Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Diego Peroni Le manifestazioni allergologiche particolari:
Orticaria / Angioedema La definizione Diego Peroni U.O.S. Allergologia Pediatrica Azienda Ospedaliera Universitaria Integrata Verona

2
Orticaria cronica- Angioedema
Orticaria associata o meno a angioedema che dura per più di 6-8 settimane con sintomatologia quotidiana. Orticaria Angioedema Pomfo: lesione cutanea evanescente, con centro edematoso, pallido e margini iperemici. Interessa gli strati superficiali del derma. Edema per stravaso capillare dai vasi del derma profondo o del sottocute Istamina LT C5a

3
Orticaria cronica- Angioedema
Orticaria associata o meno a angioedema che dura per più di 6-8 settimane con sintomatologia quotidiana. 80% dei casi di orticaria cronica presenta lesioni da orticaria associate a angioedema. Orticaria Angioedema Pomfo: lesione cutanea evanescente, con centro edematoso, pallido e margini iperemici. Interessa gli strati superficiali del derma. Edema per stravaso capillare dai vasi del derma profondo o del sottocute Istamina LT C5a

4
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
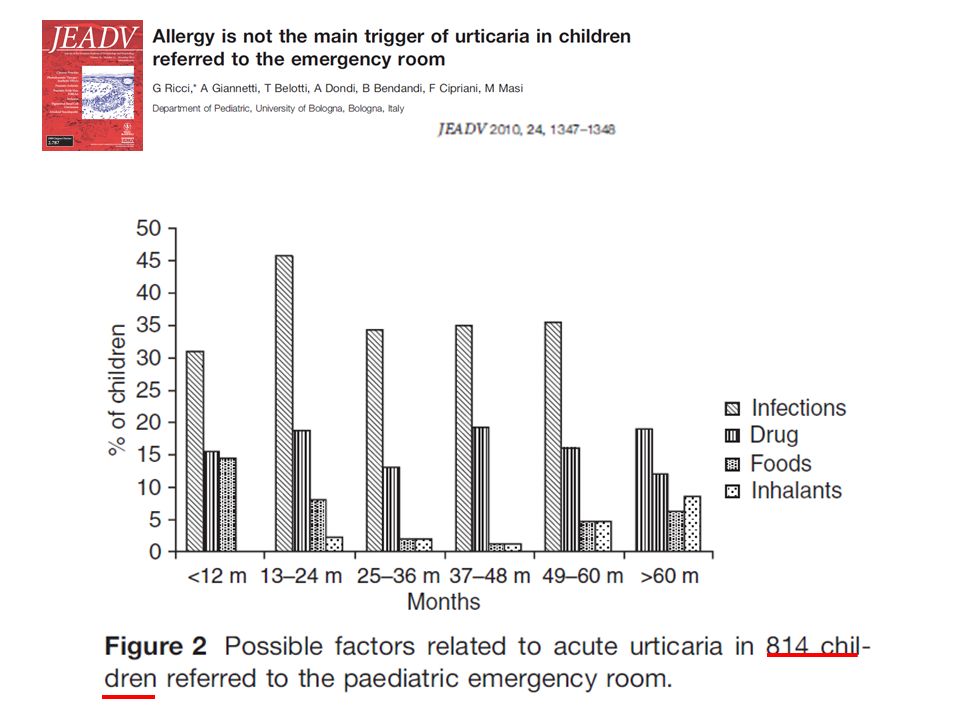
La definizione L’orticaria acuta 4

5
Una causa evidenziata in meno del 50% dei casi:
Almeno un episodio di orticaria acuta nella vita con prevalenza del 15-20% nella popolazione generale Una causa evidenziata in meno del 50% dei casi: 40% postinfettiva 10% FANS 1% alimenti Un alimento è sospettato nel 63% dei casi, ma viene dimostrato solo nell’1%

7
November 2012

8
Terapia orticaria EAACI/GA2LEN/EDF/WAO guideline: management of urticaria. T. Zuberbier, R. Asero et al. Allergy 2009: 64: 1417–1426 8

9
9

12
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’orticaria acuta L’orticaria cronica La diagnosi

13
Orticaria cronica Orticaria associata a angioedema che dura da più di 6-8 settimane …. Orticaria Angioedema Pomfo: lesione cutanea evanescente, con centro edematoso, pallido e margini iperemici. Interessa gli strati superficiali del derma. Edema per stravaso capillare dai vasi del derma profondo o del sottocute Istamina LT C5a

14
Orticaria Cronica: Diagnosi Eziologica
1° valutazione: Anamnesi Esame obiettivo (se presenti valutare le lesioni cutanee) Somministrare questionario e consegnare diario giornaliero Test per dermografismo Emocromo, VES, PCR. Prescrivere antistaminici Informare genitori del carattere benigno della malattia Informare i genitori che nella maggior parte dei casi la causa rimane ignota Laboratory tests and identified diagnoses in patients with physical and chronic urticaria and angioedema: A systematic review Martina M. et al. J Am Acad Dermatol 2003
 Somministrare questionario e consegnare diario giornaliero. Test per dermografismo. Emocromo, VES, PCR. Prescrivere antistaminici. Informare genitori del carattere benigno della malattia. Informare i genitori che nella maggior parte dei casi la causa rimane ignota. Laboratory tests and identified diagnoses in patients with physical and chronic urticaria and angioedema: A systematic review. Martina M. et al. J Am Acad Dermatol")
15
Questionario - Orticaria
1. Quando e’iniziato 2. Frequenza e durata dei ponfi 3. Variazioni nel corso del giorno 4. Capita in occasione di weekend, vacanze, e soggiorni all’estero 5. Forma, diametro, e distribuzione dei ponfi 6. Angioedema associato 7. Sintomi soggettivi associati, come dolore 8. Storia familiare e/o personale di atopia, orticaria 9. Precedenti o in corso allergie, infezioni, patologie interne, o altre possibili cause 10. Patologie Psicosomatiche e/o psichiatriche 11. Trattamenti chirurgici ed eventi durante l’intervento 12. Problemi gastrici/intestinali (feci, flatulenza) 13. Induzione da agenti fisici o da sforzo 14. Uso di farmaci (NSAIDs, iniezioni, vaccinazioni, ACE inibitori, ormoni, lassativi, gocce per orecchie e occhi e rimedi alternativi) 15. Correlazione con l’ingestione di alimenti 16. Relazione con il ciclo menstruale 17. Abitudine al fumo 18. Tipo di lavoro 19. Hobby 20. Stress (eustress e distress) 21. Qualita’ della vita in relazione all’orticaria ed impatto and emotivo 22. Terapia precedente e risposta alla terapia EAACI/GA2LEN/EDF/WAO guideline: definition, classification and diagnosis of urticaria. T. Zuberbier, R. Asero et al. Allergy 2009: 64: 1417–1426
 13. Induzione da agenti fisici o da sforzo 14. Uso di farmaci (NSAIDs, iniezioni, vaccinazioni, ACE inibitori, ormoni, lassativi, gocce per orecchie e occhi e rimedi alternativi) 15. Correlazione con l’ingestione di alimenti 16. Relazione con il ciclo menstruale 17. Abitudine al fumo 18. Tipo di lavoro 19. Hobby 20. Stress (eustress e distress) 21. Qualita’ della vita in relazione all’orticaria ed impatto and emotivo 22. Terapia precedente e risposta alla terapia EAACI/GA2LEN/EDF/WAO guideline: definition, classification. and diagnosis of urticaria. T. Zuberbier, R. Asero et al. Allergy 2009: 64: 1417–1426.")
16
DIARIO - ORTICARIA Giorno Terapia in corso Assunzione di cibi
Assunzione di farmaci Prurito Dolore Altri sintomi (febbre, g.e, artralgia) Estensione Durata Luogo e situazione (sport, doccia ..) Data e ora Nome del paziente ……………………... Settimana dal…………. al ……………..
 Estensione. Durata. Luogo e situazione. (sport, doccia ..) Data e ora. Nome del paziente ……………………... Settimana dal…………. al ……………..")
17
BSACI guidelines for the management of chronic urticaria and angio-oedema. R. J. Powell. CEA, 2007; 37, 631–650.

18
Orticaria cronica Diagnosi eziologica
2° valutazione: Valutazione andamento clinico (visione diario) Esame obiettivo Esecuzione esami diagnostici di 2° livello in base ai dati raccolti. Eventuale sospensione di farmaci considerati triggers. Prescrivere antistaminici (eventuale progressione negli step terapeutici). Laboratory tests and identified diagnoses in patients with physical and chronic urticaria and angioedema: A systematic review Martina M. J Am Acad Dermatol 2003
 Esame obiettivo. Esecuzione esami diagnostici di 2° livello in base ai dati raccolti. Eventuale sospensione di farmaci considerati triggers. Prescrivere antistaminici (eventuale progressione negli step terapeutici). Laboratory tests and identified diagnoses in patients with physical and chronic urticaria and angioedema: A systematic review. Martina M. J Am Acad Dermatol")
19
EAACI/GA2LEN/EDF/WAO guideline: definition, classification and diagnosis of urticaria
Zuberbier T, Allergy 2009; 64: 1417 Recommended diagnostic tests in frequent urticaria subtypes

20
Esami diagnostici di 2° livello – BSACI guidelines. CEA 2007
Eziologia Che esami Idiopatica (40-50%) Indagini negative Autoimmune ANA, ab antitiroide, ASST Da stimolo fisico Challenge con lo stimolo appropriato Da farmaci Sospensione (beneficio settimane-mesi) Infezioni Sierologie in base alla storia clinica Allergia SPTs, ImmunoCAP Deficit C1 esterasi-inibitore C4, C1 inibitore (Ag., Funz.) Vasculite ANCA, ANA, C3, Ig, sierologie epatite, funzionalita’ epatica e renale, biopsia cutanea Pat. linfoproliferativa Paraproteine Additivi alimentari Esclusione e reintroduzione
 Indagini negative. Autoimmune. ANA, ab antitiroide, ASST. Da stimolo fisico. Challenge con lo stimolo appropriato. Da farmaci. Sospensione (beneficio settimane-mesi) Infezioni. Sierologie in base alla storia clinica. Allergia. SPTs, ImmunoCAP. Deficit C1 esterasi-inibitore. C4, C1 inibitore (Ag., Funz.) Vasculite. ANCA, ANA, C3, Ig, sierologie epatite, funzionalita’ epatica e renale, biopsia cutanea. Pat. linfoproliferativa. Paraproteine. Additivi alimentari. Esclusione e reintroduzione.")
21
..ma non dimentichiamo altre cause di Orticaria….
Pseudoallergeni (conservanti, coloranti, additivi). Infezione da Helicobacter Pylori. Infezioni parassitarie. Infezioni delle vie urinarie. Celiachia. Manifestazione iniziale di malattie reumatologiche sistemiche (JRA, SLE). L’ OC rappresenta spesso il sintomo di esordio. BSACI guidelines for the management of chronic urticaria and angio-oedema R. J. Powell. CEA 2007; 37, 631–650.
. Infezione da Helicobacter Pylori. Infezioni parassitarie. Infezioni delle vie urinarie. Celiachia. Manifestazione iniziale di malattie reumatologiche sistemiche (JRA, SLE). L’ OC rappresenta spesso il sintomo di esordio. BSACI guidelines for the management of chronic urticaria and angio-oedema. R. J. Powell. CEA 2007; 37, 631–650.")
22
Patogenesi di asma e CU esacerbati da FANS
FANS e COX 1 inibitori Asma Urticaria angioedema Cutaneous Reactions to Aspirin and Nonsteroidal Antiinflammatory Drugs Mario Sánchez-Borges, Clinical Reviews in Allergy & Immunology Volume 24, 2003

23
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’orticaria acuta L’orticaria cronica La diagnosi Le nuove evidenze

24
Activation of blood coagulation in chronic urticaria: pathophysiological and clinical implications
Cugno Intern Emerg Med; 2010, 5:97

25
Cugno Intern Emerg Med; 2010, 5:97
Activation of blood coagulation in chronic urticaria: pathophysiological and clinical implications Cugno Intern Emerg Med; 2010, 5:97 Mechanisms of eosinophil and mast cell activation in chronic urticaria (CU).
.")
26
Cugno Intern Emerg Med; 2010, 5:97
Activation of blood coagulation in chronic urticaria: pathophysiological and clinical implications Cugno Intern Emerg Med; 2010, 5:97 Mechanisms of eosinophil and mast cell activation in chronic urticaria (CU). Mast cells release histamine and other inflammatory mediators after stimulation by autoantibodies directed against the high-affinity IgE receptor (FceRI) and IgE, complement anaphylatoxin C5a, eosinophil-derived major basic protein (MBP) and possibly other molecules
. Mast cells release histamine and other inflammatory. mediators after stimulation by autoantibodies directed against the high-affinity IgE receptor (FceRI) and IgE, complement anaphylatoxin C5a, eosinophil-derived major basic protein (MBP) and. possibly other molecules.")
27
Presenza di IgG e IgM anti IgE
Pathogenesis of chronic urticaria A. P. Kaplan Clin Exp All, 2009, 39, 777 Presenza di IgG e IgM anti IgE o anti recettore IgE con attività istamino liberatrice sulle mast cells nel 40-60% dei pazienti con orticaria cronica.

28
Cugno Intern Emerg Med; 2010, 5:97
Activation of blood coagulation in chronic urticaria: pathophysiological and clinical implications Cugno Intern Emerg Med; 2010, 5:97 Mechanisms of eosinophil and mast cell activation in chronic urticaria (CU). Eosinophils are activated by autoantibodies directed against the low-affinity IgE receptor (FceRII) and potentially by other factors, release MBP and express tissue factor which in turn activates the coagulation cascade (factors VII, X, V and prothrombin) leading to thrombin generation.
. Eosinophils are activated by autoantibodies directed against the low-affinity IgE receptor (FceRII) and potentially by other factors, release MBP and express tissue factor which in turn activates the coagulation cascade (factors VII, X, V and prothrombin) leading to thrombin generation.")
29
D-dimer in CU patients with
Thrombin generation is demonstrated in CU patients by the increased plasma levels of the fragment F1+2 released from prothrombin after its activation. Finally, fibrin degradation is documented by elevated plasma levels of the fibrin fragment D-dimer in CU patients with active disease Activation of blood coagulation in chronic urticaria: pathophysiological and clinical implications Cugno Intern Emerg Med; 2010, 5:97 Mechanisms of eosinophil and mast cell activation in chronic urticaria (CU). Eosinophils are activated by autoantibodies directed against the low-affinity IgE receptor (FceRII) and potentially by other factors, release MBP and express tissue factor which in turn activates the coagulation cascade (factors VII, X, V and prothrombin) leading to thrombin generation.
. Eosinophils are activated by autoantibodies directed against the low-affinity IgE receptor (FceRII) and potentially. by other factors, release MBP and express tissue factor which in turn activates the coagulation cascade (factors VII, X, V and prothrombin) leading to thrombin generation.")
30
Effetto della trombina
Vasodilatazione Trombina Attivazione diretta di C5a bypassando C3 Produzione di mediatori infiammatori Attivazione diretta degranulazione mastocitaria

31
Pathogenesis of chronic urticaria
A. P. Kaplan Clin Exp All, 2009, 39, 777 ASST - Autologous Serum Skin Test - Circa il 50% dei pazienti con Orticaria cronica idiopatica presenta ASST + ma: In circa il 50% non c’ è corrispondenza tra test in vivo e in vitro; Decomplementazione e deplezione di IgG dal siero non riducono la capacità di indurre reazione in vivo; Il 50% delle orticarie idiopatiche rimane comunque inspiegato.

32
Pathogenesis of chronic urticaria
A. P. Kaplan Clin Exp All, 2009, 39, 777 ASST - Autologous Serum Skin Test - Circa il 50% dei pazienti con Orticaria cronica idiopatica presente ASST + ma: In circa il 50% non c’ è corrispondenza tra test in vivo e in vitro; Decomplementazione e deplezione di IgG dal siero non riducono la capacità di indurre reazione in vivo; Il 50% delle orticarie idiopatiche rimane comunque inspiegato. Altri fattori istaminoliberatori potrebbero essere implicati nella patogenesi della malattia.

33
Orticaria cronica, ASST, APST e HRA
APST positivo nel 75-85% dei casi ASST positivo nel 50-60% dei casi HRA positivo nel 25-30% dei casi

34
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’orticaria acuta L’orticaria cronica La diagnosi Le nuove evidenze La terapia

35
Terapia orticaria cronica
EAACI/GA2LEN/EDF/WAO guideline: management of urticaria. T. Zuberbier, R. Asero et al. Allergy 2009: 64: 1417–1426

36
UAS-Score How to assess disease activity in patients with chronic urticaria? A. Młynek et al. Allergy 2008: 63: 777–780

37
EAACI taskforce position paper: evidence for autoimmune urticaria and proposal for defining diagnostic criteria. Konstantinou GN Allergy 2013 Functional autoantibodies in chronic urticaria (CU) patient sera have been demonstrated against IgE and FcεRIα by basophil and mast cell histamine release assays and by basophil activation assays Approximately 25% of CU patients have a positive basophil histamine release assay and show autoreactivity (a positive autologous serum skin test), whereas 50% are negative regarding both. Functionality of CU sera appears to be complement dependent on mast cells but not exclusively on basophils. Basophil activation by CU sera is predominantly restricted to IgG1 and IgG3 subclasses.
 patient sera have been demonstrated against IgE and FcεRIα by basophil and mast cell histamine release assays and by basophil activation assays. Approximately 25% of CU patients have a positive basophil histamine release assay and show autoreactivity (a positive autologous serum skin test), whereas 50% are negative regarding both. Functionality of CU sera appears to be complement dependent on mast cells but not exclusively on basophils. Basophil activation by CU sera is predominantly restricted to IgG1 and IgG3 subclasses.")
38
Circumstantial evidence for CU being an autoimmune disease comes from
EAACI taskforce position paper: evidence for autoimmune urticaria and proposal for defining diagnostic criteria. Konstantinou GN Allergy 2013 Circumstantial evidence for CU being an autoimmune disease comes from an observed association with other autoimmune diseases, a strong association between serum functionality and HLA-DR4 haplotype and the good response of CU patients to immunotherapies

39
Chronic urticaria and autoimmunity: Associations found in a large population study
Confino-Cohen, JACI 2012;129:1307 In patients with CU OR for 30 – 25 – 20 – 15 – 10 – 05 – 12,778 patients with CU during 17 years in a large health maintenance organization. A control group of 10,714 patients who had no CU. 28.8 17.3 13.2 6% Hypo- thyroidism Hyper-thyroidism Rheumatoid arthritis

40
Type I diabetes mellitus
Chronic urticaria and autoimmunity: Associations found in a large population study Confino-Cohen, JACI 2012;129:1307 In patients with CU OR for 30 – 25 – 20 – 15 – 10 – 05 – 12,778 patients with CU during 17 years in a large health maintenance organization. A control group of 10,714 patients who had no CU. 26.9 15.2 14.6 7.7 6% Type I diabetes mellitus Sjögren syndrome Celiac disease Systemic LE

41
Konstantinou G. N, Allergy 2013;68:27-36
EAACI taskforce position paper: evidence for autoimmune urticaria and proposal for defining diagnostic criteria Konstantinou G. N, Allergy 2013;68:27-36 Chronic urticaria (CU). Approximately 25% of CU patients have a positive basophil histamine release assay and show autoreactivity (a positive autologous serum skin test), whereas 50% are negative regarding both. Basophil activation by CU sera is predominantly restricted to IgG1 and IgG3 subclasses. Circumstantial evidence for CU being an autoimmune disease comes from an observed association with other autoimmune diseases, a strong association between serum functionality and HLA-DR4 haplotype and the good response of CU patients to immunotherapies.
. Approximately 25% of CU patients have a. positive basophil histamine release assay and. show autoreactivity (a positive autologous serum skin test), whereas 50% are negative regarding both. Basophil activation by CU sera is predominantly restricted to IgG1 and IgG3 subclasses. Circumstantial evidence for CU being an autoimmune disease comes from an observed association with other autoimmune diseases, a strong association between serum functionality and HLA-DR4 haplotype and the good response of CU patients to immunotherapies.")
42
Konstantinou G. N, Allergy 2013;68:27-36
EAACI taskforce position paper: evidence for autoimmune urticaria and proposal for defining diagnostic criteria Konstantinou G. N, Allergy 2013;68:27-36

43
How not to miss autoinflammatory diseases masquerading as urticaria
Krause K, Allergy 2012;67:

44
Prospettive terapeutiche
Eparina si è dimostrata efficace nel trattamento dell’ O.C TAO (warfarin) migliora i sintomi di pazienti con O.C non responsivi all’ antistaminico Agenti antifibrinolitici (Ac. Tranaxemico) determinano una buona risposta clinica nell’ O.C. EAACI taskforce position paper: evidence for autoimmune urticaria and proposal for defining diagnostic criteria. Konstantinou GN Allergy 2013
 migliora i sintomi di pazienti con O.C non responsivi all’ antistaminico. Agenti antifibrinolitici (Ac. Tranaxemico) determinano una buona risposta clinica nell’ O.C. EAACI taskforce position paper: evidence for autoimmune urticaria and proposal for defining diagnostic criteria. Konstantinou GN Allergy")
45
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’orticaria acuta L’orticaria cronica La diagnosi Le nuove evidenze Il caso clinico

46
2 mesi di sintomi continui.
APR: Otiti ricorrenti; Bronchiti asmatiformi ricorrenti; Autismo. P.P 5 aa e 6 mesi Persistenza del quadro: 10/02/2012: PS VR. MT dx iperemica e bombata: Deltacortene 2.5 mg/die Aerius + Fenistil Singulair Orelox (OM persistente). 20/12/2011 Otite Amoxicillina comparsa di rash orticarioide Cetirizina 0.25 mg/kg + Bentelan 4 mg/die DH allergologia 20/02/2012 Peggioramento orticaria PS a BZ: Deltacortene 15 mg/die Peggioramento PS BZ: Augmentin Zinnat; Zirtec Aerius + Fenistil la sera Ancora deltacortene 2.5 mg Totale: 2 mesi di sintomi continui. 2 mesi di CSO; 8 visite specialistiche; 4 Abt diverse. Visita allergologica BZ: Controllo esami ematici: TAS 329IU/ml, resto normale. Allergia agli acari. Scalo deltacortene a 5 mg 2.5 mg/die + Augmentin (MT iperemiche + TAS elevato). Profilassi ambientale. 2 visite dermatologiche BZ dieta bianca senza nessun beneficio
. 20/12/2011. Otite Amoxicillina comparsa di rash orticarioide Cetirizina 0.25 mg/kg + Bentelan 4 mg/die. DH allergologia 20/02/2012. Peggioramento orticaria PS a BZ: Deltacortene 15 mg/die. Peggioramento PS BZ: Augmentin Zinnat; Zirtec Aerius + Fenistil la sera. Ancora deltacortene 2.5 mg. Totale: 2 mesi di sintomi continui. 2 mesi di CSO; 8 visite specialistiche; 4 Abt diverse. Visita allergologica BZ: Controllo esami ematici: TAS 329IU/ml, resto normale. Allergia agli acari. Scalo deltacortene a 5 mg 2.5 mg/die + Augmentin (MT iperemiche + TAS elevato). Profilassi ambientale. 2 visite dermatologiche BZ dieta bianca senza nessun beneficio.")
47
diego.peroni@univr.it DH allergologia 20/02/2012 APST +
Immunoglobuline: nella norma; Sierologie HBV, HCV, EBV, Parvovirus B19: nella norma; Ricerca parassiti fecali: neg; Ab antigliadina anti TG: neg; Ricerca HP Pylori nelle feci: neg. D-dimero: 1.2 mg/l .

48
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’angioedema I meccanismi 48

49
BSACI guidelines for the management of chronic urticaria and angio-oedema. R. J. Powell. CEA, 2007; 37, 631–650. 49

50
Hereditary angio-oedema. Longhurst H. Lancet 2012; 379:474
Angio-oedema of hand Capsule endoscopy during abdominal attack Erythema marginatum on anterior chest wall 50

51
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 Simplified representation of the kinin system. Bradykinin is generated through the cleavage of high molecular weight kininogen (HK) by plasma kallikrein during contact-system activation The contact system (green box) consists of the substrate HK and the two zymogens prekallikrein and factor XII (FXII), which activate each other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK molecule, and other breakdown products (cleaved HK). Bradykinin release is facilitated by the presence of plasmin. The most important inhibitor of the contact system is C1- INH, which inactivates kallikrein and FXIIa. Tissue kallikrein cleaves low molecular weight kininogen (LK), generating kallidin, which is converted to bradykinin by aminopeptidases. The physiological inhibitor of tissue kallikrein is kallistatin. Tissue kallikrein activates prorenin to rennin, which, in turn, activates angiotensinogen to angiotensin I (purple box). Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting enzyme (ACE). Other important kininases are aminopeptidase P and neutral endopeptidase. kininase II (i.e. ACE) not only degrades bradykinin but also activates angiotensin I to angiotensin II. 51
 by plasma kallikrein during contact-system activation. The contact system (green box) consists of the substrate HK and the two zymogens prekallikrein and factor XII (FXII), which activate each. other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK. molecule, and other breakdown products (cleaved HK). Bradykinin release is facilitated by the presence of plasmin. The most important inhibitor of the contact system is C1- INH, which inactivates kallikrein and FXIIa. Tissue kallikrein cleaves low molecular weight kininogen (LK), generating kallidin, which is converted to bradykinin by. aminopeptidases. The physiological inhibitor of tissue kallikrein is kallistatin. Tissue kallikrein activates prorenin to rennin, which, in turn, activates angiotensinogen to. angiotensin I (purple box). Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting. enzyme (ACE). Other important kininases are aminopeptidase P and neutral endopeptidase. kininase II (i.e. ACE) not only degrades bradykinin but also activates. angiotensin I to angiotensin II. 51.")
52
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 The contact system (green box) consists of the substrate HK (high MW kininogen) and the two zymogens prekallikrein and factor XII (FXII), which activate each other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK molecule, and other breakdown products (cleaved HK). The contact system (green box) consists of the substrate HK and the two zymogens prekallikrein and factor XII (FXII), which activate each other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK molecule, and other breakdown products (cleaved HK). Bradykinin release is facilitated by the presence of plasmin. The most important inhibitor of the contact system is C1- INH, which inactivates kallikrein and FXIIa. Tissue kallikrein cleaves low molecular weight kininogen (LK), generating kallidin, which is converted to bradykinin by aminopeptidases. The physiological inhibitor of tissue kallikrein is kallistatin. Tissue kallikrein activates prorenin to rennin, which, in turn, activates angiotensinogen to angiotensin I (purple box). Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting enzyme (ACE). Other important kininases are aminopeptidase P and neutral endopeptidase. kininase II (i.e. ACE) not only degrades bradykinin but also activates angiotensin I to angiotensin II. 52
 consists of the substrate HK (high MW kininogen) and the two zymogens prekallikrein and factor XII (FXII), which activate each. other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK molecule, and other breakdown products (cleaved HK). The contact system (green box) consists of the substrate HK and the two zymogens prekallikrein and factor XII (FXII), which activate each. other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK. molecule, and other breakdown products (cleaved HK). Bradykinin release is facilitated by the presence of plasmin. The most important inhibitor of the contact system is C1- INH, which inactivates kallikrein and FXIIa. Tissue kallikrein cleaves low molecular weight kininogen (LK), generating kallidin, which is converted to bradykinin by. aminopeptidases. The physiological inhibitor of tissue kallikrein is kallistatin. Tissue kallikrein activates prorenin to rennin, which, in turn, activates angiotensinogen to. angiotensin I (purple box). Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting. enzyme (ACE). Other important kininases are aminopeptidase P and neutral endopeptidase. kininase II (i.e. ACE) not only degrades bradykinin but also activates. angiotensin I to angiotensin II. 52.")
53
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 The most important inhibitor of the contact system is C1-INH, which inactivates kallikrein and FXIIa. Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting enzyme (ACE). The contact system (green box) consists of the substrate HK and the two zymogens prekallikrein and factor XII (FXII), which activate each other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK molecule, and other breakdown products (cleaved HK). Bradykinin release is facilitated by the presence of plasmin. The most important inhibitor of the contact system is C1- INH, which inactivates kallikrein and FXIIa. Tissue kallikrein cleaves low molecular weight kininogen (LK), generating kallidin, which is converted to bradykinin by aminopeptidases. The physiological inhibitor of tissue kallikrein is kallistatin. Tissue kallikrein activates prorenin to rennin, which, in turn, activates angiotensinogen to angiotensin I (purple box). Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting enzyme (ACE). Other important kininases are aminopeptidase P and neutral endopeptidase. kininase II (i.e. ACE) not only degrades bradykinin but also activates angiotensin I to angiotensin II. 53
. The contact system (green box) consists of the substrate HK and the two zymogens prekallikrein and factor XII (FXII), which activate each. other to form the enzymes kallikrein and activated factor XII (FXIIa), respectively. The cleavage of HK enables the release of bradykinin, which is located inside the HK. molecule, and other breakdown products (cleaved HK). Bradykinin release is facilitated by the presence of plasmin. The most important inhibitor of the contact system is C1- INH, which inactivates kallikrein and FXIIa. Tissue kallikrein cleaves low molecular weight kininogen (LK), generating kallidin, which is converted to bradykinin by. aminopeptidases. The physiological inhibitor of tissue kallikrein is kallistatin. Tissue kallikrein activates prorenin to rennin, which, in turn, activates angiotensinogen to. angiotensin I (purple box). Bradykinin is degraded by peptidases, such as human kininase I, also called carboxypeptidase N, and kininase II, also called angiotensinconverting. enzyme (ACE). Other important kininases are aminopeptidase P and neutral endopeptidase. kininase II (i.e. ACE) not only degrades bradykinin but also activates. angiotensin I to angiotensin II. 53.")
54
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 Representation of the pathogenesis of angioedema due to C1-INH deficiency In HAE, the deficiency of C1-INH is due to a mutation in the C1-INH gene, which impairs C1-INH synthesis or function. In AAE, C1-INH deficiency is due to the cleavage of C1-INH by autoantibodies or to its consumption by neoplastic, mainly lymphoproliferative, tissue. 54

55
reduction of its plasma level.
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 Representation of the pathogenesis of angioedema due to C1-INH deficiency Reduced C1-INH plasma levels result in hyperactivation of the classical complement pathway with increased consumption of C1-INH and further reduction of its plasma level. 55

56
Criteria for diagnosis of hereditary angio-oedema
Hereditary angio-oedema. Longhurst H. Lancet 2012; 379:474 Criteria for diagnosis of hereditary angio-oedema 56

57
Type III hereditary angioedema: defined, but not understood
Type III hereditary angioedema: defined, but not understood. Kaplan, Ann Allergy Asthma Immunol 2012;109:153 Type III hereditary angioedema (HAE) is a familial form of angioedema in which complement C4 and C1 inhibitor (C1 INH) protein and function are normal. Most patients are women, although an occasional male is identified, and a close association with estrogen as a precipitant of attacks of angioedema is seen (contraception, postmenopausal symptom control). Like types I and II HAE, angioedema is recurrent, it is not associated with urticaria, and it is unresponsive to antihistamines or corticosteroids. 57
 is a familial form of angioedema in which complement C4 and C1 inhibitor (C1 INH) protein and function are normal. Most patients are women, although an occasional male is identified, and a close association with estrogen as a precipitant of attacks of angioedema is seen (contraception, postmenopausal symptom control). Like types I and II HAE, angioedema is recurrent, it is not associated with urticaria, and it is unresponsive to antihistamines or corticosteroids. 57.")
58
We do not have a test that can be used to make the diagnosis.
Type III hereditary angioedema: defined, but not understood. Kaplan, Ann Allergy Asthma Immunol 2012;109:153 Type III hereditary angioedema (HAE) is a familial form of angioedema in which complement C4 and C1 inhibitor (C1 INH) protein and function are normal. Most patients are women, although an occasional male is identified, and a close association with estrogen as a precipitant of attacks of angioedema is seen (contraception, postmenopausal symptom control). Like types I and II HAE, angioedema is recurrent, it is not associated with urticaria, and it is unresponsive to antihistamines or corticosteroids. We do not have a test that can be used to make the diagnosis. 58
 is a familial form of angioedema in which complement C4 and C1 inhibitor (C1 INH) protein and function are normal. Most patients are women, although an occasional male is identified, and a close association with estrogen as a precipitant of attacks of angioedema is seen (contraception, postmenopausal symptom control). Like types I and II HAE, angioedema is recurrent, it is not associated with urticaria, and it is unresponsive to antihistamines or corticosteroids. We do not have a test that can be used to make the diagnosis. 58.")
59
Overproduction of bradykinin is assumed, but not proven.
Type III hereditary angioedema: defined, but not understood. Kaplan, Ann Allergy Asthma Immunol 2012;109:153 Type III hereditary angioedema (HAE) is a familial form of angioedema in which complement C4 and C1 inhibitor (C1 INH) protein and function are normal. Most patients are women, although an occasional male is identified, and a close association with estrogen as a precipitant of attacks of angioedema is seen (contraception, postmenopausal symptom control). Like types I and II HAE, angioedema is recurrent, it is not associated with urticaria, and it is unresponsive to antihistamines or corticosteroids. Overproduction of bradykinin is assumed, but not proven. 59
 is a familial form of angioedema in which complement C4 and C1 inhibitor (C1 INH) protein and function are normal. Most patients are women, although an occasional male is identified, and a close association with estrogen as a precipitant of attacks of angioedema is seen (contraception, postmenopausal symptom control). Like types I and II HAE, angioedema is recurrent, it is not associated with urticaria, and it is unresponsive to antihistamines or corticosteroids. Overproduction of bradykinin is assumed, but not proven. 59.")
60
Type III hereditary angioedema: defined, but not understood
Type III hereditary angioedema: defined, but not understood. Kaplan, Ann Allergy Asthma Immunol 2012;109:153 A mutation in factor XII, exon 9 consisting of either Thr 309 lys or Thr 309 arg has been associated with type III HAE patients, and, although specific for this disorder, it is found only in 25-30% of patients whose swelling is unexplained but is clearly familial. The mutation was reported to cause excessive conversion of prekallikrein to kallikrein and was described as a “gain of function” mutation. 60

61
Marcos, Ann Allergy Asthma Immunol 2012;109:195
Clinical, biochemical, and genetic characterization of type III hereditary angioedema in Northwest Spanish families. Marcos, Ann Allergy Asthma Immunol 2012;109:195 22 of these patients had the estrogen-dependent phenotype. All had functional C1 inhibitor activity within the normal range in periods without high estrogen levels, but during attacks (in female patients) and pregnancy, activity decreased to below 50%. The C4 and antigenic C1 inhibitor levels were always normal. Population with type III hereditary angioedema. 29 patients (26 female, 3 male). 61
 and pregnancy, activity decreased to below 50%. The C4 and antigenic C1 inhibitor levels were always normal. Population with type III hereditary angioedema. 29 patients (26 female, 3 male). 61.")
62
Marcos, Ann Allergy Asthma Immunol 2012;109:195
Clinical, biochemical, and genetic characterization of type III hereditary angioedema in Northwest Spanish families. Marcos, Ann Allergy Asthma Immunol 2012;109:195 22 of these patients had the estrogen-dependent phenotype. All had functional C1 inhibitor activity within the normal range in periods without high estrogen levels, but during attacks (in female patients) and pregnancy, activity decreased to below 50%. The C4 and antigenic C1 inhibitor levels were always normal. Population with type III hereditary angioedema. 29 patients (26 female, 3 male). All studied patients had the c.1032C>A, Thr309Lys mutation in the factor XII gene. 62
 and pregnancy, activity decreased to below 50%. The C4 and antigenic C1 inhibitor levels were always normal. Population with type III hereditary angioedema. 29 patients (26 female, 3 male). All studied patients had the c.1032C>A, Thr309Lys mutation in the factor XII gene. 62.")
63
BSACI guidelines for the management of chronic urticaria and angio-oedema. R. J. Powell. CEA, 2007; 37, 631–650. 63

64
BSACI guidelines for the management of chronic urticaria and angio-oedema. R. J. Powell. CEA, 2007; 37, 631–650. 64

65
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’angioedema I meccanismi La terapia 65

66
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 Current and potentially new treatments for angioedema due to hereditary or acquired C1-INH deficiency 66

67
Terapia angioedema Terapia cronica profilattica Terapia attacco acuto
Idratazione, Antidolorifici, Androgeni blandi: Danazolo Stanazolo Metiltestosterone Antifibrinolitici Berinert (pdC1- INH pastorizzato, liofilizzato concentrato); Ecallantide (inibitore della Kallikreina); Icatibant (antagonista competitivo di BK2R); Rhucin (C1-INH ricombinante umano) FPP (fresh frozen plasma) SDP (solvent detergent- treated plasma) Effetti collaterali 67
; Ecallantide (inibitore della Kallikreina); Icatibant (antagonista competitivo di BK2R); Rhucin (C1-INH ricombinante umano) FPP (fresh frozen plasma) SDP (solvent detergent- treated plasma) Effetti collaterali. 67.")
68
pdcC1 INH umano, indicato per gli attachi acuti di HAE con interessamento addominale, facciale e laringeo negli adulti e negli adolescenti. 68

69
Le manifestazioni allergologiche particolari: Orticaria / Angioedema
La definizione L’angioedema I meccanismi La terapia Il caso clinico 69

70
Angioedema – Francesca 4 anni
Accesso al PS per comparsa di edema importante a livello dell’arto sup di sin Pregressa faringite trattata con Amox-Clavul Familiarita’ per angioedema ereditario (madre) E.O. Edema a livello della mano e avambraccio di sin, cute calda, pallida. Non dolore Rx avambraccio e mano: non lesioni ossee a focolaio Ecodoppler: pervio l’asse venoso succlavio-ascellare-omerale. Diffuso infarcimento dei tessuti molli Complemento C g/L (vn ), C1 inibitore 0.06 g/L (vn ) Conclusioni: Angioedema ereditario Si consiglia visita specialistica presso la Clinica Medica Milano In caso di emergenza Berinert f. 500 UI 70
 E.O. Edema a livello della mano e avambraccio di sin, cute calda, pallida. Non dolore. Rx avambraccio e mano: non lesioni ossee a focolaio. Ecodoppler: pervio l’asse venoso succlavio-ascellare-omerale. Diffuso infarcimento dei tessuti molli. Complemento C g/L (vn ), C1 inibitore 0.06 g/L (vn ) Conclusioni: Angioedema ereditario. Si consiglia visita specialistica presso la Clinica Medica Milano. In caso di emergenza Berinert f. 500 UI. 70.")
71
71

72
72

73
Cugno M, Trends in Molecular Medicine, 2009; 15: 69
C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Cugno M, Trends in Molecular Medicine, 2009; 15: 69 73

74
Diego Peroni Le sindromi da attivazione mastocitaria
Le manifestazioni allergologiche particolari: Le sindromi da attivazione mastocitaria Diego Peroni U.O.S. Allergologia Pediatrica Azienda Ospedaliera Universitaria Integrata Verona 74

75
Characteristics of human mast cell subsets
75

76
76

77
Mast cell activation syndrome: Proposed diagnostic criteria.
Selected mast cell activators of clinical relevance Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 77

78
Mast cell activation syndrome: Proposed diagnostic criteria
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Activation of mast cells results in (1) degranulation with resulting release of preformed mediators stored in granules, including histamine, heparin, proteases, and cytokines, such as TNF-a; (2) De novo synthesis of arachidonic acid metabolites (most notably prostaglandin D2 and leukotriene C4) from membrane lipids; (3) synthesis and secretion of cytokines and chemokines 78
 degranulation with resulting release of preformed mediators stored in granules, including histamine, heparin, proteases, and cytokines, such as TNF-a; (2) De novo synthesis of arachidonic acid metabolites (most notably prostaglandin D2 and leukotriene C4) from membrane lipids; (3) synthesis and secretion of cytokines and chemokines. 78.")
79
Le sindromi da attivazione mastocitaria
Le manifestazioni allergologiche particolari: Le sindromi da attivazione mastocitaria The mast cell Mast cell activation syndrome MCAS, SM or MMCA 79

80
Disease states associated with evidence of mast cell activation
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Disease states associated with evidence of mast cell activation 80

81
Mast cell activation syndrome: Proposed diagnostic criteria
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Classification of diseases associated with mast cell activation 81

82
Mast cell activation syndrome: Proposed diagnostic criteria
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Signs and symptoms suggested to potentially occur in MCAS or mast cell activation disorder These symptoms are attributed to mast cell degranulation in mastocytosis, and those with mast cell activation disorder/ MCAS are said to have many of the same symptoms. 82

83
Mast cell activation syndrome: Proposed diagnostic criteria
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 MCAS as a distinct clinical entity has not been generally accepted, nor do there exist definitive criteria for diagnosis. Based on current understanding of this disease ‘‘syndrome’’ and on what we do know about mast cell activation and resulting pathology, we will explore and propose criteria for its diagnosis. 83

84
The minor diagnostic criteria
WHO classification of tumours of haematopoietic and lymphoid tissues. Horny HP, Lyon:IARC Press; p The diagnostic standard for systemic mastocytosis has been the demonstration of: Major criterion multifocal mast cell clusters of atypical morphology in a bone marrow biopsy specimen. The minor diagnostic criteria a tryptase level of greater than 20 ng/mL, atypical (spindle-shaped and hypogranulated) mast cell morphology, aberrant expression of CD2 and CD25 on mast cells, detection of a codon 816 mutation in c-Kit. 84
 mast cell morphology, aberrant expression of CD2 and CD25 on mast cells, detection of a codon 816 mutation in c-Kit. 84.")
85
Proposed criteria for the diagnosis of MCAS
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Proposed criteria for the diagnosis of MCAS Episodic symptoms consistent with mast cell mediator release affecting >2 organ systems evidenced as follows: a. Skin: urticaria, angioedema, flushing b. Gastrointestinal: nausea, vomiting, diarrhea, abdominal cramping c. Cardiovascular: hypotensive syncope or near syncope, tachycardia d. Respiratory: wheezing e. Naso-ocular: conjunctival injection, pruritus, nasal stuffiness Plus 85

86
Proposed criteria for the diagnosis of MCAS
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Proposed criteria for the diagnosis of MCAS 2. A decrease in the frequency or severity or resolution of symptoms with antimediator therapy: H1- and H2-histamine receptor agonists, antileukotriene medications (cysteinyl leukotriene receptor blockers or 5-lipoxygenase inhibitor), or mast cell stabilizers (cromolyn sodium) 3. Evidence of an increase in a validated urinary or serum marker of mast cell activation: documentation of an increase of the marker to greater than the patient’s baseline value during a symptomatic period on >2 occasions or, if baseline tryptase levels are persistently >15 ng, documentation of an increase of the tryptase level above baseline value on 1 occasion. Total serum tryptase level is recommended as the marker of choice; less specific (also from basophils) are 24-hour urine histamine metabolites or PGD2 or its metabolite 11-b-prostaglandin F2. 4. Rule out primary and secondary causes of mast cell activation and well-defined clinical idiopathic entities 86
, or mast cell stabilizers (cromolyn sodium) 3. Evidence of an increase in a validated urinary or serum marker of mast cell activation: documentation of an increase of the marker to greater than the patient’s baseline value during a symptomatic period on >2 occasions or, if baseline tryptase levels are persistently >15 ng, documentation of an increase of the tryptase level above baseline value on 1 occasion. Total serum tryptase level is recommended as the marker of choice; less specific (also from basophils) are 24-hour urine histamine metabolites or PGD2 or its metabolite 11-b-prostaglandin F2. 4. Rule out primary and secondary causes of mast cell activation and well-defined clinical idiopathic entities. 86.")
87
Proposed criteria for the diagnosis of MCAS
Mast cell activation syndrome: Proposed diagnostic criteria. Akin C, JACI; 2010; 126:1099 Proposed criteria for the diagnosis of MCAS MCAS for now remains an idiopathic disorder; however, in some cases it could be an early reflection of a monoclonal population of mast cells, in which case with time it could meet the criteria for MMAS as 1 or 2 minor criteria for mastocytosis are fulfilled 2. A decrease in the frequency or severity or resolution of symptoms with antimediator therapy: H1- and H2-histamine receptor agonists, antileukotriene medications (cysteinyl leukotriene receptor blockers or 5-lipoxygenase inhibitor), or mast cell stabilizers (cromolyn sodium) 3. Evidence of an increase in a validated urinary or serum marker of mast cell activation: documentation of an increase of the marker to greater than the patient’s baseline value during a symptomatic period on >2 occasions or, if baseline tryptase levels are persistently >15 ng, documentation of an increase of the tryptase level above baseline value on 1 occasion. Total serum tryptase level is recommended as the marker of choice; less specific (also from basophils) are 24-hour urine histamine metabolites or PGD2 or its metabolite 11-b-prostaglandin F2. 4. Rule out primary and secondary causes of mast cell activation and well-defined clinical idiopathic entities 87
, or mast cell stabilizers (cromolyn sodium) 3. Evidence of an increase in a validated urinary or serum marker of mast cell activation: documentation of an increase of the marker to greater than the patient’s baseline value during a symptomatic period on >2 occasions or, if baseline tryptase levels are persistently >15 ng, documentation of an increase of the tryptase level above baseline value on 1 occasion. Total serum tryptase level is recommended as the marker of choice; less specific (also from basophils) are 24-hour urine histamine metabolites or PGD2 or its metabolite 11-b-prostaglandin F2. 4. Rule out primary and secondary causes of mast cell activation and well-defined clinical idiopathic entities. 87.")
Presentazioni simili
 Valutazione quantitativa dei pazienti sofferenti di (HAE) in Francia, Germania, Italia, Spagna e UK Condotto.>")









>")








