLA SALSA DI STATINE ?

14
SIAMO A RISCHIO DI DIVENTARE A RISCHIO ?
4 September 2010

15
BMJ International classification of non-diseases (ICND) (N= 200)
Baldness Irritable bowel syndrome Osteoporosis Menopause Cellulite Testosterone deficiency Ageing Pregnancy Erectile dysfunction Social fobia Chronic fatigue syndrome Seasonal affective disorders Unhappiness Anxiety about penis size Loneliness Tennis elbow Chinese restaurant syndr. etc., etc. 15 Source: BMJ

16
BMJ 13,April 2002 “ SI PUÒ FARE UN SACCO DI SOLDI SE SI ARRIVA A CONVINCERE I SANI CHE IN REALTÀ SONO DEGLI AMMALATI” R. Moynihan et al. BMJ 2002 Too Much Medicine?

18
USA Europa Malattie cardiache 21,8 11,4 Diabete 16,4 10,9
Tabella 3. Prevalenza di condizioni morbose e fattori di rischio nei soggetti di 50 aa. e oltre. USA e 10 paesi europei*, 2004 USA EUROPA USA/Europa differenza Malattie cardiache 21,8 11,4 10,4 Ipertensione 50,0 32,9 17,1 Ipercolesterolemia 21,7 19,6 2,1 Ictus/Malattie cerebrovascolari 5,3 3,5 1,8 Diabete 16,4 10,9 5.5 Malattie polmonari croniche 9,7 5,4 4,3 Asma 4,4 0,1 Artrite 53,8 21,3 32,5 Osteoporosi 5,0 7,8 -2,8 Cancro 12,2 6,8 Obesità 33,1 16,0 Fumatori 20,9 17,8 3,1 Ex-Fumatori 31,7 25,2 6,5 Mai fumato 47,3 57,0 * Austria, Danimarca, Francia, Germania, Grecia, Italia, Olanda, Spagna, Svezia, Svizzera. Fonte: Rif. Bibliog. 11 USA Europa Malattie cardiache , ,4 Diabete , ,9 Obesità , ,1 Cancro , ,4

20
SCENARIO DI sanità pubblica

21
Promozione della salute

22
La salute in tutte le politiche

23
E’ cruciale che gli individui si assumano la loro responsabilità nei confronti della loro salute cardiovascolare, ma è necessario che i politici affrontino seriamente la questione delle diseguaglianze nella salute e riducano il potere delle lobbies delle industrie del cibo e del tabacco che hanno l’interesse a perpetuare lo status quo.

24
Promozione della salute
Sanità d’iniziativa Promozione della salute

25
Pazienti molto complessi
Livello 3 Pazienti molto complessi CASE MANAGEMENT Livello 2 Pazienti a alto rischio DISEASE MANAGEMENT 70-80% dei pazienti Livello 1 Con il giusto supporto le persone possono imparare a essere attivi protagonisti della loro condizione PROMOZIONE DELLA SALUTE

27
DENMARK FRANCE GERMANY THE NETHERLANDS SWEDEN UNITED KINGDOM AUSTRALIA CANADA

28
The overall aim that we set ourselves in this book was to compile an in-depth assessment of the health system response to the rising burden of chronic disease in each of the eight countries, by focusing on three key areas: (1) a detailed examination of the current situation; (2) a description of the policy framework and future scenarios; and (3) evaluation and lessons learnt, building on a common template developed by the editors.
 a detailed examination of the current situation; (2) a description of the policy framework and future scenarios; and. (3) evaluation and lessons learnt, building on a common template developed by the editors.")
29
The template was informed, to great extent, by the Chronic Care Model (CCM) developed by Wagner and colleagues in Seattle. This model presents a structure for organizing health care; it comprises four interacting components that are considered key to providing high-quality care for those with chronic health problems: self-management support, delivery system design, decision support, and clinical information systems.

30
DENMARK FRANCE GERMANY THE NETHERLANDS SWEDEN UNITED KINGDOM AUSTRALIA CANADA

32
THE CHRONIC CARE MODEL

34
Barbara Starfield

35
Person-focused care Person-focused care over time makes it possible to identify, early in life, those conditions that are likely to influence subsequent ill health and, therefore, to attempt to reduce their impact. It also provides the continuity of attention that is important in reducing the impact of chronic illnesses and reducing the likelihood of the progression to more serious illness and to more multimorbidity.

36
We need guidelines that are appropriate to person-focused care, not disease- focused care. Only primary care physicians can understand this, because they do not focus on particular organ systems and because they experience these realities every day in their practices. Primary care physicians will have to continue to advocate for primary care- oriented health systems, because it is the only hope for achieving greater equity through appropriate medical interventions.

Presentazioni simili





 Università degli Studi, Pavia (founder) IRCCS Fondazione.>")

















>")